
Abstract
Introduction
In response to the opioid crisis, the 2016 Vermont legislature commissioned a study to assess acupuncture for patients with chronic pain in the Vermont Medicaid population.
Objective
To assess the feasibility, acceptability, and effectiveness of acupuncture provided by licensed acupuncturists for Vermont Medicaid patients with chronic pain.
Methods
A total of 156 Medicaid patients with chronic pain were offered up to 12 acupuncture treatments within a 60-day period at the offices of 28 Vermont licensed acupuncturists. PROMIS® questionnaires were administered prior to and at the end of the treatment period to assess changes in pain intensity, pain interference, physical function, fatigue, anxiety, depression, sleep disturbance, and social isolation. Questionnaires also captured patients’ overall impressions of treatments as well as self-reported changes in medication use and work function.
Results
One hundred eleven women (71%) and 45 men (29%) with a wide range of pain complaints received a mean of 8.2 treatments during the intervention period. Measurements captured prior to and at the end of the treatment period showed significant improvements in group mean pain intensity, pain interference, physical function, fatigue, anxiety, depression, sleep disturbance, and social isolation as assessed by Patient-Reported Outcomes Measurement Information System (PROMIS) measures (paired t tests, P < .01). Fifty-seven percent of patients using analgesic (nonopioid) medication reported reductions in use. Thirty-two percent of patients using opioid medication reported reductions in use of opioid medication following the intervention. Seventy-four percent of employed patients reported improved capacity to work. Ninety-six percent of patients said that they would recommend acupuncture to others with chronic pain, and 91% reported qualitative improvements, including physical (31%), functional/behavioral (29%), and psycho-emotional (24%) improvements.
Conclusions
Our findings demonstrate that acupuncture treatment for chronic pain is feasible and well received by patients in the Vermont Medicaid population. Receiving care from Licensed Acupuncturists was associated with significant improvements in physical, functional, psycho-emotional, and occupational outcomes compared with before receiving acupuncture treatments.
Introduction
Chronic pain is a significant public health problem, affecting between 11% and 47% of the U.S. population.1–7 The Institute of Medicine estimates the annual cost burden of chronic pain in the U.S. noninstitutionalized civilian population to be between $560 billion and $635 billion.8,9 Chronic pain is a complex biopsychosocial phenomenon that affects a person’s psychological and emotional health, ability to work, and social function.10,11 Chronic pain has been linked to premature death 11 as well as an increased risk of suicide.12,13
Opioid prescriptions have grown rapidly over the past decades in an attempt to treat chronic pain. The rise of adverse consequences of opioid use, including misuse, addiction, injury and death has been well documented. 14 Nonopioid analgesics are also associated with significant harm. 14 Physicians and patients need effective and safe strategies for managing chronic pain. Nonpharmacologic treatments, including acupuncture, are underutilized in the treatment of chronic pain. By increasing the availability of safe, effective nonpharmacologic treatments for chronic pain, patient exposure to opioids can be reduced.
A substantial body of evidence demonstrates that acupuncture is effective for chronic pain.15–35 Consequently, a number of health policy and practice-oriented guidelines have been issued that support the use of acupuncture for chronic pain. For example, the American College of Physicians Clinical Practice Guideline recommends acupuncture for acute, subacute, and chronic low back pain (cLBP).36,37 The U.S. Department of Health and Human Services Agency for Healthcare Research and Quality concluded that acupuncture is effective for cLBP compared to placebo, sham, no treatment, usual care, or wait list controls. 38 The U.S. National Institutes of Health recommends acupuncture for low back pain and for knee osteoarthritis. 35 The FDA Education Blueprint for Health Care Providers Involved in the Management or Support of Patients with Pain suggests acupuncture among a range of available therapies as part of a multidisciplinary approach to pain management. 39
Despite this guidance, one of the barriers for the utilization of acupuncture and other nonpharmacologic treatments for chronic pain continues to be the lack of insurance reimbursement. This barrier is especially acute for the financially disadvantaged Medicaid population, a population especially effected by the opioid crisis. Acupuncture is not covered by most of Vermont’s insurance plans, including the state-funded Medicaid program. Addressing this disconnect between evidence and policy, the 2016 U.S. Health and Human Services National Pain Strategy noted that the structure of insurance payment and coverage policies “exert powerful effects on how pain is managed,” noting that financial incentives may lead consumers to “gravitate to prescription drugs over complementary or alternative treatments, creating risks for subsequent problems with opioid dependency.” 40 Likewise, the National Association of Attorneys General sent a letter signed by 37 state attorneys general to America’s Health Insurance Plans (AHIP) urging AHIP to “encourage your members to review their payment and coverage policies and revise them, as necessary and appropriate, to encourage healthcare providers to prioritize nonopioid pain management options over opioid prescriptions for the treatment of chronic, noncancer pain.” 41
Pragmatic Design for Policy-oriented Questions
This article reports on the outcomes of the Acupuncture for Chronic Pain in the Vermont Medicaid Population trial funded by the 2016 Vermont legislature 42 in response to the opioid crisis.
The current trial was designed to be as pragmatic as possible in order to deploy limited resources to collecting Vermont-specific data regarding how a potential acupuncture reimbursement policy might be implemented and received locally and what benefits it might confer to the Vermont Medicaid population. The trial was designed after reviewing and discussing with stakeholders the legislative goals, resources, and timeline, along with a review of the existing scientific literature and consultation with several seasoned acupuncture researchers. A description of our rationale when designing the trial is described in a previously published paper. 43
Methods
We conducted a pragmatic, prospective intervention trial. A heterogeneous group of Medicaid patients with chronic pain were offered a short course of acupuncture care by a provider of their choosing from a group of 28 Vermont Licensed Acupuncturists. Care was provided in the private offices of acupuncturists in 3 of Vermont’s 14 counties: Chittenden, Washington, and Windsor. The study was funded by the Department of Vermont Health Access (DVHA) and carried out with input from DVHA, the Vermont Acupuncture Association, and a group of advisors from the Society for Acupuncture Research. Support with recruitment was also received from the University of Vermont Program for Integrative Health.
Population and Eligibility
We sought to include patients with a broad range of pain complaints in order to reflect the typical caseload that a primary care physician may encounter.
Inclusion Criteria
At least 18 years of age. Qualifying pain level on a 10-point numeric rating scale for at least 15 out of the past 30 days and for at least the past 3 months. Qualifying pain level determined via the following questions: Could you rate the intensity of your current, best, and worst pain levels over the past week on a scale from 0 to 10 where 0 is no pain, 5 is moderate pain, and 10 is the worst pain imaginable?
Pain today
Best pain this week
Worst pain this week
(Total of 3 scores must be 12 or greater in order to qualify)
Enrolled in Vermont Medicaid. Able to read and understand English. Able to understand and sign a consent form.
Exclusion Criteria
Self-reported onset of a new treatment for pain or any acupuncture treatment within the 4 weeks prior to the onset of treatment in this trial. Comorbid conditions that make treatment difficult, such as paralysis, psychosis, or schizophrenia. Relative contraindications for acupuncture, such as pregnancy, uncontrolled seizure, or bleeding disorders.
Recruitment of Patients
Patients were recruited during a 3.5-month period from mid-January to the end of April 2017. Outreach materials describing broad eligibility criteria (chronic pain, Medicaid enrollment) were distributed via a range of health-care providers and public bulletin boards. Major sources of referrals included primary care providers, nursing staff at the Vermont Chronic Care Initiative, Federally Qualified Health Centers, pain clinics, and allied health-care providers. The diversity of the referral pool increased the chances that our participants broadly reflected the population of interest. Interested parties were contacted as soon as possible by telephone. Eligibility was determined by the research staff based on the criteria below.
Consent and HIPAA release
Eligible and willing participants were met in person in order to discuss the study in detail. Research staff presented each patient with written informed consent and Health Insurance Portability and Accountability Act (HIPAA) release forms and a verbal description of the study to ensure the patient understood what was involved. If a patient was eligible and accepted the invitation to participate in the study, the consent form and HIPAA release were signed by the patient.
Intervention
Eligible patients who completed the baseline assessment were provided with a list of participating acupuncturists and allowed to schedule an appointment directly with the provider of their choice. Acupuncturists were expected to schedule an initial consultation and treatment promptly and were instructed to design a treatment plan appropriate for each patient’s needs and condition including up to 11 additional treatments for a total of up to 12 treatments within a 60-day period. Treatment strategies were based on each individual clinician’s assessment of each patient’s traditional acupuncture diagnosis and individual needs. Acupuncturists were allowed to perform whatever style of acupuncture they felt was appropriate for each patient during each treatment. In addition to manual acupuncture, treatments were permitted to include the full range of East Asian modalities within the providers’ scope of practice and training including electroacupuncture, infrared, moxibustion, manual therapy, cupping, gua sha, topical herbal liniments, and Chinese herbal medicines. Advice on diet, exercise, and rest was administered as appropriate. Patients were allowed to continue to have normal access to their primary care physician and any other usual care during the course of the study.
Recruitment of Acupuncturists
Suitable acupuncturists were identified by the Vermont Acupuncture Association from 3 regions chosen to provide geographical diversity while still allowing for efficient patient consent and data collection. Twenty-eight acupuncturists from 23 acupuncture clinics participated in the trial. Each acupuncturist was licensed by the state with the length of licensure ranging from 8 months to 21 years (mean length = 9.7 years). In order to reflect the heterogeneity and composition of the Vermont Licensed Acupuncturist workforce, acupuncturists were not restricted by experience or style of practice. All practitioners carried liability insurance and were paid a flat per visit fee. Billing records were coded to protect patient identity and included main and secondary complaint information as well as data regarding acupuncture styles, modalities used in addition to acupuncture, lifestyle counseling administered (eg, diet, exercise, self-care recommendations), and referrals made.
Baseline Assessments
All baseline instruments were completed in the presence of research staff after obtaining written informed consent and HIPAA release. Standardized validated instruments administered included PROMIS Pain Intensity Short Form (SF) 3a v.1.0, Pain Interference SF 8a v1.0, Fatigue SF 4a v1.0, Physical Function SF 8b v2.0, Sleep Disturbance SF 4a v1.0, Emotional Distress-Anxiety SF 4a v1.0, Emotional Distress-Depression SF 4a v1.0, and Social Isolation SF 4a v2.0.
In addition, an open-ended questionnaire posed the following questions:
Please list or attach a list of any doctor-prescribed medications or medications you purchased yourself (eg, Advil, Tylenol, Aleve) that you take to help manage your pain. Include the dosage and how often you have taken during the past week. Do you experience side effects from your medications? If so, please describe. Has your pain impacted your work? For example, has it affected the quality of your work or the number of hours you are able to work?
All baseline instruments were scored and responses were recorded by a research assistant.
Postintervention Assessments
All standardized instruments (ie, PROMIS questionnaires) administered at the baseline were reassessed after the completion of the last treatment. Open-ended questionnaires were readministered with the addition of the following questions:
“If you take any doctor-prescribed medications or medications you purchased yourself (eg, Advil, Tylenol, Aleve) for your pain, please list the medications, dosage, and frequency of use during the past week. Has this changed as a result of your acupuncture treatment?” “Has the quality of your work or the number of hours you are able to work changed as a result of your acupuncture treatment?” “Would you recommend acupuncture for someone else with chronic pain?” “Is there anything else you would like Vermont health-care policy makers to know about your experience with acupuncture?”
Measures were administered via an online HIPAA compliant platform. Patients who required assistance completed the measurements with the assistance of research staff during a face-to-face meeting.
PROMIS measures were scored and recorded by a research assistant and presented to the statistician. The first 3 “yes/no” questions were tallied by a research assistant. The final open-ended question responses were organized and analyzed by 2 independent research assistants. Analysis consisted of 2 steps:
Distinct patient comment strands were identified and categorized by the following themes:
Physical improvements Functional/behavioral improvements Psycho-emotional improvements Other No change Symptom aggravation Categorizations by each analyst were compared; differences were noted, discussed, and reorganized until a consensus was achieved.
Ethical Approval
The current study was approved by the Vermont Agency of Human Services Institutional Review Board, and all subjects provided signed and informed consent.
Statistical Methods
Descriptive statistics were used to characterize subjects based on the demographic and pain characteristics at the baseline. Paired t tests were used to test for temporal changes from pre- to posttreatment for all PROMIS measures in the subset of subjects with both pre- and posttreatment data. Two sample t tests were used to compare the baseline measures in subjects lost to follow-up with those who completed the posttreatment assessment. For all PROMIS instruments, raw scores were converted to t scores prior to analysis. PROMIS measure analyses were performed using SAS Statistical Software (SAS Institute, Cary, NC). Statistical significance was determined based on α = .05.
Sample Size and Study Power
For the purpose of determining sample size, the primary outcome measurement was the mean difference between the baseline and posttreatment PROMIS pain intensity score. It was estimated that the target recruitment of approximately 150 patients would result in estimated power (1 − β) = .80 using α = .05 to detect an effect sizes of d = 0.23 (Cohen’s d) on PROMIS scores assuming moderate correlation between scores (ρ = .50). Post hoc, having 113 evaluable patients with Pre and Post scores resulted in power = .80 to detect an effect sizes of d = 0.27.
Results
Recruitment and Enrollment
Totally, 211 patients were screened; 174 (82%) met eligibility requirements; 156 patients were enrolled (90% of those meeting criteria).
Characteristics of Enrolled Patients
Patient Characteristics.

Number of Treatments Completed
Number of Treatments Completed During Intervention.

Acupuncture Intervention
Acupuncture Styles Used.
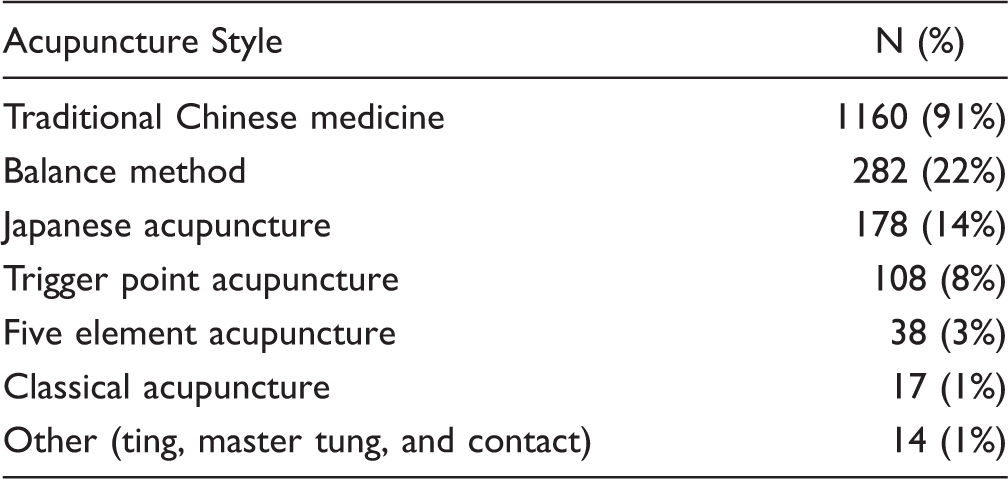
More than one style may have been used in each treatment.
Patient Outcomes
PROMIS measurements
Change in Pre- and Postintervention Mean PROMIS Scores (t Scores).

Open-ended Questionnaires
Medication use
Prior to intervention:
One hundred twelve (72%) of 156 patients reported using medications to manage their pain. Forty-eight (43%) of 112 medication users reported experiencing unwanted side effects (eg, upset stomach, nausea, drowsiness, constipation, fatigue, dry mouth, grogginess, “loopiness,” forgetfulness).
After intervention:
Forty-seven (57%) of 82 medication users who completed a posttreatment questionnaire reported a decrease in any analgesic medication use. Thirty-two percent of 47 opioid users who completed a posttreatment questionnaire reported a reduction in their opioid use.
Work status
Prior to intervention:
One hundred fifty-one (97%) of 156 patients said that their pain had negatively impacted their work.
After intervention:
Sixty-seven (59%) of 113 patients who completed the posttreatment questionnaire reported an improvement in their work capacity. Twenty-four (21%) reported no improvement in work capacity. Twenty-three (20%) not applicable—no longer working.
Patient Perceptions of Benefit
Overall, patients reported an overwhelmingly positive perception of the benefit of acupuncture care on their well-being. One hundred two patients generated 247 distinct comment strands regarding their acupuncture care via the posttreatment open-ended questionnaire. When asked, “Is there anything else you would like Vermont health-care policy makers to know about your experience with acupuncture?” Thirty-one percent of comments pertained to physical improvements (eg, pain reduction, other positive physical changes); 29% to functional/behavioral improvements (eg, improved activities of daily living, improved energy, reduced use of other medical services); 24% to psycho-emotional improvements (eg, improved sense of well-being, positive changes in emotional state, increased ability to relax, increased options and hope); 11% of comments reflected general appreciation of the care (eg, wished acupuncture could continue, felt listened to by acupuncturist); 4% of comments reflected no notable changes from acupuncture; and <1% (1 comment) reflected a flare in pain after a treatment.
When asked, “Would you recommend acupuncture to someone else with chronic pain?,” 109 of 113 patients (96%) said “yes,” 2 patients said “no,” and 2 patients said “maybe” or “with hesitation.”
Representative comments from open-ended questionnaire (selected to represent common patient comment strands):
“My acupuncture was life changing … I saw and felt and continue to feel a marked difference in my pain and mental clarity. I believe it saved my life.” “Acupuncture helped me to get my life back.” “I was very skeptical about this treatment being effective. As the weeks went by, I noticed different changes taking place in my body: my digestive system functioned much better, so my diet improved; I required less sleeping medication because my sleep was better; my pain level was much decreased; I had more genuine energy; and most especially, I had better mobility. The mobility change enabled me to walk more in fresh air and increased my good energy level. A circle of reinforcements that has made my life much better, more productive, and happier. It has cut down my need for other medical interventions like physical therapy and medications for various ailments. People have noticed the outward improvement.” “I went to a regular doctor for over 6 years and my pain only became more intense and more frequent. This is the longest I’ve gone without pain or medication in well over a year.” “This is a very necessary way to treat pain. I am very allergic to many medications, and during the study I was able to walk and do more without an allergic reaction.” “I would consider the acupuncture treatment I received to be the most effective of every treatment option I’ve ever tried in my life at reducing my pain and increasing my quality of life, as well as the quickest in producing results. I was able to stop taking all my pain medications while receiving acupuncture and was even able to try a few physical activities (such as yoga) that have caused me pain in the past. I only wish I could continue to receive acupuncture as I believe it’s the one treatment with results that would allow me to work full time … if I was able to continue treatments if/when my pain flared up again.” “I literally went in there day one thinking it was quack science and now I desperately miss it.” “Gained 2 hours of sleep a night from the acupuncture because it helped me relax. 100% would recommend to anybody with pain.” “I have received acupuncture before but it was the consistent treatments that I felt a shift happen in my healing process.” “It has somewhat improved my quality of life. It has significantly reduced the frequency of migraine headaches and helped to reduce arthritis pain in my neck and shoulders. Was not effective for osteoporosis back pain or peripheral neuropathy in hands and feet pain.” “Makes huge difference in well-being, physical, and mental. Helps with pain, sleep, cognition.” “If it had been covered, I may not of gotten [sic] so many scripts of narcotics and gotten addicted to opiates.”
Discussion
We designed this study with the goal of answering questions of interest to policy makers. Utilizing a pragmatic design, we were able to treat patients with a wide range of chronic pain conditions and multiple comorbidities. These complex patients are commonly seen in doctors’ offices but often screened out of efficacy trials in order to increase internal validity. Likewise, we provided care using the existing workforce of Licensed Acupuncturists, allowing them to treat patients using their own judgment in their own office settings, whereas less pragmatic trials often utilize uniform treatment protocols and are delivered by a small group of providers in a centralized setting. A strength of this study, therefore, is the more direct transferability of our findings to real-world people and settings. Our results represent a reasonable representation of what would likely occur if acupuncture services were widely accessible to Vermont patients receiving Medicaid benefits.
Some data suggest that acupuncture is acceptable to Medicaid users; 46 however, data regarding the use of acupuncture for this specific population are relatively scant. It is notable that our results demonstrate a high engagement with treatment from these patients: 72% of our patients received 6 treatments or more. This suggests that despite challenges related to schedules, transportation, and unfamiliarity with the therapy, these patients were motivated to incorporate acupuncture into their lives in a committed manner.
We achieved our targeted patient recruitment in less than 4 months. This indicates a significant demand for acupuncture from both patients and physicians when acupuncture is financially accessible. This comports with survey data that tell us that insurance coverage plays a bigger role in predicting patient decision-making regarding the use of acupuncture than does effectiveness or safety. 44
Also notable is the breadth of impact that the intervention had across a range of biopsychosocial outcomes. The effectiveness we documented extended beyond reductions in pain intensity to include improvements in functional, social, and psychological outcomes. The National Pain Strategy stresses the importance of treating chronic pain with therapies and approaches that work across the biopsychosocial spectrum. 47
Finally, in the context of the opioid crisis, it should be pointed out that no serious adverse events were reported during the study. Over twenty years ago, the NIH consensus conference on acupuncture noted that “One of the advantages of acupuncture is that the incidence of adverse effects is substantially lower than that of many drugs or other accepted medical procedures used for the same conditions.” 48 This statement rings truer today than ever. The opioid crisis has reminded us of the value of placing safety near the top of our list of evaluative criteria when assessing effective treatment options. The safety record of acupuncture has been well documented and is very favorable.49–51
Limitations
We did not include a placebo or sham acupuncture comparison group; consequently, we are unable to conclude that the changes we observed in our patients were due to acupuncture specifically. It is possible, for example, that the changes were influenced by the natural course of disease, regression to the mean, or some other uncontrolled variable. It is also possible that patients who entered our study hold attitudes or beliefs that predisposed them to favorable outcomes. However, a large body of high-quality randomized controlled trials has demonstrated that acupuncture is effective for chronic pain when these variables are controlled for.15–35 Although we observed significant changes in a chronic condition over a short course of 60 days, this study does not provide data regarding the long-term effects of acupuncture on our patients. However, a meta-analysis of patients with chronic pain suggests that approximately 90% of the benefit of acupuncture would be sustained at 12 months. 52
Conclusion
In this study, providing acupuncture care for patients with chronic pain was feasible and well received in the Vermont Medicaid population. Receiving care from licensed acupuncturists was associated with significant improvements in physical, functional, psycho-emotional, and occupational outcomes compared with before receiving acupuncture treatments. Our findings provide evidence that Medicaid patients with chronic pain who are provided access to acupuncture care are likely to benefit from such care. We believe that these results, when considered in context with significant high-quality safety, efficacy, and cost-effectiveness data from other randomized controlled trials, are sufficient to warrant coverage of acupuncture for Medicaid patients with chronic pain.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mr Davis reports subcontracting fees from the State of Vermont Agency of Human Services during the conduct of the study. Mr Badger, Ms Valentine, and Mr Cavert report subcontracting fees from Acupuncture Vermont during the conduct of the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Agency of Human Services—Department of Vermont Health Access (DVHA).