
Abstract
Objectives
The aim of this article is to study patient satisfaction with complementary and alternative medicine (CAM) in an in-hospital setting before and after the introduction of diagnosis-related groups (DRGs).
Methods
Patients were interviewed regarding a general evaluation of their hospital stay, the psychological talking therapy, the nutrition therapy, and the overall success of the treatment.
Results
The medical treatment was evaluated by 1158 patients. A very good success was reported by 347, a good by 609, a moderate by 181, and none by 21 patients. DRG implementation showed no significant effects. Psychological talking therapy was evaluated as “very good” (P ≤ .05). With regard to the success of the medical talking and nutrition therapy, there were no significant differences (P ≥ .05) between the time before and after DRG implementation.
Conclusion
Broadening conventional medical treatment with CAM practices can lead to a parallel treatment of DRGs in hospitals working with complementary medicine. This results in very patient-centered therapies, which may impact patient satisfaction.
Keywords
Introduction
Diagnosis-related groups (DRGs) are medico-economic patient classification system that assign patients into an appropriate case group according to their diagnose(s). The DRG system originated in the 1970s. The intention was to classify patients regarding similarities to better standardize patient management and treatment. 1 Nowadays, the classification is also used for remuneration purposes.
General Assessment of Hospital Stays in the 2 Periods.

Nevertheless, the intended reduction in costs by using DRGs and the related effects on the quality of care are increasingly discussed,8,9 especially since DRGs can have adverse effects by reducing the quality of care. 10 Moreover, negative effects on the health status of the patients were recorded due to the reduced length of the stay. 11 In this context, an increase in the readmission rates in hospitals is also reported. 12 A closely related problem is the danger of patient selection, that is, that patients with “low-cost” diagnoses or those whose treatment results in the most profit13,14 might be treated preferentially. A further problem is that the costs for care-intensive patients are often not sufficiently covered by DRGs. 15 However, the studies referred to above were conducted in hospitals using DRGs for purely conventional academic medicine. So far, the regulatory influences of DRGs for hospitals that include complementary and alternative medicine (CAM) were not examined. CAM therapies include (but are not limited to) nutrition therapy, hydrotherapy/thermotherapy, other physical methods, phytotherapy, lifestyle-regulative therapy, exercise therapy, detoxification procedures, and additional procedures (manual therapy, acupuncture/Chinese medicine, homoeopathy, neural therapy, plus art therapy [art and music therapy]). When conventional medical in-hospital procedures are broadened to a holistically orientated patient care, studies show positive effects on the quality outcomes.16–20 Yet these studies refer to condition without DRGs.
This article therefore aims to help close the resulting research gap by investigating patient satisfaction levels before and after DRG introduction in a German hospital offering CAM as a supplement to standard academic medical treatment. Regarding effects, we focus on patient satisfaction by comparing the results of in-house investigations of patient satisfaction before and after the introduction of DRGs. All patients had acute exacerbations of chronic diseases.
In-hospital CAM Treatment in Germany
The integration of complementary therapy practices in conventional medicine has gained significance in recent years.21–23 Efforts to integrate CAM-therapies into the publicly funded health-care system are also increasing.24–27 In Germany, according to § 2 art. 1 p. 2 of the German Social Law, Fifth Book (SGB V), the treatment methods, medications, and remedies of “special therapies” are “not excluded” from the scope of the health insurance. This means that complementary medicine procedures can also be provided and remunerated. As part of inpatient hospital care in Germany, attempts are being made to use complex therapy to ensure interdisciplinary and integrative treatment and a holistic approach of mostly multimorbid patients with acute states of chronic diseases.
This kind of regulatory therapy requires serial applications and frequent interventions, which both result in a prolonged hospital stay. 28 As treatment of acute conditions in chronically ill patients is also a main area of medical activity, the treatment is additionally directed at improving (or “dechronifying”) the complaints. Especially in the case of patients with comorbidities, an individually determined integrative therapy concept is necessary due to the complexity of the overall clinical picture. However, this goes hand in hand with high resource consumption. Major cost issues are the requirements of the interdisciplinary team composition and the wide array of therapeutic areas to be covered. Simultaneous acute medical diagnosis and therapy must be ensured and coded separately (OPS 2014). 29 Therefore, hospitals combining academic medicine and CAM need to adopt a more case management-related perspective as the particular situation of patients who can be considered for complex therapies comprises an extremely high degree of suffering in combination with occasional considerable symptoms of pain, a longstanding history of chronic illness with a continuous acute worsening of complaints and an ineffectiveness of various typical ambulatory and inpatient treatments.
Materials and Methods
As mentioned above, to our knowledge, no study has so far investigated the effect of the implementation of the DRG system on patient satisfaction in hospitals with CAM therapies. The study reported here does that by comparing patient satisfaction levels before and after DRG implementation in a specialized hospital focusing on internal medicine and specialized in holistic medical treatment, that is, the combination of classical medical approaches and CAM therapies. From 2004 to 2006, the hospital did not use DRGs due to specific legislation (§17b art.1, clause 15 of the Hospitals Financing Law [KHG]). (Certain facilities could be exempted from the lump sum remuneration system for a limited period (2004–2006) in case their activities were not appropriately compensated by the DRG system, for example, because a higher number of severely ill patients were treated than in an average hospital.) In 2007, the DRG system was implemented. Consequently, a comparison of satisfaction levels with and without use of DRGs is possible, creating 2 independent samples.
Comparability is granted as the same method of data collection was employed, plus patient groups and the treatment specifications remained very similar. All patients were suffering from a chronic condition, an acute deterioration of their health status and were facing complex psycho-social issues. Included among the diagnoses of the patients surveyed were for example migraines, neuralgia, irritable bowel syndrome with diarrhea, diseases and disorders of the musculoskeletal system, 26 tinnitus, Parkinson’s disease, severe infections of the respiratory tract and the urogenital system, ulcerative dermatitis, and so on. Due to the complexity of most cases, one patient may have had to be grouped into several DRGs, all of which had to be treated simultaneously and holistically.
All data were gathered using an optional, anonymous approach. The data presented are based on a patient survey with over 5000 participants that lasted for a period of over 5 years (2004–2008). All patients were given a paper-and-pencil questionnaire upon their discharge that asked about their satisfaction with the hospital stay with a specific focus on complementary medicine, the overall success of the medical treatment, the satisfaction with and the perceived effects of the psychotherapeutic treatment (talking therapy), and the medical nutrition therapy. The focus was put on talking and medical nutrition therapy as they (a) form 2 pillars of CAM approaches and (b) were received by all patients. The questionnaires were handed in anonymously by the patients.
Approval from an institutional review board or patients written informed consent were not necessary because the data were collected for administrative purposes and no respondent can be personally identified. The information regarding demographics was derived from administrative databases and cannot be linked to individual satisfaction levels. All data on outcomes are patient-reported. “Patient-reported outcome (PRO) is an umbrella term referring to questionnaires, interviews and other related methods of assessing health, illness and benefits of healthcare interventions from the patient’s perspective.” 30
For all questions, the same scaling was used: 1 (very good), 2 (good), 3 (satisfactory), 4 (acceptable), 5 (poor), and 6 (insufficient), following the German school grading system. The patients had to rate their satisfaction with and the results they felt were obtained by the interventions they received. In this article, we present the overall ratings and then focus on talking therapy and medical nutrition therapy.
The statistical evaluations were done using SPSS Version 19.0 (SPSS Inc, USA). The Mann–Whitney U test was used to compare the 2 independent, not normally distributed random samples. The chi-square test was used for examining nominal variables, and the chi-square independence test was used to test the interdependence of nominal variables. Using the 1-sided test (chi-square Pearson), we examined whether a positive or negative connection existed, and then the 2-sided test (chi-square Pearson) for in-depth analysis in case there was a relation. In the 1-sided test, the alternative hypothesis is not tested so that the probability of error is always lower. Furthermore, the 2-sided significance was tested. The significance level was set at 5%.
Results
In this section, the aggregated patient-reported outcomes are presented. First of all, the general assessment of the hospital stay is described, then specific treatments and the rating of the overall success.
General Assessment of the Hospital Stay
In both time periods, (a) 2004–2006 and (b) 2007–2008, the stay was evaluated as very good by the majority of the respondents (Figure 1). Overall, there were no significant differences (Mann–Whitney U test, P ≥ .05; Table 1) when comparing the 2 time periods (with and without DRG).
General Assessment of Hospital Stays in the 2 Periods.
Assessment of the Psychological Talking Therapy
In total, 496 patients evaluated the psychological talking therapy. Overall, the procedures of psychological therapy in both periods were evaluated as “very good” (Figure 2, Table 2). However, a significant difference in both time periods can be seen (Mann–Whitney U test, asymptotic significance [2-sided], P ≤ .05).
Assessment of Talking Therapy in the 2 Periods. Assessment of Talking Therapy in the 2 Periods.

Assessment of the Overall Effects of the Psychological Talking Therapy
The assessment of the overall effects of the psychological talking therapy was done by a total of 643 patients (Figure 3, Table 3). A very good result was reported by 247, a good result by 297, a moderate by 75, and no success was reported by 24 patients. A comparison of ratings before and after DRG introduction showed no significant difference (Pearson chi-squared, asymptotic significance [2-sided, P ≥ .05]).
Total Results—Psychological Talking Therapy in the 2 Periods. Total Success—Psychological Talking Therapy in the 2 Periods.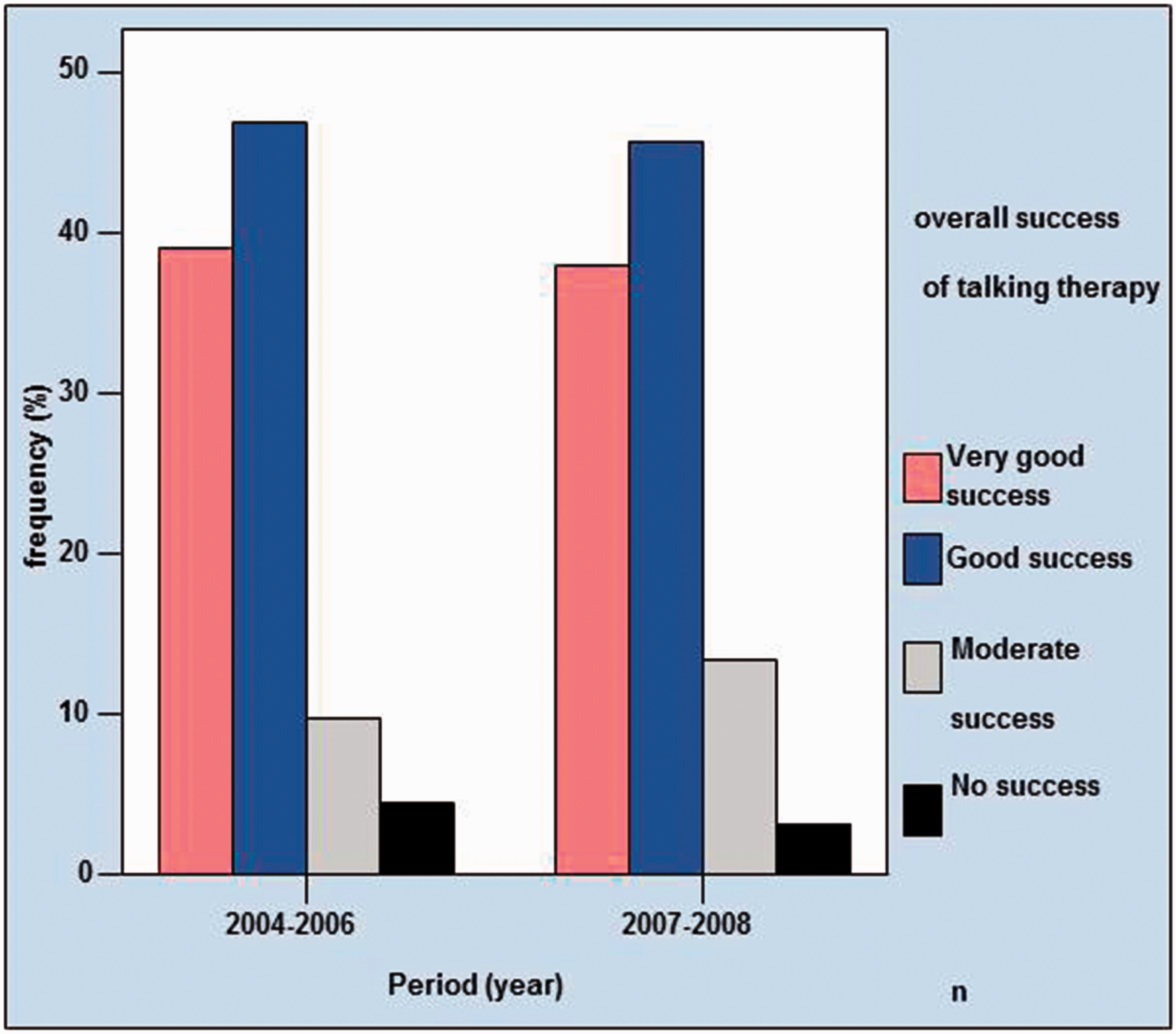

Assessment of Overall Success of the Medical Treatment
Total Success—Medical Treatment in the 2 Periods.


Total Success—Medical Treatment in the 2 Periods.
Assessment of Overall Success of the Medical Nutrition Therapy
The assessment of the overall success of the medical nutrition therapy was completed by 560 patients in both time periods (Figure 5, Table 5). Of these, 178 patients reported a very good success rate, 258 rated it a good success, 94 found it moderately successful, and 30 thought it was not successful. A comparison of the responses of those with and those without case-based compensation showed no significant difference (Pearson chi-squared, asymptotic significance [2-sided, P = .459]).
Total Success—Medical Nutrition Therapy in the 2 periods. Total Success—Medical Nutrition Therapy in the 2 Periods.

Discussion and Conclusion
DRGs are discussed in the context of the influence on costs and quality. 31 Suspected impacts on the quality of the services provided have not been confirmed yet. 32 When conventional medical in-hospital procedures are broadened to a holistically orientated patient care, studies show positive effects on the quality outcomes16–20 for conditions without DRGs. Whether these effects can be reached in a DRG context was focus of the present study. We used patient-reported satisfaction levels regarding their hospital stay and the (CAM) therapies received.
The results of the study show that before and after the introduction of the DRG system, the overall satisfaction levels and those for the CAM treatments were very positive. After the implementation of DRGs, even more positive results tended to be obtained. This may be due to an active focus of the personnel not to reduce quality or to the patient-centered nature of holistic interventions themselves. In CAM treatments, it is of great medical and social importance that the patients are actively included in the therapeutic process and thereby learn to manage their illness independently. In this way, the patients can regain a certain degree of self-competence. This sensitive process requires time and contributes to a longer period of hospitalization for the patient, 26 which can also lead to a higher success and thus satisfaction.
Although potential confounders were limited by having very similar patient groups (and needs) as the hospital is very specialized, we cannot exclude high satisfaction levels are due to the type of conditions treated. Data from other chronic diseases research33,20 suggest that satisfaction levels are very high simply because of the fact of receiving help and thus feeling relieved. Therefore, further studies are necessary in order to evaluate CAM treatment regarding quality of outcome. Nevertheless, since most health systems allowing for case-based approaches, the integration of CAM, and so on, are based on some type of DRG accounting model, real experimental conditions will be very hard to achieve. In particular, the indication-based analysis of holistic complementary medicine provision of services on patient satisfaction could thus be the object of further research projects. This would aid drawing conclusions regarding the generalizability of the results.
Also, the view of the medical personnel should be included, which was not done here. This could clarify whether the staff changed the treatment after the implementation of DRGs or not. Moreover, cost effects were not presented here but are reported elsewhere.34,35 Also, studies are required investigating whether the individualized treatment of patients is the main driver of patient satisfaction, irrespective of the accounting system used.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.