
Abstract
This study employs an integrated discourse-analytic approach, synergizing semantic macro-analysis with the
Plain Language Summary
This study analyzes personal stories about depression shared on the Chinese platform Zhihu. We examine how individuals understand and come to terms with their condition. Our findings show a three-stage process of making sense of depression. Initially, people doubt their diagnosis, feeling insecure and uncertain. Next, they often enter a phase of denial, marked by harsh self-judgment and resistance to the illness label. Finally, some reach a stage of acceptance, where they begin to see depression as a manageable condition and focus on constructive coping. We explore the challenges and turning points in this journey. The insights gained can help design more sensitive and effective support for people with depression in China.
Introduction
Depression is a prevalent global mental health challenge, affecting approximately 280 million adults worldwide (J. Li et al., 2023). In China, the scale of the issue is substantial and growing: around 41 million people were affected in 2019, representing an increase of over 30% since 1990 (Qiu & Li, 2023). Beyond its clinical dimensions, depression is associated with a range of adverse life experiences, including loneliness, diminished self-esteem, educational and occupational dissatisfaction and elevated risk of substance abuse (Avenevoli et al., 2015; Grob et al., 2020). Compounding these challenges, many individuals experience profound social seclusion and psychological distress due to their inability to articulate or make sense of their condition (Kotliar, 2016). In this context, the process of sense-making, constructing a coherent understanding of one’s illness, has been recognized as a critical mechanism whereby individuals reclaim agency and exert control (Sharf & Vanderford, 2003; Xu & Li, 2023).
The emergence of social networking platforms has opened new avenues for such sense-making. Through sharing their experiences online, individuals with depression transcend traditional barriers to communication, connect with peers, exchange social support, build online communities and break out of seclusion (J. Wang et al., 2023). These digital spaces also provide unique opportunities for users to corroborate and refine their own narratives, thereby facilitating collective and individual meaning-making (Kotliar, 2016). Moreover, the relative anonymity and accessibility of online environments often enable more candid, detailed disclosures of lived experience (Hookway, 2008), offering researchers a valuable lens through which to understand patient perspectives and to improve care practices.
Despite the development, significant gaps persist in the current scholarly literature. Existing research on sense-making in depression remains predominantly situated within Western socio-cultural contexts, limiting its applicability to non-Western settings where conceptions of mental health and illness may differ. While a small but growing body of scholarship has begun to explore depression in China, most studies focus on individuals who have successfully developed explanatory frameworks for their suffering (e.g., X. Li & Xu, 2023; Tang et al., 2021). Little attention has been paid to those who continue to struggle to make sense of their condition, a notable omission, given that the meanings attached to mental illnesses are profoundly shaped by cultural and social norms (Gary, 2005). This gap is particularly salient in the Chinese context, wherein traditional values and modern biomedical frameworks often coexist in tension.
To fill these gaps, this study sets out to investigate the online depression narratives on Zhihu, China’s most popular community question-answering (CQA) site, by asking the following research question: How do individuals with depression in China struggle to make sense of and legitimize their experiences, and what are the emotional patterns associated with this sense-making process? Methodologically, the present study adopts an integrated discourse-analytical approach that synergizes van Dijk’s (2009) semantic macro-analysis with the
Depression, Mental Illness and China
Depression is a common mental disorder that significantly affects both patients’ mental and physical health. Its symptoms can range from psychological manifestations such as a persistent bad mood, pessimistic attitude and lack of passion or vitality to physical symptoms like sleep disturbances, appetite loss and a high risk of suicide (Cui, 2015; Dong et al., 2018). Its introduction into China as a Western psychiatric construct, absent from the local medical and popular lexicon until the late 20th century (Karchmer, 2013), has inevitably engendered a complex interplay with indigenous cultural understandings of health and illness.
One prominent illustration of this cultural dissonance is the pronounced tendency to somatization among Chinese patients. Empirical studies have consistently shown that, compared to Western counterparts, Chinese individuals are more inclined to emphasize physical rather than emotional symptoms when seeking professional help (Kirmayer & Young, 1998; Kleinman, 1982; Xie et al., 2016). In one study of 72 depressed patients in general medical settings, Ren et al. (2001) find that 77.8% present primarily with physical discomfort and sleep problems, with chronic pain being the most frequently reported complaint (30.6%). Similarly, Zhang et al. (2010) showcase that among 736 depressed patients in general hospitals, 98.2% complain of physical symptoms, with a striking 69% presenting somatic issues as their only chief complaint, and 11% explicitly denying any psychological difficulties. This widespread phenomenon of somatization is deeply embedded in cultural and medical traditions. Scholars such as Ramsay (2008), Parker et al. (2001), and X. Wang and Lv (2010) have highlighted the formative influence of Traditional Chinese Medicine (TCM), whose holistic approach does not posit a strict division between mind and body. Within this worldview, emotional distress is naturally understood and expressed through the idiom of physical ailment, leading to a distinctive clinical presentation that differs from Western diagnostic expectations.
Another profound manifestation of this cultural clash is the intense and pervasive stigmatization of depression in Chinese society, which is deeply rooted in cultural and moral interpretations of mental distress. Empirical studies consistently record prevalent stigmatizing attitudes among the public. A community survey conducted by F. Yang et al. (2020) among 1,697 residents in Central China reveals high levels of stigma, with 53.0% of respondents endorsing personal stigma and 83.4% perceiving stigma in community. Notably, the most strongly endorsed belief is that “People with depression could snap out of it if they wanted,” underscoring the perception of the condition as a matter of willpower. Similarly, a survey by Wen et al. (2017) of 207 Guangzhou citizens find that 57.5% view depression a sign of personal weakness. This moralization of depression is further reflected in public discourse. Analyses of social media content (e.g., J. Li et al., 2023; Peng & Ding, 2024; W. Wang & Liu, 2016) show that individuals with depression are frequently labeled as pretentious, overthinking and weak. Critically, such societal prejudice is often internalized by sufferers, leading to debilitating self-stigma. A survey by Liang and Zhang (2023) of 330 patients with mental disorders, including depression, reveal that 43.1% of respondents report severe levels of self-stigma. The theoretical underpinnings of this heightened stigmatization frequently point to the interplay of Confucian ethics and collectivist culture. Kuo and Kavanagh (1994) theorize that in the Confucian paradigm, mental illness is interpreted as a failure of moral self-cultivation and an inability to fulfill one’s social roles. Furthermore, Lam et al. (2010) argue that within collectivist cultures, the stigma of mental illness is not confined to the individual but extends to the family, damaging its collective honor and social standing. It is crucial to note, nonetheless, that although collectivism provides a fertile ground for stigma, its specific expression varies. In the Chinese context, stigma is often channeled through a sociomoral framework (L. H. Yang et al., 2007), where mental distress is judged as a failure to meet societal, ethical expectations. This contrasts with the conceptualizations found in some African collectivist societies, where explanations for depression and similar distress may be more directly linked to spiritual or supernatural causes (Agyei et al., 2024; Opare-Henaku & Utsey, 2017). This underscores that the unique manifestation of stigma in China arises from the interplay of its collectivist social organization with its indigenous Confucian moral philosophy.
In contemporary healthcare, mental illness is primarily defined through a Western biomedical model that emphasizes genetic abnormalities, neurochemical imbalances, and pharmacological interventions (Deacon, 2013). However, as Chang (2018) reminds us, the etiology, experience, and meaning of illness are fundamentally shaped by social and cultural contexts. Research examining how patients in non-Western societies make sense of depression is therefore crucial, as it illuminates the complex processes through which imported diagnostic concepts are interpreted within specific cultural frameworks, particularly when they conflict with traditional beliefs. Such studies provide valuable insights which can help healthcare professionals transcend what Kleinman (1989, p. 9) terms the “iron cage” of reductive medicine – the tendency to reduce complex human experiences into standardized, impersonal categories, and move toward more culturally responsive forms of care.
Illness Narratives, Online Illness Narratives, and Depression Narratives
The concept of illness narratives, first coined by Kleinman (1989), refers to the stories that patients construct to give form and meaning to their experiences of suffering. These narratives serve as crucial linguistic devices through which individuals attempt to make sense of their illness subjectively and intersubjectively, revealing how they interpret their situation within broader cultural frameworks (Burchardt, 2019). Scholarship has consistently demonstrated the potential therapeutic value of such narrative practices, with studies highlighting its role in facilitating sense-making, restoring personal agency, and supporting identity reconstruction among patients facing health challenges (Beck, 2005; Sharf & Vanderford, 2003). As Sunwolf and Keranen (2005) demonstrate, the process of narrating illness facilitates social connection, enables reflective meaning-making, and imposes order on otherwise fragmentary and confusing experiences.
The digital turn has profoundly transformed the scope and social role of illness narratives. With the proliferation of social networking platforms, people with chronic conditions such as depression have increasingly turned to online spaces to share their experiences (J. Li et al., 2023). This shift has amplified the functions of illness storytelling. Research illustrates that online illness narratives facilitate a distinctive social dynamic, enabling a transition from deep, interpersonal connection to broad, community-based solidarity. For example, analyses of platforms like Weibo in China display how online illness narratives allow individuals with depression to form communities of coexistence, in which patients often evolve from seeking support to providing it, thereby establishing self-sustaining cycles of mutual aid and collective resilience (Yan & Liu, 2022). Beyond fostering social support, these narratives provide spaces for collaborative sense-making. Kotliar’s (2016) analysis of depression blogs illustrates how they enable individuals to corroborate each other’s experiences, a process vital for constructing coherent personal and shared understandings of illness. This co-creation of meaning is further evidenced in Gao and Chen’s (2024) study of illness narratives on Douban. Their findings reveal that through articulating illness and pain, patients not only forge social connections but also actively challenge stigmatizing narratives, collaboratively building alternative and empowering understandings of depression.
The unique affordances of digital platforms, particularly their relative anonymity and expanded communicative space, enable a candor in illness narration often difficult to accomplish in offline contexts (Hookway, 2008). Patients frequently share negative experiences and intimate details with unprecedented openness, creating rich naturalistic data for researchers seeking to understand lived illness experiences. This is exemplified in Xu and Li’s (2023) analysis of 160 depression narratives from Douban, which reveals that Chinese users predominantly make sense of their depression through sociocultural explanations (including parental pressure, academic stress, and bullying experiences) rather than biological frameworks. This distinct pattern of meaning-making, contrasting with Western narrative tendencies, has direct implications for mental health policy and intervention design, leading the researchers to propose concrete recommendations to China’s CDC regarding social support infrastructure. Together, these studies establish online illness narratives as a significant cultural phenomenon and a valuable resource for developing more responsive, culturally-attuned mental health care approaches.
Methodology
Research Design
This study employs a qualitative research design grounded in discourse analysis. This approach is selected because our primary aim is to explore the subjective, meaning-making processes of individuals living with depression. Discourse analysis is uniquely suited to this goal, as it treats language as a form of social practice that reveals how people construct identities, emotions, and understandings of their experiences through narrative (Potter & Wetherell, 1987). Unlike quantitative methods that seek statistical generalizability, this qualitative design allows us to capture the rich, contextual, and nuanced complexities of how individuals interpret their illness.
To this end, we adopt an integrated analytical approach that combines van Dijk’s semantic macro-analysis with
Data Collection
The present study is situated in China’s distinctive social media ecosystem. In contrast to the globalized platforms prevalent elsewhere, China’s landscape is predominated by indigenous platforms such as Weibo (a microblogging hybrid of X and Facebook) and Douyin (the domestic version of TikTok). These are not mere functional substitutes but have evolved into specific spaces that actively reflect and shape social dynamics, youth culture, and patterns of information exchange in contemporary Chinese society.
Within this ecosystem, we select Zhihu – China’s foremost community question-answering (CQA) platform, as our research site. This choice is strategic because Zhihu constitutes a unique digital space characterized by several salient features. The platform supports relative anonymity, which encourages discussion of sensitive and stigmatized topics like depression. Its community-driven, algorithmically mediated structure further facilitates the formation of affinity spaces, where individuals with shared experiences congregate to exchange stories and provide mutual support. These dynamics are central to the sense-making processes under investigation.
Our analysis focuses specifically on the question thread: “Having been diagnosed with depressive disorder, yet I always feel like I’m faking it. What should I do?” This query is chosen because its very formulation, centered on doubt and legitimacy, proves effective in eliciting rich, personal accounts of individuals struggling to make sense of their depressive experiences. The question’s substantial traction (2.91 million views and 753 responses by January 1st, 2025) confirms its profound resonance among Chinese depression sufferers, making it an ideal locus for investigating the struggles involved in illness-related sense-making.
All responses to this question are collected using a custom Python script. We then implement a rigorous selection process focusing specifically on first-person narratives detailing personal struggles with interpreting depressive experiences. To further ensure the cultural and contextual relevance of the dataset, we examine user profiles where available, prioritizing those with location data in China or predominant use of Chinese language. This process results in a curated dataset of 200 posts for qualitative analysis.
Analytical Procedures
Following data collection, we engage in a systematic analytical process using van Dijk’s (2009) semantic macro-analysis to identify and refine key thematic patterns within the data. The analysis begins with an immersive reading of all posts to establish familiarity with the content and context of the narratives. We then implement a structured coding approach, starting with open coding to identify emergent concepts and progressing to axial coding to establish relational patterns among these categories. Throughout this process, we maintain a constant comparative method, moving between raw data, initial codes, and developing thematic structures. This iterative approach ensures all themes remained empirically grounded while achieving progressive analytical coherence.
Our analytical focus specifically investigates whether patients have established a coherent illness definition, with particular attention to contextual factors facilitating or hindering this sense-making process. Through classification, we code the presence or absence of coherent illness definitions as primary themes, while treating associated challenges and enabling conditions as corresponding sub-themes. To ensure analytical rigor, we implement a reliability procedure involving independent co-coding of 30% of the dataset by two authors. Initial inter-coder agreement exceeds the recommended 85% threshold for qualitative research, with all discrepancies resolved through deliberative discussion until full consensus is achieved.
Building upon the established thematic analysis, this study further employs the attitude system (see Figure 1) from Martin and White’s (2005)

Analysis framework for attitude
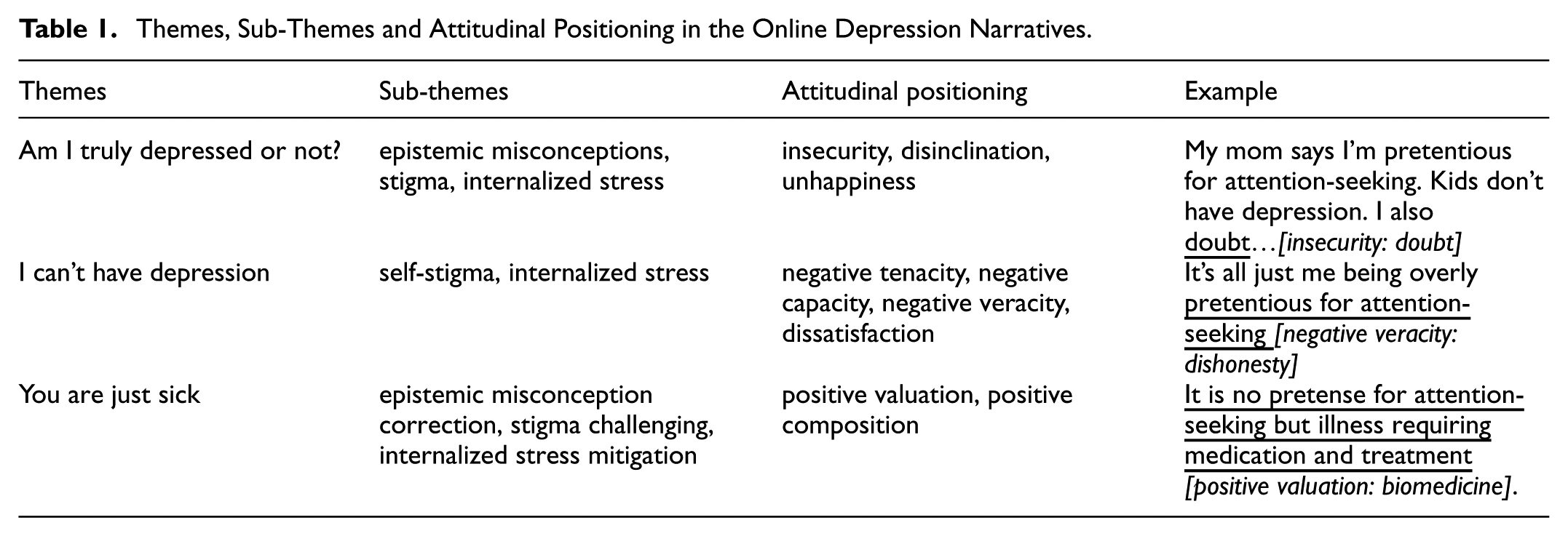
Through this integrated analytical approach, we identify three principal themes regarding patients’ illness sense-making: (a) Am I truly depressed or not; (b) I can’t have depression; and (c) You are just sick. Each theme encompasses two to three subthemes that further elaborate its dimensions. Furthermore, our analysis reveals nine attitudinal resources embedded in these narratives. For a complete overview of themes, subthemes and attitudinal patterns, please see Table 1. This multidimensional examination offers nuanced understanding of how patients subjectively experience depression, particularly illuminating emergent illness identity states and associated emotional patterns within specific socio-discursive contexts.
Themes, Sub-Themes and Attitudinal Positioning in the Online Depression Narratives.
Analysis
Am I Truly Depressed or Not?
A prominent theme emerging from the online depression narratives on Zhihu captures the initial phase of illness interpretation where individuals question whether they truly have depression. This thematic pattern consistently manifests three negative emotions, insecurity, disinclination, and unhappiness, with insecurity emerging as particularly central in reflecting a fragile, wavering illness identity. Typically arising during early stages of depression when mental distress or mild physical symptoms first appear, this theme showcases how epistemic misconceptions about depression, exposure to public stigma, and internalized pressures collectively trigger emotional responses that obstruct coherent illness identity formation.
Epistemic Misconceptions
Epistemic misconceptions – misunderstandings regarding the symptoms and diagnostic method of depression, constitute as a primary source of illness-related insecurity among individuals with depression on Zhihu. This insecurity manifests as a persistent doubt about the validity of one’s condition, even in the presence of a formal diagnosis. These misconceptions are not merely gaps in medical knowledge but are deeply embedded in culturally constructed notions of disease in China (Gary, 2005), which often equate real illness with visible, severe dysfunction or objectively verifiable physiological evidence. This cultural script imposes a restrictive framework for legitimizing suffering.
A168 exemplifies a prevalent symptom-related misconception characterized by an all-or-nothing pattern. She internalizes the belief that depression is valid only when it results in complete functional incapacitation, a notion stands in sharp contrast to the spectrum-based model of symptoms defined by Western biomedicine (Deacon, 2013). When A168 measures her experience against this demanding cultural definition, she becomes trapped in self-doubt, despite her clinical diagnosis. This legitimacy doubt, a direct consequence of the misalignment between personal experience and the culturally sanctioned script, not only prevents her from accepting the diagnosis and forming a coherent illness identity but initiates a prolonged period of psychological distress rooted in this unresolved uncertainty.
Clearly, I can still live a normal life without any difficulties to eat, learn or sleep even though diagnosed with depressive disorder. So, I begin to
A149’s narrative reveals a diagnosis-related misconception. She operates under the conviction that a real disease must be verifiable through objective instruments such as CT scan or thermometer, a belief aligned with a cultural system that grants authority to visually or technologically mediated evidence. The reliance on subjective self-report scales for diagnosing depression directly conflicts with this deeply held scientific model. Consequently, A149 questions the legitimacy of her diagnosis, agonizing over whether she might have deliberately selected the bad options. Her insecurity transcends mere medical uncertainty; it reflects a deeper epistemological crisis wherein the subjective nature of psychiatric assessment challenges not only her self-understanding but also the culturally ingrained foundations of how disease is recognized, authorized. This tension highlights the complex negotiation between modern psychiatric standards and deeply rooted, localized health epistemologies in China.
From cancer, colds to fever, they are all diseases that can be diagnosed via a CT machine or thermometer. If you have it, then you have it. Nonetheless, when it comes to depressive disorder, its diagnosis is entirely based on a scale, without taking a blood draw or CT scan. In my opinion, it’s too unreliable.
Stigma
Stigma, understood as a discrediting attribute which marks and degrades an individual, distinguishing them from complete and normal members of society (Link & Phelan, 2001), constitutes a significant source of insecurity among individuals with depression on Zhihu. Nonetheless, the manifestation of stigma here differs notably from Western context. While Western stigma often centers on perceptions of danger or incompetence (P. W. Corrigan et al., 2005; Pirkis et al., 2006; Romer & Bock, 2008), the Chinese one tends to take the distinct form of moral judgment, embodied in accusations like overthinking and pretentious for attention-seeking. This moralized stigma inflicts a harm that extends beyond social devaluation to a profound undermining of an individual’s trust in their own experience.
The cases of A45 and A81 illustrate this. Both individuals develop recognizable depressive symptoms, with A45 progressing to medication use. Yet when they attempt to articulate their suffering, their accounts are discredited and reinterpreted through a moral lens that frames their conditions as character flaws rather than medical realities. This repeated invalidation leads them to gradually question the authenticity of their own depressive experiences. Herein lies the profound harm of this moralized stigma: victims become unreliable narrators of their existence, their connection to reality and selfhood shaken. The path to recovery is thus blocked not by fear of external discrimination, but by a prior, catastrophic collapse in patient’s confidence in their reality. Addressing this crisis of self-trust is, therefore, a necessary precondition for any meaningful healing to begin.
My mother keeps telling me I am overthinking, that it is only in my head … But it only makes me
My mom says I’m pretentious for attention-seeking. Kids don’t have depression. I also
Internalized Stress
Internalized stress represents the accumulated physiological and psychological burden that results from absorbing dominant socio-cultural pressures without effective means of processing or release. Specifically, in these Zhihu narratives, such stress frequently manifests as internalized upward mobility pressure, a potent fusion of neoliberal values emphasizing relentless self-optimization and Confucian ethics prioritizing familial duty and social role fulfillment (Hsiao, 2020). This internalized stress constitutes another potent source of insecurity among depressed individuals on the platform.
In comparison with epistemic misconceptions or stigmas which directly challenge illness legitimacy, internalized stress operates through a more insidious mechanism. As patients demonstrate considerable effort in concealing their conditions to meet societal expectation, this very ability to maintain functional appearance paradoxically amplifies doubts about illness authenticity. As a result, in these narratives, the frequent emotional responses that precede insecurity are disinclination as well as unhappiness, reflecting a profound resistance to the sick role, not born of disbelief in the diagnosis, but from a conviction that accepting it would constitute a violation of their internalized imperative to remain productive, emotionally self-sufficient, and socially compliant.
For example, A43’s imperative to secure college admission produces such potent disinclination toward academic failure that he reattributes his depressive symptoms to obsessive-compulsive disorder, a condition perceived within his social context as more academically compatible. This calculated diagnostic substitution represents a strategic compromise with internalized achievement pressures, one that preserves competitive standing at the cost of authentic self-disclosure and appropriate treatment.
I have depressive disorder. When it breaks out, I
In contrast, A145’s internalized stress manifests as an obligation to fulfill ethical roles, specifically through the performance of being a good son. Despite suffering, he forces himself to embody a highly demanding version of normalcy, one characterized by perfected filial piety and emotional composure, to please his parents and relatives. His success in becoming the good kid that his parents like constitutes a pyrrhic victory, achieved only through profound self-alienation wherein external social approval masks internal psychological disintegration.
I Can’t Have Depression
A second salient theme reflects patients’ resolute conviction that they cannot possibly be suffering from depression. This pattern is characterized by institutionalized negative emotions directed toward the self, including negative assessments of tenacity, capacity, and veracity. These emotionally charged self-judgments showcase strong associations with persistent illness denial and typically co-occur with profound dissatisfaction. They characteristically manifest during later depression stages, when the illness persists and intensifies to a point where pharmacological intervention becomes necessary to manage severe symptoms. The following analysis will elucidate how these negative emotions operate within the sub-themes of self-stigma and internalized stress, creating barriers to treatment acceptance.
Self-Stigma
Self-stigma, the process whereby patients internalize public stigma through stereotype awareness, agreement, and self- application (P. W. Corrigan & Watson, 2002), serves as a key mechanism driving the negative self-judgments related to veracity and dissatisfaction observed among depressed individuals on Zhihu. However, while conventional stigma theory emphasizes components such as labeling, stereotyping, and separation (Link & Phelan, 2001), our findings reveal that in the Chinese context, self-stigma is powerfully mediated by a legitimate suffering script. This script prescribes that legitimate suffering must originate from external, significant, and socially recognized adversities such as catastrophe and sacrifice to be considered authentic and worthy of compassion.
The narratives of A31 and A27 illustrate how this script intensifies and directs self-stigmatization. A31, for instance, measures his stable living conditions and harmonious relationships against the script’s demand for external, dramatic adversity. Finding his life experience lacking these legitimizing markers, he does not process his depressive symptoms as manifestations of illness but instead morally reframes them as evidence of personal dishonesty. This process severs him from his emotional reality, negating not just the diagnosis but the legitimacy of his subjective experience.
I don’t think I have depressive disorder either. I
Similarly, A27 internalizes the script’s requirement that legitimate suffering must be severe enough to debilitate. Through comparison with others she perceives as having suffered much more, she disqualifies her distress as inauthentic. This benchmarking against extreme hardship recasts her depressive experience from a medical condition into a characterological flaw, thereby denying herself the right to suffer or even to be ill. Together, these cases demonstrate that the legitimate suffering script does not merely accompany self-stigma; it actively structures it. By providing a specific cultural logic for self-auditing, it transforms the internalization of stigma from a general agreement with negative stereotypes into a rigorous moral and existential self-repudiation.
I haven’t really suffered that much. It’s all just me being overly pretentious for attention-seeking [negative veracity: dishonesty]. There are so many who are more
Internalized Stress
Internalized stress functions as a pivotal mechanism that not only generates initial doubt about depression but facilitates negative self-judgments concerning personal tenacity and capability among depressed individuals on Zhihu. This dynamic reveals a critical paradox: the same social pressures that contribute to the etiology of depression (X. Li & Xu, 2023; Tang et al., 2021; Xu & Li, 2023) simultaneously create barriers that prevent individuals from recognizing and addressing their conditions. Within this framework, individuals attribute clinical symptoms to moral failure rather than medical pathology, creating a self-perpetuating cycle in which biologically-based symptoms are interpreted as character deficiencies.
A39’s narrative exemplifies this. She consistently attributes her hypersomnia, a clinically established symptom of severe depression (Chen et al., 2021), to moral failing of laziness and escapism rather than recognizing its medical nature. This process of symptom moralization, where biological manifestations are reconstructed as character flaws, enables fundamental denial of the depression itself.
It’s
A11’s case further demonstrates this mechanism. Confronted with his inability to meet demands for accomplishment and emotional control, he declares himself garbage. This striking self-assessment represents more than simple self-criticism; it constitutes self-disqualification from the sick role. Through this self-negation, he denies himself illness legitimacy, completing the moral transformation of psychological suffering into personal failure.
I’m
You Are Just Sick
The final theme represents a transformative stage wherein individuals who previously experienced doubt or denial gradually reconceptualize their condition, arriving at the understanding that they are, in fact, experiencing a legitimate medical condition. This thematic pattern coincides with institutionalized emotions of appreciation, particularly positive valuation and composition centered on redefining depression and establishing appropriate ways to understand and cope with the conditions. Such transitions typically follow experiences that disrupt previous denial patterns, most notably suicide attempts or severe functional impairment that necessitate medical intervention. The subsequent analysis will explore how these appreciation resources, specifically positive valuation and composition, functionally operate to correct epistemic misconceptions, challenge stigma, and mitigate internalized stress.
Epistemic Misconception Correction
Epistemic misconception correction addresses misunderstandings regarding depressive symptoms and diagnosis, with the aim of clarifying the clinical nature of depression. By anchoring distress within a biological framework, this corrective process challenges the prevailing cultural scripts that recognize only visibly severe or objectively verifiable conditions as legitimate illness, liberating patients from self-doubt and re-establishing their symptoms as valid clinical manifestations. This strategic recourse to biomedical authority, while risking limitations of biological reductionism (Haslam & Kvaale, 2015), enables patients to reconcile their lived reality with established medical understanding and establishing the foundation for therapeutic engagement and identity reconstruction.
A focus of this corrective work involves elucidating the heterogeneous clinical manifestations of depression, thereby challenging monolithic conceptions of the illness. This is exemplified in A28’s narrative, which counters the pervasive misconception that depression must present with uniformly severe or somatic symptoms. By showing how persistent sadness or anhedonia alone can constitute clinically significant depression, without requiring the presence of self-harm, or suicidality, this re-education validates the full spectrum of depressive experience and establishes less visible presentations as equally worthy of medical recognition and care.
The clinical manifestations of depressive disorder
A second avenue of correction concerns misconception about diagnostic methods, specifically by establishing the scientific legitimacy and the clinical appropriateness of psychometric scale for diagnosis. To counter skepticism regarding the subjective nature of self-report scales, proponents like A46 articulate a distinction: these instruments are not inherently subjective but derive objectivity from patients’ truthful engagement. This reframing strategically contrasts depression scales with biochemical tests, emphasizing how the former uniquely centers the patient’s subjective experience as the primary data source, thereby empowering their voice in diagnostic process. By defending the validity of the diagnostic method, this correction undercuts a source of doubt and encourages acceptance of the diagnosis’s clinical authority, establishing a critical foundation for therapeutic progress.
Stigma Challenging
Stigma challenging represents an active discursive practice through which individuals with depression on Zhihu resist moralizing interpretation of their condition, particularly the pervasive stigma pretentious for attention-seeking. Through explicitly refuting the stereotype, this practice potently counters the internalization of stereotype on the part of patients, thereby interrupting cycles of self-doubt and self-auditing concerning their veracity. Fundamentally, this constitutes a challenge to the broader cultural foundation of mental health stigma in China, specifically the legitimate suffering script inherent to its resilience culture.
A central strategy in this practice involves establishing depression’s validity as a legitimate medical condition. A97 exemplifies this by deploying linguistic negation, in specific the negative marker “not,” to reject the conflation of depression with attention-seeking. She fortifies this position by employing medically grounded terms like disease, medication, and treatment. This rhetorical move reconstructs the invisible suffering of depression as something clinically valid and urgent, which is comparable to a physical illness. By redefining the condition from a character flaw into a treatable medical reality, A28 provides a counter-narrative that helps disrupt relentless self-auditing in relation to personal veracity.
If you are diagnosed with depressive disorder, you have to get treatment! It is
Beyond medical framing, this practice incorporates a more profound assertion of the truthfulness of personal experience. A103 reveals this dimension by anchoring his narrative firmly in the domain of authentic feeling, directly asserting the validity of his suffering against accusation of pretense. This is not merely a defense but a claim to epistemic authority, the right to be recognized as the ultimate authority on one’s own mental state. By legitimizing his suffering without requiring external validation, A103 effectively interrupts destructive cycles of self-doubt and restores foundational trust in personal experience.
However, when I acknowledge my mild depression, the hatred within me gains legitimate grounds for existence, no longer requiring suppression or concealment. My pain
Internalized Stress Mitigation
Internalized stress mitigation is concerned about managing, reducing, and transforming the psychological and physiological burdens which result from absorbing socio-cultural expectations and converting them into self-directed pressure. This process specifically addresses the distinctive nature of stress that originates not from external circumstances alone, but from internalization as relentless personal demands. At its core, this process enables individuals experiencing depression to progressively decouple their sense of worth from external accomplishment and instead reclaim their intrinsic value as human beings rather than as human doings. This directly counteracts the persistent negative self-assessments regarding tenacity and capacity which characterize internalized stress and challenge the framework through which such judgments are formed. A21 and A168 illustrate this clearly.
To be specific, A21 emphasizes intrinsic worth through self-love, self-forgiveness, and openness to receiving love from others. These acts, oriented around feeling rather than output, challenge the equation of worth with utility. In A21’s view, individual value originates not from accomplishments, but from one’s inherent worthiness of love and care. This repositions identity from that of a malfunctioning tool requiring repair to a feeling, dignified human deserving compassion. Importantly, A21’s concept of love is unconditional and emotionally grounded, where loving oneself means honoring one’s feelings, and accepting love from others means permitting vulnerability. This liberates love from the burden of social responsibility, thereby disrupting the cycle of negative self-evaluation around tenacity and capacity.
The biggest and the best medicine against depressive disorder is love.
A168, on the other hand, affirms intrinsic value via self-acceptance, stating that being an ordinary person is acceptable. This counters cultural demands for exceptional achievement. Premised on this, she constructs an alternative vision of meaning centered on becoming a tailor and filling her home with flowers, a framework existing outside competitive, performance-based standards. Within this perspective, value emerges from pursuing personal interests, appreciating beauty, and cultivating joy. This perspective frees patients from the race of self-optimization and affirms the legitimacy of ordinary existence, thereby interrupting persistent self-criticism related to tenacity and capacity.
A Now, tell yourself it’s okay to be an ordinary person. Learning to be confident is the first step toward a happier life and the key to accomplishing many things. Beyond studying, there are so many other meaningful parts of life. I’ve always wanted to be a tailor and fill my home with flowers.
Discussion and Conclusion
This study analyzes 200 representative depression narratives on Zhihu, focusing on how people living with depression struggle to make sense of their depressive experiences in the Chinese context. Adopting an integrated discourse-analytic approach that combines van Dijk’s (2009) semantic macro-analysis with the
Firstly, this study identifies a distinctive form of suffering arising from epistemic misconceptions about depression in the Chinese context, which we conceptualize as symptomological suffering. Featured by profound insecurity and self-doubt regarding the legitimacy of one’s condition, this notion represents a meaningful refinement and extension of the classic somatization concept (Kleinman, 1982) in Chinese depression studies. While Kleinman’s pioneering work accurately describes how Chinese patients express psychological distress through somatic complaints, it has implicitly assumed a direct transformation of psychological distress into physical symptoms. Our findings reveal a more complex reality: before observable physical symptoms develop, many patients experience a preliminary stage of suffering rooted in conflicting cultural and epistemic frameworks. When individuals such as A168 and A149 find their subjective experience incompatible with the rigid, often extreme definition of depression available in public discourse, they develop deep-seated self-doubt about the validity of their own suffering. This distress does not stem from a mind-body conversion, but rather from a collapse in meaning-making, a misalignment between subjective assessment paradigms of modern psychiatry and the ingrained cultural preference for objective, verifiable evidence of disease within traditional Chinese medical systems (Karchmer, 2013).
Secondly, this research elucidates the distinct dimensions of suffering inherent to mental health stigma within the Chinese sociocultural context. We demonstrate that the moralized stigma, in particular the prevalent one pretense for attention-seeking, can produce a suffering that extends beyond the social devaluation processes described in conventional stigma theory (Link & Phelan, 2001). Rather than merely causing status loss and discrimination, this moralized stigma undermines individuals’ capacity to trust their own subjective experiences. This erosion of self-trust forces patients to constantly question the validity of their emotions and suffering, creating profound insecurity that compounds their original condition. Besides, we identify a legitimate suffering script as the cultural mechanism enabling self-stigma (P. W. Corrigan & Watson, 2002). This deeply embedded cultural framework requires that authentic suffering must stem from visible, socially recognized adversities to be considered authentic and worthy of compassion. This extends our understanding beyond Western individual-centered stigma models by revealing how collectivist moral frameworks shape the internalization process (L. H. Yang et al., 2007). When individuals’ experiences of depression lack these culturally sanctioned markers of legitimate suffering, their suffering becomes invalidated for failing to meet established cultural standards for genuine pain (Kleinman, 1989). The identification of this script provides a crucial bridge between macro-cultural narratives and micro-level self-stigma processes, offering a more nuanced understanding of how stigma becomes psychologically impactful in specific cultural contexts.
Thirdly, this study advances our understanding of internalized stress as a distinct mechanism shaping depression experiences within contemporary China. While existing literature predominantly frames symptom concealment as a strategy for avoiding social discrimination (P. Corrigan, 2004; Follmer & Jones, 2021), our analysis demonstrates how Chinese individuals conceal symptoms to maintain alignment with cultural success scripts and ethical role expectations. This concealment represents more than simply hiding a stigmatized identity (Goffman, 1963), it constitutes the active performance of a socially anticipated identity. The psychological costs of this sustained performance extend beyond mere fatigue to include insecurity and deepening doubt regarding the legitimacy of one’s condition. Furthermore, this research reveals that the negative self-assessments of tenacity and capacity, typically associated with diminished self-esteem and self-efficacy in stigma literature (e.g., Link et al., 2001), can originate directly from internalized sociocultural pressures rather than merely reflecting stigma. In this context of internalized stress, individuals are shaped into what can be termed as a performative self, an identity whose value resides in its productivity, resilience, and contribution to family welfare. Depression, through its direct erosion of these essential capacities, is consequently experienced not merely as an illness but as a betrayal of this performative ideal. This explains why the distress associated with depression in China is so deeply entangled with feelings of moral failure, moving beyond purely psychosocial models of stigma.
Fourth, this study identifies and conceptualizes the unique therapeutic opportunity created by algorithm-mediated platforms like Zhihu in facilitating illness sense-making among Chinese depression sufferers. While existing research has established that online communities can reduce feelings of isolation (Kotliar, 2016), our findings reveal a more nuanced mechanism: these platforms function as culturally-situated meaning-making systems which enable users to develop coherent illness identities through collaborative narrative exchange. The analysis showcases how a single question about self-doubt can catalyze a collective sense-making process, where individuals progressively construct medical understanding through shared storytelling and peer validation. This represents a departure from mere information-seeking models of online health behavior (e.g., Fox, 2011), revealing instead a dialogic identity construction process wherein patients learn not only biomedical facts about depression but, more crucially, develop the narrative resources to articulate and legitimize their subjective experiences within a community of understanding. Importantly, this research theorizes these platforms, despite potential risks (J. Wang et al., 2023), as potential culturally-embedded buffer spaces where patients navigate the profound moral and epistemological struggles inherent in Chinese mental health experiences. These digital spaces can offer temporary refuge from the legitimate suffering script and performance pressure we have identified, generating conditions for collaborative meaning reconstruction, a process which addresses not just informational needs but the human need for epistemic validation and moral realignment when one’s experiences contradict the dominant cultural narratives.
The findings of the study have practical implications. Regarding symptomological suffering, clinicians must move beyond diagnosis to proactively validate the patients’ struggle for cognitive clarity. This involves explaining the scientific basis of psychiatric diagnosis and educating patients on the wide, often invisible, spectrum of depressive symptoms, thereby countering the restrictive cultural script that equates real illness only with severe, visible dysfunction. For suffering induced by moralized stigma, therapeutic interventions must focus on restoring patients’ trust by creating clinical spaces wherein their subjective suffering is affirmed as legitimate, regardless of conformity to external cultural criteria. Public initiatives, in turn, should transcend beyond generic anti-stigma campaigns to directly deconstruct the rigid legitimate suffering script by broadening the cultural understanding of valid distress. To mitigate suffering from internalized stress, patients benefit from structured support in developing the capacity to set realistic goals and monitor incremental progress through manageable recovery stages. This approach helps rebuild agency by focusing on functional adaptation rather than idealistic cultural standard of success. Besides, digital platforms present unique therapeutic opportunities that warrant strategic engagement. Patients can be guided to use these spaces not merely as information sources but as venues for meaning-making practice, where they actively seek resonant narratives to counter isolation and self-doubt. Concurrently, public health authorities should collaborate with platforms to develop targeted intervention models. These could integrate trained peer supporters and mental health professionals to steer discussions toward constructive engagement while mitigating risks like negative social comparison and misinformation. This approach offers a valuable strategy potentially applicable across diverse cultural settings.
This study is subject to several limitations. A limitation stems from its reliance on online illness narratives without direct engagement with the individuals who share them. While this provides authentic data, it restricts deeper interpretation of subjective illness experiences. Future studies can adopt mixed-methods designs, integrating interviews to facilitate follow-up questions and yield more nuanced, co-constructed understandings of personal depression journeys. In addition, the absence of a gendered perspective also represents a limitation. Although Western research has documented differences in how depression is experienced across genders (e.g., Clarke & van Amerom, 2008), similarly nuanced studies in the Chinese context remain scarce. Future research should examine how gender norms influence acceptance of an illness identity, patterns of help-seeking, and internalization of stigma. Besides, the study does not address the role of algorithms in shaping user experience. Social media platforms such as Zhihu utilize algorithms to recommend content and connect users, structuring the information environments and community ties available to individuals. Research into how these mechanisms facilitate, or potentially impede, supportive connections and access to reliable information could inform the design of more targeted and effective online mental health resources. Finally, this study has focused specifically on how depression is understood in China’s cultural context. Nonetheless, many other collectivistic societies, particularly across Africa, also grapple with mental health stigma (e.g., Agyei et al., 2024; Dzokoto et al., 2023; Opare-Henaku & Utsey, 2017). Future research would benefit from cross-cultural comparisons to investigate how depression is conceptualized differently across collectivistic cultures. For instance, whereas Chinese context may moralize depression as manifestations of pretense for attention-seeking, some African contexts may intertwine depression with spiritual interpretation or socioeconomic adversity. Understanding these differences can help develop mental health support models that are culturally grounded and globally informed.
Footnotes
Ethical Considerations
The Ethics Committee of the Guangdong Provincial Hospital of Chinese Medicine reviewed the study protocol and determined it to be exempt from formal approval. Notwithstanding this exemption, the research was conducted in full compliance with the ethical principles of the Declaration of Helsinki and the CIOMS International Ethical Guidelines.
Consent to Participate
Informed consent was waived as this study utilized publicly available, anonymized data.
Consent for Publication
All authors provide their consent for publication of this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Project of Humanities and Social Sciences, Ministry of Education, People’s Republic of China (grant no. 20YJA740001).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.