
Abstract
The Community-Based Newborn Care program is a community level newborn care package within Ethiopia’s maternal and newborn health continuum. This evaluation assesses the process of the Community-Based Newborn Care program in Tach Armachiho district, Northwest Ethiopia. A community-based case study with mixed approaches was used to assess the community-based newborn care program. A total of 33 indicators related to acceptability, compliance, and availability were evaluated. Data from 344 mothers were analyzed in Stata using bi- and multivariable logistic regression to find the variables associated with mothers’ satisfaction with a significance level of p < .05. Manual transcription, translation, coding, and analysis were done for qualitative data. Overall program performance was evaluated against predetermined standards. The community-based newborn care program achieved an overall implementation rate of 65.35%, with 69% resource availability, 65.8% compliance, and 61.7% caregiver satisfaction. Caregiver satisfaction was significantly associated with maternal education and the timing of the newborn’s first visit: mothers who could read and write were nearly five times more satisfied than mothers who couldn’t (AOR = 4.79, 95% CI: [1.23–18.66]), while those whose newborns were seen after 14 days were 80% less satisfied than those whose newborns were seen within 1 to 3 days of birth (AOR = 0.2, 95% CI: [0.05–0.9]). The overall implementation of the community-based infant care program, and each assessed dimension, was graded fair, indicating the need for improvement. Mothers’ satisfaction was significantly related to their education level and the time of their newborn’s first visit.
Background
The Ethiopian Health Extension initiative has achieved a significant milestone with the community-based neonatal care (CBNC) initiative. This is a newborn care package integrated into the maternal and neonatal healthcare continuum, now being executed at the community level in Ethiopia (Gebremedhin et al., 2020). CBNC aims to improve the Primary Health Care Unit (PHCU) and the Health Extension Program, which serve as a community’s primary care delivery network (Berhanu & Avan, 2019).
Neonatal death is a child health issue that the worldwide community aims to minimize to the lowest possible level by 2030 (Amuka et al., 2020). In 1950, there were 216 deaths per 1,000 live births; by 2017, that number had dropped to 38 and·9 deaths worldwide. However, there are disparities in this decline across regions (GBD 2017 Mortality Collaborators & Iqbal, 2018).
Every year, 2.9 million neonates die in their first 24 hr of life, with 45.0% dying at home (Halim et al., 2016).
In the world in 2019, a newborn baby died every 13 s. Additionally, the newborn phase accounted for 47% of all deaths in children under five, up from 40% in 1990 (Sanyang, 2019). Most of these deaths occurred in low- and middle-income nations, where most births and illnesses that lead to death occur at home. Community-based initiatives are therefore desperately needed (Bailey et al., 2017; Chou et al., 2017). Under-five child mortality remains highest in WHO African countries (more than 80 per 1,000 live births, almost 7 times higher than the WHO European region’s; UNICEF, 2021; Vardell, 2020).
Every year, nearly 35,000 Nepali children die before their fifth birthday, with roughly two-thirds of these deaths occurring in the first month of life (WHO, 2020), 7.35% children die before celebrating their fifth birthday in Sub-Saharan Africa (Tesfa et al., 2021). The majority of those deaths can be prevented or avoided by implementing interventions in the primary healthcare system (Simmons et al., 2021).
South Asia and Sub-Saharan Africa accounted for 79% of the overall burden of newborn deaths, with South Asia accounting for 38%, West and Central Africa for 23%, and East and South Africa for 18% (Hug et al., 2019). In Sub-Saharan Africa, 50% of deliveries take place at home without a qualified birth attendant (Lassi et al., 2019).
A significant number of neonatal deaths occur in developing nations where access to healthcare is limited. Of all infants, about half die at home because most mothers and their babies do not receive professional care during and right after birth. Process assessments in Ethiopia have shown that inadequate supervision, uneven drug delivery, and insufficient refresher training hinder the success of CBNC programs (Gebremedhin et al., 2019).
Despite periodic reductions, newborn mortality remains a problem in Ethiopia (Belachew et al., 2022). The percentage of home deliveries in Ethiopia’s Gambella Region was 38.5%, according to the report’s findings. It was found to be substantially correlated with not having a written birth preparedness plan, not being exposed to the media, and not receiving any prenatal care visits, which leads to missing community-based newborn care and newborn care from health facilities due to lack of immediate reporting (Wang, 2022).
Ethiopia introduced community-based newborn care in March 2013 with the aim of lowering newborn and child mortality, building on the knowledge gained from integrated community case management of common childhood illnesses with strategies including the identification and management of sick newborns at the community level when referral is not possible (Mathewos et al., 2019). Although the Ethiopian government did these and many health interventions, it is still one of the top 10 countries in Africa (Agonafir et al., 2019) and ranks fifth with the highest number of neonatal deaths globally (UNICEF, 2017).
The overall customer satisfaction rate for comprehensive emergency obstetric and newborn care services was 65.1% (Tiruneh et al., 2022). According to the Ethiopian Mini Demographic Health Survey (EMDHS 2019) report, neonatal mortality rates increased from 29 per 1000 live births in the Ethiopian Demographic Health Survey (EDHS 2016) to 30 per 1000 live births (Gebremichael et al., 2023; Wolde et al., 2019). According to the 2020 HMIS report of the Tach Armachiho district health office, 41% of mothers give birth at a health facility, ANC4 was 41%, and postnatal care was 23%, which is low. All the information presented above suggests that the community-based newborn care program is being implemented in various places, but the level of implementation is doubtful in our evaluation area. Therefore, this evaluation aims to assess the CBNC program, generating comprehensive evidence regarding its implementation process and pinpointing the enablers and obstacles to inform decision-making. Additionally, evaluation findings will be available to all program stakeholders, allowing them to use them to improve the program and meet its stated goal.
Program Logic Model (Figure 1)
Problem: Despite the Ethiopian government’s many health efforts, such as training health professionals, improving referral systems, integrating health services, implementing the Health Extension Program (HEP), and routine immunization, newborn mortality remains high. Ethiopia’s mother and child health services are underutilized.
Goal: Reduce newborn mortality by providing high-quality maternal and newborn health care and creating community demand.
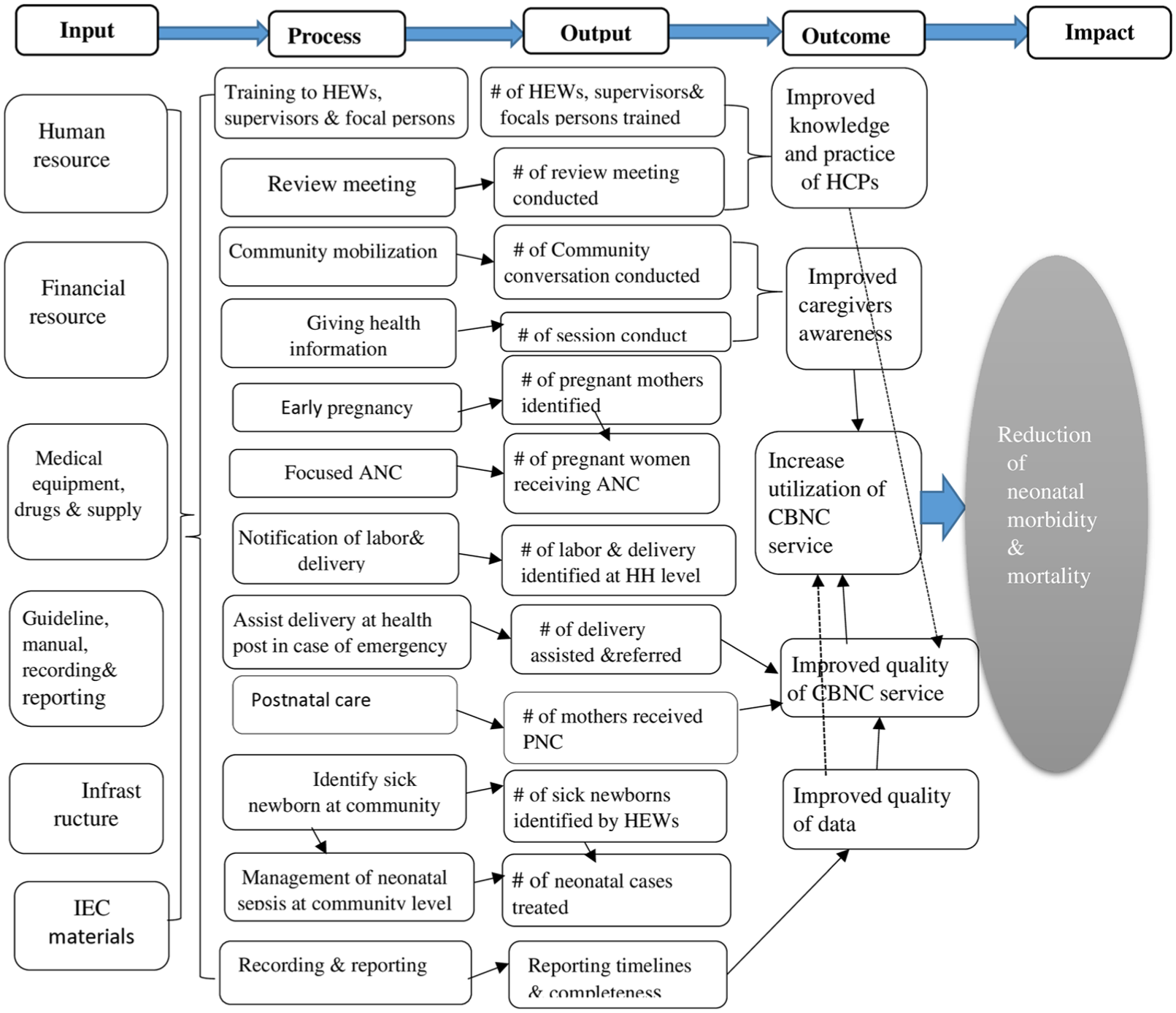
Logic model of CBNC in Tach Armachiho district, April 2021.
Methods
Evaluation Design and Setting
A case study evaluation was conducted in Tach Armachiho district, which is located 790 km Northwest of Addis Ababa, the capital city of Ethiopia, and 398 km from Bahir Dar, the capital city of Amhara National Regional State. The district’s total population is 121,321 (23), with 60,539 (49.9%) males and 60,782 (50.1%) females (Tach Armachiho District Health Office, 2021). The district has 1 primary hospital, 6 health centers, 28 health posts, 12 private clinics, and 6 rural drug vendors. Furthermore, 56 HEWs serve the district’s HPs and the CBNC service has been offered in all HPs to the community.
Evaluation Approach and Dimensions
A formative approach of program evaluation was employed to assess the implementation of CBNC, which is appropriate in the implementation stage in order to inform providers and stakeholders about patterns in results and identify implementation barriers and facilitators. This information can help to provide a clearer description of program processes, enhance the program’s functionality, and refine the overall strategy of the program. The focus of the evaluation was the process of CBNC program implementation, which means it focused on understanding, describing, testing, and improving components of a program’s process theory. Process theory includes the program’s organizational plan (activities to be accomplished and resources to be used to implement the CBNC program) and service utilization plan (assumptions taken by the program about the uptake of services produced and accessibility and utilization of the program). The program description is displayed in Figure 1. This evaluation relied on the Access Framework (availability and satisfaction dimensions; Cu et al., 2021) and the Implementation Fidelity Framework (compliance dimension; Gage et al., 2020), because they were clearly aligned with the study objectives and accessible data. These frameworks enabled focused and contextually appropriate evaluation.
The Access Framework guided the evaluation design by focusing on service availability and satisfaction, which were then converted into appropriate indicators. It helped to assess whether services were both available (present and accessible in health posts) and deemed satisfactory by clients. The Implementation Fidelity Framework provided guidance for process evaluation by identifying indicators of program compliance. This means it offered a methodical framework for assessing whether services were given as planned. Together, these frameworks offered the conceptual basis for both indicator selection and finding interpretation, assuring alignment with the study objectives, data collection, and analysis.
Sample Size and Sampling Procedure
For this evaluation, the district was purposively selected. The district had been implementing CBNC for several years, making it suitable for assessing the implementation process. Furthermore, its accessibility and the researcher’s prior professional experience within the district health office provided practical feasibility and contextual insight, which enhanced the depth and accuracy of the evaluation.
The three dimensions were used to establish the sample size. The sample size for assessing caregivers’ satisfaction was calculated using a single population proportion formula, n = (

The diagram of sample size and sampling procedure for client survey for process evaluation of CBNC services in Tach Armachiho district, April 2021.
The sample size for measuring the compliance dimension was calculated using a single population proportion formula based on the results of a prior study that found that 68% of health extension workers were following the CBNC guidelines while delivering the service. The margin of error (d) was considered to be 5% at a 95% confidence level, resulting in 335. During the quantitative data collection, approximately 344 participants were reached, as described above. We also reviewed all relevant documents to determine whether HEWs had complied with the program guidelines.
First, a lottery was used to choose nine health posts at random. Documents and records were examined at these health posts. Nine randomly chosen health posts were included to evaluate the resources available for the program’s delivery. Beginning with the most recent registration number, the registration was evaluated until each chosen health post had the required sample size.
A total of 36 observations were conducted, 4 observations in each selected HP using opportunity sampling at the time of arrival at the HP. A total of nine health posts and a district health office resource were inventoried. All documents in the last 6 months were reviewed for a compliance assessment. In addition, a total of 18 key informants were purposively selected and interviewed. The selection procedure was followed as:
As a result, this evaluation has to examine all participants in each of the specified HPs.
Variables and Measurements
Independent variables for the logistic regression model were selected based on previous empirical research on factors influencing CBNC service utilization in comparable contexts, as well as theoretical relevance from the Access Framework and the Implementation Fidelity Framework.
Availability: Refers to the physical existence or reachability of services that meet a minimum standard, such as basic equipment, drugs and commodities, the health workforce (presence and training), and guidelines for treatment (1). Availability of resources such as the CBNC guideline, the ICCM registration book for sick young infants 0 to 2 months of age, a family card (integrated maternal and newborn and child health cards), a weighing scale, a newborn Am bu-bag, a thermometer, a tape meter, a watch with a second’s arms, a reporting format, and drugs and medical supplies were assessed using 12 indicators.
Compliance: Refers to whether the actions taken to implement the program services are in line with the national CBNC guidelines and protocols, as well as standards, best practices, or both (Gebremedhin et al., 2020). The compliance of healthcare providers and HEWs with the national CBNC guideline was assessed using 11 indicators.
Acceptability: Whether available community-based newborn care services are appropriate to the norms, expectations, and cultural behaviors of the population in the area. The outcome variable (caregivers satisfaction level) was measured using 10-item questions, each containing a five-point Likert scale (1 = very unsatisfied, 2 = unsatisfied, 3 = neutral, 4 = satisfied, and 5 = very satisfied) alternatives (Gebremedhin et al., 2019). The level of caregiver satisfaction was classified into two categories: satisfied above a specified cut point and dissatisfied below that point. This value is derived from the demarcation threshold formula: [(total highest score − total lowest score)/2] + total lowest score (Belay Bizuneh et al., 2020; Gebremedhin et al., 2020) which produced a result of 31. Finally, caregivers who scored 31 points or above were considered “satisfied,” and those below that point were considered “dissatisfied.” Stakeholders decided the indicators’ weight during the evaluability assessment. The achievement was calculated by the formula
Data Collection Tools and Procedures
A structured questionnaire was developed and used for the survey and a semi-structured questionnaire for key informant interviews, observation, and document review. These questionnaires are adapted from related literature (Gebremedhin et al., 2019). To ensure uniformity, the tool was first created in English, translated into the local language (Amharic), and then returned to English by an expert. Data collectors were eight nurses, four midwives, and two public health officers (of whom one was a supervisor) who were trained on data collection by the principal investigator concerning the data collection tool, interviewing procedures, observation, and related ethical considerations. The principal investigator and the supervisor oversee the daily work of each data collector and provide feedback on each stage. The data collection tool was checked the for validity, understandability, and clarity by conducting a pretest on 5% of mothers in the same district, but from HPs that were not selected for the study, and necessary corrections were taken before the actual data collection. A key informant interview was conducted using an informant review guide and recorded voices after obtaining consent and arranging an appropriate time and place. Credibility was enhanced through probing questions, avoiding leading questions, enhancing confirmability was improved through evaluator cross-checking, and transferability was promoted through detailed descriptions of the study participants were ways used to ensure the reliability of qualitative data.
A non-participatory direct observation was carried out while healthcare providers delivered CBNC services to the customers. Initially, consent was obtained from HEWs and caregivers. The first two observations were discarded while observing from each HEW to reduce the Hawthorne effect.
Inclusion and Exclusion Criteria
Inclusion Criteria
Health extension workers assigned and working in the selected HPs for at least the last 6 months.
Mothers who have delivered in the past 6 months, whether at home or in a facility within the district.
Assigned head of the district health office and selected cluster health centers.
Health extension focal persons in the selected HCs working for at least 6 months.
CBNC service documents in the last 6 months were included.
Exclusion Criteria
Mothers who delivered in a different place and subsequently traveled to the study area were not included in the survey.
Subjects not available during evaluation period.
Data Management and Analysis
Before data collection, training was given to data collectors, and confidentiality issues were discussed with all data collectors. During the data collection process, data editing, coding, and questionnaire verification were performed. Following data collection, each data collector submitted their completed questionnaires in hard copy to the supervisor and principal evaluator, who also reviewed and coded the completed forms to ensure consistency and completeness. Soft copy files were regularly checked and stored to avoid data loss. Forms and surveys that had been completed were stored in a secure location to maintain confidentiality and privacy. Any issues were identified and immediately resolved. Finally, the data were coded, entered into Epi Data version 4.6, and exported to Stata version 14 for processing. The results were mainly presented by using frequency tables and graphs. Variables that had an association with the dependent variable with a p-value <.25 in bivariate logistic regression were candidates for multiple logistic regression and were used to assess the statistical significance. p-value <.05 and confidence interval in multivariate analysis were used to declare an association. The Hosmer and Lemeshow test was used to assess the model’s goodness of fit. We also assessed model multicollinearity using the Variance Inflation Factor which was 1.05 (with the highest 1.08, and the lowest 1.03). These diagnostics confirmed that the final models were robust and well-fitted.
Odds ratios and 95% confidence intervals were derived from each variable coefficient. The strength of the association was evaluated using the AOR with a 95% confidence interval, and variables considered significant had a p-value of less than .05.
The audio-recorded qualitative data were transcribed into the text format of Amharic and translated into the English language. The analysis was conducted on each component thematically, and the findings were shared in a narrative style to clarify the quantitative result. Both qualitative and quantitative data were mixed during the interpretation phase to justify the degree of achievement; the qualitative data was enhanced by the quantitative data. Finally, the indicators under each dimension of processes (availability, compliance, and acceptability/satisfaction) were judged based on the judgment matrix to assess the implementation level. The judgment criteria for the overall implementation were 85 to 100, 70 to 84.99, and <70, which were well implemented, needed improvement, and urgent improvement, respectively.
Results
For the quantitative survey, a total of 344 mothers participated, with a response rate of 96.90%. Eighteen 18 key informants (9 males and 9 females) from the district health office, health center, and health posts were included. About 36 observation sessions were carried out. Furthermore, program documentation of the last 6 months was reviewed.
Availability of Resources
Including 56 HEWs, there are a total of 162 healthcare workers in the Tach Armachiho district, of whom 5 public health officers (62.50%), 11 nurses (25.00%), 6 midwives (35.29%), and 48 HEWs (85.71%) were trained on CBNC.
“I was trained for the CBNC program three years ago, and there has been no refresher training.” Furthermore, I don’t currently receive CBNC program-specific supportive supervision from the zone or the district health offices. As a result, it is difficult to provide suitable care to mothers and newborns who have recently given birth. (a 26-year-old HEW)
Key informant interview results show that the program’s operations have been disrupted several times due to a lack of consistent financing partners and funds to purchase necessary pharmaceuticals and assistive technologies.
All supervisors and the district health office head agreed that women and newborns do not receive full CBNC services at health posts and home-to-home bases due to political insecurity and HEWs’ lack of motivation.
Non-governmental groups previously assisted CBNC but no longer do so. As a result, there is insufficient funding to provide medications and other supplies for all HPs, particularly this year. Due to this reason, we face serious shortages, especially of TTC eye ointment and vitamin K. (a 30-year-old male health center head)
The majority of health posts had the necessary medications and supplies for the CBNC program (average availability of 76.07%); there were significant shortages in specific items. For example, only roughly half of the facilities had TTC eye ointment and vitamin K, and paracetamol suppositories were totally unavailable. The success of the program may be compromised if these shortages adversely affect the treatment of community-based newborn care. On the other hand, the steady supply of essential antibiotics (gentamicin, amoxicillin) and supplies for delivery (syringes, surgical gloves, and weighing scales) indicates the program’s strength and ability to deliver the CBNC program (Table 1).
Availability of Drugs and Medical Supplies for the CBNC Program in the Health Posts in Tach Armachiho District, April 2021.

A 24-year-old female HEW said: “I had asked the HC store again and again about essential drugs and medical supplies like paracetamol suppository, vitamin K, cotton, and gauze, even though I couldn’t get them. They reply to me that those resources are not available even in the HC.”
The majority of health extension workers (HEWs) were trained in CBNC services (85.71%), and essential job aids such as ICCM registration books, treatment charts, and infant weighing scales were readily available, increasing the capacity to provide community-based newborn care.
However, there were significant deficiencies in other crucial areas. For example, just 18% of health center staff had CBNC training, slightly more than half of health posts maintained a constant supply of pharmaceuticals and supplies (55.55%), and only one-third of facilities had resuscitation bags. In addition, according to key informant interviews, all health posts lacked a registration book for delivering home-to-home services, identifying pregnant moms, and a referral form from the women’s health development team. The lack of regular supply chains and minimal training for staff, particularly at the supervisory health center level, poses substantial challenges to the program’s effective implementation. Overall, the availability sub-dimension received a “fair” rating (68.98%), indicating that, while the CBNC program’s foundational elements are in place, significant improvement is required in supply continuity, supervisory capacity, and the provision of lifesaving neonatal equipment to ensure full and effective implementation (Table 2).
Summary of CBNC Program Resource Availability in Tach Armachiho District, April 2021.

Note. E# = expected in number; O# = observed in number; W = weight; S = score, A% = achievement in percent (S/W*100); JP = judgment parameter.
Compliance With the National Guideline
In the last 6 months, about 277 mothers out of 344 have registered for a postnatal visit. Out of these, 145 (52.35%) were assessed between 1 to 3 days, 87 (31.40%) were seen between 3 and 7 days, 20 (7.22%) were seen between 7 and 14 days, and the remaining were seen beyond 14 days. Within 7 days following delivery, 297 (86.34%) infants were weighed, with 8 (2.69%) having a birth weight of less than 2.5 kg.
HEWs are generally good at interacting with caregivers and getting preliminary information, as evidenced by their very high scores (almost 100%) for respect, inquiring newborn age, and major problem. This suggests a high level of interpersonal skills and compliance to the most evident element of care. On the other hand, asking for unconsciousness (42%), convulsion (48%), jaundice (31%), and HIV status evaluation (36%), all showed extremely poor performance. If ignored, these conditions can be fatal. It is implied that HEWs might not identify and refer severely ill newborns, which could lead to preventable mortality and morbidity (Table 3).
Observation Result of Tasks Assessment of HEWs for Sick 0 to 2 months of Young Infants in Tach Armachiho District Nine HPs, April 2021.

According to the findings of the KII with health center heads, all examined health posts got monthly follow-ups and oversight from their catchment health center. However, this was not program-specific, and there were gaps in between. As stated by KII with HEWs, the district health office offered integrated supportive supervision to five health posts on a quarterly basis, while the zonal health department provided program-specific supporting supervision to two of the nine HPs. HEWs had 7 years of job experience on average.
Although it was not particular to the CBNC program, I had monthly supervision from the cluster health center’s health extension focal and HC health professionals; nevertheless, I had never received supervision from the zone. (a 28-year-old female HEW)
Another health extension worker also described supportive supervision as follows: “I had gotten weekly supportive supervision from cluster HC for the previous six months, but because this kebele was chosen as the year’s model kebele, the supervision is not consistent. I am confident it will stop after I accomplish this task.” (A 24-year-old female HEW)
Review meetings were held every six months to assess the achievement of HEWs on all health extension packages in addition to CBNC service due to a lack of funding. (a thirty-year-old health office head)
Every HEW interviewed agreed that the lack of rotation and inadequate pay were barriers to successfully implementing the package.
According to the study results, 331 (96.22%) respondents are familiar with HEWs, and 236 (77.90%) mothers received information on ANC from the health facility. Out of the total respondents, 293 (85.17%) said there was HDA in their kebele, of which 224 (76.45%) were members of the women’s health development (1–5 network) team, and 161 (46.80%) attended a meeting during their recent pregnancy.
Of the 297 (86.33%) mothers who had ANC services at least once, 252 (73.25%) were in the first trimester, 36 (10.46%) in the second trimester, and 9 (2.62%) in the third trimester. During their antenatal care, 232 (78.11%) mothers attend HC, 49 (16.50%) attend hospital, and 16 (5.39%) attend HP. Out of the total respondents, 269 (90.57%) consumed iron for an average of 105 days (ranging from 30 to 180 days), while 237 (79.80%) were given deworming treatment during their most recent pregnancy. Furthermore, 270 (90.91%) women received the TT vaccine, and 225 (75.76%) had their weight measured during their last pregnancy. The majority of the mothers (63.95%) delivered in HC, 99 (28.78%) in hospitals, 6 (1.74%) in HP, and the remaining delivered at home. The delivery outcome of 337 mothers (97.97%) was live birth, but the rest, 7 (2.03%), lost their infant. About 116 (33.72%) of neonates applied something to the stump immediately after delivery, with ointment or powder accounting for 97 (28.20%) and butter, oil, or other substances accounting for the remaining 19 (5.52%), which were applied by health personnel and relatives, respectively.
If medication were available, about 335 (97.38%) of caregivers would need to use it to prevent cord infection. About 305 (88.66%) of neonates begin breastfeeding within the first hour, 33 (9.59%) begin breastfeeding between 1 and 24 hr, and 6 (1.74%) begin breastfeeding beyond 24 hr of birth. Around half of the mothers (49.71%) received information about breast-feeding from health extension workers, 102 (29.65%) received information from HC health care professionals, 47 (13.66%) received information from the hospital, and the remaining 24 (6.98%) received information from community groups and relatives. Among the 344 participants, 294 mothers (85.47%) were informed about community-based newborn care offered by Health Extension Workers at both health posts and within the community.
Mothers’ awareness of important neonatal warning signs differed, as Figure 3 illustrates. Redness or discharge from the cord (79.36%), difficulty suckling/inability to feed (88.08%), and fever (88.66%) were the most commonly recognized symptoms. A smaller number of mothers, though, identified skin pustules (57.56%) and hypothermia (63.66%). In general, more mothers were aware of common and obvious symptoms, but fewer of them were aware of subtler but clinically serious danger signs (Figure 3).
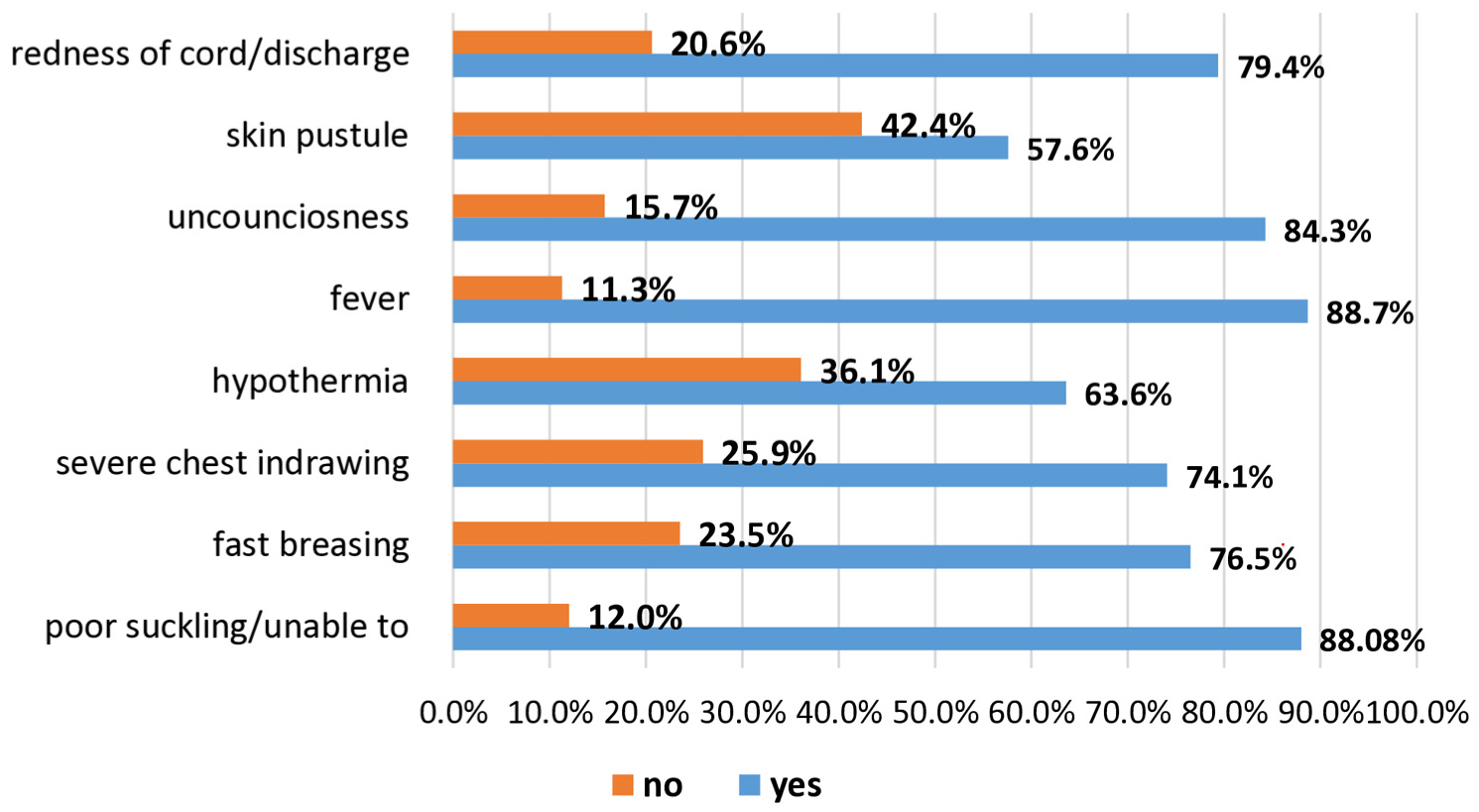
Mothers’ knowledge of danger signs for newborn infants in Tach Armachiho district, April 2021.
About 277 (80.52%) mothers checked on their newborn’s health during the first 2 months after delivery by HEWs. From these, 51 (18.41%) newborns checked only once; 76 (27.44%) checked two times; 123 (44.40%) checked three times; and the rest (9.75%) checked four and above times. About 137 (60.3%) out of 277 newborns were checked within 72 hr; 66 (22.6%) were checked between the 3rd and 7th days; 20 (7.22%) were checked between the 7th and 14th days; and the rest were checked after 14 days of delivery by health workers.
From the total respondents, 278 (80.81%) of newborns did not experience any health problems, but the rest, 66 (19.18%), had experienced at least one health problem in the first 8 weeks of life. From these, 21 (31.82%) were admitted to a health facility, and 45 (68.18%) were treated as outpatients. The mean age of young infants who experienced health problems was 35.6 days, with ±13.7 days SD. Of those, 29 (43.94%) young infants consulted HC health care professionals and went to nearby HC to receive medical services. The rest, 10 (15.15%), 5 (7.57%), and 14 (21.21%) went to hospitals, clinics, and HP, respectively, to receive medical services, with an average visit of three times. Nevertheless, eight of the newborns who experienced health problems did not visit any health facility for the reason that one perceived that there was no reliable service, 2 (25.00%) had financial problems, and 5 (62.50%) were unable to visit any health facility because of distance.
The majority of newborns (297, or 86.34%) were weighed within the first 7 days of life, with 99 (33.33%) weighing at the hospital, 181 (61.94%) at the health center, and the remaining 17 (5.72%) being measured at health posts and home by HEWs. Of those who were weighed, 289 (97.31%) had a normal birth weight, and 8 (2.69%) had a low birth weight. Mothers who had small newborns were advised to breastfeed frequently and keep the baby warm, but only 5 (62.50%) received advice about danger signs, repeat baby weighing, and repeat visits to health facilities for newborn health. Approximately 183 (53.19%) of moms were satisfied with the availability of medications in the HPs.
The overall HEW compliance in Tach Armachiho district was 65.83%, indicating a need for quick improvement. Among the specific indicators, very good performance was noted in inquiring for the primary problem of unwell young newborns (100%), referral of very severe disease cases (100%), and neonatal sepsis therapy (100%). On the contrary, poor performance was observed in babies who got PNC visits within 48 hr (40.28%). Compliance was particularly low in technical therapy components such as accurate neonatal sepsis treatment (13.00%), providing seven consecutive doses of gentamycin for very severe disease (59.00%), and administering the initial antibiotics for VSD (59.33%) (Table 4).
Summary of Performance Indicators of Compliance of HEWs in Tach Armachiho District, April 2021.

Note. E# = expected in number; O# = observed in number; W = weight; S = score; A% = achievement in percent (S/W*100); JP = judgment parameter.
Satisfaction of Mothers With CBNC Services
Sociodemographic and Socioeconomic Characteristics
The study included mothers ranging in age from 19 to 44 years old, with a mean of 31.35 (SD 5.6).
The majority of moms, 293 (85.17%), were married; 14 (4.06%) were divorced; 8 (2.32%) were widowed; and the remaining 29 (8.43%) were single. The religious background of 323 (93.89%) mothers was Orthodox, whereas 21 (6.10%) were Muslims. In terms of educational status, 147 (42.73%) of women could not read or write; 58 (16.86%) could read and write but had no formal education; 91 (26.45%) attended elementary school; 36 (10.46%) attended high school; and the rest 12 (3.49%) had college or higher education.
In this survey, 257 (74.71%) of moms worked as housewives, 26 (7.56%) as daily laborers, 24 (6.98%) as merchants, and the remaining 16 (4.65%) as government employees. In this study, moms had an average of 3.8 children (ranged 1–10, SD±1.86) (Table 5).
Socio-Demographic Characteristics of Respondents in the Survey at Tach Armachiho District, April 2021.

Mothers’ Satisfaction With CBNC Service
In this study, more than half of the clients (223, or 64.82%) were satisfied with the counseling services they received from HEWs, with a mean of 3.5 and a ±0.94 standard deviation. One hundred eighty-four (53.49%) clients were satisfied, whereas 21 (6.10%) were extremely dissatisfied with the appropriateness of the visit time to get CBNC services. Out of all respondents, 92 (26.74%) of clients were satisfied, but 22 (6.39%) were unsatisfied, and 86 (25.00%) were very unsatisfied with the availability of drugs at the health post, with a mean of three and ±0.998 SD (Table 6).
Lack of medicine in HPs and emergency transportation (ambulance) during labor, as well as early postpartum emergencies, were common complaints forwarded by clients on CBNC service. (a 28-year-old female WEW)
The Level of Client Satisfaction With Each Satisfaction Measuring Item of CBNC Services Supplied in the Tach Armachiho District in April 2021.

The level of caregiver satisfaction was classified into two categories: satisfied above a specified cut point and dissatisfied below that point (Table 7). This point was calculated using the demarcation threshold formula: [(total highest score − total lowest score)/2] + total lowest score] (Rodríguez-Herrera et al., 2021).
Clients’ Satisfaction Category on Each Satisfaction Measuring Item of CBNC Services Provided in Tach Armachiho District, April 2021.

Bivariate and Multivariate Analysis of Satisfaction
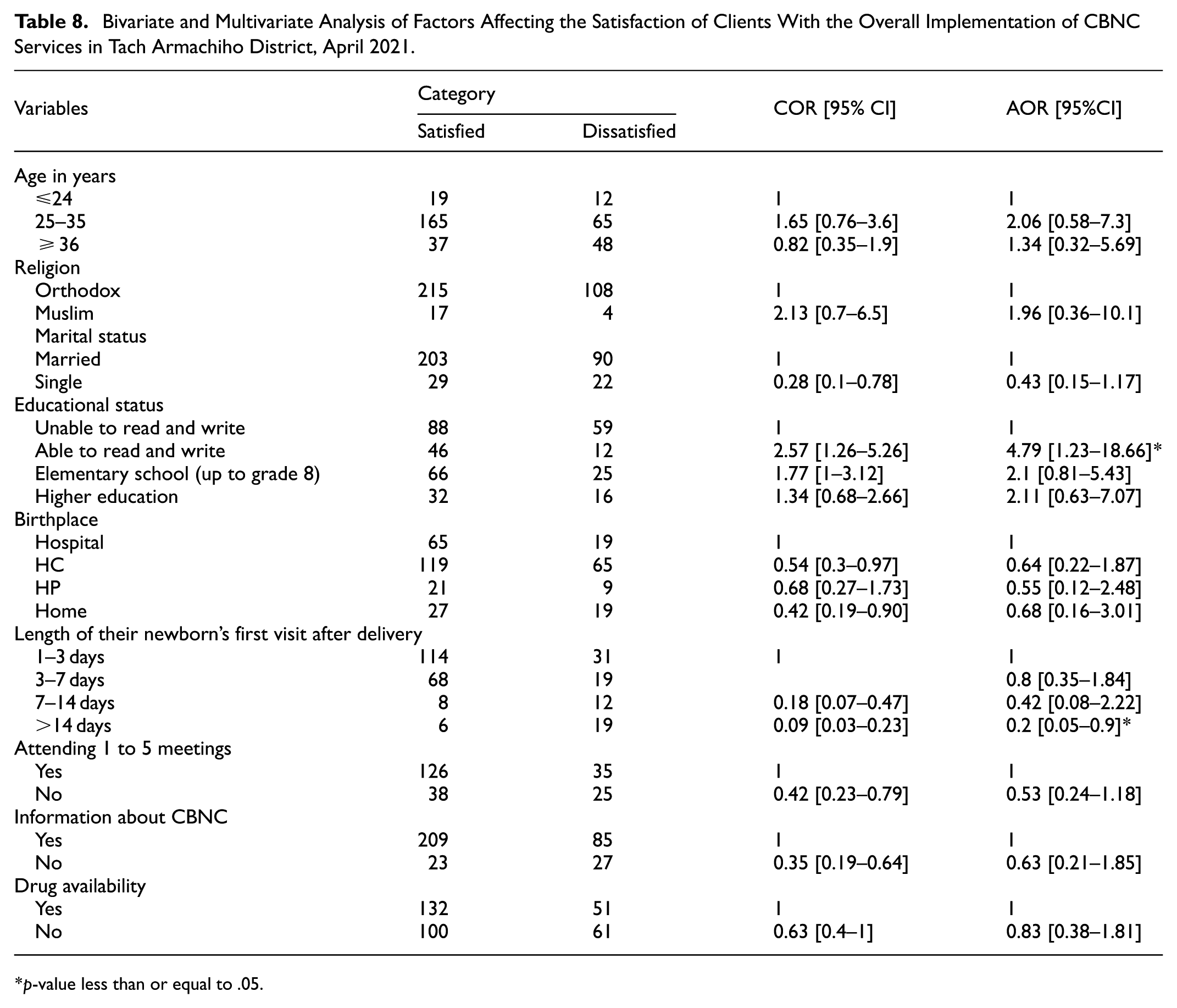
In the bivariate analysis, independent variables such as age, religion, marital status, educational status, place of birth, length of newborn first visit from delivery, post-natal visit, participating/attending 1 to 5, having information about CBNC, and convenient drug availability at health posts were candidates for multivariate analysis with a p-value ≤.25 (Table 8).
Bivariate and Multivariate Analysis of Factors Affecting the Satisfaction of Clients With the Overall Implementation of CBNC Services in Tach Armachiho District, April 2021.
p-value less than or equal to .05.
According to the judgment parameter, the overall satisfaction of caregivers was 61.69%, fair (Table 9).
Summary of Performance of Satisfaction Sub-Dimensions Indicators in Tach Armachiho District, April 2021.
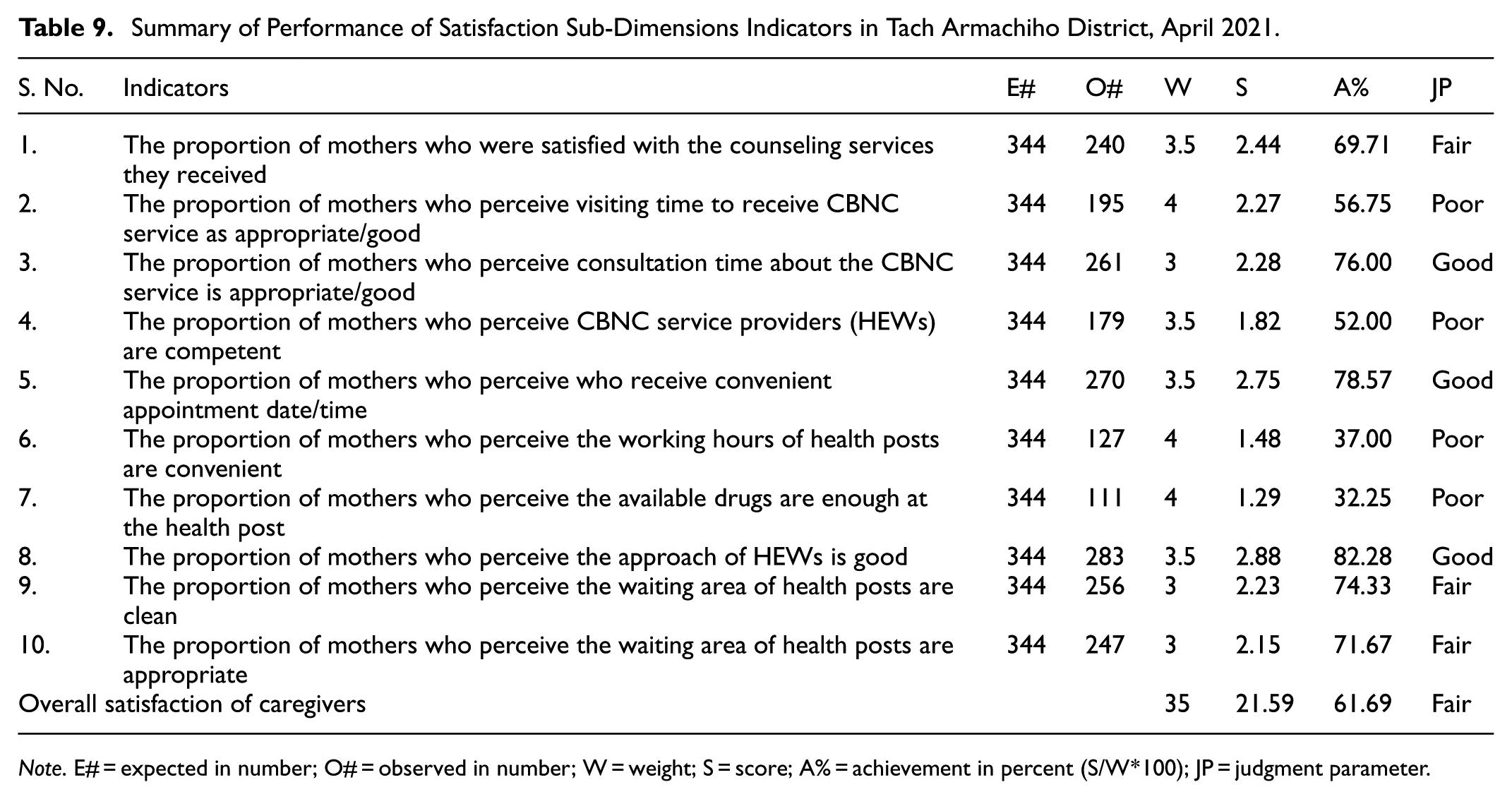
Note. E# = expected in number; O# = observed in number; W = weight; S = score; A% = achievement in percent (S/W*100); JP = judgment parameter.
Factors Associated With the Satisfaction of Mothers
The binary logistic regression model used both bivariate and multivariable regression analyses to identify characteristics related to caregiver satisfaction with CBNC services. Variables with a p-value <.25 from the bi-variable analysis were selected for the multivariable analysis.
During the multivariate analysis, educational status and the length of the newborn’s first visit after delivery were found to be substantially associated with caregiver satisfaction with the deployment of community-based newborn care services. As A result, mothers who could read and write were around five times more satisfied than mothers who couldn’t (AOR = 4.79, 95% CI: [1.23–18.66], p-value = .02). Furthermore, women whose newborns were visited beyond the 14th day were 80% less likely to be satisfied than mothers whose newborns were seen within 1 to 3 days of birth (AOR = 0.2, 95% CI: [0.05–0.9]) (Table 8).
In summary, the overall process of CBNC services was found to be 65.35% based on the weight given for each dimension of the process, which requires urgent improvement (Table 10).
Summary of Overall Performance Indicators of the Process of CBNC Services in HPs of Tach Armachiho District, April 2021.

Note. I# = number of indicators; E# = expected in number; RW = relative weight; S = score; A% = achievement in percent (S/W*100).
Discussion
The process of a community-based newborn care program implementation was evaluated in terms of availability, compliance, and caregiver satisfaction with CBNC service. The findings of this evaluation showed that the overall process of CBNC program implementation was 65.35%. This finding is less than what was reported in the research carried out in southern Ethiopia. The availability of resources, compliance of HEWs with national guidelines, and client satisfaction were 68.98%, 65.83%, and 67.44%, respectively. This finding may suggest that a lack of resources contributes to low HEW compliance and caregiver satisfaction.
The overall assessment of the availability of CBNC program resources was 68.98% and deemed fair. This result was lower than the study conducted in the Gezie Gofa district, southern Ethiopia, which discovered that program resources were available at 81% (Gebremedhin et al., 2019). This might be due to the current political instability issue in the study area and the COVID-19 outbreak during the data collection period of this evaluation.
The results of this evaluation showed that program resources such as dispersible amoxicillin, fetol (iron with folic acid), and syringes were entirely accessible in all health posts. This is in accordance with the WHO recommendation (World Health Organization, 2022) and research conducted in the Gezie Gofa district health posts of southern Ethiopia (Gebremedhin et al., 2019). In addition, surgical glove were available in all assessed health posts. This result was in line with the national guideline, but higher than the above-mentioned study in which was only available in 45% of HPs. Paracetamol suppository, on the other hand, has been stock out in all HPs for nearly a year, which is in contrast to a study conducted in Southern Ethiopia public health posts, where it was available in all HPs (Gebremedhin et al., 2019).
The results of this assessment indicated that the program supplies, such as gentamicin and examination gloves, were accessible in only 77.77% of health posts. This finding is lower than that of the study conducted in southern Ethiopia, in which 100% available. Chlorohexidine was available in 77.77% HPs, which is higher than the study conducted in southern Ethiopia, in which it was not available at all. In addition, TTC eye ointment was available in 55.55% of health posts, which is lower than the study conducted in southern Ethiopia, in which 100% available. Vitamin K was only accessible in 55.55% of health posts; however, this finding is greater than the study conducted in southern Ethiopia, which found it was stock out at all HPs for 6 months (Gebremedhin et al., 2019) and lower than the WHO recommendation (World Health Organization, 2022). These shortages might be caused by the absence of a partner supporting the program since 2018 G.C., as well as a lack of resupply of these pharmaceuticals and medical supplies from other sources, such as the zonal health department, district health offices, and catchment health centers, due to budget constraints.
In the Tach Armachiho district, there were also few trained human resources because the program’s training was interrupted due to a lack of budget and supporting partners. The qualitative results of the KII also revealed that finance was a significant barrier to supporting training in the district. Even if there are qualified HEWs in situ, there is no fulfillment of needed pharmaceuticals and medical supplies to deliver CBNC service, no refreshment training, and no regular program-specific supportive supervision and feedback.
In this evaluation, registration books for 0 to 2 months of age, service delivery reporting format, service delivery tally shits, weighing scale, and malnutrition assessment tape meter were available in all health posts, which is in line with the study conducted in southern Ethiopia (Gebremedhin et al., 2019) and higher than community-based interventions for newborns in Ethiopia, in which around 10% of HPs did not have the above-mentioned resources (Mathewos et al., 2017). This difference might be due to the study area; community-based intervention was conducted in a wider area of the country, but ours is at the district level.
Furthermore, the HDA team leader did not have a home-to-home service delivery registration book, a registration book for identifying pregnant mothers, or a referral form at any of the HPs. As a result, some pregnant mothers and referrals were not accurately recorded and reported. his aligns with the research carried out in southern Ethiopia (Gebremedhin et al., 2019). This finding is supported by the following qualitative result:
A 26-year-old HEW said that “due to a lack of a home-to-home service delivery registration book, we write services provided home-to-home on a piece of paper and lose it before reporting it.”
Based on the pre-set judgment criteria, this evaluation discovered that HEWs had an overall compliance rate of 65.83%, similar to the report in a study of southern Ethiopian public health posts (Gebremedhin et al., 2019). This review uncovered low performance in providing ANC1 and PNC, treating newborn sepsis cases, and identifying live births at the household level in the catchment area.
The result of this evaluation showed that 85.17% of respondents had heard about HDA, of which 76.45% of women were involved in women’s health development team membership, and 71.88% of them attended meetings frequently during their last pregnancy. This finding was higher than one obtained in Malawi, where only 34% of women reported knowing about a core group in their community and 9.6% got a home visit from a core group member during pregnancy (Callaghan-Koru et al., 2013). In addition, this finding is lower than that of a study in southern Ethiopia, in which 91.5% were aware of the Health Development Army (HDA), 86% were members, and 58% attended community meetings during their most recent pregnancy (Gebremedhin et al., 2019). This might indicate that the meeting’s interruption puts pregnant women at risk of missing ANC follow-up appointments.
Our research revealed that 59.72% of babies did not have their first postnatal visit within 48 hr by HEWs, which is lower than the study conducted in southern Ethiopia, where 65% of newborns did not receive their PNC within 48 hr after birth (Gebremedhin et al., 2019). The possible reason for this difference might be due to the revised postnatal care for mothers and newborn guidelines, which recommended the delay of facility discharge for at least 24 hr in turn gives the chance to get PNC visit.
This evaluation finding showed that all sick neonates with very severe disease were referred, of which 59.40% were given an initial dose of antibiotics, and 40.60% were referred without it. This result is less than the CBNC national guideline (Ethiopian Federal Ministry of Health & Tulane University’s Technical Assistance Program for Ethiopia, 2012) and ICCM treatment booklet chart for 0 to 2 months of age (Abtew et al., 2022), but, higher than the finding of a community-based intervention to reduce neonatal mortality in Bangladesh, which showed that 34% were referred successfully, 43% were treated by CHWs due to unsuccessful referral, 18% did not receive any outside care (49).
This evaluation finding is also higher than a study in Southern Ethiopia, which showed that 45.5% of sick neonates with very severe disease were referred with an initial dose of gentamicin and dispersible amoxicillin, 31.8% were referred without an initial dose, and 22.7% of VSD were treated at the health post level due to unsuccessful referral (Gebremedhin et al., 2019).
All assessed health posts obtained monthly-based follow-up and supervision from their corresponding catchment health center, although it is not program-specific, and there were interruptions in between. The zonal health department provided program-specific supportive supervision for two of the nine HPs, which is comparable with the findings of an evaluation done in southern Ethiopia. A quarter of nine HPs obtained supportive supervision related to the CBNC program from the zonal health department (Gebremedhin et al., 2019).
The result from the document review revealed that 84% of neonatal cases were correctly classified and treated according to the booklet chart, which is lower than that of the national guideline, which ordered to classify (diagnose) all cases based on signs and symptoms (Ethiopian Federal Ministry of Health & Tulane University’s Technical Assistance Program for Ethiopia, 2012).
This study attempts to measure the acceptability of the CBNC service by assessing caregivers’ satisfaction. Caregivers’ total satisfaction with CBNC services was found to be 67.44%, which is deemed fair and urgently needs to be improved. The result was less than that of a related study carried out in the southern Ethiopia, Gamo Gofa zone (75.05%; Gebremedhin et al., 2019), and a study conducted in Jimma zone public health facilities, in which client satisfaction with Emergency Obstetric and Newborn Care services (79.4%; Kumsa et al., 2016). The possible reasons for this difference might be due to the lack of availability of essential drugs, the working hours of HEWs to provide CBNC service, and the poor cleanliness of the HPs in our evaluation area compared to Gamo Gofa.
This finding was greater than the study conducted in Boloso Sore District, Southern Ethiopia (48.8%; Dargaso et al., 2019). This discrepancy might be due to the difference in study area, and there were a considerable number of participants had higher education in the Boloso district as the study suggests.
In this evaluation, the lowest satisfaction of caregivers with CBNC service was observed in the availability of drugs, the convenience of working hours of HEWs to provide CBNC service, and the convenience of the competency of HEWs, which were found to be 32.27%, 36.92%, and 52.03%, respectively. On the other hand, a higher level of caregiver satisfaction was observed in the approach of HEWs to caregivers; the appropriateness of appointment dates and the appropriateness of consultation times were found to be 82%, 78.5%, and 76%, respectively.
In this evaluation, 182 (52%) of mothers, whose newborns were visited in the first 7 days of birth, were satisfied. Still, only 6 (1.7%) of mothers, whose newborns were visited after 14 days of delivery, were satisfied.
Moreover, this study’s finding shows that educational status and the length of the first newborn visit after delivery were statistically associated with the satisfaction of caregivers. Accordingly, mothers who can read and write were nearly five times more satisfied than mothers who cannot read and write. This finding is consistent with studies conducted in Tigray (Weldeargeawi et al., 2020), the Boloso district in southern Ethiopia (Dargaso et al., 2019), Nepal (Bhatta & Aryal, 2015), South Asia, and sub-Saharan countries (Singh et al., 2016). This conclusion could be attributed to the fact that learning increases a woman’s knowledge and awareness of the necessity of services and the ability to obtain information. This finding also differs from the study conducted in mid-western Nepal, where illiterate postnatal mothers were 2.710 times more likely to be satisfied than those who were literate (Panth & Kafle, 2018).
In addition, mothers whose newborns’ first visits were after the 14th day were 80% less likely to be satisfied than mothers whose newborns’ first visits were within 1 to 3 days after delivery. The findings suggest a strong association between maternal satisfaction and timely postnatal visits, particularly within the first few days following birth. So, this study adds to the body of evidence already in existence and has obvious policy implications.
Generally, our findings showed issues in the availability and acceptability aspects of CBNC as viewed through the Access Framework. Likewise, the Implementation Fidelity framework describes how program implementation was affected by noncompliance with training and supervision requirements. The convergence of qualitative and quantitative evidence reinforces confidence in these interpretations.
Limitations of the Evaluation Study
Since the study was intended to evaluate and enhance a specific program in a specific situation, the results are context-specific and not generalizable. Because caregivers recalled events in retrospect, results may have been affected by potential recollection bias (e.g., timing of ANC/PNC visits, length of iron intake). Only mothers who had recently given birth were included to mitigate this, and skilled data collectors gave them enough time to remember. Although residual prejudice persists, social desirability bias—participants providing too positive responses to meet expectations—was mitigated by neutral questioning and confidentiality assurances. In order to reduce the impact of social desirability and the Hawthorne effect on observations in the facility, the first and last two observations were eliminated.
Conclusion and Recommendation
Based on the predetermined judgment criteria, the overall implementation process of the community-based newborn care (CBNC) program was rated as fair. Similarly, each evaluated dimension was also considered fair, indicating that while minimum service requirements were being met, substantial room for improvement remains.
Mothers’ educational status and the timing of their newborns’ first postnatal visit were identified as significant factors influencing mothers’ satisfaction. These findings suggest that both health-seeking behaviors and timely service delivery play a critical role in shaping community perceptions of community-based newborn care services.
Regarding essential drugs and medical supplies, dispersible amoxicillin, iron with folic acid, syringes with needles, surgical gloves, and weighing scales were available in all assessed health posts. Gentamycin, chlorhexidine, examination gloves, and gauze were available in all but two health posts. However, paracetamol suppositories, home-to-home service registration books, pregnancy identification registers, and women’s health development team referral forms were out of stock across all health posts. Furthermore, there were limited CBNC-trained health workers in health centers and at the district health office, and most health extension workers (HEWs) had been trained a considerable time ago.
In terms of service delivery, HEWs performed well in several core tasks, including asking about the age of sick neonates, identifying main problems, showing respect to caregivers, asking about postnatal care, measuring body temperature, and asking about vomiting and diarrhea. However, key assessments such as evaluating maternal and newborn HIV status, checking for jaundice, unconsciousness, and convulsions, as well as measuring infant weight, were frequently missed. Notably, there was no regular, program-specific supportive supervision in place.
These findings highlight critical areas requiring attention. Regular and program-specific supportive supervision, accompanied by constructive feedback, is essential to improve compliance with CBNC guidelines and sustain HEW motivation. Ensuring a continuous supply of essential medicines and logistics is necessary to prevent service interruptions and maintain community trust. Additionally, periodic refresher training for HEWs and health center staff is recommended to strengthen competencies, update skills, and address existing gaps in newborn and maternal care practices.
This study sheds light on the contextual and implementation factors that influence the performance of the community-based newborn care program. Future research could build on these findings by using longitudinal or mixed-method approaches to better understand the sustainability and long-term effects of such community-based interventions on newborn health. It would also be valuable to explore the perspectives and experiences of frontline health workers and community members to identify practical strategies that strengthen program ownership, improve supervision, and enhance integration within the broader health system. Comparative studies across different districts could further clarify how local contexts influence implementation fidelity and overall program success.
Footnotes
Acknowledgements
The authors are thankful to the University of Gondar, the Central Gondar zone health department, and the Tach Armachiho district health office. We also need to extend our gratitude to the data collectors, study participants, and supervisors.
Ethical Considerations
Ethical approval was obtained from the Ethical Review Committee of the Institute of Public Health, College of Medicine and Health Sciences, the University of Gondar with a reference number IPH/1481/2013. A letter of permission was obtained from the Central Gondar Zone Health Department.
Consent to Participate
After explaining the purpose of the study, we obtained written informed consent from study participants before the data collection process. Throughout the data collection procedure, the provided information was kept confidential.
Author Contributions
A.Y.B. and N.W. designed the study, developed data collection tools, performed the analysis and interpretation of data, and drafted the manuscript. G.A.A. and W.D.N. participated in the acquisition, the preparation of the evaluation proposal, trained data collectors, managed the data collection procedure, and revised the manuscript. All authors reviewed, revised, agreed, and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data are incorporated in the manuscript and the corresponding author will make the data available upon reasonable request.