
Abstract
With the growing demand for rehabilitation services, particularly in the post-COVID-19 era, novice rehabilitation physicians face increasing complexity in constructing their professional identities. This study employs ecological systems theory to explore the multi-layered professional identity construction of novice rehabilitation physicians, using a single-case study of Dr. X. Data were collected over a 16-month period through retrospective interviews, ethnographic observations, and a digital portfolio, and analyzed thematically. The findings revealed that Dr. X’s professional identity is constructed by his personal attributes and self-reflection, which are continuously influenced by his family members, workplace relationships and patient care in the microsystem. In addition, interdisciplinary collaboration and role negotiation in the mesosystem, and institutional expectations and societal norms in the macrosystem further construct his evolving professional role. From the chronosystem perspective, Dr. X’s identity construction unfolds dynamically over time, culminating in a confident, resilient, and collaborative rehabilitation physician. This study proposes an ecological model of novice rehabilitation physicians’ identity construction and offers valuable insights into professional development in rehabilitation medicine.
Plain Language Summary
After the COVID-19 pandemic, more people need rehabilitation treatment to recover from illness or injury. Novice rehabilitation physicians, who are just starting their careers, must learn not only medical skills but also how to see themselves as professionals in rehabilitation medicine. This study explores the journey of a novice rehabilitation physician, Dr. X, over 16 months. Retrospective interviews, ethnographic observations, and a digital portfolio were utilized to understand how his professional identity was constructed. This study found that his professional identity was shaped by personal qualities such as resilience, self-reflection, and values, as well as support and challenges from family, colleagues, and patients. Working with professionals from other medical areas, adjusting to workplace expectations, and responding to the society’s needs also played important roles. Over time, these experiences helped Dr. X become more confident, adaptable, and collaborative. The study presents a new model showing how different layers of a novice rehabilitation physician’s environment interact to influence his professional growth, offering insights for improving training in rehabilitation medicine.
Introduction
In recent years, rehabilitation medicine has gained significant attention due to its critical role in improving patient outcomes, particularly in the face of aging populations, chronic diseases, and post-acute care following severe illnesses like COVID-19 (Guaraldi et al., 2022). The post-pandemic landscape has further underscored the importance of rehabilitation, as millions of patients continue to experience complications from long COVID, requiring sustained, multidisciplinary care approaches (Rao & Dhamdhere-Rao, 2023). Rehabilitation physicians are crucial in supporting patients’ recovery, focusing on restoring functionality and improving quality of life (Warden & Bayley, 2020), while simultaneously facing new challenges. They must not only master technical skills, but also navigate evolving expectations from healthcare systems, patients, and interdisciplinary teams. The complexity of modern healthcare environments, combined with societal expectations for more personalized and holistic care, places additional pressure on novice rehabilitation physicians to construct an adaptable professional identity early in their careers. Therefore, it is essential to investigate how novice rehabilitation physicians develop their professional identities and what factors shape this process.
Although previous studies have examined professional identity construction in healthcare settings (Barrow & Xu, 2023; Venters et al., 2024), their focus is not exclusively on novice rehabilitation physicians. The rehabilitation medicine, a field that is distinct because of its collaborative nature and the long-term relationships rehabilitation physicians develop with patients (Singh et al., 2018). Novice rehabilitation physicians must acquire not only clinical expertise but also leadership, communication, and empathy, particularly as they work closely with nurses, attending doctors and social workers. Furthermore, with patient engagement recognized as a key determinant of successful rehabilitation outcomes (Jiang et al., 2025), emotional intelligence has become integral to professional identity construction. Despite these demands, little is known about how novice rehabilitation physicians make sense of their roles and form their professional identities within such a complex and evolving environment. The ecological perspective, though typically applied in language teaching and acquisition research (Zhao et al., 2024), shows significant potential to scrutinize the complex process involved in professional identity construction among novice rehabilitation physicians. It is rooted in Bronfenbrenner’s (1979) ecological systems theory, which emphasizes that human development takes place within a complex system of relationships influenced by multiple environmental layers. While this theory has not yet been widely adopted in rehabilitation medicine, it provides a valuable framework for understanding how the professional identities of novice rehabilitation physicians are shaped by interactions occurring at different ecological levels.
In all, this study adopts an ecological perspective to investigate how novice rehabilitation physicians construct their professional identities, with particular attention to the social, institutional, and cultural factors that might shape this process across multiple environmental levels.
Literature Review
Professional Identity Construction in Healthcare
A well-formed professional identity helps healthcare professionals maintain resilience, adapt to diverse clinical environments, and provide high-quality patient care (Lewis et al., 2023). Especially for physicians who are expected to adapt to diverse clinical environments and interact with patients, colleagues, and institutions in ways that influence their professional development.
Previous research has primarily focused on professional identity construction among medical students (Sarraf-Yazdi et al., 2021), general physicians (Hill et al., 2021), and nursing professionals (Philippa et al., 2021). Professional identity construction is understood as a continuous process shaped by the interplay between personal experiences, training, and professional expectations (Caza & Creary, 2016). Existing research has explored the factors influencing professional identity construction across different medical specialties. In general medicine, mentorship from senior physicians plays a crucial role in shaping the professional identities of novice doctors, with clinical experiences challenging them to develop resilience and adaptability (Cruess et al., 2016). In surgery, postgraduate surgeons described learning personal values or attitudes that they regarded as core to becoming a surgeon and key to professional identity construction (Cope et al., 2017). In nursing, the transition from education to practice requires novice nurses to reconcile theoretical learning with real-world patient care. The skills developed through problem-based learning equip novice nurses with the confidence to handle routine practice and unfamiliar situations (Arreciado Marañón & Isla Pera, 2015). While these fields share common elements in professional identity construction, they reflect the distinct professional cultures, skills, and demands of each specialty.
In rehabilitation medicine, while several studies have explored professional identity in rehabilitation professions (Mak et al., 2022; O'Brien et al., 2018; Takashima & Saeki, 2019), little is known about how the professional identity of novice rehabilitation physicians is constructed from the ecological perspective. Specifically, O'Brien et al. (2018), based on semi-structured interviews with 20 speech-language pathologists, found that working with assistants could be seen as a threat to speech-language pathologists’ professional identity, as it challenged their values and uniqueness. Takashima and Saeki (2019), through semi-structured interviews with 30 occupational therapists, further identified three distinct internal structures of professional identity. The first type centered on therapists’ knowledge and technical skills, while the second emphasized empathy toward their patients. The third type was characterized by flexibility, with therapists demonstrating the ability to switch between different approaches depending on the situation. Mak et al. (2022) conducted a systematic review on the professional identity in rehabilitation professions, revealing two key themes: conceptual descriptors (dynamic states and multiple identities) and influencing factors (person, professional education/environments, and profession-at-large). These studies suggest a lack of multi-dimensional, multi-level, and longitudinal investigations into professional identity within rehabilitation settings. In particular, research on novice rehabilitation physicians remains scarce. Operating in a multidisciplinary environment alongside nurses, attending doctors, and social workers, novice rehabilitation physicians may experience a unique identity construction process that differs from other medical specialties. Therefore, it is essential to investigate the ecological factors that shape their professional identities during the early stages of their careers.
The Role of Collaboration in Rehabilitation Medicine
Rehabilitation medicine is inherently interdisciplinary, which makes the role of collaboration central to the practice. Rehabilitation physicians must develop their identities while working alongside a wide array of specialists. Previous research has demonstrated the importance of interprofessional collaboration in long-term care and rehabilitation (Doornebosch et al., 2022), but it also places additional demands on novice rehabilitation professions (e.g., novice occupational therapists; Šuc et al., 2020). In addition, it is noted that successful interprofessional collaboration when caring for patients requires integration, understanding, and recognition of the interdependency from all persons involved, including patients and family caregivers (Doornebosch et al., 2022).
Studies concerning collaboration and teamwork with other health professions have been conducted in rehabilitation medicine (Babur & Liaqat, 2017; Singh et al., 2018; Törnudd et al., 2024). Babur and Liaqat (2017) investigated interprofessional collaboration among rehabilitation professionals in stroke rehabilitation using a structured questionnaire. Their study emphasized that while the benefits of interprofessional collaboration are undeniable in developing countries, the development of multidisciplinary teams still faces numerous barriers. Singh et al. (2018) reviewed the role of interdisciplinary teams in physical and rehabilitation medicine, examining the evidence supporting the benefits of interdisciplinary teamwork and its recommendation in rehabilitation services. Törnudd et al. (2024), through semi-structured interviews with nurses (n = 9) and physicians (n = 8), further revealed that close and clear collaboration between nurses, physicians, physical therapists, and occupational therapists is a key factor in ensuring that rehabilitation interventions deliver the greatest possible benefit to patients. Despite this growing body of research, few studies have examined how novice rehabilitation physicians construct their professional identity from the ecological perspective while working within interdisciplinary teams.
Furthermore, rehabilitation physicians are often caught between the desire to assert their clinical authority and the necessity of relying on the expertise of their interdisciplinary colleagues (Kraft et al., 2014). This balancing act might influence how novice rehabilitation physicians perceive their own professional identity—whether they see themselves primarily as leaders, coordinators, or partners within a larger team. Thus, examining how novice rehabilitation physicians navigate collaborative dynamics offers valuable insights into the processes of identity negotiation and construction in early professional development. From the ecological perspective, their identity construction is not only shaped by individual aspirations or competencies but also by the complex interplay of institutional expectations, team structures, and patient needs. Understanding this relational and context-dependent process may inform the design of support systems, mentorship models, and interprofessional training programs that foster both collaborative competence and a stable sense of professional self among novice rehabilitation physicians.
Ecological Systems Theory in Professional Development
Ecological systems theory, originally developed by Bronfenbrenner (1979), provides a comprehensive framework for understanding human development within the context of multiple environmental layers. It emphasizes that individual development is influenced by the interactions between a person and the various environments they engage with, ranging from immediate social settings to broader cultural and institutional structures. This study further adopts the chronosystem from Bronfenbrenner’s (2005) bioecological systems model to explore how individuals’ interpretations of events over time influence the construction and ongoing development of their professional identity.
For novice rehabilitation physicians, ecological systems theory offers valuable insights into how their professional identity is constructed. Identity construction is not a singular, linear process but is instead influenced by several interdependent systems. Adapted to the context of rehabilitation medicine, the model (see Figure 1) depicts a series of concentric circles representing different levels of systems: microsystem, mesosystem, and macrosystem. The influence of life events over time is captured by the chronosystem. (1) Microsystem: The microsystem encompasses the immediate environment in which the novice rehabilitation physician operates, including direct interactions with family members, patients, colleagues, and mentors. These everyday interactions occur within home, or hospital ward. (2) Mesosystem: The mesosystem consists of the connections and interactions between multiple microsystems in which the individual is involved. For novice rehabilitation physicians, this includes interdisciplinary collaboration with other healthcare professionals, communication and coordination across teams, and navigating role expectations within the team. (3) Macrosystem: The macrosystem refers to the broader cultural, societal, and institutional or organizational forces that shape professional expectations and values. Within rehabilitation medicine, the societal perception, the growing demand for holistic patient care, and the push toward personalized medicine all contribute to the expectations placed on novice rehabilitation physicians. (4) Chronosystem: The chronosystem captures temporal changes and the evolving nature of identity construction, emphasizing how individuals’ experiences and professional identities develop and transform over time. For novice rehabilitation physicians, exploring how their professional identity evolves over time, from the moment they begin their careers to 1 year later and beyond, is essential to understanding the dynamic process of identity construction.

Bronfenbrenner’s (1979, 2005) ecological model.
The ecological systems theory provides a powerful framework for systematically examining the complexity of professional identity construction among novice rehabilitation physicians. It highlights that identity is not constructed in isolation but through continuous interactions within a broader ecological network (Härkönen, 2001). Each of these systems plays a pivotal role in shaping how novice rehabilitation physicians perceive their roles and responsibilities, collaborate with colleagues, and ultimately define their professional identities.
Methodology
Research Design
This study aims to explore the process of professional identity construction among novice rehabilitation physicians, as well as the influencing factors at different ecological levels. To gain deeper insight into this process from an ecological perspective, a single-case study approach was adopted (Stake, 1995). Yin (2018) suggests that “single-case studies can be invaluable when the single case has any of five characteristics—being a critical, extreme or unusual, common, revelatory, or longitudinal case” (p. 24). Although this approach does not ensure the generalizability of the findings, it provides an ideal tool for investigating a phenomenon within its specific context (Baxter & Jack, 2008). In addition, single-case studies have also been recognized as effective in exploring identity construction in fields such as education (Özkaynak, 2025) and medicine (Curtis & Morris, 2015). Thus, Dr. X (pseudonym), a novice rehabilitation physician, was selected as the focal case. This study addresses the following research questions:
(1) What factors influence the professional identity construction of Dr. X across different ecological systems?
(2) How does the professional identity of Dr. X evolve over time from the beginning of clinical practice?
Research Participant
The participant of this single-case study is Dr. X, a novice rehabilitation physician working at a tertiary hospital in Henan Province, China. He earned a degree in rehabilitation medicine from a local university in June 2021 and began working in the rehabilitation department of a public hospital in his hometown in December 2022. The first author and Dr. X have been classmates since middle school and have maintained continuous contact since then.
Dr. X was selected through purposive sampling (Campbell et al., 2020). Through in-depth conversations with him, it was found that his experiences align with the typical challenges encountered by early-career rehabilitation physicians, such as navigating complex medical environments, managing interprofessional collaboration, and responding to diverse patient expectations. These experiences suggest that his case offers valuable insights into the professional identity construction of novice rehabilitation physicians in similar contexts. With Dr. X’s consent, the research was initiated.
Data Collection
Data collection was conducted over one and a half years (June 2023 to October 2024), a period identified through initial observations and in-depth conversations with Dr. X as a critical stage in his professional identity construction as a novice rehabilitation physician. To ensure the research reliability of the study through method triangulation (Heale & Forbes, 2013), three primary qualitative data sources were employed: retrospective interviews, ethnographic observations, and a digital portfolio.
The retrospective interviews consisted of six in-depth semi-structured sessions, totaling approximately 360 min, focusing on Dr. X’s negotiation of his professional identity, challenges, and interactions within the rehabilitation setting. All interviews were transcribed, resulting in approximately 52,000 words of textual data. Then, ethnographic observations were conducted on six separate occasions, accumulating around 50 hr of observation time. During these sessions, Dr. X’s interactions with patients and colleagues would be documented, along with his engagement in team meetings and other professional activities, resulting in approximately 6,000 words of field notes. Additionally, a digital portfolio was maintained by Dr. X, incorporating personal reflections recorded on his mobile device, case summaries and treatment notes prepared for departmental discussions, and screenshots of professional interactions and achievements shared via WeChat Moments, which may offer a multidimensional exploration of his evolving identity as a rehabilitation physician.
Data Analyses
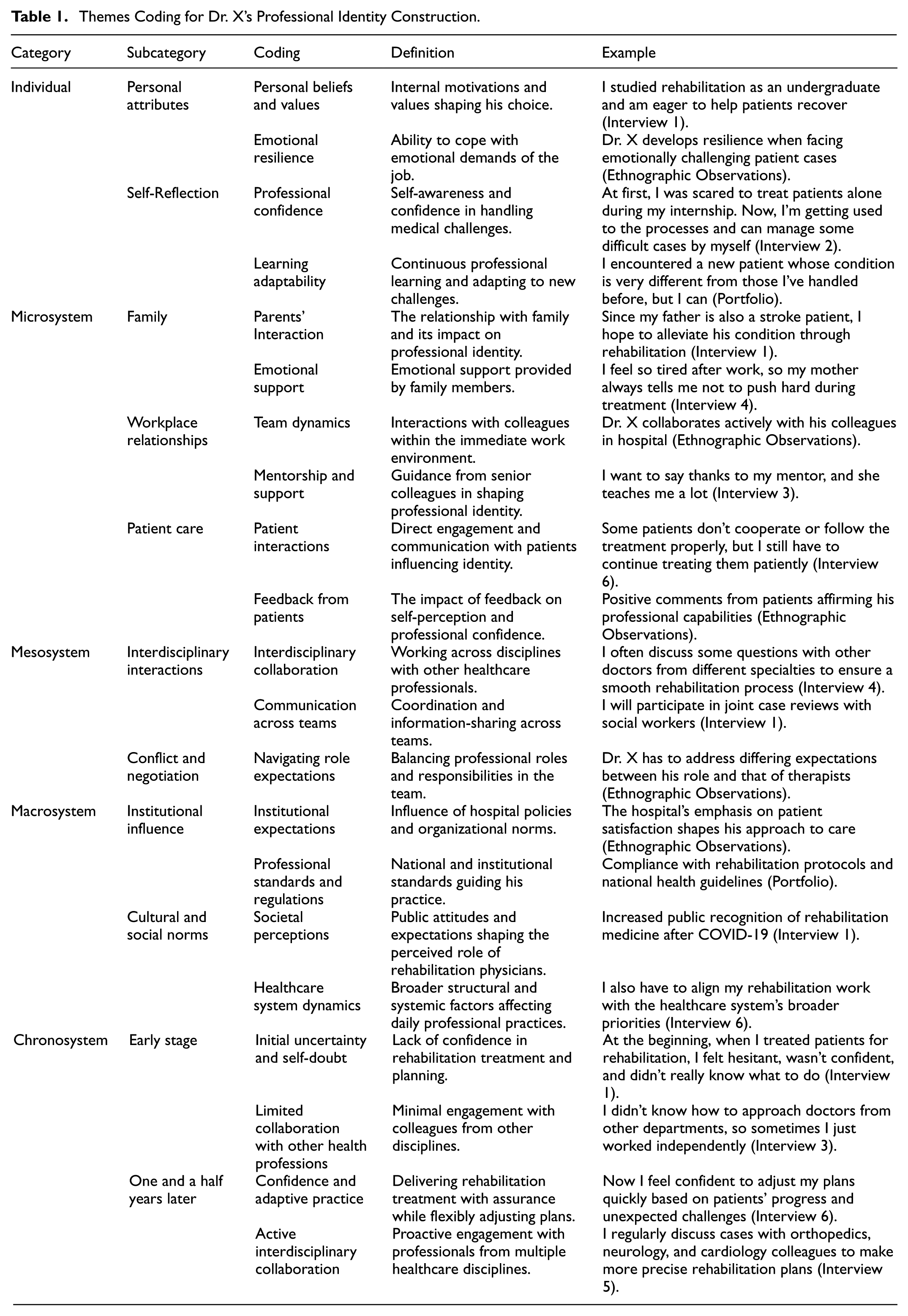
Grounded in the ecological framework, the first author analyzed the transcribed interviews and observational notes by employing thematic analysis (Braun & Clarke, 2006). It is particularly suited to exploring the layered and dynamic interactions between individuals and their environments, which aligns well with the ecological perspective central to this study. Thematic analysis was conducted using Nvivo 14.0 software, following Braun and Clarke’s (2006) six-phase analytical framework: (a) familiarizing with data; (b) generating initial codes; (c) searching for themes; (d) reviewing themes; (e) defining and naming themes; and (f) producing the report. The initial coding process categorized the data into preliminary themes such as “personal beliefs and values,”“parents’ interaction,”“Interdisciplinary collaboration,”“institutional expectations.” Through iterative rounds of analysis, observation, and reflection, these were further condensed and refined. Ultimately, the final analysis distilled Dr. X’s identity construction process into five thematic categories based on the ecological perspective (see Table 1).
Themes Coding for Dr. X’s Professional Identity Construction.
To ensure analytical rigor, member checking (Lincoln & Guba, 1985) was conducted. The second author, with extensive qualitative research experience, independently reviewed a subset of the coded data. Any discrepancies in coding were discussed collaboratively until consensus was reached, enhancing the confirmability and reliability of the findings.
Trustworthiness and Reflexivity
This study complies with the principles of trustworthiness as outlined by Lincoln and Guba (1985), including credibility, dependability, transferability, and confirmability. To establish credibility, the first author leveraged a background in clinical linguistics to engage in prolonged and in-depth interaction with the participant. This not only facilitated the establishment of rapport during interviews but also enabled a deeper understanding of the clinical context of the participant. Additionally, data source triangulation was employed by collecting information from multiple perspectives, ensuring breadth and diversity in the study’s data.
Dependability was addressed through method triangulation, incorporating retrospective interviews, ethnographic observations and a digital portfolio to provide a comprehensive understanding of the participant’s professional identity construction as a novice rehabilitation physician. To strengthen transferability, the study offers rich, thick descriptions of the contextual setting and participant experiences, allowing readers to assess the applicability of the findings to other similar contexts. Purposive sampling was employed to select a participant whose experiences aligned closely with the study’s focus, and the resulting dataset illuminated salient factors in the identity construction of novice rehabilitation physicians. Confirmability was safeguarded by the second author’s active involvement in data analysis. Collaborative discussions between both authors throughout the analytic process helped to ensure that themes were grounded in the data and not unduly shaped by individual preconceptions.
Reflexivity was integral to this study. Although the first author was not a member of the field of rehabilitation medicine, the clinical linguistics background offered a foundation for understanding the professional context while also encouraging critical awareness of personal assumptions. To this end, the first author maintained a reflexive journal throughout the research process to record assumptions, emotional responses, and potential influences on data collection and analysis.
Ethical Considerations
The research participant was informed of the purpose of the study and provided written informed consent prior to participation. To protect his privacy, all identifying information was removed, and a pseudonym (X) was used in the reporting. In addition, this study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Shandong University.
Results
This section presents the findings from the single-case study of Dr. X, a novice rehabilitation physician, highlighting the multi-layered factors that influence his professional identity construction through the ecological perspective. The results include five key thematic categories in Table 1.
Personal Attributes and Self-Reflection
At the core of Dr. X’s professional identity construction are his personal beliefs and values, which provide internal motivation for choosing rehabilitation medicine and sustaining his commitment to patient care. As noted in interview 1, Dr. X expressed a deep personal drive rooted in altruism and professional purpose.
I studied rehabilitation as an undergraduate and am eager to help patients recover (Interview 1). Dr. X develops resilience when facing emotionally challenging patient cases. He adjusted the treatment plan calmly and offered encouragement instead of showing frustration to his patients (Ethnographic Observations).
Closely intertwined with these beliefs is Dr. X’s emotional resilience, which enables him to cope with the emotional challenges inherent in rehabilitation practice. This resilience acts as a crucial bridge between his personal motivations and the demanding realities of the profession. Ethnographic observations demonstrated how Dr. X develops resilience when managing emotionally difficult cases, allowing him to persist and maintain professional commitment. His personal beliefs and values, and emotional resilience together form the foundation of his personal attributes as a novice rehabilitation.
Dr. X’s professional identity is further constructed through self-reflection, which helps him build confidence in handling challenges during rehabilitation treatment. He expressed this in the following excerpt from Interview 2. Over time, his reflective practice enables him to evaluate his own performance, recognize progress, and identify areas for improvement.
At first, I was scared to treat patients alone during my internship. Now, I’m getting used to the processes and can manage some difficult cases by myself (Interview 2). I encountered a new patient whose condition is very different from those I’ve handled before, but I can approach it methodically and consult with colleagues if needed (Digital Portfolio).
In parallel, Dr. X exhibits strong learning adaptability, showing readiness to acquire new knowledge and adjust to unfamiliar situations. He documented in a note on his phone that he encountered a new patient with a condition very different from those he had previously managed but successfully handled the case and shared the note with the first author. This adaptability ensures that Dr. X can respond effectively to the varied and complex nature of rehabilitation treatment (Stockley & Graham, 2023). Taken together, professional confidence and learning adaptability illustrate how self-reflection functions as a mechanism for Dr. X to continuously refine his practice, adapt to evolving demands, and construct his professional identity.
Dr. X’s professional identity is fundamentally constructed by an “inner compass” composed of his personal beliefs, emotional resilience, and reflective practice. These elements collectively empower him to navigate the complexities of rehabilitation treatment, fostering ongoing growth and adaptation. This internal guidance system not only sustains his motivation and confidence but also enables him to respond effectively to professional challenges.
Family, Workplace, and Patient Care
Dr. X’s professional identity is constructed by multiple interactions within his immediate microsystem, which includes his family, workplace colleagues, mentors, and patients. These relationships collectively influence how he understands and negotiates his role as a rehabilitation physician. At the family level, Dr. X’s relationship with his father, who suffers from a stroke, deeply impacts his motivation to pursue rehabilitation medicine. As demonstrated in interview 1, this personal connection grounds his professional dedication.
Since my father is also a stroke patient, I hope to alleviate his condition through rehabilitation. At home, I often help my father with rehabilitation exercises to make his walking smoother (Interview 1). I feel so tired after work, so my mother always tells me not to push too hard during treatment. She comforts me by saying that it is okay to take things slowly and that I am already doing my best (Interview 4).
In addition, his mother’s reassurance functions as an emotional regulatory resource, helping him maintain functional coping strategies in high-pressure situations and reducing the risk of burnout. In short, the family offers both a moral anchor for his vocational motivation and tangible support for emotional recovery and self-care, thereby reinforcing his resilience as a novice rehabilitation physician.
Dr. X collaborates actively with his colleagues in the hospital, exchanging ideas and collaborating on patient care to improve rehabilitation treatment effectiveness (Ethnographic Observations). I want to say thanks to my mentor, and she teaches me a lot. Her patience and encouragement helped me overcome challenges and build confidence in rehabilitation treatment practice as a novice rehabilitation physician (Interview 3).
Within the workplace, Dr. X actively engages with his colleagues through regular collaboration and exchange of ideas, which enhances the effectiveness of rehabilitation treatments. Ethnographic observations demonstrate that these interactions foster a supportive professional environment conducive to knowledge sharing and problem-solving. Mentorship also plays a pivotal role in constructing his professional identity. As evidenced in interview 3, his mentor not only facilitates his rehabilitation skill development but also provides professional support, enabling Dr. X to navigate the uncertainties of early rehabilitation treatment practice and consolidate his professional identity.
Some patients don’t cooperate or follow the treatment properly, but I still have to continue treating them patiently, understanding that building trust takes time (Interview 6). Positive comments from patients affirming his professional capabilities (Ethnographic Observations).
Patient interactions form another crucial dimension of Dr. X’s microsystem, constructing both his clinical approach and self-perception as a novice rehabilitation physician. Such encounters, as described in interview 6, serve as important opportunities for Dr. X to cultivate patience, empathy, and interpersonal negotiation skills, which are essential for achieving long-term therapeutic success in rehabilitation medicine (Reynolds, 2004). Positive comments from patients recorded in ethnographic observations and the digital portfolio (e.g., a banner given to Dr. X by a patient to express gratitude, shared by him on WeChat Moments; see Figure 2) further validate the development of Dr. X’s rehabilitation treatment skills and professional confidence through patient interactions.

A patient presenting Dr. X with a banner to express gratitude; Dr. X is on the right (Digital Portfolio).
It is noted that family provides the foundation for motivation and emotional support, the workplace offers a socialization channel for acquiring professional norms and skills, and patient interactions serve as the immediate context for Dr X’s identity enactment and validation by patients. These three elements intertwine at the microsystem level, collectively shaping Dr. X’s pathway as a novice rehabilitation physician in transforming his personal beliefs into practical professional actions.
Interdisciplinary Dynamics
Interactions across different healthcare disciplines within the mesosystem contribute significantly to Dr. X’s professional identity construction as a novice rehabilitation physician by broadening his professional skills. Engaging with doctors, nurses, therapists, and social workers from various departments enables him to appreciate diverse perspectives and integrate multiple areas of expertise essential for comprehensive rehabilitation. Dr. X shared this experience in interview 4.
I often discuss some questions with other doctors from different specialties to ensure a smooth rehabilitation process. They come from departments such as orthopedics, neurology, and cardiology, and their expertise helps me better understand patients’ primary conditions, and develop more precise rehabilitation plans (Interview 4). I will participate in joint case reviews with social workers. They are usually non-hospital professionals from different communities, and through case discussions, they provide insights into patients’ living environments and available social resources, enabling me to better identify rehabilitation needs and improvement areas (Interview 1).
Furthermore, joint case reviews bring Dr. X an additional layer of understanding to patient care, as noted in interview 1. Insights into patients’ living environments and available community resources sharpen Dr. X’s ability to align rehabilitation goals with real-world constraints. Such interactions cultivate his cross-disciplinary communication skills essential for his identity construction as a novice rehabilitation physician.
Dr. X has to address differing expectations between his role and that of therapists (Ethnographic Observations).
At the same time, Dr. X faces challenges in aligning differing expectations between his role and those of other healthcare professionals. Navigating these professional boundaries and negotiating responsibilities helps him clarify his position within the broader rehabilitation team and strengthen his identity as a novice rehabilitation physician who can integrate diverse disciplinary perspectives into cohesive, patient-centered treatment plans. Through these interdisciplinary dynamics in the mesosystem, Dr. X’s professional identity as an adaptive and integrative rehabilitation physician is continuously constructed and refined.
Institutional and Societal Forces
Within the macrosystem, institutional policies, professional regulations, and broader cultural and social norms collectively frame Dr. X’s professional identity as a novice rehabilitation physician. At the institutional level, the hospital’s emphasis on patient satisfaction, as observed ethnographically, shapes his approach to rehabilitation treatment by reinforcing the importance of responsiveness, clear communication, and holistic care. National rehabilitation protocols and health guidelines, documented in his digital portfolio, further serve as formalized standards that structure his clinical decision-making and align his practice with evidence-based expectations.
The hospital’s emphasis on patient satisfaction shapes his approach to care, encouraging Dr.X to prioritize effective communication, empathy, and responsiveness to patients’ needs (Ethnographic Observations). At the same time, he ensures strict compliance with rehabilitation protocols and national health guidelines to maintain high standards of clinical practice(Digital Portfolio).
Cultural and social norms also influence Dr. X’s professional identity construction as a novice rehabilitation physician. In interview 1, he reflected that the increased public recognition of rehabilitation medicine after COVID-19 has elevated societal expectations for rehabilitation physicians, positioning his work within a broader narrative of recovery, making him more conscious of how his role is perceived beyond the hospital setting. Finally, structural forces of the healthcare system further influence his daily practice. As he described in interview 6, aligning rehabilitation work with broader system priorities requires him to consider policy goals alongside individual patient needs.
Increased public recognition of rehabilitation medicine after COVID-19 has heightened expectations for rehabilitation physicians in long-term patient recovery (Interview 1). I also have to align my rehabilitation work with the healthcare system’s broader priorities, including resource coordination and multidisciplinary service delivery (Interview 6).
In all, these macro-level forces define the parameters of Dr. X’s professional practice while shaping the values, priorities, and adaptive strategies that guide his growth as a novice rehabilitation physician.
Professional Identity Construction Over Time
Dr. X’s professional identity construction undergoes a clear developmental trajectory over the course of his first year and a half in rehabilitation treatment practice, demonstrating notable changes in confidence, interdisciplinary collaboration, and adaptability. This temporal dimension reflects how his self-perception and professional behaviors evolve through lived experience and ongoing learning. In the initial phase, Dr. X confronts a lack of confidence in delivering rehabilitation treatment and planning. As he recounts in interview 1, he felt hesitant and unsure when managing patient rehabilitation treatment independently.
At the beginning, when I treated patients for rehabilitation, I felt hesitant, wasn’t confident, and didn’t really know what to do (Interview 1). I didn’t know how to approach doctors from other departments, so sometimes I just worked independently (Interview 3).
This self-doubt also extends to his interactions with other healthcare professionals. He reports limited collaboration across disciplines, often working independently due to unfamiliarity with colleagues in other specialties. These early challenges highlight the difficulties he faced as a novice rehabilitation physician. After one and a half years of clinical experience, Dr. X’s narrative reveals substantial growth in his confidence and professional adaptability. He now approaches rehabilitation treatment with assurance, flexibly adjusting his plans based on patients’ progress and emerging challenges.
Now I feel confident to adjust my plans quickly based on patients’ progress and unexpected challenges (Interview 6). I regularly discuss cases with orthopedics, neurology, and cardiology colleagues to make more precise rehabilitation plans (Interview 5).
Furthermore, his interdisciplinary collaboration has become more active and deliberate. He regularly engages with colleagues from different departments to refine treatment plans, demonstrating an integrative approach to patient care. This progression reflects a maturing professional identity characterized by increased self-efficacy and a collaborative mindset, both essential for effective rehabilitation practice.
Discussion
This study identified key factors operating at different levels: the individual (personal attributes and self-reflection), the microsystem (family, workplace relationships and patient care), the mesosystem (interdisciplinary collaboration and role negotiation), and the macrosystem (institutional expectations and societal norms). In addition, the chronosystem was applied to trace how his professional identity was constructed across the early stage and one and a half years later. This section discusses how factors within each layer contribute to the construction of Dr. X’s professional identity, characterized by confidence, resilience, and collaboration, as depicted in Figure 3.

Dr. X’s professional identity construction model.
At the center of Dr. X’s professional identity construction are his personal attributes (i.e., personal beliefs and values, and emotional resilience) and self-reflection, partially consistent with previous studies (Cope et al., 2017; Cornett et al., 2023; Toubassi et al., 2023). At first, this study revealed that his personal beliefs and values act as a stable internal drive that motivates Dr. X’s dedication to rehabilitation medicine and patient care, echoing prior research emphasizing the role of intrinsic motivation and professional purpose in sustaining commitment among healthcare professionals (Karaferis et al., 2022). In addition, emotional resilience enables Dr. X to manage the emotional challenges of rehabilitation practice, such as slow patient progress and setbacks. Rather than merely serving as a protective factor against burnout, his resilience functions actively to adapt his clinical approach, consistent with previous studies that highlight resilience as an important coping resource (Fullerton et al., 2021). Finally, self-reflection plays a crucial role in shaping Dr. X’s professional growth by allowing him to critically evaluate his performance, build confidence, and develop learning adaptability. This ongoing reflective practice supports his ability to manage unfamiliar cases and continuously improve, demonstrating how self-reflection acts as an indispensable characteristic in improving practical competence (Ardelt & Grunwald, 2018).
Then, within Dr. X’s microsystem, his immediate interactions with family members, patients, colleagues, and mentors constitute the core setting where his professional identity takes shape. Consistent with Bronfenbrenner’s (1979) ecological systems theory, the microsystem provides the most direct and frequent social exchanges, where values, attitudes, and behaviors are continually negotiated and reinforced. Similar to previous studies on healthcare professionals (Kline et al., 2020; Mann & Gaufberg, 2016), these interactions function as both a source of support and a site of professional socialization. First, this study found that family relationships provide both personal motivation and emotional support. Dr. X’s father’s stroke experience strengthens his commitment to rehabilitation medicine, while his mother’s reassurance helps him manage fatigue and avoid overexertion. Such familial influences align with research showing that family contexts can construct healthcare professionals’ identity (Mao et al., 2021). Second, this study unveiled that workplace relationships, including collaboration with colleagues and mentorship from senior physicians, play a crucial role in skill development and socialization. Ethnographic Observations and interviews showed that active teamwork enhanced his collaborative capacity, while mentorship offered guidance in clinical reasoning and professional conduct, echoing previous research that emphasizes the value of supportive workplace networks for career growth (Cornett et al., 2023; Lockyer et al., 2016). Third, this study confirmed that patient interactions provide both challenges and affirmation. Managing uncooperative patients tested Dr. X’s patience and reinforced his commitment to compassionate care, while positive feedback from patients boosted his professional confidence. These findings reflect earlier research highlighting patient feedback as a potent factor in shaping self-perception and reinforcing professional identity (Mattick et al., 2019).
The mesosystem, situated at the intersection of the microsystem and macrosystem in the model, reflects Dr. X’s interdisciplinary collaboration, cross-team communication, and negotiation of professional roles. First, this study demonstrated that regular engagement with healthcare professionals from other specialties enables Dr. X to integrate diverse perspectives into rehabilitation planning, which not only improves patient outcomes but also broadens his understanding of his professional role. This finding confirms previous studies highlighting that interdisciplinary collaboration enhances clinical competence and fosters a more holistic professional identity among practitioners (Doornebosch et al., 2022; Törnudd et al., 2024). Second, effective communication across teams, such as joint case reviews with social workers, facilitates information sharing and coordinated care. These cross-team exchanges extend his professional network beyond the immediate rehabilitation unit, consistent with literature showing that cross-contextual communication strengthens role clarity and collaborative skills (Singh et al., 2018). Third, negotiating differing expectations with therapists encourages Dr. X to define and adjust his professional role, reflecting how role negotiation fosters professional growth (Šuc et al., 2020).
At the macrosystem level, institutional, cultural, and social factors construct Dr. X’s professional identity by framing the broader context in which his daily rehabilitation treatment practice occurs, consistent with previous research that underscores the significant impact of such macro-level forces on healthcare professionals’ identity construction (Barbour & Lammers, 2015; Obling, 2023). First, this study found that institutional expectations, such as the hospital’s emphasis on patient satisfaction, directly shape Dr. X’s approach to care, reinforcing patient-centered values. Ethnographic observations demonstrated how organizational priorities guide his clinical behaviors in alignment with hospital goals. Second, this study revealed that adherence to professional standards and national health guidelines ensures compliance and professional legitimacy. Dr. X’s portfolio documentation confirmed his commitment to rehabilitation protocols, echoing studies highlighting national regulation as a key factor in identity development (Caza & Creary, 2016; Warren & Braithwaite, 2020). Third, this study showed that cultural and social norms, including increased public recognition of rehabilitation medicine following COVID-19, have elevated the perceived role of rehabilitation physicians. Dr. X acknowledged this shift in societal expectations, which strengthens his professional identity and sense of purpose (Wong & Trollope-Kumar, 2014). Finally, it is noted that broader healthcare system dynamics require Dr. X to align his rehabilitation work with systemic priorities, balancing individual patient needs with public health goals. This systemic alignment reflects the macro-level influences identified in prior research as crucial for integrating personal and professional roles (Ackerhans et al., 2024; Kyratsis et al., 2017).
The chronosystem captures the temporal dimension of Dr. X’s professional identity construction. Early on, he experienced uncertainty and a lack of confidence in rehabilitation planning, working mostly independently due to limited interdisciplinary collaboration. Over time, particularly after about 18 months, his growing clinical exposure and accumulated experience enhanced his ability to make flexible treatment adjustments, seek and integrate feedback from colleagues in different specialties, and contribute meaningfully to joint case discussions. This evolution illustrates how the passage of time, coupled with sustained professional engagement, facilitates the shift from a novice toward a more confident and collaborative practitioner, echoing findings from previous studies on early-career healthcare professionals (St-Martin et al., 2015).
In the end, this study revealed that interactions occur across ecological layers. The macrosystem not only constructs Dr. X’s professional identity directly but also influences the meso- and microsystems. Specifically, the post-COVID societal recognition of rehabilitation medicine has heightened patient expectations, which in turn affects the feedback Dr. X receives from his mentor, who now stresses balancing technical competence with patient-centered communication. Similarly, institutional priorities on patient satisfaction influence interdisciplinary interactions, as physicians, nurses, and therapists across departments adopt comparable communication and care approaches, enabling more seamless cross-specialty collaboration. Through these pathways, broad institutional and societal forces are operationalized in daily mentorship, teamwork, and patient encounters. In addition, it is noticed that these interdisciplinary dynamics within the mesosystem also directly influence his daily interactions in the microsystem. For example, clearer role definitions and collaborative strategies developed through the mesosystem enhance Dr. X’s communication and teamwork with colleagues and patients. More importantly, his personal attributes and self-reflection form a reciprocal cycle that continuously reinforces his professional development. His personal beliefs and emotional resilience provide the motivation and strength needed to engage in reflective practice, while his ongoing self-reflection deepens his self-awareness and professional confidence, which in turn strengthens his emotional resilience. This interplay creates a feedback loop that supports his sustained learning, adaptation, and identity construction throughout his early career. Therefore, from an ecological perspective, this study constructs an ecological model of novice rehabilitation physicians’ professional identity construction and its core factors in Figure 3, based on an in-depth longitudinal investigation of Dr. X.
Conclusion
This study, framed within the ecological systems theory (Bronfenbrenner, 1979, 2005), illuminates the dynamic interplay of multiple systemic layers that collectively shape Dr. X’s evolving identity as a novice rehabilitation physician. Drawing on retrospective interviews, ethnographic observations, and a digital portfolio, the findings revealed that his identity was constructed by multi-layered interactions among individual level (personal attributes and self-reflection), microsystem (family, workplace relationships and patient care), mesosystem (interdisciplinary collaboration and role negotiation), and macrosystem (institutional expectations and societal norms). Then, the chronosystem was employed to detect his professional identity construction into a confident, resilient and collaborative rehabilitation physician over time. Overall, Dr. X’s professional identity construction as a novice rehabilitation physician is a continuous, complex and multi-layered process.
Theoretically, this study advances the understanding of professional identity construction by applying Bronfenbrenner’s (1979, 2005) ecological systems theory to the context of novice rehabilitation physicians. It highlights the complex, multi-layered, and temporal nature of identity construction, emphasizing the dynamic interplay between personal attributes and various social and institutional environments. This holistic perspective moves beyond isolated factors, providing a comprehensive lens to explore how novice healthcare professionals adapt and grow within their ecological contexts. Such insights can guide future research on professional development across diverse medical fields. Practically, the findings offer concrete implications for stakeholders involved in supporting novice rehabilitation physicians. Training programs should integrate structured reflective practice and resilience training, alongside opportunities for interdisciplinary collaboration, to strengthen the internal and external resources essential for identity growth. Hospital administrators are advised to establish formal mentorship systems that offer emotional support and professional guidance, while fostering environments conducive to cross-disciplinary communication and teamwork. Policymakers should ensure institutional policies promote patient-centered care and allow flexible role adaptation, enabling novice physicians to navigate complex healthcare demands effectively. Collectively, these measures can create a supportive ecosystem that facilitates novice rehabilitation physicians’ transition into confident, resilient, and collaborative professionals.
While these findings provide valuable insights, several limitations should be acknowledged. First, although single-case studies have been demonstrated to possess strong validity for in-depth exploration, multiple-case studies could provide broader perspectives and enhance generalizability. Therefore, future research could incorporate additional cases across diverse settings to identify new factors and further refine the ecological model of professional identity construction. Then, due to the limitation of the time frame, although this study conducted a 16-month longitudinal follow-up, professional identity construction is a long-term and dynamic process. Future research could extend the investigation period to explore more comprehensively the identity construction of novice rehabilitation physicians across different career stages and within evolving ecological contexts.
Footnotes
Acknowledgements
We would like to thank the participant who took part in this study.
Consent to Participate
The research participant was informed about the purpose and nature of the study, including his rights to confidentiality and the option to withdraw at any point. He agreed to participate in this study.
Informed Consent Statement
Informed consent was obtained from the participant involved in the study.
Author Contributions
Funding
This study has been supported by the scientific and technological innovation 2030 - the major project of the Brain Science and Brain-Inspired Intelligence Technology (2021ZD0200534).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.