
Abstract
Over the past decade, and in particular since the onset of the COVID-19 pandemic, increasing proportions of Canadian post-secondary students have reported experiencing symptoms of mental illnesses and psychological distress, including anxiety and depression. The present study aims to describe trends in self-reported anxiety and depression reported by students during the COVID-19 pandemic period of February 2021 to January/February 2023 and to assess whether there were significant differences in these outcomes between students and the general adult population. A secondary analysis of a repeated measures cross-sectional dataset collected by Mental Health Research Canada (MHRC) was conducted to assess self-reported symptoms of anxiety and depression using the GAD-7 and PHQ-9 scales. Generalized linear models were used to assess how the prevalence of mental health symptoms changed over time, stratified by students compared to the general population. Generally, the proportion of respondents who screened positive for anxiety or depression was higher among the student compared to the general population across time points. Female respondents also had higher average scores on both scales compared to male counterparts. Proportions screening positive for both anxiety and depression were not significantly different over time points. Findings suggest Canadian post-secondary students experience higher levels of anxiety and depression compared to the general population, with females and students scoring particularly high on mental health assessments. It highlights the need for further research on the ongoing impact of the COVID-19 pandemic on student mental health and the importance of continuing mental health assessments through future MHRC polling.
Plain Language Summary
This study looked at how anxiety and depression levels among Canadian college and university students have changed from February 2021 to early 2023 during the COVID-19 pandemic. It found that students generally reported higher levels of these mental health concerns compared to the general adult population, with there not being significant changes in scores over time. These results highlight the significant mental health challenges faced by students and the need for continued research and monitoring to understand and address these issues better.
Keywords
Background
Given that the majority of mental disorders have their onset between late adolescence and early adulthood, post-secondary students have been identified as an at-risk population for the development of mental health difficulties (Kessler et al., 2007). The majority of post-secondary students belong to the “emerging adulthood” age group (18–25 years), a period during which significant cognitive and psychosocial development takes place, increasing susceptibility to stressors and the development of mental illnesses (Arnett, 2000; Linden et al., 2022). Risky behaviors and maladaptive coping mechanisms are also common among this age group, encouraged by increases in autonomy and other lifestyle changes (Duffy et al., 2020; Gollust et al., 2008; Patel et al., 2007). Poor coping ability combined with ongoing exposure to stressors within the post-secondary environment can result in ongoing stress, which can contribute to the development of common mental illnesses such as anxiety and depression (Eisenberg et al., 2007; Patel et al., 2007), poor academic performance (Keyes et al., 2002), dropouts (Hjorth et al., 2016), burnout (Evans et al., 2018), and, in the most extreme cases, self-injury and suicidal ideation (Eisenberg et al., 2007). Anxiety and depression, in particular, are common mental health difficulties experienced by post-secondary students (American College Health Association, 2019; Esmaeelzadeh et al., 2018). In fact, data collected through the 2019 National College Health Assessment (NCHA II) revealed large proportions of students self-reporting “above average” to “extreme” stress (60%), “overwhelming anxiety” (69%), and feeling “so depressed it was difficult to function” (52%) within the past year (American College Health Association, 2019). Between the 2013 and 2019 iterations of the NCHA II, self-reported prevalence estimates for anxiety, depression, and other mental health outcomes significantly increased, providing evidence in support of considering student mental health to be a major public health concern (Linden, 2019). Anxiety disorders are characterized by excessive or uncontrollable worry, while mood disorders like depression are characterized by low mood, sadness, and feelings of hopelessness (American Psychiatric Association, 2022).
In 2019, the onset of the global COVID-19 pandemic introduced yet another layer of stressors for post-secondary students, including academic stressors associated with the mandatory shift to online learning (Yang, 2021), campus closures leading to isolation from campus and peers, disrupted academic and social activities, loneliness, and economic uncertainty related to employment and pandemic-associated expenses (Mental Health Research Canada, 2020). Following its onset, the spread of the virus and the associated public health measures (e.g., social distancing, isolation, and quarantine) had a significant impact on individuals’ lifestyles, work, academics, and plans for the future (Sahu, 2020). These abrupt changes and novel stressors increased the risk of mental health deterioration among all Canadians, particularly among already vulnerable emerging adults (Sahu, 2020). Existing, cross-sectional studies have suggested depression, anxiety, insomnia, and post-traumatic stress disorders among post-secondary students increased following the COVID-19 outbreak (Akiba et al., 2024; Arnett, 2000; Lorenzo et al., 2023; Moghimi et al., 2023; Watkins-Martin et al., 2021). Indeed, while the observed rates of anxiety, depression, and other mental health outcomes among post-secondary students appeared to be on par with the general population prior to the pandemic (Wiens et al., 2019), national, population-based data collected by Mental Health Research Canada (MHRC) throughout this unprecedented global event suggest that the emerging adult age group tended to experience higher rates of mental disorders such as anxiety and depression relative to others (Mental Health Research Canada, 2020). In fact, by February 2021, MHRC data had revealed the highest proportions of self-reported anxiety (25%) and depression (17%) reported among Canadians during the pandemic (Mental Health Research Canada, 2021). A significant reduction in these proportions was not observed until July 2022 (Mental Health Research Canada, 2022). Proportions stabilized near the end of 2022, with estimates around 10% and 8% for anxiety and depression, respectively (Mental Health Research Canada, 2023). Across all time points, the highest proportions of both anxiety and depression were observed among young, post-secondary-aged Canadians, who were also more likely to report feeling exhausted, burned out, and that they were not coping well with stress (Mental Health Research Canada, 2023).
Despite growing evidence of the pandemic’s impact on this population, to our knowledge, no published work has examined trends in self-reported anxiety and depression among Canadian post-secondary students compared to the general Canadian population over these 2 years of the pandemic using population-based data from all provinces. The majority of published research on this topic is made up of small, descriptive cross-sectional studies using samples with limited variability. Contributing to this gap in the literature is imperative to improving our understanding of how the pandemic has uniquely affected post-secondary students’ mental health. This knowledge may inform targeted interventions, policies, and support mechanisms to address the ongoing mental health crisis within this population as we navigate the post-pandemic period. By examining data collected over a substantial period of the pandemic (February 2021 to February 2023), this study aims to evaluate the evolving impact of the COVID-19 pandemic on post-secondary students’ mental health outcomes using a representative sample of participants from all 10 Canadian provinces. The results of this study will provide valuable insights that can be applied to a broad population of Canadian post-secondary students and aid in guiding directions for future research and the development of mental health interventions and supports in this area. This comparison between the general population and students across the same time frame will also help contextualize the mental health challenges faced by post-secondary students, enabling a more nuanced understanding of the pandemic’s impact and how best to support students moving forward.
Objectives
The objectives of this study were: (1) to describe trends in self-reported anxiety and depression reported by post-secondary students during the COVID-19 pandemic period of February 2021 to January/February 2023 and (2) to assess whether there were significant differences in these mental health outcomes during this time period between post-secondary students and members of the general adult population.
Methods
Data Source and Sample
We conducted a secondary analysis of a repeated measures cross-sectional dataset collected by Pollera Strategic Insights on behalf of Mental Health Research Canada (Mental Health Research Canada, 2020). This was a national polling effort intended to monitor the impacts of the COVID-19 pandemic on Canadians’ mental health and well-being. A random sample of Canadians over the age of 18 was selected to participate in the study, with demographic and regional quotas employed to improve the representativeness of the data to the broader Canadian population. Data was weighted by the most current gender, age, and region Census data, including participants from all 10 provinces (territories excluded). Online surveys were released roughly every 2 months beginning in April 2020, with polling ongoing to date. Participation was voluntary, and participants reserved the right to decline to respond to questions. No participation incentives were offered. For the present study, our focus was on self-reported symptoms of anxiety and depression as reported on the GAD-7 and PHQ-9 scales, respectively. As these scales were not included in the MHRC survey until Poll #5 (February 2021), data were included from this point until Poll #15, available in January/February 2023. Participants from the MHRC dataset were included in the present study if they (1) responded to a poll where the outcomes of interest were measured, and (2) belonged to one of the two populations of interest (identified as “students” or “employed” Canadians). To create our subsample, we filtered the dataset by responses to the employment status demographic question. Single response options included: employed part-time, employed full-time, self-employed, not employed, student, or retired. We extracted those who indicated “student” to create our student group and those who reported being “employed full-time” to create our comparison group representing members of the general Canadian population. We chose to exclude the remaining groups as we felt the full-time employment group would be the most comparable in terms of mental health outcomes and exposure to pandemic-related stressors such as disruptions to daily routines.
Measures
Demographics
To assess the nature of our sample, several demographics were evaluated: student/employment status, age, gender, total household income, region, visible minority status, ancestry/ethnic background, and LGBTQ+ status. Most demographic variables were categorical, with some continuous variables recoded for ease of presentation (e.g., age group, income status).
Mental Health Measures
To assess anxiety, the 7-item General Anxiety Disorder (GAD-7) scale was used. This widely validated tool is used to evaluate symptoms of anxiety and has continually demonstrated strong psychometric properties (Spitzer et al., 2006). Each item assesses the frequency of a specific symptom of anxiety. Response categories for each item range from 0 (not at all) to 3 (nearly every day) and are summed for a composite score ranging from 0 to 21, where higher scores indicate more severe levels of anxiety (Spitzer et al., 2006). Scores ≥10 are recommended as a clinical cut-off, indicating a positive screen for at least moderate anxiety (Spitzer et al., 2006). The GAD-7 has been extensively used among both adult and post-secondary populations (Byrd-Bredbenner et al., 2020).
The Patient Health Questionnaire (PHQ-9) is a nine-item scale used to assess symptoms of depression. The tool has high sensitivity (88%) and specificity (88%) and has been widely validated across multiple populations (Kroenke et al., 2001). Response categories for each item range from 0 (not at all) to 3 (nearly every day) and are summed for a composite score ranging from 0 to 27, where higher scores indicate more severe levels of depression. Scores ≥10 indicate a positive screen for at least moderate depression. Like the GAD-7, the PHQ-9 has been validated for use among both adult and post-secondary populations (Fonseca-Pedrero et al., 2023). For the purposes of analysis, both GAD-7 and PHQ-9 were recoded from continuous to dichotomous variables using the clinical cut-off point of scores ≥10. In addition, we also looked at whether participants reported having received a previous diagnosis for either anxiety or depression (yes/no), as well as the timing of that diagnosis (before/after the onset of the pandemic).
Analysis
Descriptive statistics were calculated for all demographic variables at each time point. For both the student and general population samples we calculated the proportion of respondents who screened positive for depression or anxiety, in addition to categorizing GAD-7 and PHQ-9 scores by severity using the recommended cut-offs. Data visualizations were created to display trends in positive screenings over time, stratified by gender and population of interest.
Generalized linear models were used to determine whether the rate of change for prevalence estimates differed significantly over the given time period for each of the two outcome variables (symptoms of anxiety and depression). Predictor variables included time point, gender, population (student or employed) age group and income groups. Baseline prevalence and the estimated change per wave, with associated confidence intervals were generated for anxiety and depression. All predictor variables were categorical in nature. Two separate models were used, one for each of the outcome variables.
Results
Demographics
A breakdown of the number of respondents at each time point (poll number) who indicated they were employed (overall n = 22,829) or a student (overall n = 2,817) is included in Supplemental Material. Table 1 presents the demographic characteristics for the subsamples used, stratified by gender. The majority of student respondents (67.5%) identified as female, while the employed sample was equally balanced between male and female respondents. Students (mean age of 21.93; SD = 6.52) were younger on average than the employed sample (mean age of 42.14; SD = 13.2). As expected, the vast majority of those in the student sample were in the emerging adulthood age group (82% 18–25 years). Household income varied between the samples, which was to be expected. The most prevalent income groups for the employed population were those above $50,000 per year. In contrast, the most common annual income reported in the student sample was $20,000. A large proportion of students also selected “Don’t know/unsure.” This lower income may reflect either the majority of students working lower-paying, part-time jobs, or intermittent jobs (e.g., seasonal work during the summer months). Regionally, the highest proportion of respondents indicated living in Ontario, followed closely by Quebec. There were no respondents from any of the territories in either group, but Respondents were included from each of the 10 Canadian provinces. A total of 17.2% of the student sample identified as part of the LGBTQ+ community, compared to 7.5% of the employed sample. In total, 25.4% of the student sample identified as a visible minority, compared to 17.3% of employed respondents. No respondents identified as Indigenous.
Demographic Characteristics for Student and General Population Subsamples, Stratified by Genderc.

Results presented as n (%).
Northern Territories were excluded from Mental Health Research Canada’s sampling frame.
64 students and 101 employed individuals indicated “other gender identity,” but cell counts were too small to include in subsequent analyses.
Mental Health Measures
The distributions of anxiety and depression scores per the recommended cut-offs (Kroenke et al., 2001; Spitzer et al., 2006) as well as means and standard deviations for overall scores are displayed in Table 2. The average score on the GAD-7 among the student sample was 7.05 (SD = 5.37), compared to the employed sample’s average score of 5.14 (SD = 5.13). Both scores fell within the “mild anxiety” cut-off category. This difference was statistically significant (t = −25.933, df = 2913.1, p < .05). Notably, nearly 30% of students reported a score above 10 (“moderate or severe anxiety”) compared to less than 20% of the employed sample. Similarly, the average PHQ-9 score among the student sample was 8.71 (SD = 6.63), compared to the employed sample’s average score of 6.25 (SD = 6.31) This difference was also statistically significant (t = −32.661, df = 2955.5, p < .05). As with anxiety, both scores fell within the “mild depressive symptoms” cut-off category. Nearly 40% of students experienced “moderate, moderately severe, or severe” depressive symptoms (scores >10), compared to 25.6% of the employed sample.
Descriptive Statistics for Mental Health Measures.

Results presented as n (%).
In total, 32.1% and 26.8% of student respondents reported they had received an anxiety or depression diagnosis, respectively. For both anxiety and depression diagnoses, about 9% were received after the onset of the pandemic. Among the employed sample, the proportion who reported receiving an anxiety or depression diagnosis was 26.3% and 31%, respectively, with 7% of diagnoses occurring after the onset of the pandemic.
Anxiety
Figure 1 shows the proportion of participants who scored positive for anxiety (i.e., scored ≥10 on the GAD-7) at each data collection point, stratified by both population of interest (i.e., student and general population) and gender. Shaded areas indicate the confidence intervals across time points. In both samples, larger proportions of female respondents met the clinical cut-off for anxiety compared to males over time. Estimates of the proportion of students experiencing both anxiety and depression are less precise than those for the employed sample due to the smaller sample size.

Proportion of participants who screened positive for anxiety at each time point in student and general population samples, stratified by gender.
In general, the proportion of respondents who screened positive for anxiety was higher among students compared to the general population across all time points. Further, the proportion screening positive for anxiety appears to be relatively consistent in both the student and general samples, until a visible dip in proportions around the eighth and ninth time points. After this point, proportions begin to increase again. However, the change observed may be statistical noise due to the small sample size.
Depression
Figure 2 displays the proportion of participants who scored positive for depression (i.e., scored ≥10 on the PHQ-9) at each data collection point, stratified by both population of interest (i.e., student or general population) and gender. Shaded areas indicate the confidence intervals across time points. In both the student and general populations, larger proportions of females met the clinical cut-off for depression compared to males over time.

Proportion of participants who screened positive for depression at each time point for student and general population samples, stratified by gender.
In general, the proportion of respondents who screened positive for anxiety was higher among students compared to the general population across all time points. Further, the proportion screening positive for anxiety appears to be relatively consistent in the student and general samples, with slight fluctuations over time. However, the change observed may be statistical noise due to the small sample size.
Multivariate Analyses
Table 3 displays the results of generalized linear models used to model the relationship between the binary outcome variables (screening positive for anxiety or depression, scoring ≥10 on the GAD-7 or PHQ-9, respectively) and the predictors of interest. The final models included an interaction between time point, gender, population, and age group and controlled for income group. Table 3 displays the results from the regression models for anxiety and depression by age, gender, and population, controlling for income. Baseline prevalence and change per time point are provided with 95% confidence intervals.
Results of Regression Models.
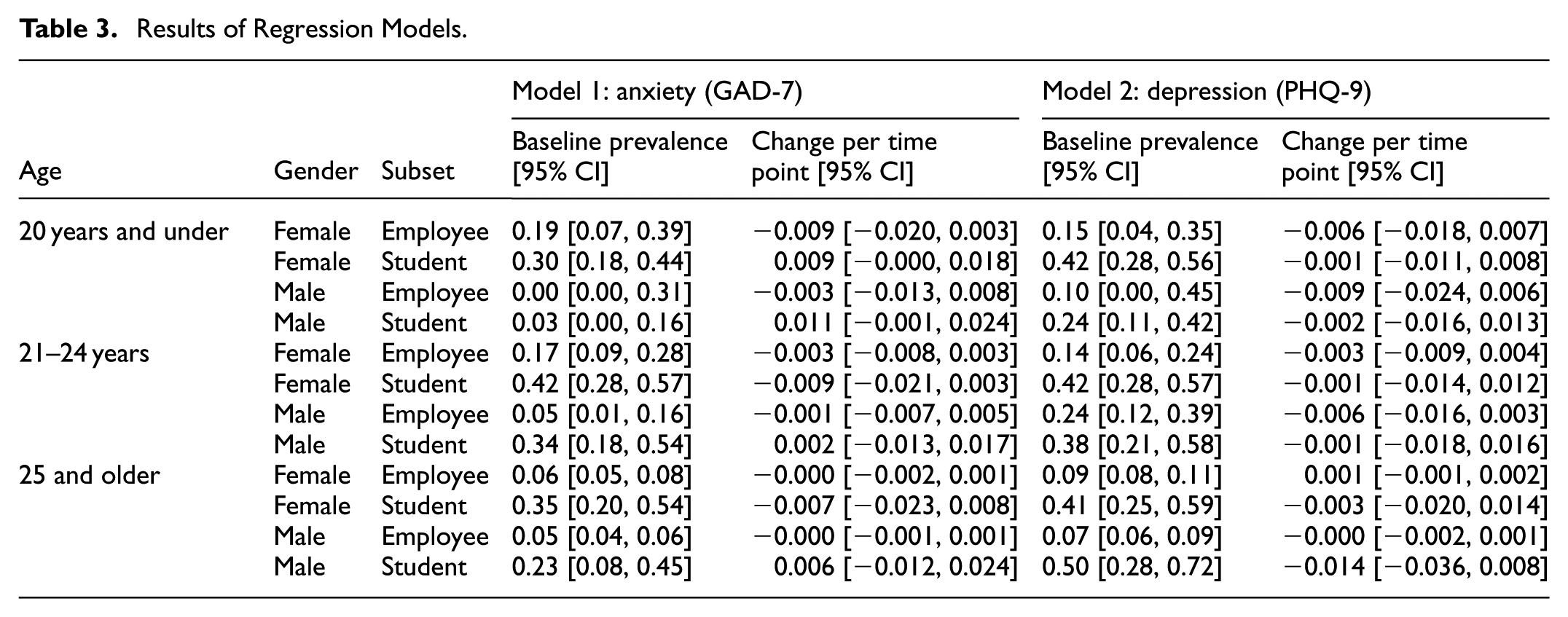
The student population had a higher baseline prevalence of both anxiety and depression compared to the general population, with higher prevalence estimates observed among younger age groups. Changes in proportions per time point were close to 0, indicating little change in the prevalence of anxiety and depression over the study period within age-gender-employment strata. Baseline prevalence was generally higher in the student population compared to the general population across age and gender strata and was consistently higher among females compared to males.
Discussion
Over the past decade, increasing proportions of Canadian post-secondary students have reported symptoms of mental illnesses such as anxiety and depression, with substantial increases observed among this age group over the course of the COVID-19 pandemic (Appleby et al., 2022; Dubale et al., 2024). Alongside these self-reported estimates, post-secondary institutions have reported an increased burden of care, with more students than ever seeking mental health support (Lipson et al., 2019; McGartland-Kinsella, 2013) such that the demand for services is outpacing institutions’ ability to provide timely care and inflated caseloads contributing to increased counselor burnout and turnover (Jaworska et al., 2016; Linden et al., 2021). Additionally, many institutions report increases in the proportion of incoming undergraduate students with pre-existing mental illnesses in need of continued support, further contributing to the bottleneck in service provision (McGartland-Kinsella, 2013). Previous studies have indicated that mental health problems, such as depression, anxiety, insomnia, and post-traumatic stress disorder, significantly increased following the COVID-19 outbreak (Appleby et al., 2022; Lorenzo et al., 2023; Watkins-Martin et al., 2021). However, the majority of published studies are small in scope (Dubale et al., 2024; Lorenzo et al., 2023; Moghimi et al., 2023; Nwachukwu et al., 2020; Turna et al., 2021), focusing on a specific type of stress or student sub-population (Akiba et al., 2024), are cross-sectional, do not use a comparison group, or focus on a brief point in time during the early pandemic (Vigo et al., 2021; Watkins-Martin et al., 2021). In comparison, this study successfully compared trends in student mental health outcomes to those observed among members of the general Canadian population over a 2-year period during the pandemic, using a large, national sample, thereby contributing to existing gaps in the literature.
In the present study, we found that the proportion of students screening positive for anxiety and/or depression did not change significantly over time but remained consistently higher compared to prevalence estimates observed among the general population throughout the study period. The impact of gender was also clear, with the proportion of female students screening positive for anxiety and/or depression significantly higher than that among males, which is consistent with existing literature. Similarly, higher prevalence estimates were consistently observed among younger age groups in both the student and general population samples.
Although change over time was not significant in this study, it is important to note that about one-quarter of students in this sample met the clinical cut-off for anxiety and/or depression, with these proportions remaining constant over the first year of the pandemic and beyond. Screening positive on either of these validated measures suggests that an individual has met the threshold for a clinical diagnosis and may require psychiatric support, such as counseling or pharmacotherapy. Screening positive on either measure suggests a likely need for formal psychiatric intervention—something many institutions are currently unequipped to provide at scale. With post-secondary institutions already reporting a demand for services that outpaces their ability to provide timely care to all who require it (Jaworska et al., 2016), this substantial prevalence of anxiety and depressive disorders among the student population is cause for concern.
The findings from this study can be interpreted through the lens of the diathesis-stress model, which argues that psychological distress emerges when individual vulnerabilities interact with significant environmental stressors (Goforth et al., 2011). In this case, abrupt changes that resulted from the pandemic, including the transition to online learning, social isolation, financial uncertainty, and concern over academic futures, likely functioned as acute stressors that overwhelmed students’ coping capacities. From an ecological systems perspective (Eriksson et al., 2018), the pandemic disrupted students’ environments at multiple levels, including the institutional (e.g., peer and faculty relationships), individual (e.g., school-home dynamics), and societal (e.g., public health mandates and economic pressures). Stressors and overall uncertainty emerging at all levels is likely to have compounded stress and eroded protective factors, such as typical coping mechanisms that students might have turned to in normal circumstances. In keeping with this, the Transactional Model of Stress and Coping (Biggs et al., 2017) highlights the role of individual appraisals in shaping stress responses. Students who perceived pandemic-related challenges as exceeding their usual coping resources (or alternatively, those who found themselves unable to access coping resources due to campus closures and stay-at-home orders) may have experienced higher psychological distress. Additional studies conducted in Canadian contexts have identified similar, increased mental health challenges during this pandemic period among other populations, particularly equity-deserving groups, underscoring the need for responsive, upstream mental health strategies on campus (El-Gabalawy & Sommer, 2021; Gibson et al., 2021; Jenkins et al., 2022).
In light of these findings, post-secondary institutions should prioritize upstream, system-level responses to address the sustained mental health burden among Canadian university students. Key strategies include expanding mental health services, embedding mental health literacy into academic life, offering flexible academic accommodations, strengthening peer support programs, and fostering stronger partnerships between campuses and community-based services. These efforts must be guided by a commitment to equity and consideration of the broader social determinants of mental health. Suggested next steps include conducting longitudinal research to monitor student mental health trends over time, examining regional and demographic variations, and evaluating the effectiveness of existing and emerging mental health supports within the post-secondary education system.
Strengths and Limitations
In this study, we evaluated both anxiety and depression using a large, nationwide sample of post-secondary students using valid and reliable measures. Our analysis covered a 2-year period during the height of the COVID-19 pandemic, with data collected from February 2021 to January/February 2023, evaluating prevalence estimates for anxiety and depressive symptoms among post-secondary students using a comparison sample of members of the general, employed population. Analyses controlled for variables shown to be impactful in the extant literature, including gender, age group, and income.
Despite strengths, several limitations to this research should be acknowledged. The PHQ-9 and GAD-7 are both self-reported assessments of symptoms of anxiety and depression. Self-report measures are prone to social desirability bias, as participants may have chosen not to fully disclose the extent of their experiences due to perceived stigma. As this was a secondary analysis of previously collected data, information on the sampling methods and associated rationale is limited. For example, data was not collected from residents of the Northern Territories, thus we are unable to draw conclusions regarding mental health trends throughout the pandemic for this segment of the Canadian population. Additionally, we were restricted to using the available data and were therefore unable to assess additional variables relevant to mental health impact, such as stressors specifically relevant to students, and overall psychological distress. Other factors that could have been considered include international student status, enrollment status, school type, and degree type. These variables may have allowed us to gain a more comprehensive picture of post-secondary students’ mental health during this time.
Conclusions
This research examines the results of a repeated cross-sectional study assessing symptoms of anxiety and depression in a large sample of Canadian adults during a 2-year period of the COVID-19 pandemic. We found higher prevalence estimates for both anxiety and depression among post-secondary students compared to the general population across time points. Females scored higher on average on both the PHQ-9 and GAD-7, and students scored higher than members of the general population, consistently. Despite the associated limitations, this study builds upon previous research, demonstrating the high prevalence of mental health issues in the Canadian post-secondary student population during the pandemic period. Future longitudinal studies should be conducted to determine the continuing effect of the COVID-19 pandemic and its fallout regarding the mental health of post-secondary students, assessing specific stressors and overall psychological distress, in addition to a more in-depth investigation of relevant sociodemographic factors.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440251389262 – Supplemental material for Comparing Self-Reported Symptoms of Anxiety and Depression Among Canadian Post-Secondary Students to the General Canadian Population During the COVID-19 Pandemic: A National Repeated Cross-Sectional Trend Analysis
Supplemental material, sj-docx-1-sgo-10.1177_21582440251389262 for Comparing Self-Reported Symptoms of Anxiety and Depression Among Canadian Post-Secondary Students to the General Canadian Population During the COVID-19 Pandemic: A National Repeated Cross-Sectional Trend Analysis by Amy Ecclestone, Brooke Linden, Randall Boyes and Heather Stuart in SAGE Open
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific funding for this work. AE independently received a Canadian Graduate Scholarship (Master’s) from the Canadian Institute of Health Research.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HS is the Bell Canada Mental Health and Anti-Stigma Chair and provided financial support for these research activities. AE, BL, and RB have no conflicts of interest to disclose.
Ethical Considerations
The Ethics Committee of Queen's University waived the need for ethics approval and patient consent for the collection, analysis and publication of the retrospectively obtained and anonymised data for this non-interventional study.
Informed Consent
Informed consent was obtained from all individual participants included in the study upon completion of MHRC's online de-identified survey.
Data Availability Statement
Data for this study was provided by Mental Health Research Canada. The data is not publicly available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.