
Abstract
The purpose of this study is to examine American and Japanese clergy’s perception of their role in the prevention of suicide. The research questions are as follows: (a) How do clergy in the United States and Japan perceive suicide? (b) Do they see suicide differently? and (c) How do they envision the role of suicide prevention? The hypotheses are as follows: (a) Christian clergy think that suicide is an unacceptable “sin”; (b) Buddhist clergy are more accepting of suicide than Christian clergy; (c) there are role differences related to suicide prevention in the Japanese and American religious communities; and (d) American and Japanese religious leaders have a different view of their obligations related to suicide prevention. The investigator sent 400 anonymous mail surveys, respectively, to New York and Tokyo. The surveys asked about the clergy’s personal beliefs and the Church’s role in suicide prevention. The investigator analyzed the responses using both quantitative and qualitative methods. The major findings are that many American Christian clergy consider suicide to be a sin, but that “God’s love is available for people who committed suicide.” Many Japanese Buddhist clergy think how one dies is not the most important issue.
Keywords
Introduction
The Role of Clergy in the Prevention of Suicide
In this study, the investigator explores the critical issues of suicide and the role of clergy in suicide prevention in the United States and Japan. Much current scholarship overlooks the role of clergy in suicide prevention. However, the investigator thinks that clergy can prevent suicide by means of counseling and preaching about people at risk. The purpose of this study is to examine American and Japanese clergy’s perception of their role in the prevention of suicide.
In many cases, individuals who commit suicide have had family members, relatives, or friends who have killed themselves (Sakinofsky, 2007). As suicide survivors, they may have spoken with clergy about the meaning of suicide, including its morality, at the time of a loved one’s funeral or memorial service. If clergy speak negatively about suicide, then suicide survivors run the risk of exacerbated grief and vulnerability to suicide. On the contrary, if clergy demonstrate their empathy and compassion toward the survivors, then the pain of losing loved ones could be alleviated. In this regard, the main role of clergy may be in counseling survivors, thereby decreasing the risk of “intergenerational suicide” (Joiner, 2005; Ratnarajah & Schofield, 2007; Sandage, 2009; Stake, 2005) in the same family, or among relatives and friends.
Early (1992) mentioned the role of the church in the African American community and said, “If the church is to provide social integration and moral values that will pervade the African American community, then its role must go beyond the religiously active” (p. 26). In this regard, outreach activities led by religious institutions might benefit nonreligious survivors and lead to social change. To maximize the role of religious leaders in suicide prevention, we should develop an understanding of cultural differences within and among religious communities.
The research questions are as follows:
Research Question 1: How do clergy perceive suicide in the United States and Japan?
Research Question 2: Do they see suicide differently?
Research Question 3: How do clergy perceive the role of suicide prevention in the United States and Japan?
The hypotheses are as follows:
Hypothesis 1: Christian clergy think that suicide is a “sin” and not acceptable.
Hypothesis 2: Buddhist clergy are more accepting of suicide than Christian clergy.
Hypothesis 3: There are role differences related to suicide prevention in the Japanese and American religious communities.
Hypothesis 4: American and Japanese religious leaders have a different view of their obligations related to suicide prevention.
The investigator sent 400 anonymous mail surveys to places of worship in New York and Tokyo. He received 79 American and 78 Japanese clergy replies. Response rate is low, about 20%. However, the investigator found several significant differences between the two religious communities related to the role of clergy in suicide prevention. One possible reason for the low response rate might be the result of some clergy experiencing depression or suicidal feelings. We need further research about the impact of a congregant’s suicide on clergy’s mental health. Although the response rate is low, the investigator believes that these findings may enhance understanding of clergy’s roles and attitudes with regard to suicide and thereby suggest how they may contribute to prevention.
Theoretical Framework
Stack and Kposowa (2011) wrote about “Religion and Suicide Acceptability” by using four frameworks: (a) Durkheim’s notion of social integration, (b) religious commitment, (c) religious networks, and (d) moral community thesis. By contrast, this investigator focuses more on the following three theoretical frameworks: (a) Durkheim, (b) Shame and Guilt, and (c) Morality and Ethics of Suicide. The investigator chose these three frameworks because of their relevance for addressing American and Japanese social and cultural differences. For instance, Western society is based on a culture of “Guilt.” Eastern or Asian Society is based on a culture of “Shame” (Benedict, 1946; Scheff, 2000; Sugiyama, 1983). For reasons described within the body of this article, the investigator thought that “Shame and Guilt” are the key concepts for suicide prevention.
The investigator also tried to explore recent theological trends that include Stack and Kposowa’s (2011) observation that the acceptability of suicide among Buddhists is significantly lower than among Protestants; however, it is higher than among Catholics, although many researchers mentioned that there is no significant difference with regard to suicidal ideation among Christian and Buddhist believers (Stack & Kposowa, 2011). However, the investigator found significant differences among clergy’s attitudes toward suicide in his research. Thus, the investigator also decided to explore denominational differences in suicide prevention attitude among clergy in both countries.
Durkheim
Theoretically, the investigator has chosen Durkheim’s work as an orienting framework (Durkheim, 1897). To conceptualize the content of the surveys that were sent to clerics, the investigator used Durkheim’s four types of suicide: (a) egoistic suicide, due to a weakening and loss of close social ties to groups and collectivities; (b) anomic (normless), the result of deregulation of the individual’s desires and passions; (c) altruistic, the result of the individual’s integration into a group being so excessive that the individual commits suicide for the good of the group; and (d) fatalistic, the result of male structural rules that dissolve very rapidly (Durkheim, 1897). Yet, the use of Durkheim’s theories still leaves some unsolved issues, for example, “Do suicide survivors who have lost their loved ones to suicide feel guilty?” “Is suicide a sin or morally wrong?” To extend “Shame and Guilt” theories, the investigator explored the question whether committing suicide is regarded a sin or not in these two religious communities.
Shame and Guilt
In addition to Durkheim, Benedict (1946) hypothesized that the Western Christian tradition is based on a culture of “Guilt,” while the Japanese Buddhist tradition is based on a culture of “Shame.” The investigator tried to explore these cultural differences in his survey. Furthermore, the theoretical frameworks of Sugiyama (1983) on “Shame and Guilt” and Scheff (2000) on “Shame and Social Bond” were used. Few American and Japanese investigators refer to any relationship between spirituality and suicide prevention; however, many mention that American Christian culture is based on the concept of “sin” while Japanese Buddhist culture is based on the concept of “shamefulness” (Stack, 1950; Sugiyama, 1983). In other words, American Christians focus more on an individual morality rather than social or community norms. They believe that they might be judged by God if they commit immoral activities, such as homicide or suicide. On the contrary, Japanese Buddhists might not believe that they will be judged by an almighty God, but they might be judged by the community and their own conscience.
Morality and Ethics of Suicide: Whether Suicide Is a Sin or Not a Sin
The Christian Bible implies that suicide is both a “sin” and a “shameful” behavior. For instance, the Old Testament treats Abimelech who committed suicide as weak.
54. Then he called hastily unto the young man his armourbearer, and said unto him, Draw thy sword, and slay me, that men say not of me, A women slew him. And his young man thrust him through, and he died. 55. And when the men of Israel saw that Abimelech was dead, they departed every man unto his place. 56. Thus God rendered the wickedness of Abimelech, which he did unto his father, in slaying his seventy brethren. (Old Testament, Judges, 9:54-56)
In addition to “Judges,” in the “Ten Commandments” of the Old Testament, the sixth commandment is “Do not kill.” A narrow definition of the sixth commandment, “Do not kill” includes only “homicide”; however, a broader definition includes both “homicide” and “suicide.”
One of the Greek Orthodox texts mentions the similarity of “homicide” and “suicide.” According to the Greek Orthodox Archdiocese of America, The killing of a man is forbidden and is considered one of the three major sins. It is forbidden not only to take the life of a man, but even to think of killing. The faithful Christian also is forbidden from taking his own life. His own life does not belong to him, but to the Creator to whom life returns. (Greek Orthodox Archdiocese of America, 1996)
The norm that “His own life does not belong to him, but to the Creator to whom life returns” is much the same in Buddhism. The investigator will mention examples in Buddhism later. According to Cragg (2005), “That ‘law of Christ’ was against all voluntary self-destruction. The self-instigator of martyrdom was an accomplice in sin” (p. 56). However, Cragg mentioned there was an exception for Christian suicide. If believers are fully “selfless,” they will try to help others, in which case suicide might be justified (Cragg, 2005, p. 59). 1 In short, suicidal people might not have legitimate decision-making abilities if mental illness is a factor. If people were controlled by disease and cannot judge any proper decision, they are “me-ness” or “selfness.” Under this condition, their behavior, committing suicide, might be justified and it might not be sin. In short, people who committed suicide can be justified, if they cannot make rational decisions because of mental illness.
Although Benedict mentioned that suicide is more acceptable in Buddhism than Christianity, the founder of Buddhism, Buddha, prohibits any kinds of homicide and suicide by his “Five Precepts (pancasila)” that are known as the Buddhist version of the “Ten Commandments of Christianity” (Keown, 2005). The “Five Precepts” are as follows:
I undertake the precept to refrain from harming living creatures.
I undertake the precept to refrain from taking what was not given.
I undertake the precept to refrain from sexual immorality.
I undertake the precept to refrain from speaking falsely.
I undertake the precept to refrain from taking intoxicants.
In addition to “Five Percepts,” the third “Pārajikā” prohibits killing others. It says, “Do not kill other human beings” (“The Third Pārajikā,” Gethin, 1998).
Method
Using Both Quantitative and Qualitative Methods
To explore the role of clergy in suicide prevention, the investigator sent questionnaires to U.S. and Japanese clergy. The questionnaire included fixed-choice, closed-ended questions for quantitative analysis and open-ended questions for qualitative analysis. For analyzing quantitative data, SPSS was used; for analyzing the qualitative data, MaxQda was used. In the first phase, the investigator quantitatively analyzed closed-ended questions by using the statistical tests chi-square and t test, and to compare the two religious communities. Although it was analyzed using two quantitative methods, the investigator also wanted to analyze the meaning of suicide in more depth. Thus, the investigator analyzed open-ended questions by using qualitative analysis in the second phase.
Sample
The investigator created lists of 1,000 Christian churches and 1,000 Buddhist temples. A total of approximately 2,000 churches and temples in New York and Tokyo comprise the sampling frames taken from the Eastern suburbs of New York City, which include Queens (NYC), Nassau, and Suffolk counties (Long Island, New York state), and the Western suburbs of Tokyo, which include the Three Tama Area, Nerima, Setagaya, and Toshima wards. The churches and temples were selected, respectively, from Verizon (New York) and NTT (Tokyo) phone books. A 40% random sample, 400 churches and temples in each country, was generated from the list of all churches and temples using SPSS.
Sample Profile
According to Table 1, the demographic characteristics of the sample are as follows: 92.3% male (United States: 86.1% male; Japan: 96.2% male), 44.8% Caucasian, 49.9% Japanese, 6.7% African American, 3.0% Asian and Pacific Islanders, and 0.7% Latino. The total average age is 56.8 years, and the range is 31 to 88 (median = 59.0, mode = 60.0, SD = 10.9). The U.S. clergy’s average age was 56.7 (median = 56.5, mode = 52.0, SD = 9.3), and the Japanese clergy’s average age was 57.1 (median = 62.0, mode = 60.0, SD = 12.9).
Empirical Profile of Sample (n = 157).

Multiple modes exist.
The number of clergy in the U.S. sample is 79, and that of Japan is 78. The United States constitutes 50.1% of the total sample and Japan, 49.9%. In the United States, there are 68 males (86.1%) and 10 females (12.7%). In Japan, there are 76 males (97.4%) and 1 female (1.3%). Age demographics are similar in the two countries. The average age in the United States is 56.7 and 57.1 in Japan. The median and mode in the United States are 56.5 and 52.0, and those in Japan are 57.1 and 62.1. The difference in the SD between the two countries is relatively small; SD in the United States is 9.3, and that in Japan is 12.9. In the U.S. sample, races or ethnicities are mainly divided into Caucasian (75.9%), African American (11.4%), and Asian and Pacific Islanders (5.1%). In the Japanese sample, Buddhist clergy are dominated by Japanese (98.7%), far less diverse than the United States. According to the Suffolk (NY State) County’s government website (http://www.co.suffolk.ny.us/), in the 2000 Census data, NY Suffolk County’s racial demographics include Caucasian (84.6%), Latino (10.5%), African American (6.9%), Asian (2.4%), and Native American (0.3%). Demographic characteristics are very similar in Nassau County (NY State). Compared with the clergy in general, the Latino clergy’s number is relatively small. Although there are more diverse races or ethnicities, there might be less diverse clergy in this area (Greater NYC area). In short, clergy’s racial demographic characteristics might be less diverse than those of the believers in this area. All 12 Roman Catholic priests answered “single” for marital status. The number of “married” U.S. clergy is 55.
Survey
There are 15 questions that include closed-ended and open-ended inquiries. The investigator introduced the questionnaire carefully in the “Results” sections. There are three characteristics of the questionnaire: (a) using a two-step approach (asking “Yes” or “No” questions first, and then asking “Why” questions), (b) exploring cultural and religious differences in clerical thinking related to suicide prevention in the United States and Japan, and (c) exploring the role differences of clerics in suicide prevention in the two countries.
Survey questions are as follows:
Question 1: What do you think are the most important factors that contribute to suicide?
Please rank “1 (Lowest)” to “10 (Highest).”
For Example, [1] Economic Issues, [2] Others: ( ), [3] Aging Issues . . . [10] Racism
Question 2: Do you think that you have an obligation to help people who are thinking about suicide?
Please check one (“Yes” or “No”).
Question 3: Do you think that religion can prevent suicide?
Please check one (“Yes” or “No”).
Question 4: Do you think that committing suicide is a “sin”?
Please check one (“Yes” or “No”).
Question 5: Do you think that counseling with pastors can prevent someone from committing suicide?
Please check one (“Yes” or “No”).
Question 6: In the past 3 months, have you counseled (talked) with individuals who reported thinking about committing suicide?
Please check one (“Yes” or “No”).
Question 7: In the past 3 years, are you aware of any attempted suicides among your congregation or their relatives?
Please check one (“Yes” or “No”).
Question 8: In the past 3 years, are you aware of completed suicides among your congregation or their relatives?
Please check one (“Yes” or “No”).
Question 9: Does your church have any resources about preventing suicide (such as educational pamphlets, brochures, or leaflets)?
Please check one (“Yes” or “No”).
Question 10: In the past 3 months, have you ever mentioned suicide during Mass (services)?
Please check one (“Yes” or “No”).
Question 11: Are there any penalties for your church’s members who committed suicide?
For example, Different funeral services, or in entombment different grave sites, or penalty imposed on family members.
Please check one (“Yes” or “No”).
Question 12: Would you be willing to counsel people who are not members of your Church?
Please check one (“Yes” or “No”).
Question 13: If you mention suicide during Mass (services), what do you say? Please describe.
Question 14: What do you say to families who have lost a family member to suicide? Please describe.
Question 15: Do you think that “honorable suicide,” as part of a military mission, or a Japanese Kamikaze mission, or a rescue mission, can be justified from the religious stand point?
Please elaborate (Why or Why Not).
Question 16: Demographic Data (Please answer each item):
1. Gender: [ ] Female (woman) [ ] Male (man)
2. Birth Year: Year: ( )
3. Race/Ethnicity: [ ] White, [ ]African American, [ ] Latino,[ ]
Native American, [ ]Asian and Pacific Islanders, [ ] Others
4. Marital Status: [ ] Married, [ ] Single, [ ] Divorced, [ ] Widow
5. Religion: Please include your Church’s denomination: ( )
6. Years of Formal Education: [ ] years
7. Job Title: ( )
8. Years in Position: [ ] years
9. Could you check your approximate of gross (pre–tax) annual income?
*Please check one.
• [ ] Under $20,000 [ ] $20,000 – $29,999
• [ ] $30,000 – $39,999 [ ] $40,000 – $49,999
• [ ] $50,000 – $59,999 [ ] $60,000 – $69,999
• [ ] Over $70,000
10. Have you ever taken any “suicide prevention training”?
Yes [ ], No [ ]
If Yes, please describe what type of trainings and how many days did you take?
Types of Training: ( ),
Total Days: [ ] days
11. How many people are in your congregation?
• [ ] people
Social Indicators: Variables of Suicide Factors
Kposowa (2001) reported, “Unemployment is strongly related to suicide.” He also pointed to gender differences and said, “Unemployed men were a little over twice as likely to commit suicide as their employed counterparts” (p. 131). Bhatia, Khan, Mediratta, and Sharma (1987) compared factors in the United States and India that might place an individual at increased risk of suicide. They identified seven factors related to suicide in the United States: (a) major depression, (b) schizophrenia, (c) alcoholism, (d) recent losses, (e) retirement, (f) limited social support system, and (g) aging issues. In India, nine factors were identified: (a) humiliation, (b) economic loss, (c) poverty, (d) examination failure, (e) relationship disappointments, (f) disputes with spouse and in-laws, (g) property disputes, (h) loss of a loved one, and (i) chronic medical illnesses.
In Question 1, the investigator asked the most important factors that contribute to suicide and also asks them to rank them from “1 (lowest)” to “10 (highest)” and analyzed data by comparing the means (t test) using SPSS software.
The investigator identified the following factors as potentially contributing to suicide: economic issues, aging issues, adolescent issues, mental health issues, substance abuse issues, racism, gender issues, family issues, and lack of spirituality. This identification of social factors that might contribute to suicide was based on the review of literature. However, some factors might be vague and unclearly defined. For instance, the investigator should have clearly defined the conceptualization of “gender issues,” which could be interpreted as “gender inequality at work” or “women’s rights.” Similarly, the definition of family issues might be too broad and might overlap with gender issues in such areas as “issues of single mothers.” The vagueness of the definitions of social factors is a limitation of my research.
Results
“Age, Marital Status, and Income” Versus “Sin or Not Sin”
Initially, the investigator analyzed the entire data and tried to find any correlations between social factors (age, gender, marital status, income, position, etc.) and clergy’s perception of suicide as a sin. Likewise, he was not able to find any significant differences in the entire data set relative to suicide prevention. However, he was able to identify multiple significant differences between American Christian and Japanese Buddhist communities. He also found significant differences among Christian denominations.
Sin or Not Sin?
In one of the investigator’s hypotheses, the independent variable (IV) is type of clergy (American Christian or Japanese Buddhist) and the dependent variable (DV) is “Suicide is a sin (Yes or No).” Table 2 shows that a religious difference exists. More than 12% of the U.S. Christian clerics answered “Yes” for suicide as a sin than Japanese clerics. Statistically, there is a significant relationship between U.S. Christian and Japanese Buddhist clergy, because the p value (.006) is smaller than .05.
U.S. Christian Versus Japanese Buddhist Clergies: Is Suicide a Sin?.

Chi-square (χ2), df = 1, p < .05. This is statistically significant.
Number of “No (n = 35)” includes “not sure (3).”
There are no significant differences between social factors (age, gender, marital status, income, etc.) and regarding suicide as “sin or not sin”; however, there are some significant differences among Christian denominations and perception of suicide as “sin or not sin” (see Table 3).
Denominational Differences Among U.S. Christians: Is Suicide a Sin?.
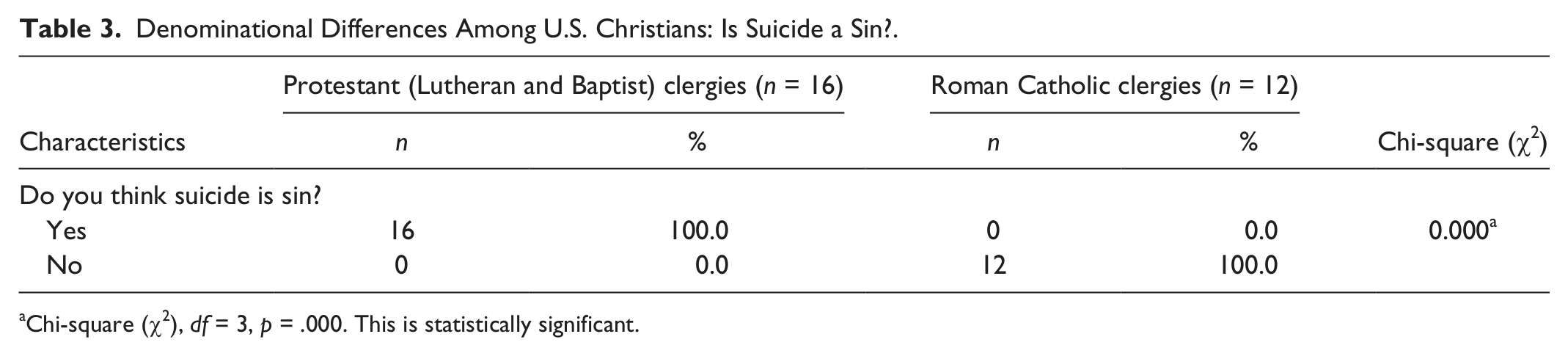
Chi-square (χ2), df = 3, p = .000. This is statistically significant.
Although Durkheim (1897) mentioned that Protestants are more accepting of suicide and Catholics more strictly prohibit it, the investigator got the totally opposite result. Further research might be needed to explore the result.
Obligation to Help or Not?
The question, “Do you think that you have an obligation to help people who are thinking about suicide?” was intended to explore clerics’ individual stances regarding suicide prevention. As shown in Table 4, there is a significant relationship between type of clergy (Christian or Buddhist) and thinking of suicide prevention as an obligation. There is a significant relationship, however. About 80% of Japanese clerics think that they have an obligation. There is a similarity between two countries. Although the results might be rooted in religious/spiritual differences, in qualitative questions, some Buddhist clergy stated they lacked time and finances for suicide preventions. In other words, they wish to help people who are depressed, but they do not have the proper time and resources.
U.S. Christian Versus Japanese Buddhist Clergies: Obligation to Help.

Chi-square (χ2), df = 1, p < .005. This is statistically significant.
Number of “No (n = 16)” includes “not sure (1)” and “both yes and no (2).”
Can Counseling With Clergy Prevent Suicide?
The question, “Do you think that counseling with pastors can prevent someone from committing suicide?” shows significantly different results between the US and Japan. Positive attitudes of believing religious/spiritual power can aid in suicide prevention are much clearer for Christian clergy than Buddhist clergy. However, the attitudes toward suicide prevention cannot be oversimplified, such as positive and passive attitudes, because there might be hidden organizational and/or financial pressures in the Japanese Buddhist community (see Table 5).
U.S. Christian Versus Japanese Buddhist Clergies: Can Counseling With Pastors Prevent Suicide?.

Chi-square (χ2), df = 1, p < .005. This is statistically significant.
Number of “No (n = 3)” includes “both yes and no (1).”
Number of “No (n = 28)” includes “both yes and no (6),” “no answer (5),” “not sure (2).”
Social Factors of Suicide
The first question asks, “What do you think are the most important factors that contribute to suicide? Please rank ‘1’ (lowest) to ‘10’ (highest).” The question focuses on the religious leaders’ awareness of social issues that are the root causes of suicide. To make a comparison between the U.S. and Japanese clergy, the investigator used a t test for analyzing data. Table 6 shows a significant difference in means of Social Factors of Suicide between the responses of American and Japanese clergy on economic, aging, substance abuse, gender issues, and lack of spirituality. Concerning economic issues, Japanese clerics had a tendency to think economic factors contribute more to suicide than clerics in the United States. The means of the American and Japanese clergy are 4.90 (SD = 3.16) and 7.55 (SD = 3.34), respectively. T-score is −5.11 and p value is .000. This result indicates that Japanese clerics think that economic issues are a more crucial factor contributing to suicide than U.S. clerics. Economic difficulties might be the same in both countries, but the physiological and psychological impacts might be heavier in Japan than in the United States.
Means of Social Factors of Suicide (t test).

p < .05. **p < .005. They are statistically significant.
Also included might be social welfare and systemic problems, such as unemployment insurance and age discrimination especially when people try to find a job. More Japanese clerics thought that aging issues contributed to suicide than American clerics. The means of the American and Japanese clergy are 4.22 (SD = 2.81) and 5.24 (SD = 3.03), respectively. T-score is −2.21 and p value is .029. According to the Statistic Bureau of Japan (2005), the percentage of the elder population (people 65 years old and older) is 20.1% in Japan and that in the United States is 12.4%. Although the aging issue is a problem in both countries, political and social support systems are different.
In the United States, older adults can find a job more easily than in Japan, because the legal retirement age is 60 years old in Japan and 65 years in the United States (The Statistic Bureau of Japan, 2005). Concerning substance abuse, more American clerics thought that substance abuse might contribute to suicide than Japanese clerics. The means of the American and Japanese clergy are 6.77 (SD = 1.90) and 5.89 (SD = 1.75), respectively. T-score is 2.73 and p value is .007. In short, the substance abuse issue is more serious in the United States than in Japan. With regard to the gender issue, more American clerics thought gender might contribute to suicide than Japanese clerics. The means of the American and Japanese clergy are 2.97 (SD = 2.46) and 1.81 (SD = 1.49), respectively. T-score is 3.60 and p value is .00. In this context, there were two possible reasons why more American clerics thought gender was a suicide factor: (a) There were more American female (n = 10) clerics who answered the question than Japanese female clerics (n = 1) and (b) Japanese clerics might overlook gender issues as a reflection of systematic discrimination against women. Female clerics might be more sensitive to gender discrimination, because some occupations are dominated by men.
Counseling
Question 6 asks, “In the past 3 months, have you counseled (talked) with individuals who reported thinking about committing suicide?” There is a significant difference between the two countries. The portion of clerics who answered “Yes” for Question 6 is relatively small; however, as seen in Table 7, there is a significant difference between religious types of clergy (Christian and Buddhist) and counseling experiences. Although the results might be rooted in religious/spiritual differences, some Buddhist clergy stated that they lacked funding for suicide prevention. In short, 100% of American Christian and 80% of Japanese Buddhist clerics wish to help people who are depressed, but they do not have adequate resources.
U.S. Christian Versus Japanese: Counseling With Pastors in Past 3 Months.

Chi-square (χ2), df = 1, p < .05. This is statistically significant.
Number of “No (n = 58)” includes “not sure (1).”
Number of “No (n = 49)” includes “not sure (2).”
Training Experiences
The question, “Have you ever taken any ‘suicide prevention training’?” led to the following results.
As reported in Table 8, there is a significant association between country or religious differences (Christian and Buddhist) and suicide training experiences. Although the results might be based on religious/spiritual differences, some Buddhist clergy stated that they lacked time and funds for training. In other words, they wish to help people who are suicidal, but they do not have the necessary time and resources.
U.S. Christian Versus Japanese Buddhist Clergy: Suicide Prevention Training Experiences.

Number of “No (n = 69)” includes “not mentioned (2).”
Chi-square (χ2), df = 1, p < .001.
Number of “No (n = 46)” includes “not mentioned (3).”
Analyzing Open-Ended Questions
The investigator also asked about 10 open-ended questions, and analyzed them by using computer software for qualitative (text) data, “MaxQda 2007.”
In Question 1, the typical Japanese Buddhist answers are related to “reincarnation” and “class slippage.” The Buddhist definition of class slippage differs from the Christian one (Crossan, 1999). In Buddhism, believers think life is always “uncertain” and class would slip without reasons or punishment. According to Chodron (2002), “We can never avoid uncertainty. This not-knowing is part of adventure. It’s also what makes us afraid” (p. 5).
In Question 2, “Do you think that you have an obligation to help people who are thinking about suicide?” clergy in both countries provided reasons why they said “Yes.” American clergy wrote in “professional obligation” as the main reason, along with “professional task” and “job as clergy.” The Japanese clergy also wrote “professional obligation,” and cited “religious obligation” as a reason.
In Question 3, “Do you think that religion can prevent suicide?” no American clergy answered “No,” but 16 Japanese clergy answered, “No.” There are mainly three types of answers: (a) We cannot “save” a life by religion; (b) That’s not my “obligation”; and (c) I respect their choices. For instance, they answered, “My obligation is not to change their minds from death to life.”
In Question 4, “Do you think that committing suicide is a ‘sin’?” there are three typical responses from the Americans: “Religion gives hope”; “Community and prayer can prevent suicide”; and “Religion gives purpose to life.” For example, they said, “Faith provides hope and validation”; “By offering hope and helping to find purpose in living”; “The religious community is compassionate”; and “It gives us positive truth.” There are three keywords in the answers of the American clergy: (a) hope, (b) community help, and (c) purpose in life. In the Japanese answers, there are also three typical answers: (a) thinking about the meaning of life, (b) thinking about reincarnation, and (c) a betrayal of your beliefs.
In Question 5, “Do you think that counseling with pastors can prevent someone from committing suicide?” there are some similarities and differences in the “No” responses, such as “Religion alone cannot take away the mental disorders and other factors that often lead to suicide” (United States and Japan). Although there are some similarities, there are also differences: “Religion itself cannot prevent suicide, but ‘Faith in God’ can prevent suicide” (United States) and “How they pass away (e.g., suicide or homicide) is not a problem; however, how they pray is important in deciding whether they can go to heaven or not” (Japan). Questions 6 to 11 ask only closed-ended questions with no open-ended question. Thus, the investigator will not mention them here and skip to Question 12.
In Question 12, “Would you be willing to counsel people who are not members of your Church?” there are similarities among the clergy who answered “Yes.” “God cares about all people” (United States); “We will be saving lives” (United States); “Every life has meaning” (Japan) and “Their concerns are the same as our concerns” (Japan). In other words, for American clergy, the relationship with God is important, while for the Japanese clergy, the world is one big “family” and it is natural for them to take care of each other.
In Question 13, “If you mention suicide during Mass (services), what do you say?” there were two types of answers for each country. In the United States, Christian clergy said, “All life is precious; help is available” and “It is a sin, but it is not unforgivable.” In Japan, Buddhist clergy said, “Every human being is determined by ‘En (fate/destiny)’” and “Think about reincarnation.”
In Question 14, “What do you say to families who have lost a family member to suicide?” there are some linguistic differences between the United States and Japan. However, the answers are very similar in both countries: (a) “Do not blame yourself” (United States) and “Do not take judgmental attitudes” (Japan); (b) “God’s love reaches all” (United States); and “Going to Heaven” (Japan). In short, clergy in both countries focus more on (a) “nonjudgmental attitudes” toward families who lost their loved ones to suicide and (b) “God’s/Buddha’s love is still available and they can go to heaven.” Those “nonjudgmental” and “sympathetic” attitudes might be helpful in preventing intergenerational suicide.
Discussion
Sin or Not Sin?
The investigator found that more American clerics than Japanese clerics think that suicide is a sin; clerics have an obligation to help suicidal believers; and counseling pastors can prevent someone from committing suicide. More Japanese clerics answered “Yes” for lack of suicide prevention training experiences. Before conducting this study, the investigator thought that these differences were based on religious and cultural difference; however, after analyzing quantitative data, the investigator found that these differences were rooted more in individual philosophy than theological dogmas.
Hope Is the Keyword in the U.S. Christian Clergy
“Hope” is one of the keywords that American Christian clergy mentioned many times. A total of 32 out of 79 clergy mentioned hope. More than 30 Japanese Buddhist clerics mentioned the same theme, that is, “life is a gift from Buddha, and we do not have a right to quit it.” In addition, some Japanese Buddhist clerics said, “Buddhist believers have a right to choose suicide.” These Buddhist answers look contradicted; however, as the investigator mentioned in literature review sections, Buddhist tenets are different by sects. Although there are some religious differences between two countries, both American and Japanese clerics have a sympathetic attitude toward suicide survivors who lost loved one by suicide.
“Life Is a Gift From Buddha” for Japanese Buddhist Clergy
Although the expression or words might be varied, more than 30 Japanese Buddhist clergy mentioned the same theme that “life is a gift from Buddha, and we do not have a right to quit it.” Some clergy referred to the people who quit the gift of life as “arrogant.” Other clergy described them as sinful because they escaped from the duty of life. Or they treated suicide as a sin, because it is a denial of their future. There is a golden rule in Japanese Buddhist culture that is, we human beings have no right to choose death or life and only Buddha or “En/Innen (fate)” can decide the future. Buddha’s choice and fate might crush Christian values, and there are contradictions. From an Eastern or Buddhist point of view, there are no contradictions, because the individual self is connected to Buddha’s will or “En/Innen (fate)” and no one can escape from the fate that Buddha already programmed before human beings were born.
Buddhist Believers Have a Right to Choose Suicide
Another feature that many Buddhist clergy pointed out was, “Buddhist believers have a right to choose suicide as an option, because Buddhist culture accepts suicide as an option.” This theme looks like a contradiction; however, as mentioned earlier, suicide is an option if it does not hurt others.
Lack of Training and Confidence in Suicide Prevention
Among Japanese clerics, the most common feature might be lack of training and confidence in suicide prevention. For example, many clergy mentioned that they were too busy to counsel people and they had no experience: “I wish I could ‘help’ them, but my counseling ability and what I can do is limited.” “I want to refer them to mental health professionals.” “I have no ability to ‘teach’ them.” In short, there is a gap between their will to help people and their acknowledged lack of training experiences, time, and funding.
Life Is a Gift From God
There are some similarities and differences in thinking among both countries’ clerics. The most similar answer is “Life is a gift from God or Buddha, and we do not have a right to quit it.” This common belief is based on the Bible, dogma, and sutras. However, some Buddhist clerics are more accepting of suicide and said, “Buddhist believers have a right to choose suicide.” Even clerics who mentioned an “individual choice of suicide” have a sympathetic attitude toward suicide survivors who have lost a loved one by suicide. In spite of these differences, both groups of clerics pointed out lack of time and financial resources for suicide prevention.
Conclusion
In terms of policy implications, there are some obstacles to creating suicide prevention programs: (a) a lack of financial resources, (b) a lack of time, and (c) a lack of training opportunities. The role of the clergy is the missing link in the prevention of suicide, especially intergenerational suicide, and raises a red flag for mental health professionals, such as psychiatrists, psychologists, nurses, and social workers. Although collaboration between clergy and mental health professionals is essential for suicide prevention, many workers are overlooking the role of clergy in suicide prevention. Whether suicide is a sin or not is a sensitive issue, because it might be adversely important to family members who have lost a loved one to suicide. In addition, sin is also related to morality and ethics. Thus, family survivors might feel guilty if clergy have negative comments to make regarding suicide. Collaboration between clergy and mental health professionals should focus more on how to reduce this guilty feeling.
Limitations of This Research
Limitations of this study are small sample size, low return rate, and sample biases. This study should be considered exploratory for at least two reasons: There is little or no prior research and funding is very limited. The sample size for each country is small due to minimal funds. Possible sample biases exist because it is limited to the suburbs of New York City and Western Special Districts of Tokyo. In addition, only 1 Japanese and 10 American women clergy members responded to the survey.
In addition to the limitations related to the sample size, limited numbers of survey participants (about 16% in Japan and 24% in the United States), answered all qualitative (open-ended) questions. Some participants answered only briefly and others provided long answers. Mail-in surveys have a limitation with regard to space and time.
Furthermore, vagueness of the definitions of social factors is a limitation of my research. For example, the investigator should have clearly defined the conceptualization of “gender issues,” which could be interpreted as “gender inequality at work” or “women’s rights.”
The investigator calls for further research into the role of clergy in suicide prevention. Studies should include large random samples. Alternatively, a study might be designed for in-depth interviewing or large sampled cross-cultural/cross-national surveys.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Notes
Author Biography