
Abstract
Unreliable health care financing undermines the wellbeing of older people in Nigeria – a growing population facing significant vulnerabilities due to age-related health challenges, limited financial resources, and inadequate social support. We use an exploratory sequential mixed-methods research technique to collect primary data from 32 key informants and 430 respondents in Ibadan. The qualitative and quantitative data were analysed using thematic and descriptive analyses respectively. Our results revealed that though older people largely expected to receive social support for health care mostly from state actors, household members, non-state actors and community members, the reality seems to be that they received the least support from state actors, community members, non-state actors and household members in that order. Furthermore, the results showed that the government’s instrumental support was highly coveted and seemed to be the last hope for vulnerable older people. Concerted efforts are required to provide adequate social support for older people and for healthy ageing.
Plain Language Summary
Many older people in Nigeria face difficulties accessing health care due to unreliable financing systems, a challenge made worse by growing numbers, health issues, limited income, and weak social support. In our study in Ibadan, we spoke with 32 key informants and surveyed 430 older people. We found that although older people expected help with health care mainly from the government, families, communities, and other groups, the reality was different. In practice, they received the least support from the government, followed by communities, non-governmental groups, and finally their families. The study also showed that government help, when available, was highly valued and often seen as the last hope for the most vulnerable older people. To ensure healthy ageing, stronger and more reliable support systems are urgently needed.
Keywords
Introduction
In 1982, global leaders adopted the International Plan of Action on Ageing (IPAA) and this signalled the global strategic call to action on care and support for the older people. The primary objective of the IPAA was to ensure healthy ageing (United Nations, 1982). Twenty years later, the Madrid International Plan of Action on Ageing (MIPAA) was adopted during the Second World Assembly on Ageing. These, and similar events, mark a breakthrough in the way the world addresses key challenges of ageing and the provision of social support for older people as part of efforts toward building a fair and inclusive society (United Nations Organization, 2002). Notwithstanding the marginal progress, especially in low- and middle-income countries (LMIC), a United Nations (UN) review shows that the implementation of MIPAA remains on course, though with uneven success across countries and regions. Major constraints being the lack of financial protection and unreliable health care financing (United Nations Department of Economic and Social Affairs (UNDESA), 2018). Financial protection and reliable health care financing are essential for healthy ageing, as they ensure older adults have continuous access to needed health services without facing financial hardship, thereby supporting disease prevention, effective management of chronic conditions, and overall wellbeing in later life.
Along the same line, efforts from within the African continent to ensure the provision of reliable health care financing for older people through social support in the evolving ageing population are also evident. Between 5th and 7th March 2019 for example, more than 1,500 participants from over 40 countries attended the Africa Health Agenda International Conference (AHAIC) held in Kigali, Rwanda. The main aim was to strengthen the drive for universal health coverage (UHC) for the populace. Participants’ concerns rest on the social reality that African countries are lagging in achieving Sustainable Development Goal Three (SDG 3) – ensure healthy lives and promote wellbeing for all at all ages – one of the 17 SDGs set to be achieved by 2030. The conference particularly emphasised the provision of affordable health care for the ‘poor’ and ‘vulnerable’– older adults inclusive – through the social pooling of health resources (Africa Health Agenda International Conference, 2019). Furthermore, in 2021, the Nigerian government adopted the National Policy on Ageing (NPA), which recognises ageing as a national issue to be addressed (Lamai, 2021). The objective of the NPA is to address the special needs of older adults, improve their wellbeing and provide financial protection for their comprehensive health care needs.
Population is ageing rapidly in all regions of the world and unreliable health care financing is capable of hindering the older people from seeking competent medical attention. This in turn may lead to suffering, insecurity and/or death. The experiences of many older adults, who cannot afford to pay for health care services in Ibadan metropolis particularly, raise serious concern and call for an urgent need for the provision of reliable health care support to this increasing demographic category. The older people are often confronted with various diseases and many health care challenges that require huge financial costs (World Health Organization, 2018). While very few older people (‘third agers’– active, independent older adults, before significant physical decline) are capable of financing health care services without resulting in catastrophic or impoverished health spending, majority of them (‘fourth agers’– frail, dependent older adults with advanced aging and health challenges) are not financially protected (Akinyemi et al., 2021; Oyekola & Ajani, 2021).
Ibadan, being one of the three largest cities in Nigeria with increasing number and proportion of older population (World Population Review, 2022), has no dedicated formal health care financing system for the older people (Ani & Isiugo-abanihe, 2017; Dokpesi, 2017). The National Health Insurance Authority (NHIA) and the Oyo State Health Insurance Agency (OYSHIA) that were flagged off in 2005 and 2017 respectively record low enrolment amongst the older people (Akinyemi et al., 2021; Fenny et al., 2018; Oduola, 2021). This has resulted in catastrophic and/or impoverished health spending with serious implications on the wellbeing of older adults in Ibadan, a population facing significant vulnerabilities due to age-related health issues, financial constraints, and inadequate social support (Ani & Isiugo-abanihe, 2017; Salami & Okunade, 2020). Unreliable health care financing exacerbates the vulnerability of older people, undermines healthy ageing, limits access to essential health services and insurance coverage, worsens chronic and age-related diseases, reduces quality of life, as well as increases poverty, social isolation and financial burden on families and communities (Ani & Isiugo-abanihe, 2017; Salami & Okunade, 2020).
The provisions of social support by households, communities, and non-state actors for the older people in the Ibadan metropolis have not been well integrated to cater for their health care needs and challenges. Ensuring that the older people in Ibadan have access to social health insurance, and other possible social support mechanisms that encourage the provision of reliable health care financing in general remain a challenge to healthy ageing. Therefore, the need to investigate the social support provision by households, communities, state and non-state actors for reliable healthcare financing of the older people constitutes the motivation for this paper.
Conceptual Framework and Methodology
The paper is situated within the theoretical construct of social support systems, introduced in the 1970s by Epidemiologist John Casse (1974). The construct emphasises the availability of an efficient web of support (from such entities as households, communities, as well as state and non-state actors) in times of need/crisis. An important function of social relationships/networks across all socio-demographic categories is the provision of social support, which can either be expected/perceived support – defined as the general belief that support is available if needed – or received/actual support – the specific help that has been provided or received from others (Ajani & Oyekola, 2022). Also, social support is usually grouped into four different types of supportive behaviours: instrumental, emotional, interactional and informational supportive behaviours (Dykstra, 2015; Oyekola & Ajani, 2021).
As shown in Figure 1, four different sources of social support are identifiable. These are household members, community members, state actors, and non-state actors. In addition, levels of social support are categorised into ‘no support’, ‘low support’, ‘moderately low support’, ‘moderately high support’ and ‘high support’ depending on the quantity of the different types received from the various sources. Social support theory helps to unravel different social network that older adults have established in the life course and the types of social support expected and/or received from support providers. Social support also plays an important role in sustaining health and reducing vulnerability to illnesses and diseases. Considering the health and financial vulnerability of older people, the availability of social support is vital to an improved quality of life and to ensure healthy ageing.

Types, sources and levels of social support.
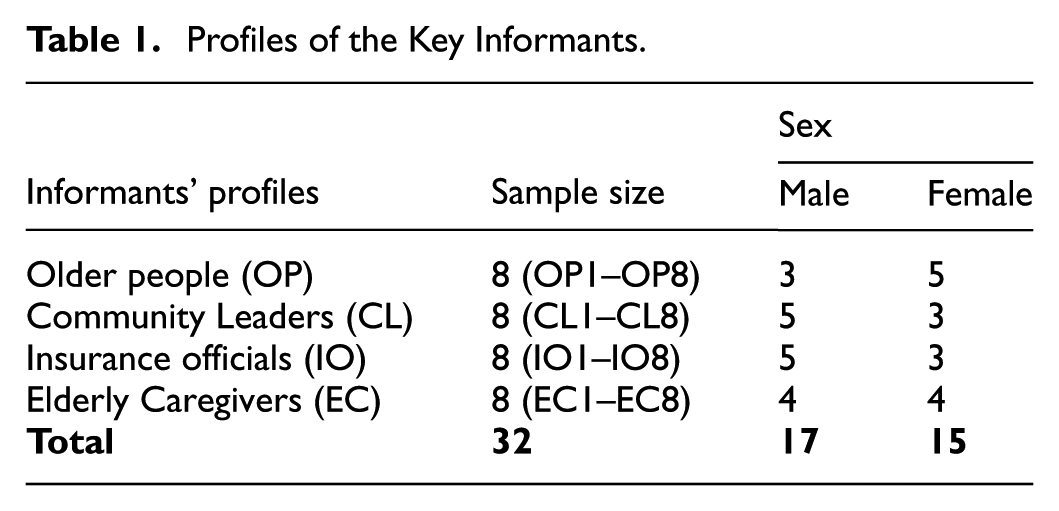
The empirical analysis in this paper used data from a survey conducted in six communities of Ibadan, Nigeria, namely: Inalende, Oje, Agodi Gate, Sabo, Secretariat and University College Hospital (UCH). These communities were selected because they were home to the key stakeholders who were the focus of analysis. An exploratory sequential mixed-methods design was employed for the analysis, that entails an adoption of both qualitative and quantitative methodologies on a sequential basis (Amir-Behghadami & Sadeghi-Bazarghani, 2024). Primary data were collected from four categories of sample population. First, older people (OP) who were 60 years and above. Second, community leaders (CL) including market leaders such as iyaloja and babaloja, religious leaders such as pastors and Imam, political leaders such as key local government officials, and economic leaders such as proprietors/proprietress and major business owners. Third, insurance officials (IO) including officials of NHIA and OYSHIA. Lastly, elderly caregivers (EC) including doctors in geriatric hospitals, and representatives of elderly caregiver centres. Stratified purposive and multi-stage sampling methods were used to select participants and respondents respectively. General selection criteria for the study sample included location, study population category, age, sex, position and affiliation. Based on suggestions from existing literature regarding qualitative study sample size for data saturation (Creswell & Poth, 2017) and the design of this study, 32 participants, as shown in Table 1, were selected from the study population. Additionally, 430 respondents were selected to ensure reliable statistical analysis within the quantitative component of this mixed-methods study. The sample size provides sufficient power to detect patterns and relationships, complements the qualitative findings, and enhances the overall validity and generalisability of the research results.
Profiles of the Key Informants.
Research Methods and Instruments
The method for the qualitative analysis part of this paper is key informant interviews (KII). The KII guides help to elicit qualitative data on social support provisions by households, communities, state and non-state actors. The KII guides were designed for each of the sample population, and have been considered relevant in qualitative research inquiry (Creswell & Poth, 2017; Olajire & Oyekola, 2022). The interviews were conducted, audio-recorded and transcribed verbatim in English language. Five interviews with older participants who had limited access to formal education were translated from the local language into English. The remaining three interviews with older participants were conducted directly in English and therefore did not require translation. Afterwards, the responses were analysed in readiness for the second phase, which involves only older people.
To integrate qualitative elements into the quantitative phase of this study, qualitative data were analysed to generate key themes, patterns and/or categories that reflect participants' experiences, perspectives and existing literature (Ani & Isiugo-abanihe, 2017; Salami & Okunade, 2020). The themes identified were translated into constructs, which form the basis for designing survey questions used in the quantitative phase. The survey was developed using language and concepts grounded in the qualitative findings. The final version of the instrument was then used to collect data from a broader sample, allowing for the analysis of prevalence and/or patterns suggested by the qualitative phase. Finally, results from both phases were merged during interpretation and discussion, to show how the qualitative findings informed and shaped the quantitative outcomes and conceptual framework. This process ensures that the quantitative phase is grounded in the lived experiences of participants, thereby increasing the validity and contextual relevance of the study. The quantitative phase involved administering pre-tested, semi-structured copies of questionnaire for the collection of data on the perceived/expected and received/actual social support provisions by households, communities, state and non-state actors.
The qualitative research instrument was subjected to face and content validity to ensure clarity, credibility, relevance and alignment with the study objectives, and was deemed appropriate by subject matter experts. The quantitative research instrument was also subjected to both face and content validity in order to check for robustness, and it was judged to pass the validity tests. Specifically, the quantitative research instrument was subjected to two different reliability tests in order to ascertain consistency. First, the test-retest correlation results among 20 different older people outside Ibadan were very high as all the items received almost the same answer from the participants in the pilot study (within a week interval). Also, the internal consistency of the instrument was ascertained using Cronbach’s Alpha and the result was 0.953, indicating very strong internal consistency among the items on the pilot study instrument (Cronbach, 1971). Therefore, the instrument passed face and content validity, and its reliability (using test-retest and α internal consistency) was ascertained. As a result, the qualitative and quantitative research tools were considered good for the main data collection exercise after relevant modifications.
Data Analysis
Thematic analysis was used to analyse the qualitative data in order to develop adequate understanding of the themes that emerged inductively and to organise such themes into meaningful categories. The interview transcripts were analysed with the aid of NVivo 12, involving systematic coding, theme development and intercoder agreement to ensure reliability. Member checking was also conducted with a subset of participants to validate the credibility and accuracy of the themes. Key quotations were cited to support emerging themes, and survey items were adapted from the themes. For the five interviews conducted using the local language – Yoruba – translation into English language were done promptly. And all responses during the interview sessions transcribed not later than 3 days after the interview so as to ensure the freshness of the information, capture all the necessary information noted (but not recorded) during the interview (Liem, 2018). All transcriptions are proofread (and edited where applicable) in order to gain adequate understanding of and familiarity with the scripts (Liem, 2018). The summaries and narratives then serve as a guide for the development of survey instrument.
The second phase involved the analyses of quantitative data. After data cleaning, raw primary quantitative data were analysed descriptively using frequency, percentages, and summation. Specifically, thirteen survey items representing the perceived and received social support provisions by households, communities, state and non-state actors were adapted from the themes that emerged from qualitative study. The summation of each survey item was generated and ranked (from 1st to 13th). Considering the coding of the categories of each item (being 2 for often, 1 for sometimes, and 0 for never), 645 to 860 was taken for high, 430 to 644 for moderately high, 215 to 429 for moderately low, 1 to 214 for low and 0 for none (see Figure 1).
Ethical Approval
The study obtained ethical clearance from the Institute of Public Health, Obafemi Awolowo University, Ile-Ife (with HREC No: IPH/OAU/12/2218) on July 20, 2023. Key principles of research ethics and protocols were followed strictly before, during and after the conduct of the study. Following the principles of voluntary participation and informed consents (Millum & Bromwich, 2021), all research participants were duly and fully informed about the purpose of the study, and assured of their rights to withdraw their participation without being coerced. Consent forms were submitted to participating organisations in Ibadan (such as NHIA, OYSHIA, geriatric hospitals and elderly caregiver centres), and verbal consents were obtained from participants to demonstrate voluntary participation. Additionally, the protection and confidentiality of participants and their responses were ensured by preventing potential threats to participants’ safety, avoiding undue intrusion into their privacy or sensitive areas during data collection, and securing the data with password protection to prevent unauthorised access.
Results
Descriptive Statistics of Respondents
The results showed that more female older people (58.8%) were represented. The mean age and standard deviation were 70 years and 8 years respectively, while the median age and interquartile range were 68 years and 13 years respectively, with majority (53.7%) between the common ages of 60 and 69 years. Furthermore, the mean and standard deviation of respondents’ average personal monthly income were approximately US$26.38 and US$36.67 respectively. Also, the median and interquartile range of respondents’ average personal monthly income were US$13.33 and US$30.67 respectively, which ranged between US$ 0 and US$333.33. These findings showed remarkable income gap among the respondents. Detailed descriptions of the sample are presented in Table 2.
Descriptive Statistics of Respondents: Socio-demographic Characteristics.

US$1 = N1,500.
Social Support Provisions by Households, Communities, State and Non-State Actors for the Older People
First, household members were very germane in providing instrumental, emotional, interactional and informational social support for the older people, and lack of household support could render other forms of social supports ineffective. “They [household members] are the major, first person to take care of … elderly person. …so they are the first call”(Female, 55 years, EC1). Social support provisions by household members were emphasised and cannot be underrated. For example, family members mobilised emergency funds for older people whenever required. Although fund mobilisation for the older adults might not be convenient sometimes and might even result in bankruptcy especially in poor families, the goal was often to ensure adequate heath care of every member, older people inclusive (Q9 in Table 3). In addition, during visit to the hospitals or health centres, older people needed at least a family member to help use the Automated Teller Machine (ATM) to withdraw cash, or to visit the bank for cash withdrawal, among other instrumental social support (Q26). Reports from the older participants demonstrated that children were also trying their best in providing social supports despite the political-economy situation in the country. “They always do for me as much as they can afford. I give glory to God”(Female, 71 years, OP2). Also, children often provided emotional and interactional social support by ensuring that they yielded to older people call whenever the need arises, and provided instrumental social support by ensuring that they sent money to older people whenever request for money was made, among other forms of social support.
Adapted Survey items from Qualitative Phrase codes on Social Support Provisions for Health Care Financing of the Older People, with Corresponding Quantitative Summation of Survey items under Various Sources of Social Support.

N = Never, S = Sometimes, O = Often, Σ = Sum.
Second, on the social support provision by community members, “I am not sure how much the community helps, I haven’t seen that around…”(Female, 30 years, EC3). Also, “For the community, everyone takes care of themselves”(Female, 67 years, OP1). Although neighbours were sometimes providing instrumental and interactional social support in the forms of running errand for and interacting with older adults, such supportive behaviours were not much substantive. Some neighbours provided such support with the expectation that it would be rewarded by the older people or relatives; some others provided such social support as eye service, and still some few others provided such support out of free will. Whichever, the low social support provision by community members or neighbours were not totally without reason or condition. Also, while some community members were found to be unfriendly to older people, the attitudes and behaviours of some older people seem to discourage such friendly relationship:
I am not receiving any help from community members, government or organisations. For my neighbours, although they help me sometimes, some of them are not good. But no one gives me money at all. (Female, 75 years, OP5)
Perceived/expected social support provision by community members were geared toward the establishment of community-based insurance. For example, it was suggested that community members (up to 2,500 members, older people inclusive) could come together under one healthcare facility to form Community-Based Social Health Insurance Programme (CBSHIP), under the umbrella of Oyo State Health Insurance Agency (OYSHIA). This allowed community members to keep the healthcare facility functional, cater for the health care needs of older people, and create employment for younger generation (Q18). In addition, “Not only the communities, even philanthropist among us can also adopt some elderly people and register them [under CBSHIP]”(Male, 57 years, IO6).
On the part of government, “There is …a programme we call the basic health care provision fund. These fund is …actually put aside to be able to cater for the vulnerable groups”(Male, 40 years, IO7). However, the older people were neither aware of the provision nor enrolled under it. The Basic Healthcare Provision Fund (BHPF) was reserved for pensioners who earn below US$4 monthly since their financial records could easily be ascertained. If host of vulnerable non-pensioners in the state and vulnerable pensioners earning up to US$4 could not access the BHPF, then financial ruin might be their experience. In addition, government provided free drugs for all populace especially through the basic healthcare facilities (Q8). Provision of free drugs was one of the means through which government provided instrumental social support for the populace, older people inclusive. Nonetheless, whether these drugs were for the major treatment that older people require, whether these drugs eventually got to the facilities for the use of the populace, and whether these facilities were close to the older people’s residence, were not ascertained by the older people. Government’s instrumental support (such as payment for medical bills and periodic medical check-up) was highly coveted and it seemed to be the last hope for the vulnerable older adults (Q19). Importantly, government needed to provide free health care for the older people (Q7), and advocate for their welfare (Q15), among others. Social support provision by state actors (or government) was considered very vital for the survival of vulnerable older people but many older people were not receiving expected support from state actors. This probably left some older persons at a wits end. Going forward, government is expected to ensure that older people welfare is given priority, drive the implementation of policies against older people abuse and laws that protect their rights and privileges, as well as ensure their access to health care:
They [state actors] need to take care of them [older people], make sure that their welfarism is given top priority, they are not open to abuse, there should be law that protect them, they should be able to access care, with or without the help of their family members or well-wishers around. (Male, 41 years, EC7)
Lastly, Faith Based Organisations (FBOs) were providing certain instrumental, emotional, interactional and informational social support for the older people. Essentially, religious organisations often organised programmes for older people (especially the dependants among them such as widows/widowers) majorly for gifts or food distribution (Q14). This physical responsibility was in tandem with their faith (or spiritual) responsibility which emphasised the need to take care of the widows/needy among them. Aside giving of arms in the form of food and other material items, FBOs sometimes invited doctors/physicians to treat older people and conduct medical tests on them free of charge (Q11). Furthermore, religious institutions often visited hospitals or health centres to cater for the health care needs of patients especially the vulnerable older ones:
Well, I have heard that in situation where some patients are not able to pay for their care, there are some religious institutions that have actually been invited and they have been able to offset bills for those people. So yes, I think they have been doing, religious institutions have been helping. (Female, 30 years, EC3)
Nevertheless, older people had not been receiving direct financial assistance from FBOs. “Even in my church, for me to do for them is what they are waiting for”(Female, 71 years, OP2). Aside some forms of social support received from non-state actors (especially religious institutions), FBOs and private companies were expected to perform their corporate social responsibilities (CSRs) by purchasing health insurance (such as the Group, Individuals, and Family Social Health Insurance Programme [GIFSHIP] under NHIA and CBSHIP under OYSHIA) for older people with legislative backings (Q22, Q23). By so doing, FBOs, Community-Based Organisations (CBOs), private companies such as telecommunication companies, petroleum industries, factories, among others would be committed to providing social support for reliable health care financing of the older people. This in turn was expected to complement government’s support for population health, especially the health care of the older population.
Social Support Provision by Household Members
As shown in Table 3, 13 (I1–I13) perceived and/or received social support from four sources of social support (households, communities, state, and non-state actors) were explored and further investigated using quantitative approach. The results showed that the older people expected household members to provide seven notable forms of social support (I7, I5, I13, I6, I8, I4, and I3). First, the respondents expected household members to pray for them for provision and sound health (Σ = 752) as 77.7% of them often expected such role to be performed while 19.5% sometimes expected that. Second, the older people expected household members to pay for their medical bills and drugs (Σ = 592), with more than half (53.7%) of them often expecting that role to be performed and 30.2% sometimes expecting such role. Third, the respondents expected instrumental and interactional social support from household members such as transporting them to health care centre/hospital when require and staying with them during the period (Σ = 571). Nonetheless, older adults received only one notable form of social support from households (I7); that is, prayer for provision and sound health (Σ = 737).
Social Support Provision by Community Members
The older people expected three forms of social support provision (instrumental, informational and interactional social support) from community members, and these included prayer for provision and sound health (Σ = 572), provision of adequate information on reliable health care financing (Σ = 515), and support for elderly association such as championing its establishment and ensuring its sustenance (Σ = 473). However, older people received no form of social support from community members except for only one that was sometimes provided (I7): prayer for provision and sound health (Σ = 321).
Social Support Provision by State Actors (Governments)
Furthermore, respondents often or sometimes expected all the 13 forms of social support from the state actors except that respondents did not expect government to employ social workers for them and pay for the persons (I3, Σ = 401, being the least). The top three most perceived social support provisions by state actors were instrumental and interactional in nature, and these included payment for medical bills and drugs (I5, Σ = 617), performance of periodic check on elderly health (I6, Σ = 617), and provision of functional primary health care centre near elderly residence (I10, Σ = 615). Nevertheless, Table 3 shows that older people received no single support from the government as indicated by the proportion of the respondents who never received (385 ≤ Σ ≤ 430). In fact, overall assessment of all sources of social support (households, communities, state and non-state actors) showed that respondents expected most from the government (Σ = 7286), but received least from the same government (Σ = 272).
Social Support Provision by Non-State Actors
Lastly, respondents expected five major forms of social support from non-state actors (I7, I8, I2, I12, and I5) as shown in Table 3. One, the respondents expected non-state actors to pray for them for provision and sound health (Σ = 655). Two, they expected non-state actors to provide adequate information on reliable health care financing (Σ = 538). Three, they expected non-state actors to conduct medical outreach for the elderly (Σ = 472). Despite much expectations, older people received only one form of social support from non-state actors (I7) – prayer for provision and sound health (Σ = 508).
Discussion of Results
Social support for reliable health care financing need and other forms of support is vital to experiencing healthy ageing (Oyekola et al., 2021). Household members, community members, state actors and non-state actors are crucial in providing reliable health care financing and other support systems for older people. The vitally importance of the presence of more significant others has been noted to facilitate the recovery of older people from illness as these support providers are capable of providing all the types of social support (Ebimgbo et al., 2017; Oyekola & Ajani, 2021). Importantly, household members are the first point of call and their role in mobilising emergency fund cannot be underestimated. Although respondents desired financial support from households due to their health vulnerability and their average monthly personal income to meet their health care needs, only prayer, being a means to connect to the supernatural, was received, and this reflects the cultural beliefs of the Yoruba in the supernatural (Usman & Falola, 2019). While the quantity of financial support from household might not meet older people expectations due to political economy situation in the country, household members performed their intergenerational duty to the best of their abilities. Out of all the roles analysed, only prayer was not influenced by the political economy situation of the country. Since offering of prayer for the older people was not influenced by any government policy or financial resources, political economy situation of the country might have hindered household members from providing adequate social support that was expected of them such as provision of free health care, presence during hospital visits, periodic medical check-up, and provision of information on reliable health care financing (Arisukwu et al., 2021; Dykstra, 2015; Oyekola et al., 2020; Salami & Okunade, 2020). Hence, the need for household members to be empowered financially in order to provide social support for the older people, as such cannot be undermined.
Community members did not provide substantive support for the older people. Although the older people expected communities to provide instrumental, interactional and informational social support, community members only provided little and convenient assistance such as running errand. Existing studies have put neighbours and other community members in compensatory hierarchy after spouse, children, relatives and friends (Dykstra, 2015; Oyekola & Ajani, 2021), but the role of community members in ensuring the provision of reliable health care financing cannot be overemphasised. Importantly, suggestive roles of community members tend toward the establishment of community-based social health insurance programme (CBSHIP) for the benefit of the older people. This conforms to various calls for health insurance at the community level, and which has been considered capable of providing reliable health care financing and universal health coverage if well governed (Archibong et al., 2023; Oyekola et al., 2020; Waelkens et al., 2017). Although CBSHIP under OYSHIA and GIFSHIP under NHIA were existing in the study locations, older adults were not beneficiary of the programmes due to lack of awareness and/or financial and health vulnerability. Community members should therefore come together and provide social support for the older people especially through the establishment of community-based associations or social health insurance programmes.
The older people expected highest level of social support from the government as they considered such support to be very vital for their survival. For example, government was expected to pay for medical bills and drugs of the older people since older persons were often confronted with many health care challenges that require huge financial costs and many of them were not financially protected. Also, considering the health and financial vulnerability as well as the importance of early disease detection, older persons considered it imperative for government to perform periodic checks on their health as this was expected to improve their wellbeing and enhance healthy ageing. Universal primary health care is a key target of the United Nations in realising Sustainable Development Goal (SDG) 3, and primary health care is a fundamental human right of older people (Oyekola et al., 2020). Hence, without qualified personnel in a functional primary health care centre, the realisation of SDG 3 is questionable and the protection of the fundamental human rights of the ageing population is increasingly challenged. These, among others, must have made the respondents to expect government to provide such instrumental type of social support.
Although government had made provision for the establishment of social health insurance that was capable of providing reliable health care financing for the older people, many of them were not enrolled due to lack of awareness and/or financial incapability. The basic healthcare provision fund (BHPF) that was supposed to cater for vulnerable older people were restricted to pensioners who earned less than US$4 monthly and who might find it difficult to pay for OYSHIA premium from their monthly pension. Hence, the need for collective efforts from social support providers to ensure the provision of reliable health care financing, especially for the vulnerable older population (Dykstra, 2015; Oyekola et al., 2021). Also, while government made provisions for all citizens to receive drugs at basic healthcare facilities when in need, the drugs were not always available at the facilities when require, and the drugs were not always suitable for the treatment of older people’s sicknesses/diseases. Still, government role in providing functional primary health care centres and safeguarding population health cannot be over-emphasised (Akinyemi et al., 2021; Ebimgbo et al., 2017; Oyekola et al., 2020). Overall assessment of all sources of social support showed that respondents expected most from government, but received least from the same government. This demonstrates the level of government commitment to her older populations. Government should therefore take a leading role by driving the implementation of the national policy on ageing and by rejiging her commitment to population health especially for the older people, in order to ensure the provision of reliable health care financing for the increasing proportion of the older population.
Lastly, religious institutions or Faith-Based Organisations (FBOs) were providing social support for the older people such as constant prayers, intermittent provision of food and financial resources, as well as occasional medical outreach, test and treatment. The respondents considered prayer for provision and sound health to be indispensable in old age. As a results, prayer requests resonate in all their expectations from social support providers. Despite the perceived social support from non-state actors, older people could only receive prayers especially from FBOs. Non-governmental organisations (NGOs), Community-Based Organisations (CBOs), private companies, and the likes were however not providing social support for the older people despite their corporate social responsibilities to the communities. The roles of non-state actors in providing social support for health care financing of the older people and in ensuring better life for community members including older ones are vitally important (Olajire & Oyekola, 2022; Olivier et al., 2015). Legislations that will commit non-state actors to provide social support for health care financing need and other forms of support for the older people are therefore required, as these are expected to improve their wellbeing and ensure healthy ageing. In all, households, communities, state and non-state actors still have a long way to go in ensuring the provision of reliable health care for the older population. The older people have contributed their part to societal development; therefore, posterity demands all stakeholders to be responsible for their wellbeing by providing social support as this is considered to be respect for intergenerational contract (Ajani & Oyekola, 2022).
This study, which employed an exploratory sequential mixed-methods analysis, encountered some limitations. First, the initial qualitative phase was conducted among a limited purposively selected sample of older people in Ibadan. While this provided rich insights, the views expressed may not fully represent the broader older population across diverse socioeconomic and cultural settings in the Ibadan metropolis. To address this, the emergent themes were used to inform the design of a structured survey instrument administered to a larger and more diverse quantitative sample, enhancing the external validity of the study. In addition, some participants in the qualitative phase had limited formal education, requiring interviews to be conducted in Yoruba. The process of translating these responses into English presented the possibility of losing some cultural or contextual nuances. However, this was mitigated by engaging bilingual researchers familiar with both the local language and the study context, and by conducting back-translation checks to preserve meaning. Finally, the social support structures and health care financing mechanisms identified in this study are highly contextual, likely influenced by Yoruba culture, family systems and access to health care services in Ibadan. While this limits generalisability to other regions, the study provides a foundation for comparative research and offers valuable insights for local policy and programme design.
Conclusion, Implications and Recommendations
The lack of household support can render other forms of social supports ineffective, and government’s instrumental support is highly coveted as it seems to be the last hope for the vulnerable older people. Most definitely, government is expected to take leading role in ensuring health care for all. Also, although older people largely expect to receive social support for health care mostly from state actors, household members, non-state actors and community members, the reality seems to be that they receive the least support from state actors, community members, non-state actors and household members in that order. The paper concludes that stakeholders (such as households, communities, state and non-state actors) are very crucial in providing instrumental, emotional, interactional and informational social support for the older people. This knowledge is useful for all stakeholders and policy makers that are interested in healthy ageing, especially as it relates to health care financing of vulnerable older population. This empirical study investigates, for the first time, various perceived and received social supports for the health care financing of older people in Ibadan, Nigeria.
Considering the health and financial vulnerability of the older people as well as inadequate support from households, communities, state and non-state actors, the hope of experiencing reliable health care financing may be lost. The social implication of this is unhealthy ageing which may in turn put higher pressure on the economically struggling children or relatives. Also, for government not to support the provision of reliable health care financing for the older people, beside the establishment of social health insurance that many of them cannot afford, has serious implications on health care financing. Going forward, there should be concerted efforts on the parts of households, communities, state and non-state actors, and not on any particular stakeholder, to provide social support for reliable health care financing needs and other forms of support for the older population. Also, government should establish legislations that would commit non-state actors to perform their corporate social responsibilities for the older people as these are expected to improve wellbeing and ensure healthy ageing. Lastly, government must rejig her commitment to population health, especially for the older population by providing functional and efficient primary health care, and by ensuring that all older persons are enrolled in social health insurance schemes that cover their medical expenses without financial hardship or ruin. Investigation on social support provisions for the older people in other parts of Nigeria is required in future studies for comparative analysis and policy formulation. This is important because the peculiarity of the Yoruba culture, as against notable culture in other regions of Nigeria, may have had a significant influence on the results of the analysis in this paper.
Footnotes
Acknowledgements
The authors sincerely thank all participants for their time and valuable contributions to this study. We also appreciate the editors and anonymous reviewers for their constructive feedback, which significantly improve the quality of this manuscript.
Ethical Considerations
The study obtained ethical clearance from the Institute of Public Health, Obafemi Awolowo University, Ile-Ife (with HREC No: IPH/OAU/12/2218) on July 20, 2023. Key principles of research ethics and protocols were followed strictly before, during and after the conduct of the study. Following the principles of voluntary participation and informed consents, all research participants were duly and fully informed about the purpose of the study, and assured of their rights to withdraw their participation without being coerced. Consent forms were submitted to participating organisations in Ibadan (such as NHIA, OYSHIA, geriatric hospitals, and elderly caregiver centres), and verbal consents were obtained from participants to demonstrate voluntary participation. Additionally, the protection and confidentiality of participants and their responses were ensured by preventing potential threats to participants’ safety, avoiding undue intrusion into their privacy or sensitive areas during data collection, and securing the data with password protection to prevent unauthorised access.
Consent Details
Following the principles of voluntary participation and informed consents, all research participants were duly and fully informed about the purpose of the study, and assured of their rights to withdraw their participation without being coerced. Consent forms were submitted to participating organisations in Ibadan (such as NHIA, OYSHIA, geriatric hospitals, and elderly caregiver centres), and verbal consents were obtained from participants to demonstrate voluntary participation.
Authors’ Contributions
IAO and OAAj conceived the study. IAO, OAAj, and OAAk reviewed literature and designed study proposal. IAO and OAAj collected research data. IAO and JOO analysed and interpreted research data. IAO drafted the manuscript. OAAj, OAAk and JOO edited the manuscript for scholarly content. The manuscript was critically revised by all authors, who approved the final version for publication. IAO and OAAj are guarantors of the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Royal Society of Tropical Medicine and Hygiene (RSTMH) Early Career Grant, in partnership with National Institute for Health and Care Research (NIHR) United Kingdom.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
All data are available in this paper. That is, detailed analysis and presentation of all relevant data have been provided.