
Abstract
This study aims to examine whether the integrated medical and elderly care is conducive to improving the utilization of health management services for older adults. We utilized the China Health and Retirement Longitudinal Study (CHARLS) database covering 2011 to 2020, employing the DID model and mediation effect testing for empirical analysis. We also employed the PSM-DID model and a series of other methods for robustness tests and placebo tests. The main findings are as follows: Firstly, the integrated medical and elderly care increases the probability of the treated group’s older adults participating in physical examinations, health assessments, and chronic disease management by 2.4%, 2.7%, and 0.3%, respectively. Secondly, the integrated medical and elderly care has a higher impact on aged 60 to 80, females, rural residents, and healthier older adults. This fully demonstrates that the pilot projects of integrated medical and elderly care can improve the inequality in health management service utilization among vulnerable groups and truly play a role in preventing diseases for older adults. Thirdly, the integration of medical and elderly care enhances the utilization of health management services by increasing the policy agglomeration effect and service accessibility in pilot cities. This study concludes that integrated medical and elderly care can enhance the utilization of health management services among older adults, which is crucial for improving their health and quality of life. The government should fully integrate medical and elderly care service resources to provide one-stop health management services.
Introduction
Establishing an integrated medical and elderly care service system that combines medical and elderly care resources is a crucial measure for actively addressing population aging. Compared with 2010, the proportion of China’s population aged 60 and above increased by 5.44% in 2020, and the dependency ratio for older adults rose by 7.80% (National Bureau of Statistics of China, 2021). The level of aging in China has reached the highest among countries at a similar level of development. Especially by the end of 2023, the number of older adults will be close to 300 million, marking the official entry into a moderately aged society (Wang, 2024). Influenced by factors such as the accelerating pace of aging, the extension of life expectancy, and the continuous decline in fertility rates, older adults faced multiple risks including the prevention and treatment of chronic diseases, increased health risks, and escalating pension burdens. The emergence of these issues has led to a sustained growth and diversification in the demand for medical and elderly care services among China’s elderly population (Liu et al., 2023). However, for a long time, the segmentation between China’s medical and elderly care sectors, as well as the dispersion of service provision across different levels, have constrained the comprehensive provision of medical-care and elderly-care services for older adults and hindered the improvement of supply efficiency. Therefore, integrated elderly care and healthcare resources across different sectors and levels, controlling the costs of elderly care and medical services, and achieving the policy goal of “ensuring that the elderly have adequate care and medical support” constitute important directions for the socialization of elderly care services in China (Du et al., 2025). Against this backdrop, since 2016, the National Health Commission and the Ministry of Civil Affairs have designated 90 national pilot cities for the integration of medical and elderly care across the country, requiring these pilot cities to actively explore new models of elderly care services and fully play a leading role as demonstrations. This approach also represents a universal practice among governments worldwide. As early as the 1970s, the United States initiated the Continuing Care Retirement Community (CCRC), which provides integrated residential facilities and services for elderly individuals across different age groups and health statuses, spanning from independent living, assisted living to nursing care. In the 1990s, the British government promulgated The New NHS (National Health Service), with a key principle being to enable the NHS to collaborate with other departments, break down the barriers between medical services and social care, and deliver integrated medical and elderly care services to citizens. Japan proposed the establishment of a community-based integrated care system in 2003, and further advanced this by enacting the Act on Comprehensive Assurance of Regional Medical and Elderly Care in 2014, aiming to promote effective communication of medical and elderly resources and strengthen the legal guarantee for integrating medical and elderly care within the comprehensive care support system. In November 2023, Singapore’s Ministry of Health, Ministry of National Development, and Ministry of Transport launched the Silver Generation SG Initiative, which is designed to facilitate healthy aging for the elderly within communities (Zheng et al., 2025). Research indicates that, as a novel elderly care service model, the integration of medical and elderly care plays a significant role in alleviating the contradiction in medical service supply and reducing the burden on society for elderly care (Wu & Wang, 2024a).
With the increase in age and the extension of average life expectancy, the physical functions of older adults gradually decline, and the probability of developing various chronic diseases, such as hypertension, diabetes, and coronary heart disease, increases. This has gradually become one of the important factors affecting life safety. Therefore, relying solely on medical treatment after illness onset is insufficient to meet the medication needs of older adults for long-term care. Health management that involves early intervention in health factors is more conducive to enhancing the quality of life and health of older adults. Health management for older adults is one of the national basic public health service projects. Older adults who receive health management can detect diseases early, initiate prompt treatment, prevent the onset of diseases, reduce complications, and lower the rates of disability and mortality. Health management for older adults contributes to improving the quality of life and alleviating the economic burdens on society, families, and individuals (Huang & Zhang, 2021). Health management is a crucial aspect of the pilot policies integrated medical and elderly care. In this context, “medical” refers to the early identification of major diseases, necessary examinations, treatment, rehabilitation, and training, encompassing medical services, health consultation services, health screening services, disease diagnosis and treatment services, major illness rehabilitation, and end-of-life care. “Elderly care” forms the foundation, which includes services for daily living assistance, emotional support, cultural and recreational activities, among others (Li & Feng, 2024). At the current stage, has the implementation of pilot projects integrated medical and elderly care in China enhanced the utilization level of health management services for older adults? Existing literature primarily focuses on the policies integrated medical and elderly care services in specific provinces or cities, while studies evaluating these pilot policies from a nationwide perspective are relatively scarce. Especially from the perspective of the utilization of health management services for older adults, there is still room for further improvement in assessing the policies integrated medical and elderly care services.
Based on this, the marginal contributions of this study are primarily reflected in the following three aspects: Firstly, this article treats the two batches of pilot cities for integrated medical and elderly care services in 2016 as a quasi-natural experiment. Using CHARLS data from 2011 to 2020, it empirically investigates the impact of these pilot projects on the utilization of health management services for older adults through the DID model and various robustness test methods. This shifts the focus from the more localized research found in existing literature to a more comprehensive analysis, addressing the deficiencies in identification strategies and research design present in current studies. Secondly, this article analyzes the pathways through which the integration of medical and elderly care services influences the utilization of health management services for older adults from a theoretical perspective (Liu et al., 2025). It empirically tests the impact of channels such as policy agglomeration effects and service accessibility, thereby complementing and enhancing the existing literature through mechanism analysis. Thirdly, the article explores the heterogeneity of the impact of policies integrated medical and elderly care services on the utilization of health management services from multiple dimensions. The research findings hold practical significance. These insights provide a reference for subsequently refining policies integrated medical and elderly care services and enhancing the utilization level of health management services for older adults.
Policy Background and Literature Review
Policy Background
In the late 20th century, the World Health Organization (WHO) proposed “healthy aging,” whose core philosophy is to ensure that older adults maintain good physical health, mental health, and social adaptation. In the early 21st century, WHO further introduced “active aging,” a concept centered on three pillars—health, participation, and security—to maximize the quality of life for older populations. With the deepening of research, the integrated development of elderly care and medical services has emerged as a globally recognized consensus for addressing population aging (Tao & Yuan, 2023). However, for a long time, China has faced a high incidence of illnesses and a relatively high proportion of disability among older adults. The existing medical service system, which is centered on treating acute diseases and relatively fragmented, forces older adults to rely on outpatient or inpatient services when they become ill, resulting in the dual negative consequences of medical resource wastage and health losses. In addition, due to the lack of health management awareness and professional, scientific medical nursing techniques, the current pension system is unable to provide professional and scientific medical and elderly care services for older adults. Therefore, promoting the integration of medical and elderly care has become a crucial measure to meet the medical and elderly service needs, actively address population aging.
The concept of integrated medical and elderly care has broad connotations and extensions. Among them, “medical care” is the core, including disease diagnosis, treatment, preventive healthcare, and rehabilitation nursing, while “elderly care” serves as the foundation, encompassing daily care, emotional comfort, and comprehensive services (Gao et al., 2020). The medical and elderly care integration model emphasizes organically combining medical resources and elderly care service resources in approach, and enabling their close connection in status and degree. The theoretical background of medical and elderly care integration is multi-dimensional and interdisciplinary, with its core lying in addressing the fragmentation of medical and elderly care services in aging societies and promoting service model optimization through theoretical innovation (Qiao et al., 2024). Multi-dimensional and interdisciplinary theories, such as the Continuum of Care theory, Healthy Aging theory, Resource Integration and Systems theory, and Social Equity theory, all provide theoretical support for integrating medical and elderly care services. Its essence lies in resolving the segmentation of medical and elderly care services in aging societies and driving service model optimization via theoretical innovation. In practice, developed countries entered the aging phase earlier, and based on their social systems and cultural traditions, they have formed different application paths of theories. However, the common theoretical core remains “centering on the needs of older adults, taking resource integration as the means, and aiming at sustainable development.”
Overall, the development of China’s policy on integrated medical and elderly care can be roughly divided into three stages. The first stage is the initial development phase (2013–2015). In September 2013, the State Council issued the “Several Opinions on Accelerating the Development of the Elderly Care Service Industry,” which pointed out the need to actively promote the integration of healthcare and elderly care services, and set clear requirements for the specific forms and service content of integrated medical and elderly care. Building on this foundation, in November 2015, the former National Health and Family Planning Commission issued the “Guiding Opinions on Promoting the Integration of Medical and Elderly Care Services,” which once again emphasized the importance of integrated medical and elderly care. It also proposed establishing and improving cooperation mechanisms between medical and healthcare institutions and elderly care institutions, as well as promoting the extension of medical and elderly care services to communities and households. This marked the initial formation of a policy framework for integrated medical and elderly care. The second phase is the pilot exploration phase (2016–2021). In June 2016, the National Health and Family Planning Commission and the Ministry of Civil Affairs issued the “Notice on Selecting National Pilot Units for Integrated Medical and Elderly Care Services,” identifying 50 cities, including Shijiazhuang, as the first batch of pilot cities. In September of the same year, an additional 40 cities, including Nanjing, were selected as the second batch of pilot cities. The government aims to explore and form localized models of integrated medical and elderly care through these 90 national pilot cities, developing replicable and scalable local experiences that can serve as a reference for the comprehensive promotion of medical and elderly care integration. The distribution of pilot cities is shown in Figure 1. The third phase is the comprehensive promotion phase (After 2022). In April 2022, the National Health Commission proposed launching demonstration projects for integrated medical and elderly care services, hoping to drive the overall annual development of medical and elderly integration through experience sharing from demonstration regions. In March 2023, the Health Commission again emphasized the need to fully summarize and promote typical experiences from the pilot work (Li et al., 2024).
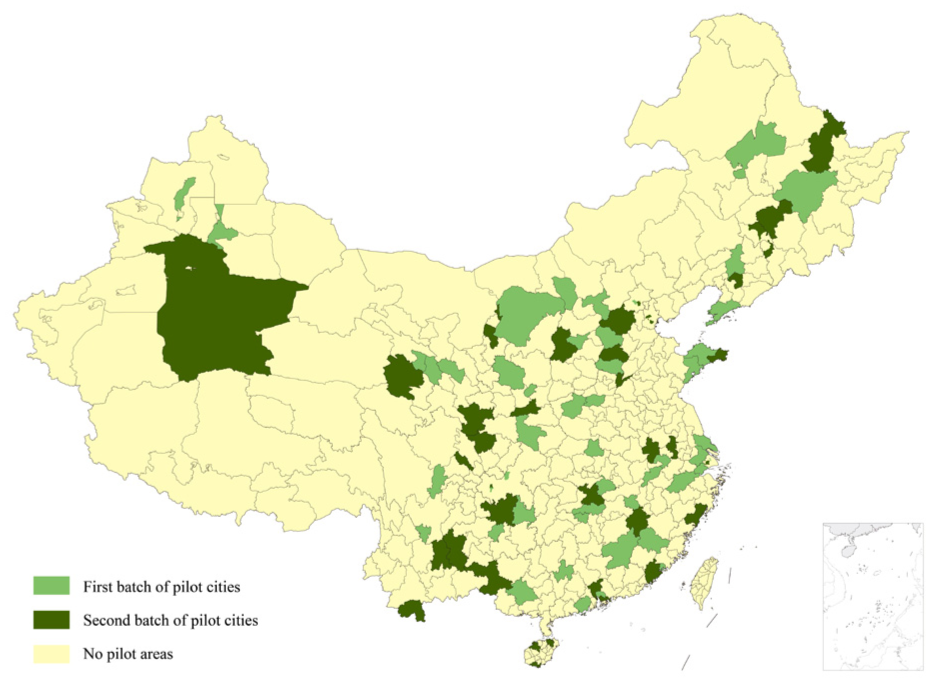
Pilot cities for China’s policy on integrated medical and elderly care.
China’s integrated medical and elderly care policies exhibit the following characteristics: Firstly, adhering to the policy goal of “active aging,” a full-chain service system is constructed. Aiming at the interwoven medical and elderly care needs of older adults, the policies prioritize addressing the long-term care of disabled seniors, gradually covering all age groups of older adults, and emphasize building a full-chain service system of “prevention-treatment-rehabilitation-care.” Secondly, the model innovation of “government-led + multi-stakeholder participation” is highlighted. The policies clarify the primary responsibility of local governments in planning, fiscal subsidies, and standard-setting, introduce preferential policies to attract enterprises and social organizations, and support public-private partnership (PPP) models for medical and elderly care integration projects. Thirdly, the policies follow a progressive promotion path from “pilot exploration” to “national rollout.” Since 2016, the state has designated multiple batches of pilot areas for integrated medical and elderly care, exploring models such as “community-based medical and elderly care integration,” and promoting nationwide adoption through experience summarization. The main reasons for these characteristics lie in the increasing aging population, interwoven medical and elderly care needs of older adults, and the inadequacy of traditional service models. The government needs to safeguard people’s livelihoods, while the fragmentation of medical and elderly care resources requires integration and optimization. Meanwhile, China’s deep-rooted tradition of family and community-based elderly care, coupled with the potential of social forces, has driven the formation of multi-dimensional policy features to address aging challenges.
Literature Review
Most health issues that arise as individuals enter their senior years can be prevented or delayed through early adoption of an active and healthy lifestyle along with proper management. Compared to seeking medical services in hospitals after becoming ill, engaging in proactive health management is more conducive to enhancing the physical and mental health of older adults (Hung & Jen, 2012). The existing literature explores two dimensions. The first dimension focuses on research from the perspective of supply entities. As a public service, health management is crucial for the well-being of older adults and should rightly receive attention and participation from various sectors of society (Haimi & Sergienko, 2024). Ai et al. (2019) pointed out that health management for older adults should transcend the limitations of traditional single-entity government dominance and foster a new pattern of multi-entity supply. Especially at the current stage, China’s resident medical insurance has basically achieved full coverage. Establishing a market-oriented health management mechanism to attract more social entities to participate can facilitate the integrated development of health management services (Hofmann, 2007). Furthermore, scholars have conducted targeted research based on the functions of different entities. Sui et al. (2020) noted that the government should formulate relevant policies to guide the development of the health industry. The market and communities, as the primary providers of health management, should fully integrate resources to establish a supportive health management service system (Luo et al., 2019). Families and individuals should also bear corresponding health responsibilities, enhance their awareness of health management, and jointly create a favorable environment for health management (Haimi & Sergienko, 2024). The second dimension from the perspective of supply methods. Zhou and Fu (2018) pointed out that receiving medical management services at health service centers is currently the primary approach for older adults. Given the annual increase in the population of older adults with chronic diseases, community elderly care services are burdened. Integrated medical and elderly care resources through various means and innovating service models that combine medical and elderly care have become inevitable trends for future development (Alum et al., 2023). Besides community institutions, health management centers can be established to further integrate resources from different entities, providing integrated and continuous health management services (Gross et al., 2023). Therefore, based on existing research, the integration of medical and elderly care not only fully integrates medical and elderly care resources from different entities but also innovates service supply methods. On this basis, this article advances the following hypothesis:
As a welfare system that spans both the elderly care and medical sectors, and is dedicated to promoting the national strategic initiatives of “Healthy China” and “Active Aging,” the policy of integrated medical and elderly care can facilitate the effective utilization of healthcare services for older adults (Collet et al., 2010). Firstly, when advancing the development of the integration of medical and elderly care, both central and local governments have promoted this integrated approach through the introduction of a series of policies. Sun et al. (2023) pointed out that central and local governments have continuously issued a range of policy measures, which not only extend from healthcare services to the integrated development of elderly care but also encourage social forces to establish institutions that integrate medical and elderly care. These integrated services have significantly expanded the connotation and denotation of China’s medical and elderly care integration, effectively elevating the crucial aspect of healthcare and rehabilitation to the policy level, marking the official entry of China’s medical-elderly care integration into a new development stage (Yang, Xue, & Ren, 2023). Secondly, the implementation of the integration of medical and elderly care has facilitated a coherent set of methods and models at the financial, management, organizational, supply, and clinical levels, thereby improving the institutional environment. On one hand, in regions designated as pilot sites for the integration of medical and elderly care, the government has introduced supportive policies, creating a policy agglomeration effect that attracts the active participation of market entities and fosters a favorable atmosphere and mindset for health management. The policy agglomeration effect refers to the synergistic impacts generated by the concentrated implementation of a series of related policies within a specific region or domain. Research by Sabharwal et al. (2019) indicates that government investments in the healthcare sector can effectively reduce healthcare costs and enhance the utilization of health services. On the other hand, during the initial stages of policy implementation when market operation mechanisms are not yet fully established, the government enhances the affordability of integrated medical and elderly care services by providing institutional subsidies, tax incentives, and bed subsidies, thereby promoting the utilization of health services (Sun, 2021). Therefore, this article posits that the government has instituted a series of strategic measures in policy support, financial investment, and public health input—thereby generating a policy agglomeration effect that has demonstrably enhanced health management service utilization among older adults. Specifically, through the issuance of special plans, cultivation of cross-dimensional policy synergy, optimization of resource allocation efficiency, streamlining of service processes, and activation of healthcare demands within the older adult demographic, the government has effectively elevated both the accessibility to and utilization rate of medical and health services for this population. This article puts forward the following hypothesis:
From the perspective of service provision, the integration of medical and elderly care creatively consolidates different medical and elderly care providers, facilitating the utilization of health management services by promoting the proximity of medical-elderly care service facilities and expanding service modes (Maciel et al., 2020). For a long time, more than 90% of older adults in China have relied on home-based or community-based care. To further enhance the quality of elderly care services, local governments across the country are committed to building the “last mile” of elderly care services (Feng, 2022). In fact, when piloting the integration of medical and elderly care, the state encourages the fusion of relevant entities and the embedding of such services within communities, better meeting the demand for integrated medical and elderly care services among community-residing older adults. Næss et al. (2017) introduced four models of integrated medical and elderly care. As the physical functions of elderly individuals gradually decline, older and disabled older adults, due to mobility issues, have reduced access to health management services (Du et al., 2023). The pilot projects for integrated medical and elderly care have promoted the signing of family doctor contracts between older adults and grassroots communities, providing services for older adults with mobility issues, thereby enhancing their utilization of medical services (Zhang et al., 2023). Meanwhile, some capable institutions integrated medical and elderly care can provide services such as daily care, medical nursing, and health monitoring at older adults’ doorstep, increasing the likelihood of their utilization of medical services (Yang, Chen, & Chen, 2023). Therefore, the following hypothesis is proposed:
Through a literature review, it is evident that scholars have conducted systematic research on the research topic of this paper. However, several research gaps remain: Firstly, while scholars have elucidated the positive effects of pilot projects integrated medical and elderly care from dimensions such as supply entities and methods, few have directly explored the inherent logical relationship between the integrated medical and elderly care and health management services. Secondly, although the existing literature has reached a research consensus on the importance of health management for older adults, there is a lack of research on the factors influencing health management services, especially a lack of exploration based on national policy pilots (Wang & Wang, 2025). Thirdly, regarding the pathways through which the integrated medical and elderly care affects the utilization of health management services by older adults, few scholars have delved into this area, and the scattered research has not formed systematic findings.
Based on this, this article constructs an influence framework diagram, as shown in Figure 2. The contributions of this study to the existing literature are as follows: Firstly, using panel data of CHARLS from 2011 to 2020, and adopting models such as DID and Sobel mediation effect tests, this paper empirically analyzes the mechanism of the integration of medical and elderly care on health management services for older adults, expanding the micro-level evidence of pilot projects for integrated medical and elderly care. Secondly, this article studies the influence mechanism of health service management from the perspective of national policies, filling the gaps in the existing literature and providing a reference for improving the utilization level of health management services for older adults. Thirdly, this article discusses the mechanism of how the integrated medical and elderly care affects the utilization of health management services from two perspectives: policy agglomeration effect and service accessibility, serving as an innovative supplementary study to the existing literature.

Theoretical framework of this research.
Data, Variables, and Methods
Data Source
The data utilized in this article are derived from the CHARLS, a large-scale interdisciplinary survey conducted under the auspices of the National School of Development at Peking University and executed by the Institute of Social Science Survey at Peking University. The sample covers tens of thousands of households across 150 districts and counties and 450 village-level units nationwide, with the objective of promoting interdisciplinary research on China’s aging population and related issues such as health and retirement, and providing a more scientific basis for formulating and refining relevant policies. There are primarily two reasons for using CHARLS data in this article. Firstly, the survey questionnaire, designed with reference to international experiences from the United States, Europe, and elsewhere, employs various sampling methods such as Probability Proportional to Size (PPS). The questionnaire covers fundamental aspects including personal information, family structure, social security, multiple types of income and consumption, providing high-quality data support for studying health management issues among the elderly population. Secondly, the five survey waves span the implementation cycle of policies integrated medical and elderly care, and the data includes information on elderly health management services and provincial/municipal pilot projects integrated medical and elderly care, which serve the research needs of this article. Based on this, balanced panel data are derived from processing the complete five waves of CHARLS data from 2011 to 2020. Additionally, to further address endogeneity issues and control for relevant variables at the provincial level, this paper also utilizes statistical yearbook data from relevant cities as supplementary data materials. After processing, a total of 48,044 samples were obtained, including 10,188 in the treatment group and 37,856 in the control group.
Variables
Dependent Variables
The dependent variable in this study is health management services. Health management services for older adults are comprehensive services targeted at individuals aged 60 and above, primarily encompassing physical examinations, health assessments and interventions, as well as prevention and control of chronic diseases. The objective is to detect early-stage diseases and provide targeted treatment to prevent disease progression, thereby reducing complications, disability rates, and mortality rates. Based on this, this paper evaluates from three aspects. Firstly, physical examinations. This is measured by the question in the survey, “When was your last routine physical examination?” Older adults who have participated in physical examinations are assigned a value of 1, while those who have not are assigned a value of 0. Secondly, health assessments. Health assessments for older adults generally refer to actively seeking health interventions at primary healthcare institutions. With reference to the survey design, this is measured by the question, “In the past month, have you visited a medical institution for an outpatient consultation?” Older adults who have participated in health assessments are assigned a value of 1, otherwise, they are assigned a value of 0. Thirdly, chronic disease management. This is evaluated using two questions from the survey: “Has a doctor told you that you have any of the following chronic diseases?” and “Are you currently receiving treatment for any of the following chronic diseases?” The CHARLS survey primarily examines the management of two chronic diseases: hypertension and diabetes. Therefore, older adults who are managing chronic diseases are assigned a value of 1, and those who are not are assigned a value of 0.
Explanatory Variable
The explanatory variable in this study is the integrated medical and elderly care. Firstly, with reference to the CHARLS data setup, if an older adult resides in a city that has implemented the integrated medical and elderly care policy pilot program in the survey year, indicating that the individual is covered by the policy, they are assigned a value of 1; otherwise, they are assigned a value of 0. Based on Figure 1 presented earlier, a total of 90 pilot cities from the first and second batches are selected as the treatment group samples for this study, while other non-pilot areas serve as the control group samples. Secondly, in terms of time, the CHARLS data conducted nationwide surveys in 2011, 2013, 2015, 2018, and 2020, which fully cover the period before and after the integrated medical and elderly care pilot program, thereby adequately meeting the temporal requirements of this study. Taken together, the explanatory variable in this paper is the interaction term between the dummy variable for the integrated medical and elderly care pilot program and the dummy variable for the pilot program’s timing.
Control Variables
To control the influence of other variables, this article selects demographic factors, lifestyle, and city-level characteristics of older adults as control variables for this study. In terms of demographic variables, the factors considered include age (the actual age of the respondent), gender (male = 1, female = 0), household registration (urban = 1, rural = 0), education level (years of education), marital status (married/with spouse = 1, not married/without spouse = 0), disability status (disabled = 1, healthy = 0), pension insurance (participating = 1, not participating = 0), and medical insurance (participating = 1, not participating = 0). For lifestyle factors, considerations include smoking (yes = 1, no = 0), drinking (yes = 1, no = 0), and social interaction (participating in any of 11 activities = 1, not participating = 0). City-level variables encompass the level of urban economic development (logarithm of per capita GDP) and the degree of urban industrial service orientation (logarithm of the ratio of the tertiary industry to the secondary industry value added for the given year).
Mechanism Variables
Based on the research framework, the mechanism variables examined in this article are categorized into two types: The first type is the policy agglomeration effect, which is measured using two variables: the number of integrated medical and elderly care policies issued by each city and the government’s public health investment. The number of policies is quantified using the PKULAW Policy Database, based on the count of integrated medical and elderly care policies issued by each city in the survey year. Public health investment is measured according to the health and wellness expenditures recorded in the statistical yearbooks of each city. The second type is the service accessibility variable, assessed through two variables: facility accessibility and home-based services. With reference to the policy planning that aims to “establish a 15-min elderly care service circle in cities” and “bridge the last mile,” if the distance from an elderly person’s home to a medical institution is less than 1 km or a one-way trip takes 15 min, it is assigned a value of 1; otherwise, it is assigned a value of 0. Home-based services are measured based on the question in the survey, “Have you received home-based medical services (excluding physical examinations)?” with a value of 1 assigned for “yes” and 0 for “no.”
Methods
DID Model
The pilot projects of integrated medical and elderly care in various Chinese cities provide a quasi-natural experimental setting for this study. Therefore, theoretically, accurately evaluating medical and elderly care integration policies requires eliminating estimation biases caused by temporal and individual variations, as well as analyzing trend changes before and after policy implementation. To precisely evaluate the impact of integrated medical and elderly care on the utilization of health management services for older adults, this paper employs a Difference-in-Differences (DID) model to assess the policy effect. The DID model employed in this study follows the methodological framework proposed by Ashenfelter and Card (1985) and has been widely used in policy evaluation research (Jaeger et al.,2020; Wang, 2024). Unlike traditional regression models, using DID model to assess policy effects has become a common practice in academia, offering the following advantages: Firstly, it reduces estimation biases arising from policy self-selection or time trends. Secondly, it captures dynamic effects. It enables analysis of changes before and after policy implementation to identify short-term and long-term impacts. Thirdly, it strengthens causal inference. Under the parallel trend assumption, it reliably identifies causal policy effects, ranking among the mainstream methods for evaluating public policies. Cities implementing integrated medical and elderly care pilots in different years and for different individuals are included in the treatment group, while the remaining non-pilot cities are included in the control group. This study systematically assesses the impact of integrated medical and elderly care on the utilization of health management services for older adults. Based on this, the DID model constructed in this paper is as follows:

Here,
PSM-DID Model
Since the selection of cities for the pilot implementation of the integrated medical and elderly care program was not random, this article employs the PSM-DID method for robustness testing. By controlling for covariates and matching treated and control groups based on similar or identical scores, this approach eliminates selection bias and allows for a more precise assessment of the policy effects of integrated medical and elderly care on the utilization of health management services among older adults. Based on this, the article constructs a PSM-DID regression model, as shown in Equation 2:

Sobel Mediating Effect Model
This article uses the Sobel mediation effect model (Sobel, 1982) to conduct an in-depth exploration of the mediating effect between the integrated medical and elderly care policy and the utilization of health management services. According to this method, it is necessary to fit three regression equations respectively for the four mediating variables to be tested, namely Number of policies, public health input per capita, Facility convenience, and On-site service, as shown in Figure 3. Firstly, it is necessary to test whether the impact c of the main independent variable X on Y is significant without adding the mediating variable (M). Secondly, to test whether the coefficient a of the impact of the main independent variable X on the mediating variable (M) is significant. Thirdly, to test whether the impact coefficient

Mediating effect model.
In the analysis of mediating effect test results, if c is significant,

Results
Descriptive Statistical Analysis
Table 1 reports the descriptive statistics of the relevant variables. In terms of explanatory variables, 21.2% of older adults participated in the pilot program integrated medical and elderly care. For the explained variables, the proportions of older adults participating in physical examinations, health assessments, and chronic disease management were 54.5%, 20.6%, and 32%, respectively. Notably, the sample mean of the treatment group was higher than that of the control group. Specific results await further verification. In terms of control variables, the average age of older adults was 68.469 years; male older adults accounted for 48.9%, slightly fewer than female. The majority of older adults, 74.9%, had spouses, and 26% were urban residents. The average number of years of education was only 5.175. The disability rate among older adults was 12.2%. The participation rates in pension insurance and medical insurance were 69.7% and 92.1%, respectively. The proportions of older adults with smoking and drinking habits were 30.6% and 31.3%, respectively. The proportion of older adults who participated in at least one social activity was 47.1%. The urban per capita GDP and the degree of urban industrial service were 10.811% and 12.6%, respectively. Through group comparisons, the treatment group had higher means than the control group in terms of marriage, household registration, education, medical insurance, drinking, social activities, urban per capita GDP, and the degree of urban industrial service. Conversely, the control group had higher means than the treatment group in terms of age, gender, disability status, pension insurance, and smoking. Regarding mechanism variables, the average number of integrated medical and elderly care facilities in urban areas was 3.027, and the average logarithm of per capita public health investment was 4.263. The proportion of older adults living within the “last mile” or “15-min living circle” from such facilities was 13.4%, and 21.6% of older adults had received home-based services.
Results of Descriptive Statistics.

Note. Keep three digits after rounding the decimal point.
Benchmark Regression Analysis
Table 2 reports the impact of the pilot program integrated medical and elderly care on health management services for older adults. The study demonstrates that, compared to the control group, the policy pilot increases the probability of the treatment group’s older adults participating in physical examinations, health assessments, and chronic disease management by 2.4%, 2.7%, and 0.3%, respectively. These findings are statistically significant at the 1% level, supporting the validity of Research Hypothesis 1. This fully demonstrates that the integration of medical and elderly care can enhance the utilization of health management services for older adults, holding significant practical implications for early prevention and intervention of disease indicators, as well as reducing the incidence of diseases. In terms of control variables, as age increases, the probability of older adults participating in physical examinations and health assessments also rises. Compared to female older adults, male elderly exhibit a higher level of utilization of health management services. Compared to rural older adults, Urban older adults have a higher probability of participating in physical examinations and chronic disease management by 8.2% and 10.2%, respectively. The higher the number of years of education, the greater the probability of older adults participating in health assessments and chronic disease management. Although disability decreases the probability of older adults participating in physical examinations, it increases their enthusiasm for health assessments and chronic disease management. Unhealthy lifestyles, such as smoking and drinking, reduce the utilization level of health management services. Engaging in social activities increases the probability of older adults participating in physical examinations, health assessments, and chronic disease management by 6.9%, 3.5%, and 2.6%, respectively. Furthermore, the higher the per capita gross domestic product and the degree of urban industrial service development, the greater the probability of older adults undergoing physical examinations, health assessments, and chronic disease management.
Results of Baseline Regression.

Note. Robust standard error in brackets.
p < .1. **p < .05. ***p < .01.
Equilibrium Trend Test and Dynamic Effect Analysis
A crucial underlying assumption when using the DID model for policy effect evaluation is that, prior to the pilot program integrated medical and elderly care, the development trends in the utilization of health management services among older adults in the treatment and control groups should be consistent, with no systematic differences between the two. Any differences between the two groups should emerge after the policy pilot. Based on this, this article conducts a parallel trends assumption. Firstly, according to the specific time when each city implemented long-term care insurance, the first year of the pilot program is designated as the base year, set as 1, the year before the pilot as −1, the year after as 2, and so on. In this way, the years are divided into 10 periods from −5 to 4. Secondly, older adults who participated in the medical and elderly care integration pilot program after its initiation are selected, and this subset is designated as the treatment group for all periods prior to the pilot’s launch. Finally, regression analysis is employed to derive the estimated coefficients for each period, representing the differences in the utilization of health management services. The regression results are then visualized through graphical representation.
The results are shown in Figure 4, where the vertical axis represents the estimated coefficients of the medical and elderly care integration pilot, and the horizontal axis represents the relative periods from the first phase of the pilot. The results indicate that before the first phase, there is no statistically significant difference in the utilization of health management services between the treatment and control groups. This suggests that, prior to the medical and elderly care integration pilot, there were no notable disparities in health management service utilization between the two groups. However, starting from the current phase of the pilot, a positive and significant difference emerges between the treatment and control groups. This indicates that, following the implementation of the medical and elderly care integration pilot, the utilization of health management services among older adults gradually shows divergence. This also corroborates the regression results presented in Table 2, suggesting that medical and elderly care integration can significantly enhance the utilization of health management services in pilot cities.

Equilibrium trend test and dynamic effect (95% CI).
Robustness Tests
This article employs three methods to conduct a robustness check on the benchmark regression results. Firstly, PSM-DID test. The prerequisite for the benchmark DID regression is the satisfaction of the random assignment assumption. Based on this, we adopt the PSM-DID method to eliminate the endogenous problem of changes in individual characteristics between the treatment and control groups. Figures 5 and 6 report the standardized deviations of variables and the common support of propensity scores. We performed PSM using a 1:1 matching approach with physical examination as the explanatory variable. It is evident that before matching, most variables exhibited large standardized bias. After matching, all variables’ bias concentrated near zero, controlled within 10%, passing the balance test. Four samples in the control group and two samples in the treatment group fell outside the common support, with sample loss less than 0.1%. Secondly, the Variable Substitution Method. The dependent variable studied in this article is the utilization of health management services, encompassing three categories: physical examinations, health assessments, and chronic disease management. Based on this, we employ the variable substitution method for robustness checking. Specifically, we use the question from the survey, “Have you received community health management services?” as the substitution variable. Thirdly, Adjusting for Fixed Effects. The benchmark regression only controls for individual fixed effects and year fixed effects. Therefore, building upon the benchmark regression, we additionally control for province and city fixed effects to eliminate the differential impacts arising from policy changes across different provinces. The regression results using these three methods, presented in Table 3, indicate that there is a significant positive correlation between medical and elderly care integration and the utilization of health management services by older adults. This strongly suggests that medical and elderly care integration has significantly improved the utilization of community health management services, further supporting the robustness of the benchmark results.

Standardized bias of each variable.

Common value range for propensity score matching.
Results of robustness tests.

Note. Robust standard error in brackets.
p < .1. **p < .05. ***p < .01.
Placebo Tests
The placebo test refers to the examination of whether a policy effect truly exists by setting a virtual policy implementation time or a treated group sample. Based on this, we conduct placebo tests using two common approaches: virtual treated groups and virtual policy times. Firstly, the virtual treated group. This paper utilizes city samples from the long-term care insurance pilot programs conducted between 2011 and 2020, excluding those that overlap with the integrated medical and elderly care pilot cities. Subsequently, we designate the remaining samples as the fictitious treated group (
Results of the Placebo Tests.

Note. Robust standard error in brackets.
p < .1. **p < .05. ***p < .01.
Heterogeneity Analysis
As shown in Figure 7, this article further examines the heterogeneity of the impact of integrated medical and elderly care on the utilization of health management services through four dimensions: age, gender, household registration, and disability status. Firstly, in terms of physical examinations, the influence of integrated medical and elderly care is more pronounced among aged 60 to 80 (p < .01), females (p < .01), rural residents (p < .01), and healthy older adults (p < .01). This suggests that integrated medical and elderly care can effectively increase the likelihood of these groups participating in physical examinations, thereby enhancing the utilization of health management services. Secondly, regarding health assessments, the impact of integrated medical and elderly care on the utilization of health management services is more significant for females (p < .01), rural residents (p < .01), and healthy older adults (p < .01). Additionally, integrated medical and elderly care has a notable effect on both aged 60 to 80 (p < .05) and 80+ older adults (p < .01), with a higher impact observed among aged 60 to 80 older adults. Lastly, in terms of chronic disease management, integrated medical and elderly care exhibits a more pronounced influence on aged 60 to 80 (p < .01), females (p < .01), and healthy older adults (p < .01). Furthermore, it significantly affects both urban (p < .01) and rural older adults (p < .01), with a greater impact noted among urban older adults.

Results of heterogeneous analysis.
Influence Mechanisms Analysis
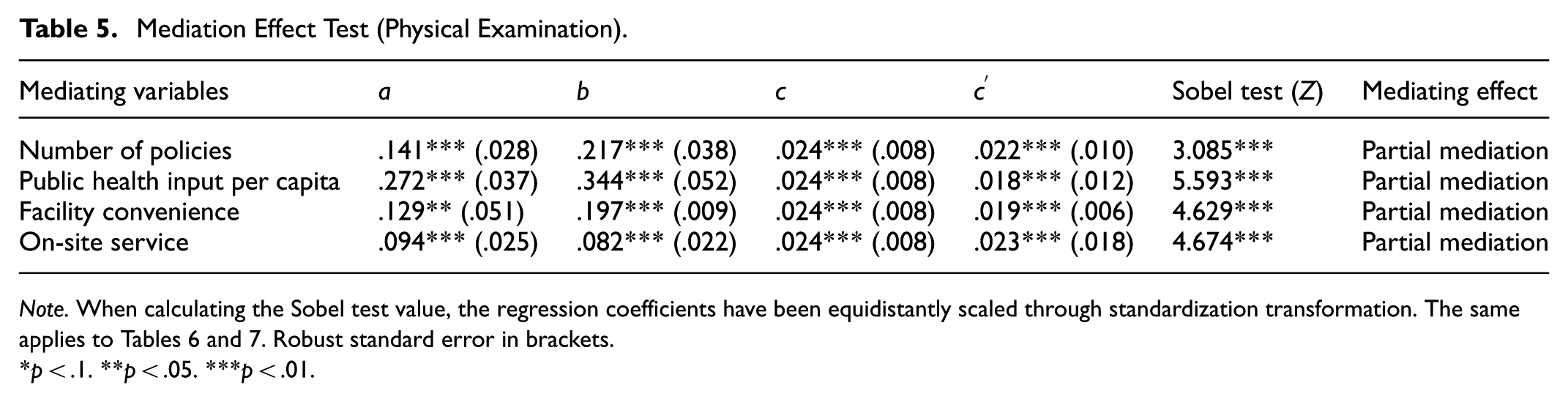
In this article, the mediating effects of four potential mediating variables, namely Number of policies, public health input per capita, Facility convenience, and On-site service, are calculated respectively. Herein, the value of a represents the impact coefficient of the main independent variable X on the mediating variable M; the value of b represents the impact coefficient of the mediating variable M on the dependent variable Y (Physical examination, Health assessment, Chronic disease management); the value of c represents the impact coefficient of the main independent variable X on the dependent variable Y without controlling the mediating variable, and the value of
Tables 5 to 7 report the mediating effect test results for the three variables of the utilization of health management services. Table 5 presents the mediating effect test results for physical examination. The impact of number of policies on physical examination is significant (b = .217; p < .001), and the impact of integrated medical and elderly care on physical examination is significant (a = .141; p < .001). After controlling for number of policies, the impact of integrated medical and elderly care on physical examination remains significant (
Mediation Effect Test (Physical Examination).
Note. When calculating the Sobel test value, the regression coefficients have been equidistantly scaled through standardization transformation. The same applies to Tables 6 and 7. Robust standard error in brackets.
p < .1. **p < .05. ***p < .01.
Mediation Effect Test (Health Assessment).

Note. Robust standard error in brackets.
p < .1. **p < .05. ***p < .01.
Mediation Effect Test (Chronic Disease Management).

Note. Robust standard error in brackets.
p < .1. **p < .05. ***p < .01.
Discussion
Based on CHARLS data and China Statistical Yearbook data spanning from 2011 to 2020, this study empirically examines the impact of the pilot program integrated medical and elderly care on elderly health management services using the PSM-DID model and mediation effect test model. It also analyzes heterogeneity and impact mechanisms. Our research indicates that the integrated medical and elderly care can effectively increase the probability of older adults participating in physical examinations, health assessments, and chronic disease management. These research findings remain robust after undergoing robustness checks and placebo tests. These conclusions are also consistent with the research findings of scholars such as Gross et al. (2023), and Haimi and Sergienko (2024). Yin (2024) similarly demonstrates that the Chinese government’s implementation of policies integrated medical and elderly care is an important measure to actively address population aging, effectively enhancing health management and improving the quality of life for older adults. Not only in China, but since the 21st century, the international community has universally recognized the importance of integrating medical care and elderly care. The World Health Organization’s Framework for Integrated and Continuous Long-Term Care Systems emphasizes strengthening care services and social support networks. By integrating medical and elderly care resources, Japan provides comprehensive services including preventive healthcare, health management, and psychological comfort, which have delayed the decline of physical functions and improved the quality of life for older adults (Siette et al., 2022). The Sechelt Community Hospital in Canada transformed its original buildings into outpatient care units to enhance the quality and continuity of care services, achieving the sharing and convenient integration of regional medical resources (Jiaxuan et al., 2024). Therefore, it is evident that the research conclusions of this paper are consistent with the effects of integrated medical and elderly care practices in other countries. Especially for older adults with chronic diseases or who are disabled or semi-disabled, the integration of medical and elderly care has increased community-based elderly care and medical service facilities, providing convenience for daily medical and elderly care for older adults (Wei & Zhang, 2020).
This study also analyzes the heterogeneity in the utilization of health management services by older adults. Our findings are generally consistent with the research conclusions of Gao et al. (2020), Wu and Wang (2024b), and Ouyang and Shen (2025). The research indicates that the integrated medical and elderly care has a more significant impact on enhancing health management services for aged 60 to 80 older adults. Gao et al. (2020) pointed out that people of different age groups show varying policy effects when enjoying community-integrated medical and elderly care services due to differences in their health conditions. Among them, older adults aged 65 to 80 have shown significant improvements in outpatient follow-up visits and chronic disease management. The possible reason for this result may be because health management should be prospective; for middle-aged and younger older adults, engaging in health management can effectively reduce the probability of illness and increase life expectancy. However, aged 80+ older adults often already have related diseases, making health management less efficient (Wang et al., 2020). Furthermore, the integrated medical and elderly care can effectively improve health management services for women and those in rural areas. Wu and Wang (2024a) argued that integrated medical and elderly care has a higher impact on older women, which may be related to the differences in personality traits between females and males. Ouyang and Shen (2025) pointed out in their study that there is a significant health inequality issue between rural and urban older adults, and integrated medical and elderly care has a higher health impact on older adults with different incomes in rural areas. This fully demonstrates that policies integrated medical and elderly care can narrow the gap in health management utilization among vulnerable groups or regions and alleviate health inequalities. For a long time, influenced by a series of factors, compared to men and urban older adults, women and rural older adults have had lower utilization rates of health management services, resulting in gender and regional inequalities in health (Bergen et al., 2022). Lastly, the integrated medical and elderly care has a higher impact on health management services for healthy older adults, which is also consistent with the original intention of implementing such integration. In recent years, the proportion of older adults with chronic diseases and disabilities in China has been increasing, becoming one of the important issues that urgently need to be addressed (Mihu et al., 2024). The pilot programs integrated medical and elderly care can effectively increase the probability of healthy older adults engaging in health management, reduce the incidence of chronic diseases and disability rates, and contribute to promoting healthy aging (Escrivá Gracia et al., 2019).
This study further conducted an analysis of the influence mechanism. The research findings indicate that the integrated medical and elderly care enhances the utilization of health management services by older adults through improving policy agglomeration effects and service accessibility in pilot cities. This research conclusion is consistent with the findings of scholars such as Sabharwal et al. (2019) and Maciel et al. (2020). Sun (2024) demonstrates that, influenced by policies issued by the central government, pilot cities have continuously introduced a series of policies integrated medical and elderly care. These policies not only increase investments in the medical and public health sectors but also construct a range of infrastructure in grassroots areas such as communities, improving the convenience for older adults to utilize related services. Especially in rural areas, due to mobility limitations among older adults bridging the “last mile” of medical and elderly care services have become a crucial aspect of the government’s pilot projects (Jiang et al., 2024). By innovating pilot models and enhancing service methods, pilot regions have created practical conditions for health management among rural older adults (Verkerk et al., 2018).
There are also some limitations to this study. Firstly, the study utilizes CHARLS, which is authoritative data in the field of older adults’ health in China. However, some pilot cities are not included in the database. Fortunately, the sample size of this excluded portion is relatively small. The sample proportion of the experimental group is 21.21%, which adequately meets the research needs. Secondly, this study measures health management services from three perspectives: physical examinations, health assessments, and chronic disease management, and employs community health management for robustness testing, basically covering the crucial aspects of health management services. Supplementary research is still required to measure health management services from other perspectives.
Conclusions and Policy Recommendations
Using data from CHARLS spanning 2011 to 2020 and the China Statistical Yearbook, this article empirically analyzes the impact of the integrated medical and elderly care on the utilization of health management services by older adults through the application of the DID, PSM-DID model and the mediation effect test model. It also delves into the heterogeneity and underlying mechanisms. The research findings are as follows: Firstly, the pilot projects integrated medical and elderly care have effectively increased the probability of older adults participating in physical examinations, health assessments, and chronic disease management. These conclusions remain valid after robustness and placebo tests. Second, the integration of medical and elderly care has a higher impact on aged 60 to 80, females, rural residents, and healthy older adults, effectively mitigating inequalities in the utilization of health management services. Thirdly, the integrated medical and elderly care enhances the utilization of health management services by older adults through two channels: increasing policy agglomeration effects and improving service accessibility. All mediation variables exhibit partial mediation effects. The conclusions of this study provide valuable insights for promoting the development of policies integrated medical and elderly care in China and improving health management for older adults.
Based on the above, this paper proposes the following policy recommendations. Firstly, the government should expand the scope of integrated medical and elderly care and consolidate policy outcomes. Given the demonstrated effectiveness of these pilot programs in promoting the utilization of health management services, their coverage should be gradually expanded beyond current areas, with particular emphasis on regions with limited medical resources. Concurrently, a dynamic monitoring mechanism for pilot outcomes should be established, integrating metrics such as physical examination participation rates and chronic disease management coverage into performance evaluations to ensure the efficacy of policy implementation. Additionally, continuous robustness assessments should be conducted to optimize pilot designs in a timely manner, mitigating implementation deviations and reinforcing the core achievement that “integrated care enhances engagement in health management services.” Secondly, implement precision service interventions targeting key populations. Focus on policy-sensitive groups, including individuals aged 60 to 80, women, rural residents, and healthy older adults, and design differentiated service packages: add mobile medical examination vehicles and set up health outreach stations in rural areas to lower the threshold for accessing services; provide targeted health assessments for elderly women (such as gynecological disease screenings); and conduct health education and preventive interventions for young and healthy elderly individuals to delay health decline. Through such precise policy implementation, the disparity in health service utilization across population groups can be further narrowed, and the equitable distribution of health resources can be promoted. Thirdly, strengthen policy coordination and improve service accessibility. On the one hand, integrated medical and elderly care policies of departments such as civil affairs and health commissions to form a “policy agglomeration effect”—for example, incorporating chronic disease management into the scope of elderly care service subsidies and promoting the connection between medical insurance and long-term care insurance benefits. On the other hand, enhance “service accessibility” through measures such as optimizing the layout of community elderly care service centers, promoting family doctor contract services, and simplifying the procedures of health management services. A two-pronged approach will activate the mediating mechanism, forming a closed loop from policy design to service implementation, and maximizing the role of integrated medical and elderly care in promoting health management.
Footnotes
Ethical Considerations
Ethical review and approval were waived for this study, due to the data used in this article coming from the public database, with which all subjects involved are anonymous.
Author Contributions
Lianjie Wang: Writing the draft, data collection, and conceptualization; Jingjing Wang: Data analysis, manuscript sorting, and manuscript revision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Social Science Fund Youth Project of China: Research on Behavioral Measurement, Obstacle Identification, and Refined Governance Pathways for the Integration of older adults into the Digital Society (24CSH113).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.