
Abstract
By referring to Welter’s classification method of “three-point construction” of trust, this paper divides rural older adult trust into three categories: institutional trust, social trust, and emotional trust, discusses the influence of different types of trust on the health status of rural older adults, and reveals the mediating role of active use behavior in the process of trust affecting the health status of rural older adults. The hierarchical regression estimation method and Bootstrap method were used to test the direct effect of trust on the health status of rural older adults and the mediating effect of active use behavior in the process of trust on the health status of rural older adults. On this basis, the moderating effects of institutional endowment resources, social mutual endowment resources, and family endowment resources supply the environment for the process of trust affecting the health status of rural older adults, are analyzed. The empirical results show that: (1) Institutional trust, social trust, and emotional trust have significant positive effects on the health status of rural older adults; (2) The active use behavior of rural older adults plays a mediating role in the process of trust affecting their health status, but the effect degree is not high on the whole; (3) The moderating effects of institutional resources, social capital and family resources on the influence of trust on the active use behavior of rural older adults are not consistent. Accordingly, the corresponding policy enlightenment is drawn.
Introduction
Integrating healthy ageing into the entire process of economic and social development is a key task in strengthening work on ageing in the new era. At present, the aging of the population is intensifying, which leads to the increase in the prevalence of chronic diseases, disability, and mortality among older adults, which will inevitably lead to an increase in the demand for medical and health services and pension services for the older adults. However, due to the influence of regional economy, social environment, family culture, and other factors, it is difficult for some older adults’ medical and old-age service needs to be transformed into actual medical and old-age service needs. In rural areas, medical and health resources are relatively scarce compared with urban areas, coupled with the outflow of young labor force and the weakening of intergenerational support, which alienates the traditional “hometown” and “family” relations, resulting in increased difficulty for rural older adults to obtain medical and old-age service resources, thus affecting the health status of rural older adults. As a result, it has become more difficult for older adults in rural areas to access medical and elderly care resources, affecting the health of rural older adults. In this regard, the Party and the government have made efforts to promote the equalization of basic public health services in urban and rural areas and the development of rural mutual-help old-age care services, to provide a strong guarantee of access to healthcare and old-age care services for rural older people, and a series of efforts have already been carried out in rural areas (Zhang & Shang, 2020) . However, in Chinese practice, it has been found that rural residents’ trust in providing of basic public health services is still insufficient, and the inherent social networks in rural areas are weakening (Liang & Chen, 2021), constraining rural older people’s access to healthcare and old-age resources. Trust, as a core mechanism for bridging formal institutional gaps and providing sustained emotional support, has been shown to promote civic engagement, enhance satisfaction with public services, strengthen subjective well-being, and promote psychological well-being among older adults (Bao et al., 2022; Li & Gao, 2020; Ma & Huang, 2022; Zhou et al., 2023). Existing literature underscores that health status, as a multidimensional construct, typically encompasses domains such as self-rated health, mental well-being, and functional capacity in activities of daily living. These dimensions collectively reflect individual physiological functioning, psychological adaptation, and socio-functional integration. Trust, serving as a core component of social capital, has been extensively demonstrated to influence health outcomes through mechanisms including facilitating resource acquisition, reinforcing social support networks, and enhancing psychological security. Notably, rural elderly populations exhibit systematically poorer health profiles compared to their urban counterparts, necessitating urgent exploration of ameliorative pathways through social support mechanisms. In China’s rural contexts, characterized by scarce medical resources and fragmented relational networks, trust mechanisms assume particular significance in mitigating health resource inequities. This study posits that trust-based interventions could operate as critical mediators in bridging health access gaps, thereby offering actionable insights for policy formulation targeting rural health equity. Then, how should the trust mechanism of rural older adults be reshaped to promote healthy aging? This paper will conduct an in-depth study on this issue.
Focusing on the realistic background of comprehensively implementing the national strategies of rural revitalization and actively coping with population ageing, and combining with the reform practice of healthy ageing in rural areas, this paper draws on Welter’s classification of the “three-part construct” of trust. It classifies the trust categories of the older adults in rural areas into three categories: institutional trust, social trust, and emotional trust. (1) Since the launch of the “new healthcare reform” in 2009, governments and health departments at all levels have provided free basic public health services to older adults in rural areas, which has provided a strong guarantee for older adults to carry out disease prevention and chronic disease management. In addition, governments around the world are actively exploring the extension of professional institutional services to communities and families, increasing the effective supply of home-based community older adults care services, and committing to innovative home-based community older adults care service models, which provide policy support for rural older adults to access older adults care services. Therefore, this paper defines rural older adults’ knowledge and acceptance of policy-based healthcare and older adults’ care resources as institutional trust. (2) In the acquaintance society, under the background of weakening intergenerational support, rural older adults can form a benign village mutual support mode for old-age care based on their own needs, interests, and living environment, increase social capital, and improve medical and old-age service security. At present, most regions have established mutual-help older adults care platforms such as village neighborhood mutual-help points and rural homes for happiness, which provide effective ways for older adults to obtain assisted meals, medical care, recreation, and psychological comfort services. Psychological comfort services, therefore, this paper defines rural older adults search for and identification with acquaintances’ social mutual aid medical and older adults care resources as social trust. (3) The increasingly prominent trend of rural family miniaturization and empty nesting has had a greater impact on the traditional family old-age relationship. However, the weakening of the family old-age function in rural areas is not entirely equivalent to the loss of filial piety. A number of studies have shown that the children’s going out to work has not completely weakened the old-age support for their parents (Tian, & Xu, 2020), and some scholars believe that changes in the structural relationship of the family have a positive correlation with the economic support and spiritual comfort of the parents. Spiritual comfort and other related factors have a positively correlated influence relationship (Song & Li, 2008; Yu et al., 2017); therefore, in the context of the outflow of young labor, changes in family structure, and changes in traditional intergenerational support models, this paper defines emotional trust as the recognition and adaptation of rural older adults to the above heterogeneous family pension service resources. Based on this, this paper will explore the impact of institutional, social, and emotional trust on the health status of rural older adults from the perspective of institutional trust, social trust, and emotional trust.
It is important to point out that trust does not directly translate into the efficiency of old-age services for rural older adults. However, it only means that rural older adults have the opportunity to perceive and identify old-age service resources. The process of transformation also relies on rural older adults to actively identify and use institutional old-age resources, social and mutual old-age resources, and family old-age resources, so this paper will explore the role of active use of the behavior of the trust in the process of the influence of the health status of rural older adults. Therefore, this paper will explore the role of active utilization behavior in the process of trust influencing the health status of rural older adults. In addition, due to the different pension policies issued by governments at different levels, as well as regional economic, social and humanistic differences, which makes the pension service resources available to rural older adults have heterogeneous characteristics, so this paper will further discuss the moderating role of the resource supply environment in the process of trust affecting the health status of rural older adults.
Theoretical Analysis and Research Hypotheses
Based on the above analysis, this part will explain the relationship between institutional trust, social trust, and emotional trust and the health status of rural older people from the theoretical level, explore the mediating role of rural older people’s active use of behavior in this process, analyze the moderating roles of the resource supply environment and the social capital environment in this process, and put forward the corresponding hypotheses.
Institutional Trust and the Health Status of Rural Older Adults
Institutional trust is mainly reflected in rural older adults’ knowledge and recognition of policies related to basic rural old-age service facilities, rural old-age security, and basic public health services provided by the government. Adequate institutional trust helps to enhance residents’ psychological recognition of policies, which leads to positive health behaviors (Nie & Wu, 2021). Conversely, institutional mistrust exacerbates rural residents’ negative risk perceptions concerning social security, economic income, living environment, and psychological well-being, thereby contributing to a decline in their quality of life (Osei et al., 2021; Zou et al., 2023). Additionally, the negative feedback from rural residents caused by institutional mistrust will in turn affect rural leaders’ willingness to participate in public affairs, thereby further impacting farmers’ own lives and creating a vicious cycle (Mengjuan et al., 2023). Wen (2021) argued that the relevant older adults policy in rural areas carries multiple functions, such as rural life care, emotional comfort, value realization, etc., and effectively solve the challenge of insufficient accessibility of rural older adults services, thus enhancing the health status of the older adults. Zhao (2021) pointed out that rural old-age security relies on the active participation of older adults, and needs to be fully integrated with the subjectivity, conscientiousness, and creativity of rural farmers to improve the efficiency of old-age security provision, thereby improving the quality of older adults health and old age. Zhang and Miao (2020) found that basic public health services reduce the health gap between residents while improving the health knowledge of the poor and promoting their health behavior. At present, the construction of a policy system and social environment for old age, filial piety, and respect for older adults have become a key task for the work on aging in the new era, which also provides an institutional guarantee for actively responding to the reality of the challenges of rural population aging. Accordingly, this paper puts forward the following hypotheses:
Social Trust and the Health Status of Rural Older Adults
Social trust is mainly reflected in the active participation of rural older people in social activities, volunteer services, and mutual care. Xie et al. (2021) found that the higher the level of social participation of older Chinese people, the stronger their social adaptability. Chen et al. (2019) pointed out that the active integration of older people into society can significantly improve their cognitive ability and health status. Bi (2011) used qualitative research to find that participation in volunteering can meet the psychological needs of corporate physically disabled people and positively affect their mental health status. Gao and Wen (2019) analyzed the impact of volunteering participation on the health of urban older adults, and the results showed that participation in volunteering activities can significantly improve the health of urban older adults. In mutual care, Liu (2022) pointed out that the development of village and community mutual care is an effective way to actively deal with rural aging, and the participation of low-age older people in mutual care is not only enjoyable but also productive and spiritually fulfilling. Le and Qin Xi (2020) believe that the participation of older adults in social mutual aid can be pleasurable both physically and mentally, and at the same time, in the process of meeting the health needs of others in old age to realize their value, to better enjoy their later life. Accordingly, this paper proposes the following hypotheses:
Emotional Trust and the Health Status of Rural Older Adults
Emotional trust is mainly reflected in the degree of adaptation to the changes in the traditional intergenerational support model received by rural older adults, and their awareness of heterogeneous family resources for the older adults. Many studies in the field of health economics have explored the changes in parental health status in the context of changes in intergenerational support patterns for children and heterogeneous family aging, which can be broadly categorized into two views: the “health-promoting view” and the “health-suppressing view.” Among them, the “:health promotion theory” believes that changes in the traditional intergenerational support model can bring parents more economic support, which is conducive to improving their quality of life and ability to pay for medical care, thus positively affecting parental health (Böhme et al., 2015); the “health suppression theory” believes that changes in the traditional intergenerational support model can bring parents more economic support, which is conducive to improving their quality of life and ability to pay for medical care, thus positively affecting parental health. “Inhibition theory” suggests that changes in traditional intergenerational support patterns affect children’s care and emotional comfort for their parents, increase their burden of housework and labor, and thus have a negative impact on their health (Huang et al., 2016). Wang and Zhou (2020) pointed out that the relationship between changes in intergenerational support patterns and parental health has been a hot topic of general concern for scholars in China, and his study concluded that after children go out, the health status of rural left-behind parents exists both a positive economic support effect and a negative time-loss effect. Therefore, after the change of the traditional intergenerational support model, increasing the understanding and trust of rural older adults in their children will help to improve their health status. Accordingly, this paper proposes the following hypothesis:
The Mediating Role of Active Use Behavior Among Rural Older Adults
A number of scholars in existing studies have tested the relationship between the impacts of trust on health (Mkhize, 2023; Deng et al., 2021). However, trust is not equivalent to resource digestion and absorption, the process also requires active utilization by the participating subjects, which has been argued by a number of studies, for example, Xu et al. (2022) found that older people’s trust in, and active utilization of, basic public health services can help to improve their disease prevention and health management. Shang and Zhao (2022) argued that social transformation and changes in family structure have had a certain impact on traditional family pensions in rural areas, but rural older people have made up for the lack of family pension resources by utilizing policy resources such as the New Rural Cooperative and the New Rural Insurance, which has cracked the pension dilemma of rural residents. Li and Gao (2020) pointed out that the effect of interpersonal trust on mental health under the social network perspective relies on the mediating role of interpersonal interactions and reciprocal behaviors. Ma et al. (2021) found that after the weakening of the family old-age function, children’s financial support has a significant and robust positive effect on the older adults’ consumption choice of institutional old-age care, which provides a useful guarantee of their healthy old-age. Accordingly, this paper proposes the following hypothesis:
The Regulatory Role of the Resource-Supplying Environment
The resource-supplying environment is mainly characterized by institutional resources, social capital, and family resources in the rural old-age situation. Although institutional trust, social trust, and emotional trust may all have a certain impact on the health status of rural older people, there are differences in regional economic, social, and cultural development, which makes the type of older adult care practice in China show differentiated characteristics across the country (Gan, 2022), which results in an inconsistent supply environment for the older adults care resources, which may affect the rural older people’s initiative to use the accessibility of the above resources. For example, Feng et al. (2008) argued that rural old-age security objects have different group characteristics, coupled with the impact of factors such as uneven regional economic development, the supply of rural social pension insurance system is not the same at this stage. Yao and Zhang (2018) pointed out that at the current stage of the pension policy is not only the policy content is complex, but the design, organization, matching, and use of various policy tools also profoundly affect the policy effect. Zhao (2020) argued that due to the changes in China’s social structure, traditional social capital has been lost, which hinders interpersonal mutual aid and interaction, thus restricting the quality of mutual aid for older adult care services. Chen and Huang (2018) study concluded that the massive export of rural labor force has caused empty nesters to face a double lack of social capital at the individual and collective levels, which in turn affects the health status of rural older adults. In terms of family resources, scholars have found that the number of children is significantly negatively correlated with caregiving support for rural older adults (Yin & Liu, 2017), while caregiving support significantly and positively affects the self-assessed health of rural older adults (Bai, & Gu, 2021). Accordingly, this paper proposes the following hypothesis:
Study Design
Date Sources
The data used in this paper come from the China Longitudinal Aging Social Survey (CLASS) implemented by the China Survey and Data Centre of Renmin University of China. The data employed in this study were derived from the China Longitudinal Aging Social Survey (CLASS). Specifically, the 2018 CLASS dataset represents the most authoritative and methodologically rigorous publicly available database that systematically integrates multidimensional indicators, including trust levels, active use behavior, and health status among rural elderly populations. Employing a cross-sectional research design with stratified multistage probability-proportionate-to-size sampling (PPS) methodology, this large-scale social tracking survey was conducted across 28 provincial-level administrative regions in China. Targeting adults aged 60 years and older, the survey comprehensively captured respondents’ demographic characteristics, health indicators, socioeconomic conditions, social support networks, psychological well-being, and family dynamics, yielding a dataset characterized by robust national representativeness and analytical reliability. According to the research design and object selection of this paper, the research group screened and excluded some incomplete data, and obtained a total of 3,078 valid sample data.
Variable Description
(1) Dependent variable. The dependent variable is the health status of rural older adults. Focusing on the basic connotation of health and combining the content and results of the questionnaire survey of the 2018 China Learning to Age Socially Tracking Survey (CLASS), the three dimensions of self-assessed health, mental health, and daily activity ability were selected to examine the health status of rural older adults, and the specific scale design is shown in Table 1.
(2) Independent variables. The independent variable is trust. Combined with the content and results of the questionnaire survey of the 2018 China Learning to Age Socially Tracking Survey (CLASS), its influence on the health status of rural older adults was examined in the three dimensions of institutional trust, social trust, and emotional trust, and the specific scale design is shown in Table 1.
(3) Mediating variables. The mediating variable is the active utilization behavior of rural older adults. Combined with the content and results of the questionnaire survey of the 2018 China Learning to Age Socially Tracking Survey (CLASS), the mediating role in the process of trust influencing the health status of rural elder people was studied from the three dimensions of elder people’s proactive utilization of basic public health services, proactive utilization of community assistance services, and proactive utilization of old-age security services, and the design of the specific scales is shown in Table 1.
(4) The moderating variable is the resource supply environment. Combining the content and results of the questionnaire survey of the 2018 China Learning to Age Socially Tracking Survey (CLASS), the moderating role of institutional resources, social capital, and family resources in the process of trust influencing the active utilization behavior of rural elder people is examined, and the specific scale design is shown in Table 1.
(5) In alignment with the structured framework of the 2018 China Learning to Age Socially Tracking Survey (CLASS) questionnaire and the analytical requirements of this study, four demographic factors were strategically incorporated as control variables: gender, age, educational attainment, and marital status. These variables were selected from the survey’s core demographic module to account for potential confounding effects arising from fundamental socio-demographic characteristics that may influence the relationship between key study constructs, and the specific scale design is shown in Table 1.
Description of the Core Variables.

Model building
Direct effect and mediation effect model
The selection of statistical methodologies and subsequent analytical procedures in this study were implemented under the professional guidance of statisticians. This paper adopts the hierarchical regression estimation method to test the direct effect of trust affecting the health status of rural older adults, and the mediating effect of active utilization behavior in the process of trust affecting the health status of rural older adults. The specific model is as follows.



In Equations (1), (2), and (3), Y denotes the health status of rural older adults; X denotes trust; M denotes the active utilization behavior of rural older adults;
Moderating Effect Model
To test how the resource supply environment affects the direction and strength of trust and the active utilization behavior of rural older adults, this study adopts the moderating effect model, the specific model is as follows.

Where M is the active utilization behavior of rural older adults, X is the independent variable trust, and W is the moderating variable resource supply environment.
Empirical Analyses
Descriptive Statistics
To facilitate the analysis, this paper has operationalized some of the variables, in which the scores of the dependent, independent, mediating, and moderating variables are the arithmetic mean of the scores of each question item, and the results of the descriptive statistical analysis are shown in Table 2. It is not difficult to see that the mean value of rural older adults’ ability to perform daily activities is 1.941, while the mean values of mental health and self-perceived health are 1.365 and 1.325, which infers that Rural older adults generally have a strong ability to perform daily activities, but their mental health and self-perceived health are relatively weak. In addition, the mean value of institutional trust is 1.235, the mean value of social trust is 1.264, and the mean value of emotional trust is 1.941, indicating that against the background of the weakening of the family’s function of providing for the older adults and the gradual increase in the support of the state and society, rural older adults’ awareness of the resources for providing for the older adults within the family is still higher than that of the policy-based medical resources for providing for the older adults and the village mutual aid-type medical care and resources for providing for the older adults. The mean value of the active use of basic public health services by rural older adults is 1.126, the mean value of the active use of community assistance services is 1.007, and the mean value of the active use of old-age security services is 1.027, indicating that the level of the active use of basic public health services by rural older adults is higher than that of the active use of community assistance services and old-age security services, but that the overall active use of such services is at a lower level. With regard to the environment for the supply of old-age resources, the mean value of institutional resources is 1.114, the mean value of social capital is 1.360, and the mean value of family resources is 1.417, which indicates that the level of resources possessed by rural elder persons from within the family is higher than that of resources for old-age care from the outside, but that rural older adults as a whole live in a poorer environment for the supply of resources for old-age care.
Descriptive Statistics of Variables.

Hypothesis Testing
In this paper, the hierarchical regression estimation method is used and all regressions use heteroscedasticity robust standard errors. Multiple covariance diagnosis is also performed for all regression models, and the results show that the variance inflation factors (VIF) are all around 1.0, indicating that the degree of correlation covariance between variables is within reasonable limits and there is no serious covariance problem.
Table 3 shows the results of the hierarchical regression test, equation 1 and Equation 2 tested the direct effect of trust on the health status of rural older adults, where Equation 1 tested the relationship between the control variable and the dependent variable, and Equation 2 tested the effect of institutional trust, social trust and emotional trust on the health status of rural older adults. Equation 3, Equation 4, and Equation 5 tested the mediating role of active utilization behavior in the process of trust affecting the health status of rural older adults, where Equation 3 tested the relationship between the control variables and the active utilization behavior of rural older adults, Equation 4 tested the effect of institutional trust, social trust, and emotional trust on the active utilization behavior of rural older adults, and Equation 5 tested the effect of the active utilization behavior of rural older adults on their health status.
Hierarchical Regression Test Results.
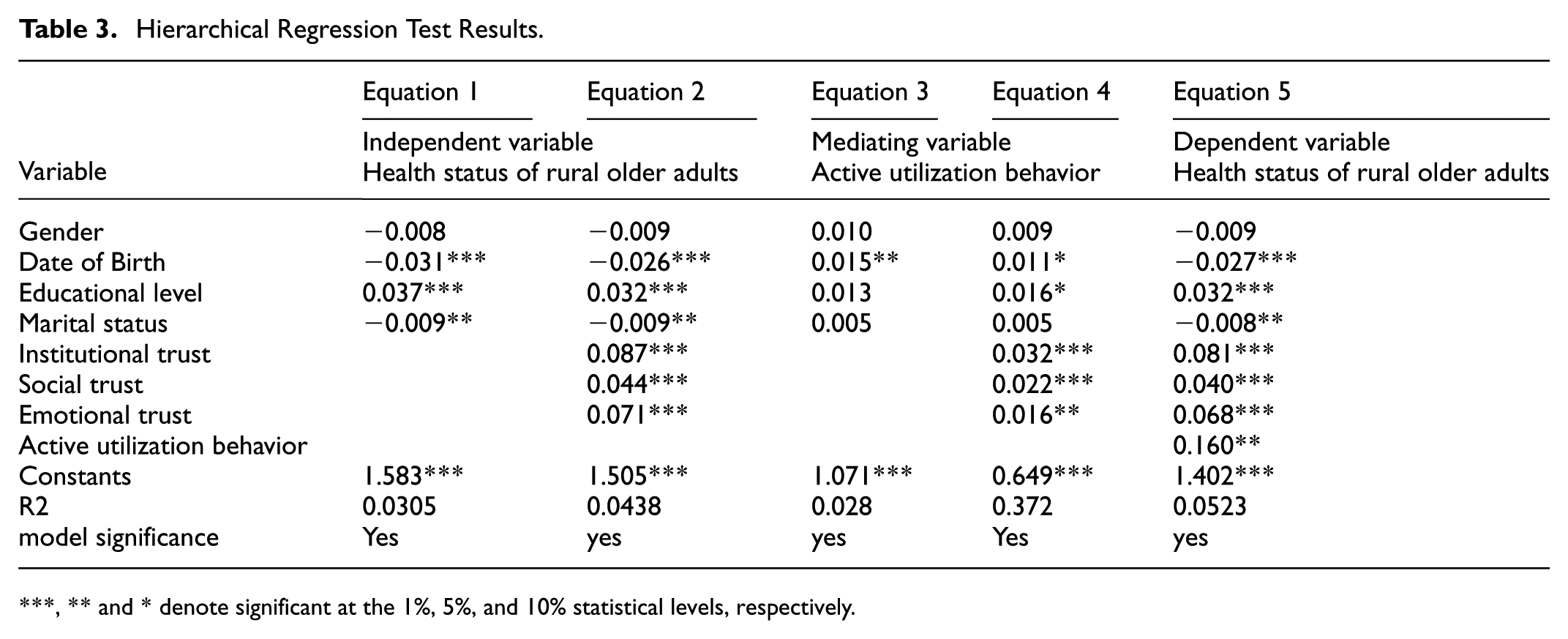
, ** and * denote significant at the 1%, 5%, and 10% statistical levels, respectively.
As shown in Table 3, Equation 1 shows that rural older adults’ year of birth and marital status have a significant negative impact on their health status, educational level has a significant positive impact on their health status, and gender has a non-significant impact on their health status. The results of Equation 2 show that institutional trust, social trust, and emotional trust all have a significant positive effect on the health status of rural older adults, that is, hypothesis H1 is valid. It means that rural older adults’ recognition of policy, social participation, and adaptive ability are all helpful to improve their health status. The results of Equation 3 show that the year of birth of older adults has a significant positive effect on their active utilization behavior, and it is analyzed that, along with the age of the older adults, their demand for basic public health services, community assistance services, and old-age security services increases, and thus their active utilization behavior increases, whereas the gender of the older adults, their education level and their marital status do not have a significant effect on their active utilization behavior. The results of Equation 4 shows that institutional trust, social trust, and emotional trust have a significant positive effect on the active utilization behavior of rural older adults, indicating that rural elder people with higher levels of trust are more inclined to actively utilize basic public health, community assistance, and old-age security services. The results of Equation 5 show that the active utilization behavior of rural older adults has a significant positive impact on their health status. Comparing Equations 2 and 5, it is found that the regression coefficient β value of the impact of institutional trust, social trust, and emotional trust on the health status of older adults decreases after the inclusion of the active utilization behavior, which indicates that the active utilization behavior plays a mediating role in the path of the impact of trust on the health of rural older adults, and initially verifies hypothesis H2.
Table 4 further tests the mediating effect of active utilization behavior of rural older adults in the process of trust influencing their health status using the bias-corrected nonparametric percentile Bootstrap method. The results show that the mediating effect of active utilization behavior of rural older adults in the process of trust influencing their health status is significant, that is, hypothesis H2 is valid. For each independent variable individually, the mediating effect of rural older adults’ active utilization behavior in the process of institutional trust affecting their health status accounted for 6.897% of the total effect, the mediating effect in the process of social trust affecting their health status accounted for 8.211% of the total effect, and the mediating effect in the process of emotional trust affecting their health status accounted for 3.595% of the total effect, which indicates that rural older adults active utilization behavior, although in the process of trust affecting their health status, is significant behavior, although it plays a significant mediating role in the process of trust affecting their health status, the degree of effect is not high overall.
Bootstrap Test for Mediating Effects.

denote significant at the 1% statistical levels, respectively.
Table 5 analyzes the moderating effect of resource supply environment in the process of trust influencing the active use behavior of rural older adults. Equation 6 tests the overall moderating effect of institutional resources, social capital, and family resources in the process of trust influencing the active utilization behavior of rural older adults, and the results show that institutional resources and social capital present a significant positive moderating effect in the process of trust influencing the active utilization behavior of rural older adults, and the analysis suggests that the higher the awareness level of rural older adults of the government-provided policy support initiatives and external resources, such as social voluntary services and mutual care, the more conducive it is to promoting their active utilization. It is analyzed that the higher rural older adults’ awareness of policy support initiatives provided by the government and external resources such as social volunteer services and mutual care, the more conducive it is to promote their active utilization. Family resources, on the other hand, show a significant negative moderating effect in the process of trust influencing the active utilization behavior of rural older adults. To further explore the moderating mechanism, the article further examines the moderating effect of resource supply environment in the process of trust influencing rural older adults’ active utilization of basic public health services, community assistance services, and old-age security services.
Moderated Effects Test Results.

and * denote significant at the 1% and 10% statistical levels, respectively.
Equation 7 tests the moderating effects of institutional resources, social capital, and family resources in the process of trust influencing rural older adults’ active utilization of basic public health services, and the results show that institutional resources and family resources have a positive moderating effect in the process of trust influencing rural older adults’ active utilization of basic public health services, and social capital has a negative moderating effect in the process of trust influencing rural older adults’ active utilization of basic public health services. Social capital has a negative moderating effect on the process of trust influencing rural older adults’ active utilization of basic public health services. The analysis suggests that, in the context of the “society of acquaintances” in rural areas, the more social capital an older adult possesses, the more varied his or her access to healthcare services, which affects his or her active use of basic public health services. Equation 8 tests the moderating effects of institutional resources, social capital, and family resources in the process of trust influencing rural elder people’s active use of community assistance services, and the results show that institutional resources and social capital positively moderated the process of trust influencing rural elder people’s active use of social assistance services, while family resources negatively moderated the process of trust influencing rural elder people’s active use of community assistance services. The analysis suggests that the supply of sufficient family resources has a positive effect on trust. The analysis concludes that the provision of sufficient family resources can guarantee the old-age life and health needs of rural older adults, and thus their motivation to actively utilize community assistance services is insufficient. Equation 9 tests the moderating effects of institutional resources, social capital, and family resources in the process of trust influencing the active utilization of old-age security services by rural older adults. The results show that institutional resources have a positive moderating effect in the process of trust influencing rural older adults’’ active utilization of old-age security services. The moderating effect of social capital in the process of trust influencing the active utilization of old-age security services by rural older adults is not significant, and the analysis concludes that at present, old-age security services in rural areas are mainly supplied by the government on its initiative, so social capital trust does not have a significant effect on the active utilization of old-age security services by rural older adults. Family resources in the process of trust influence rural older adults’ active use of old-age security services in the process of negative moderating effect, the analysis that rural older adults in the traditional “family-oriented” concept of the impact of their active use of old-age security services are mostly manifested as “last resort.” Therefore, once rural older adults have sufficient family resources worthy of their trust, they will not actively seek and actively utilize external support such as old-age security services, which restricts their active use of old-age security services. In summary, hypothesis H3 is partially true.
Discussions
This study empirically elucidates the mechanisms through which multidimensional trust among rural elderly individuals influences their health outcomes, offering a novel theoretical lens and practical foundation for healthy aging policy design. In comparison to existing literature, our findings both corroborate certain established conclusions and reveal distinctive patterns. For instance, the positive health effect of institutional trust aligns with Xu et al.’s (2022) argument regarding policy trust’s role in facilitating service utilization; however, this study demonstrates quantitatively weaker effect sizes compared to social trust, which may stem from fragmented policy implementation and elderly populations’ limited information acquisition capabilities in rural settings (Zhang & Shang, 2020). Furthermore, while the pathway through which social trust enhances health via mutual-aid participation resonates with theory of village-based elderly care efficacy, our moderated mediation analysis reveals a negative regulatory effect on basic public health service utilization. This counterintuitive result likely reflects the substitution effect between informal networks and formal services within rural “acquaintance societies” (Zhao, 2020). With regard to affective trust, our findings support the “health promotion hypothesis”, yet paradoxically indicate that abundant familial resources inhibit pension security service utilization—a phenomenon closely tied to the psychological mechanism of “external dependency stigma” rooted in traditional familial care norms (Chen & Huang, 2018). These discrepancies collectively demonstrate that trust’s health impacts operate through complex interactions with resource environments and socio-cultural contexts rather than linear pathways, thereby constituting a significant theoretical refinement to existing frameworks. This study advocates for contextualized interventions that consider trust’s embeddedness in structural constraints and cultural legacies when addressing rural health inequities.
Conclusions and Implications
This paper systematically explored the relationship between the influence of multiple trusts of rural older adults on their health status. The results of the study show that: (1) institutional trust, social trust, and emotional trust all have a significant positive impact on the health status of rural older adults, that is, the higher the level of trust of rural older adults, the better their health status. (2) Rural older adults active use of behavior plays a mediating role in the process of trust affecting their health status, but the degree of the role is not high overall. This suggests that trust can, to a certain extent, improve rural older adults’ knowledge and acceptance of relevant resources, and promote their active identification and utilization of basic public health services, community assistance services and old-age security services, thus enhancing their health status. (3) Institutional resources play a significant positive moderating role in the process of trust influencing rural elder people’s active use of behavior; social capital plays a significant positive moderating role in the process of trust influencing rural elder people’s active use of community assistance services, and a non-significant moderating role in the process of trust influencing rural elder people’s active use of old-age security services, and a significant negative moderating role in the process of trust influencing rural elder people’s active use of basic Family resources play a significant positive moderating role in the process of trust influencing rural elder people’s active utilization of basic public health services, and a significant negative moderating role in the process of trust influencing rural elder people’s active utilization of community assistance services and old-age security services.
This study offers three pivotal theoretical innovations for health system optimization: First, it conceptualizes a “trust-active utilization-health” chain-mediated pathway, transcending conventional research paradigms that oversimplify the trust-health nexus. This framework establishes an intervention logic of “cognitive guidance → behavioral incentives → resource alignment,” providing actionable insights for policy design. Second, it identifies the pivotal moderating role of institutional resources in trust translation, suggesting that governments should enhance the supply of aged-care infrastructure and refine policy dissemination strategies through dialect-based and community-centered communication to strengthen institutional trust efficacy. Third, the heterogeneous moderating effects of social capital and familial resources are revealed, advocating for the integration of specialized services into community-based mutual-aid models to circumvent informal network limitations, while implementing intergenerational communication education to mitigate the crowding-out effect of familial resources on formal health services. Future research should further explore: (1) the empowering role of digital technologies (e.g., AI-assisted health monitoring) in trust construction, and (2) the threshold effects of collaborative trust-based interventions across multiple governance levels. These investigations would contribute to developing dynamically adaptive solutions for achieving healthy aging in resource-constrained contexts.
Based on the findings of the study, the following policy implications have been drawn: first, strengthen the publicity and guidance of heterogeneous old-age resources, and reshape the trust mechanism of rural older adults. The results of the analysis show that institutional trust, social trust, and emotional trust all help to improve the health status of older adults. Therefore, against the background of the increasing abundance of institutional resources for older adults, the growing importance of social resources for older adults, and the heterogeneity of family resources for older adults, it is important to strengthen publicity and guidance to reshape the older adults knowledge of and trust in multiple categories of resources for the older adults, which will help to improve their health status. Secondly, innovate the supply mode of older adult care services to stimulate the level of active utilization by rural older adults. Research results show that the active utilization behavior of rural older adults play a mediating role in the process of trust influencing their health status. Therefore, governments and organizations at all levels need to further innovate the supply mode of old-age services, enrich the content of all kinds of old-age services, and motivate and enhance the enthusiasm of rural older adults to actively use old-age resources, to improve their health status. Thirdly, to improve the quantity of institutional resources supply, empirical analysis found that institutional resources play a significant positive moderating role in the process of trust influencing the active use of rural older adults, therefore, the government needs to further increase the quantity of rural basic pension service facilities, rural pension security, basic public health services and other related institutional pension resources supply, to ensure that rural older adults active use of old-age resources accessible, which has a positive impact on their trust and active use of old-age resources. This will have a significant effect on their trust in and active use of old-age resources.
Footnotes
Ethical Considerations
The data utilized in this study were sourced from the public database. The project adhered to the ethical guidelines stipulated in the Declaration of Helsinki and received formal approval from the institutional review board prior to data collection. As this study exclusively employs de-identified, publicly available datasets, no additional ethical review was required.
Consent for Participate
Informed consent procedures for the survey were rigorously implemented. All participants provided voluntary, written consent after being fully informed of the study’s objectives, data usage protocols, anonymity safeguards, and their right to withdraw at any stage. Given the secondary nature of this analysis and the public accessibility of the data, no further consent was solicited from individual participants.
Funding
This research was funded by the National Natural Science Foundation of China under the General Program titled “Research on the Driving Path and Long-Term Mechanism of Urban and Rural Residents’ Proactive Participation in Insurance Based on Policy Experience Utility (Grant No. 72574086)” and the Social Science Project of Jiangsu Province titled “Research on the Mechanism and Policy of Digital Intelligence Empowering the Integration of Medical Care and Public Health at the Grassroots Level in Jiangsu Province under the Background of Coexisting Multiple Diseases (Grant No. 24GLB023)”.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets employed by the researchers in the analysis of the study is available by the authors upon reasonable request. We confirmed that informed consent was obtained from all participants.