
Abstract
Somalia has developed its first National WASH Sector Policy to increase equitable access to sustainable sanitation facilities, promote large-scale hygiene behavior change, and eliminate open defecation, in alignment with national priorities and the Sustainable Development Goals, notably Target 6.2, to ensure universal access to adequate and equitable sanitation and hygiene facilities. Therefore, this study aims to evaluate the disparities in access to improved hygiene facilities between rural and urban households. The study used cross-sectional data from the Somali Integrated Household Budget Survey (SIHBS) 2022, which analyzed a total of 7,212 households. The Pearson Chi-square test for independence was adopted to assess the association between predictor and outcome variables. The Fairlie decomposition assessed how much rural-urban disparities in access to improved hygiene facilities are explained by the predictors. The multivariate logistic regression was applied to determine if the predictors are significantly associated with the outcome variable. This study reveals that 32.5% of households had access to improved hygiene facilities. Based on logit model, sex (AOR: .844, 95% CI [.767, .929]), education of the household head (AOR: .881, 95% CI [.777, .999]), household water treatment (AOR: .775, 95% CI [.703, .855]), poverty status of the household (AOR: .636, 95% CI [.579, .699]) and type of residence (AOR: .861, 95% CI [.779, .952]) were all significant predictors associated with access to improved hygiene facilities. This highlights a lack of understanding of education, water treatment, and financial constraints as structural barriers to accessing improved hygiene facilities in rural areas. Addressing these concerns is crucial for improved hygiene facilities.
Keywords
Introduction
Since 2015, the population with access to fundamental hygiene facilities has increased by more than 500 million, from 5 billion (67%) to 5.5 billion (71%). In 2020, 2.3 billion people lacked basic hygiene, with 670 million not having access to a handwashing facility (WHO/UNICEF/JMP, 2020). This is because a number of nations have acquired fresh data indicating better coverage than prior surveys. More than half of those without access to facilities, around 374 million, lived in unstable or conflict-affected areas. Data on basic hygiene services were available for 79 nations and four of the eight SDG areas, representing over half of the world’s population. Four countries have already achieved almost universal access (more than 99%) to basic hygiene services, with six more were on track to reach this goal between 2020 and 2030. Meanwhile, in 16 nations, there was a greater than 20%-point gap in basic hygiene coverage between urban and rural areas, and in 12 countries, the disparity between the best- and worst-performing regions exceeded 50% points (WHO/UNICEF/JMP, 2020). Previous research on urban-rural disparity demonstrates spatial variability. Colombia has the largest inequality, 37.1%, whereas Turkmenistan has the lowest urban and rural differences (a value of zero; Quispe-Coica & Pérez-Foguet, 2020). In 2020, the COVID-19 pandemic brought significant attention to the importance of hand hygiene like never before. A prior study revealed that mothers washing their hands with soap before a meal or after defecation were 15% less likely to have stunted children (Rah et al., 2015).
A previous study found that one in every four persons globally does not have access to a handwashing facility with soap and water on premises, and only 26% of possible fecal encounters are followed by handwashing with soap (Wolf et al., 2019). Improved water, sanitation, and hygiene (WASH) promote the fundamental universal healthcare principles of quality, justice, and dignity for all (Kayiwa et al., 2020). Handwashing facilities with soap and water on facility premises are a worldwide indicator of Sustainable Development Goal (SDGs) 6.2.1b (Walsh et al., 2022). The World Health Organization urged nations to ensure that public handwashing facilities are universally accessible and to mandate their use when entering and exiting both public and private facilities, along with public transportation locations (WHO/UNICEF/JMP, 2020). Safe drinking water, sanitation, and hygiene are essential for maintaining human health and well-being. Clean WASH promotes good health, increases livelihoods, school attendance, and enhances dignity (H. A. Ahmed & Ali, 2024). Regular hygiene habits are frequently considered by society as desirable and well-mannered activities, but neglecting to maintain hygiene can be perceived as unpleasant, disrespectful, or even possibly hazardous (Ali et al., 2025).
Progress toward the SDG target on hygiene is monitored through indicator 6.2.1b, “the proportion of the population with handwashing facilities with soap and water at home.” Handwashing facilities are now available in 60% of the world, but it remains difficult, particularly in Sub-Saharan Africa, where just 25% of the population has access to them, with one in every four individuals able to use facilities with water and soap (Ssemugabo et al., 2021). Achieving sustainable development goals (SDGs) targets 6.1 and 6.2, which include ensuring access to safely managed drinking water, sanitation, and basic hygiene services for all, is a major challenge, particularly in peri-urban and informal settlements, due to inadequate progress in water, sanitation, and hygiene services (Aydamo et al., 2023). Based on a nationally representative report from six countries, it portrays 39% lack handwashing soap. Handwashing with soap is a cost-effective way for reducing the spread of infectious in healthcare settings and priority for hygiene monitoring (Ali et al., 2025; WHO/UNICEF/JMP, 2020).
However, a 100 million individuals contract illnesses every year as a result of inadequate handwashing practices, which are exacerbated by a lack of available handwashing supplies and facilities. Health care providers frequently fail to comply with handwashing regulations, and thus frequently transfer illness (Cronk & Bartram, 2018). Hand-washing facilities in urban areas remain low, at 39.6% (UBOS, 2016). Overall, in Sub-Saharan Africa, hygiene practices are inadequate, particularly in rural areas. This is a severe matter since poor hygiene practices by households may offset the benefits of utilizing clean drinking water (Ohwo, 2019). Many studies have revealed that disparities in water and sanitation coverage exist between socioeconomic categories, with gaps in coverage across geographic areas within a nation (Baayenda et al., 2018). For instance, Bangladesh has made significant progress in providing improved sanitary facilities over the years, but the disparity between rich and poor remains a matter of concern (A. Ahmed et al., 2023) while Disparities in improved hygiene services are widely observed across India in terms of social, economic, cultural, and infrastructural variance (Kumar et al., 2024). Notably, there are significant rural-urban disparities and geographical variations in the utilization of improved sanitation in Bangladesh (Biswas et al., 2022; Chaudhuri & Roy, 2017).
In Somalia, access to sanitary facilities is quite limited. Only 38% of the population has access to basic sanitation facilities; rural regions have fewer facilities than urban areas, and people defecate in the open in rural areas than in urban areas (WHO and UNICEF, 2019). Different methods of handwashing are used across places of residence, and a third of the population use soap and water to wash their hands. Urban residents use soap and water the most, followed by rural residents, and very few nomads use soap and water for handwashing (SNBS, 2022). The WASH sector’s strategic plan in Somalia aims to improve access to safe, affordable, equitable, sustainable, and quality water and sanitation services, as well as increased adoption of hygienic practices at the personal, household, and community levels, resulting in (i) reduced morbidity and mortality rates and (ii) improved people’s health, productivity, and quality of life (FGS, 2019b). According to the WASH KAP Survey 2015, less than half of the population has a general hand-washing facility, among those with hand-washing facilities (FGS, 2019b). Furthermore, household access to sanitary services and availability to hand-washing facilities near toilets is quite low, while availability to water near toilets is also low, as nationwide. The prevalence of open-air defecation is high, whereas the bulk of nomads defecate in the wilderness (FGS, 2019a).
Limited studies that may provide information to impact programming for improved hygiene facilities have been undertaken in Somalia, including a study on the determinants of water, sanitation, and hygiene (WASH; Ali et al., 2025) and research on universal coverage (what it takes for fragile nations): a case study of the Jariban (Mafuta et al., 2021). Access to basic sanitation facilities varies greatly across rural and urban households in Somalia, posing major challenges to public health and development. Understanding the factors that contribute to the gap is crucial for achieving the Sustainable Development Goals (SDGs) and improving environmental and public health through evidence-based solutions. Limited studies have addressed rural-urban variations in households’ access to improved hygiene facilities (Ali et al., 2025; Keleb et al., 2024). Prior studies have widely employed the decomposition analysis approach to investigate rural and urban differences in water, sanitation, and hygiene (WASH) facilities among households globally (Ayele, 2025; Chaudhuri & Roy, 2017; Keleb et al., 2024; Kumar et al., 2024), while studies in Somalia mostly utilized logit, probit, multilevel logistic regression, and machine learning model estimations to address WASH status (Ali et al., 2025; Ismail et al., 2024). Therefore, to the best of our knowledge, this is the first study in Somalia to apply Fairlie decomposition analysis to assess rural-urban variations in access to improved hand hygiene facilities among Somali households using SIHBS 2022, a nationally representative dataset.
Method and Materials
Study Context
Somalia, formally known as the Republic of Somalia, is situated in the Horn of Africa and covers around 637,657 km2. Its topography is mostly composed of plateaus, plains, and hills. The country has the longest coastline on the African continent, spanning 3,333 km between the Gulf of Aden in the north and the Indian Ocean in the east and south. Somalia shares borders with Djibouti to the northwest, Ethiopia to the west, and Kenya to the southwest. Somalia experiences a hot tropical climate characterized by minimal seasonal fluctuations and average daily temperatures ranging from 30°C to 40°C. In terms of socioeconomic distribution in Somalia, education is a fundamental right and one of the most significant determinants for a country’s long-term social and economic growth. Just over half of the population, 53.7% is literate. The literacy rate is higher among males than females at 63.6% and 45.3%, respectively and nearly two-thirds 65.5% of the Somali population have no formal education. The educational level most commonly reported is some primary education, as this group represents 16.6% of the population. Solely 4.6% of the population claims to have completed secondary education, and 4% attained higher education. The national average household size is 6.7; however, there are substantial differences between urban and rural/nomadic areas (SNBS, 2022). The nationwide incidence of multidimensional poverty, also known as the poverty rate or headcount ratio, was estimated to be 67.0%. Rural and nomadic areas have high rates of multidimensional poverty, with 74.3% and 81.5%, respectively. Urban areas have the lowest incidence 61.7%, with 6 out of 10 persons experiencing multidimensional poverty (MoLSA and SNBS, 2024).
Sampling Procedure and Data Source
We used data from the Somali Integrated Household Budget Survey (SNBS, 2022). This study applied a cross-sectional method to explore rural and urban disparities in access to improved hygiene facilities among households and associated predictors. The target population for this study is all Somali households. A sample size of 7,212 households from 17 Somali regions, including urban, rural, and nomadic areas, was analyzed. Sampling weights were used to confirm representativeness and account for a non-proportional distribution throughout regions, rural and urban disparities, and anticipated response rate differences. The 2022 SIHBS sampling frame was designed using a stratified multi-stage cluster design. Both urban and rural regions were applied a stratified cluster sample approach with three stages, whereas nomadic locations utilized a stratified cluster sample strategy with two stages. The primary sampling units (PSUs) were chosen based on a probability proportional to the number of dwellings in the sample frame. The secondary sampling units (SSUs) were selected for both urban and rural areas based on the number of households stated in the frame. The ultimate sample units (USUs) for rural, urban, and nomadic regions were selected randomly from the cluster’s listed households. To begin, all households in the sample frame in the specified urban, rural, and nomadic Enumeration Areas (EAs) were included as the first level, which included information on the household head.
The data was cleaned, and a summary of households listed by EA was used to create household sample frames for the second stage of sampling; 12 households were chosen from each EA within each stratum. The primary interview focus was the head of household (HoH) and/or their spouse. The survey sample was drawn from 601 EAs located throughout Somalia. Each of the 17 regions included in the study had 35 EAs sampled. Within each EA, 12 households were questioned, totaling 420 households per area. The survey excludes Middle Juba, the 18th pre-war region, due to security concerns. The data was gathered from May 10th to July 31st, 2022. The nationwide response rate was 96%. The highest response rate was among nomadic households, 99% followed by rural households 97% and urban households 95% (SNBS, 2022).
Data Quality Assurance
Data collection was subject to rigorous quality control standards that were implemented at various stages of the field activities. Quality assurance techniques involved supervised interviews, spot-checks, back-checks, and automated high-frequency data checks. Each area has an independent quality control team reporting to the project manager. Supervisors monitored 10% to 15% of interviews to assess and improve interviewer performance, with a focus on mistakes during the first several days of data collection. Meanwhile, 5% of the interviews were back-checked (SNBS, 2022).
Study Variables and Measurements
Dependent variable: The dependent variable of the study is “household access to improved hand hygiene facilities.” In SIHBS 2022, household heads were asked to report on these two questions. (i) Please show me where members of your household frequently wash their hands and (ii) observe for the presence of soap, detergent, or other cleansing agent (bar, liquid, powder, ash, mud, sand, none), etc., at the handwashing station. Direct observation of behavior is difficult, but household surveys increasingly include a module in which the surveyor visits the handwashing facility and observes if water and soap are present (WHO/UNICEF/JMP, 2020). Finally, the dependent variable was created as a binary variable (coded as 1 = for improved, if the household had access to water and soap or other cleaning agents, and 0 = for unimproved, if it had no).
Independent variable(s): The explanatory variables were found based on literature: sex of the household head (1 = male, 2 = female) (Gizaw et al., 2023), age of the household head (1 = 15–34 years, 2 = 35–54 years, 3 = 55+ years) (Simelane et al., 2020), educational level of the household head (0 = no education, 1 = primary, 2 = secondary, 3 = university) (Gaffan et al., 2022), household size (1 ≤ 6, 2 ≥ 6), household water availability (1 = No, 2 = Yes) (SNBS, 2022), household water treatment, (1 = No, 2 = Yes) (SNBS, 2022) and the type of residence, which was categorized as (0 = urban and 1 = rural) after merging nomadic and rural classifications (Victor et al., 2025). Additionally, we obtained a poverty status variable from the SIHBS dataset measured as binary (0 = Not poor, 1 = Poor) (SNBS, 2022).
Operational Definition
Hygiene is a long-standing notion in medical and personal/professional care practices (Ali et al., 2025). Hand hygiene is a broad phrase that encompasses cleansing hands with alcohol-based hand rub (ABHR). Basic hygiene facilities: Functional handwashing facilities (with water and soap and/or an alcohol-based hand massage) are available and accessible at the point of care and within 5 m of toilets (Berihun et al., 2022). No hygiene facilities access: No functional hand hygiene facilities are available either at the point of care or near toilets (WHO and UNICEF, 2019). It is an important part of infection prevention and control in healthcare facilities, both at sites of service and in restrooms (WHO/UNICEF, 2006). Handwashing facility: refers to a fixed or mobile device designed to contain, transport, or regulate the flow of water to facilitate handwashing. Soap: includes bar soap, liquid soap, powder detergent, and soapy water. Handwashing facilities include sinks with tap water, buckets with taps, tippy-taps, and jugs or basins designated for handwashing. Ash, soil, sand, or other traditional handwashing agents are less effective and do not count as “soap.” Availability of a handwashing facility on premises with soap and water is defined as “Improved hygiene facility or services (WHO and UNICEF, 2019). Poor hygiene practices include not having handwashing and bathing facilities or detergents in the house, as well as washing hands with water but no soap or other detergents. Good hygiene habits include using hand washing and bathing facilities, as well as keeping soap and other detergents on hand (Admasie & Debebe, 2016). A household was defined as a group of people who lived together under the same roof and ate from the same food pot, who answered to the same HoH, and were covered under the same household budget. The Head of Household (HoH) is a member of the household who holds the role of decision maker in that household. In most cases, the Head of Household takes part in the economy, control and welfare of the household (SNBS, 2022).
Data Processing and Analysis
The unit of analysis was the household. Descriptive statistics, such as frequencies and percentages, were run to describe the data using STATA 17. The Pearson Chi-square test for independence was utilized to determine the association between predictor variables and outcome variable for inclusion in model analysis, whereas a multivariable logit regression model was used to investigate whether the predictors are statistically associated with the outcome variable. The coefficients with a 95% confidence interval and a p-value of .05 were adopted to determine statistical significance. Meanwhile, the variance inflation factor (VIF) is also applied to test multicollinearity among explanatory variables. Finally, the Fairlie decomposition method was used to assess the degree to which the differences in household access to improved hygiene facilities (rural vs. urban) can be attributed to the variables included in the analysis. This technique splits regression model results into components attributed to disparities. This approach is particularly well-suited for binary outcome variables (rural vs. urban) due to its flexibility in accommodating non-linear functional forms, such as logit or probit models, and its ability to quantify the contribution of group differences in explanatory variables to differences in predicted probabilities of the outcome. The Fairlie method splits the disparities in the likelihood of improved sanitation facilities between rural and urban households into two categories: (1) explained (endowment) part by differences in observable characteristics (sex, education, age of HH, poverty status, water sources of HH, and Household water treatment) and (2) an unexplained (coefficients) part, often attributed to variations in the effects of these characteristics or unobserved factors such as preferences, access to markets, or policy environments. The explained part supports in determining which variables are the most significant contributors to the disparity between rural and urban households in terms of access to improved facilities. In contrast, an unexplained portion may be a reflection of structural disparities, discrimination, or variables that were not taken into account by the model. In the Fairlie decomposition approach, when the overall rural-urban disparity in household access to improved hygiene is negative, it indicates lower access to improved hygiene facilities in rural areas. The presence of a negative coefficient for a particular variable indicates that the factor in question is one of the contributors to the deepening of the disparity. On the other hand, a positive coefficient shows that the variable contributes to the reduction of the disparity by creating a smaller difference between rural and urban areas. For our study, we opted not to focus on the unmeasurable section of the gap because of the difficulties in understanding the data, consistent with earlier studies that have used similar decomposition methodologies.
Findings of the Study
Table 1 shows that the prevalence of hand hygiene facilities is quite low in Somalia, with only 32.5% of the population having access to improved hygiene, while the majority, 67.5% depend on unimproved.
Prevalence of Access to Improved Hygiene Facilities in Somali Households, SIHBS 2022 (n = 7,212).

Source. Own compilation from SIHBS (SNBS, 2022).
Descriptive Statistics of Socio-Economic, Demographic, and Other Variables
Table 2 demonstrates the distribution of household characteristics based on gender, age, and education level of the household head, household size, household poverty status, water availability (sources), water treatment, as well as the type of residence. This study examined 7,212 sample households, with 52.37% female and 47.63% male respondents. In terms of age of the household head, the greatest representation, 59.87% was aged 15 to 34 years, while the lowest at 18.32% aged 55+ years. Furthermore, nearly 70% (69.20%) had no education, with 19.74% of household heads having completed primary, and only 3.84% having completed university level. Households with six or fewer members accounted for 53.13%, and those with more than six members made up 46.87%. Households with poor status accounted for 51.59% and 48.41% for non-poor households. The majority of households, 80.44% had access to water sources, while only 19.56% did not. Furthermore, household water treatment was 82.11%. Approximately 60.23% of households reside in urban areas, while 39.77% live in rural areas.
Socio-Economic, Demographic, and Other Variables of the Study Population Using SIHBS 2022.

Association Between Explanatory Factors on the Type of Residence of the Study Population, SIHBS 2022
As shown in Table 3, the Pearson Chi-square test for independence (χ2) results depict the association of explanatory factors with the type of residence. The sex of the household head, educational level of the household head, household size, water treatment, availability of water, and household poverty status all have a significant association with the type of residence of the household. The disparity in access to improved hand hygiene facilities, regarding type of residence, is a concern, with only 868 (38.36%) of rural households compared to urban areas, 1,395 (61.64%). Regarding the type of residence, significant sex disparities exist among household heads. Female household heads were more prevalent in urban areas, accounting for 2,408 (63.75%) of the households, compared to 1,369 (36.25%) in rural areas. furthermore, the educational level of the household head varied greatly, with 244 (88.09%) urban household heads with university education, compared to only 33 (11.91%) in rural areas. Urban households were usually bigger, with 2,244 (66.39%) having more than 6 members, while rural households had a smaller proportion of 1,136 (33.61%). Households with non-poor status residing in urban areas were 216 (61.90%) higher than those living in rural areas with poor status, 1,330 (38.10%). Rural households had 2,061 (35.53%) water availability than urban households, 3,740 (64.47%). Finally, urban households treated water outnumbered rural households 908 (70.39%) to 382 (29.61%) respectively.
Association Between Explanatory Factors and Type of Residence of the Study Population, SIHBS 2022.

Source. Own compilation from SIHBS (SNBS, 2022).
Note. Bold entities are statistically significant variables.
The disparity in access to improved hand hygiene facilities, regarding the type of residence, is a concern. with only 868 (38.36%) of rural households accessing improved facilities compared to urban areas, 1,395 (61.64 %), while urban households accessed unimproved hand hygiene facilities at a rate of 59.59% greater than rural households with unimproved hygiene, 40.41% (Figure 1).
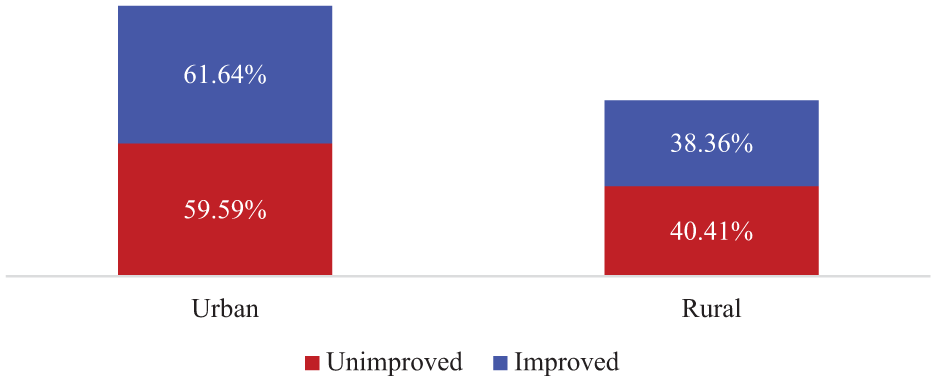
Distribution of household access to improved hygiene facilities regarding type of residence using the SIHBS 2022.
Estimation for the Multivariate Logistic Regression Model Analysis
Based on the results presented in Table 4, the multivariable binary logistic regression analysis reveals significant socioeconomic and residential disparities in access to improved hand hygiene facilities in Somalia. Sex, education level of the household head, household’s poverty status, household water treatment, as well as the type of residence, were found to be statistically significant predictors of improved hand hygiene facilities. Female-headed households (AOR: .844, 95% CI [.767, .929], p < .005) were 15.6% less likely to access improved hand hygiene facilities compared to male-headed households. Similarly, household heads with a primary education (AOR: .881, 95% CI [.777, .999], p < .005) were 11.9% more likely to have access to improved hand hygiene facilities compared to their counterparts. Regarding household water treatment (AOR: .775, 95% CI [.703, .855], p < .005), were 22.5% a significantly lower likelihood of getting improved hand hygiene facilities. In comparison, households with poor status (AOR: .636, 95% CI [.579, .699], p < .005) are roughly 36.4% less likely to obtain improved hand hygiene facilities than their counterparts. Finally, the type of residence plays a pivotal role; rural households have a significantly lower 13.9% access to improved hand hygiene facilities compared to urban households (AOR: .861, 95% CI [.779, .952], p < .005).
Estimation for Multivariate Logistic Regression Model Analysis.

Note. Bold entities are statistically significant variables.
Multicollinearity Assumption Test
Table 5 presents the VIF values and their reciprocals (1/VIF) for the variables included in the analysis. The VIF values indicate very low collinearity, with the sex of the household head (1.104), age of household head (1.047), households’ water availability (1.035), education level of the household head (1.140), Household size (1.026), Household water treatment (1.013), Household’s poverty status (1.007), type of place of residence (1.096). The corresponding 1/VIF values are .878, .906, .912, .955, .967, .974, .987, and .993, respectively. The mean VIF of 1.058 shows that multicollinearity is not a concern, as all values are substantially below the standard threshold of 5.
Variance Inflation Factor (VIF).

Non-Linear Decomposition Analysis
Table 6 presents the results of the Fairlie decomposition analysis, which explores rural-urban disparities in household access to improved hand hygiene facilities. The analysis identified the educational level of the household, poverty status, and household water treatment as the key factors contributing to these disparities. The decomposition analysis revealed that the household head’s education level was the most important explanatory factor for the observed disparity. Variations in household head education accounted for 43.8% of the overall rural-urban gap in access to improved hygiene facilities. Although the household head’s educational level appeared as the most significant predictor of this disparity, other variables also played a role, including the household’s economic condition 5.9% and the household water treatment 16%. This finding highlights the persistent rural-urban divide in access to essential hygiene infrastructure. The estimated difference in the probability of accessing improved hand hygiene facilities between rural and urban households is −.0185, indicating that rural households, on average, have a significantly lower likelihood of access compared to their urban counterparts. The findings show that socioeconomic and demographic factors influence household access to improved hygiene facilities, particularly education, poverty status, and household water treatment remains the most significant structural barrier to accessing hygiene facilities in rural areas. In contrast, the unexplained component may reflect structural inequalities, discrimination, or omitted factors not captured in the model.
Decomposition Analysis of the Disparities in Household Access to Improved Hand Hygiene Facilities Between Rural and Urban.

Source. Own compilation from SIHBS (SNBS, 2022).
Note. Bold entities are statistically significant variables.
Discussion
This study explored rural-urban disparities in access to improved hand hygiene facilities, as well as the contributing factors (endowment) of this disparity, using data from the SIHBS 2022. The study found that the sex, education level of the household head, poverty status, household water treatment, and type of residence all had a statistically significant positive association with the possibility of accessing improved hand hygiene facilities. This study found that only 32.5% of households have access to improved hand hygiene facilities. The multivariable logistic regression result reveals that female household heads were less likely to access improved hygiene than their male counterparts. This conclusion is consistent with prior studies, which found that female-headed households had a much higher odds ratio for access to basic water and sanitation services than their counterparts (Andualem et al., 2021; Gaffan et al., 2022). Some authors found, most women in Sub-Saharan Africa have higher responsibilities within households related to greater water utilization compared to their counterparts (Agbadi et al., 2019). The educational level of the household head was found to be a statistically significant predictor of the household’s access to improved sanitary facilities. Particularly, primary-educated heads were more likely to have access to improved hygiene facilities than their counterpart. This finding contradicts prior studies that revealed higher educated heads had access to improved sanitation facilities and had a vital role in reducing disparities in access to basic sanitation services (Abubakar et al., 2024; Ayele, 2025; Keleb et al., 2024; Kumar et al., 2024).
Poverty status was significantly associated with household access to improved hygiene facilities, with poor households being less likely to have access to improved hygiene than non-poor households. This finding is consistent with other studies that show households having non-poor status are more likely to have access to improved sanitation facilities compared to poorer households (A. Ahmed et al., 2023; Dongzagla & Adams, 2022; Kumar et al., 2024; Soboksa et al., 2021; Tesfaw et al., 2023). This could be because wealthy people will be able to pay for improved hygiene services. Access to improved handwashing facilities grew as household poverty levels fell. This is because increased household income creates greater choices and opportunities. As a result, households with a stable economic status may be able to afford the resources needed to improve sanitary conditions. In contrast, rural residents were less likely to have access to improved hygienic facilities than rural households. Because urban households benefit from greater economic opportunities, higher living standards, and improved infrastructure, all of which allow access to a broader variety of sanitation facilities than rural residents (Mulenga et al., 2017; Ohwo, 2019).
A Fairlie decomposition analysis identified education, household water treatment, and household poverty status as the only statistically significant predictors contributing to the overall rural-urban gap, respectively. The estimated difference in the likelihood of having improved hand hygiene facilities indicates that rural households are substantially less likely to have access compared to their urban counterparts. These findings underscore the importance of education, water treatment, and financial constraints as key structural barriers to improved hygiene access, particularly in rural communities. Meanwhile, the unexplained portion of the disparity may point to deeper structural inequities, potential discrimination, or other unmeasured variables not included in the model.
Strengths and Limitations
The study’s strengths include the use of nationally representative data, which allows for further generalization of the findings. The study employed the Fairlie decomposition approach to explain the contributing factors of rural-urban disparities in access to improved hygiene facilities. This study analyzed the poverty status variable, due to the absence of a wealth index in the SIHBS dataset, to determine the household’s economic status. Limitations of the study include: this study depends on cross-sectional data, making it difficult to determine causal correlations. Significant determinants such as culture may have an influence on the behavior of accessing improved sanitation, but they were not included in the SIHBS. Therefore, this study solely captures the selected socioeconomic and demographic variables of the households available in the SIHBS dataset.
Conclusion and Recommendations
Limited access to improved hygienic facilities in households and their significant rural-urban disparities remain a matter of concern in Somalia. Key contributing factors of this variation in accessing improved hygiene facilities include the educational level of the household head, the household’s poverty status, and the household water treatment. Based on the findings, this study recommends the following: first, the government should initiate and prioritize targeted programs like Shock Responsive Safety Net for Human Capital Project (SNHCP), also known as BAXNAANO in Somali, and provide financial support to female-headed households, particularly and those with large household sizes to reduce the disparity in household access to improved sanitation facilities, particularly in rural areas. Second, policymakers should implement effective sanitation strategies and policies with a higher focus on educating communities to raise awareness of the detrimental impacts of poor hygiene. Finally, future studies should be conducted using similar multi-survey data from different countries for comparative analysis.
The Robustness of the Model
As an alternate method, we adopted a multivariate probit model to confirm the results of the multivariate logistic regression model and determine if they are significant determinants of household access to improved hand hygiene facilities. Table 7 presents the multivariate probit model results. These findings verify that the sex of the household head, educational level of the household head, poverty status of the household, household water treatment, and type of residence of the household are key significant predictors of household access to improved hygiene facilities. Therefore, these findings are consistent with those of the multivariate logit model.
Results of the Multivariate Probit Model.
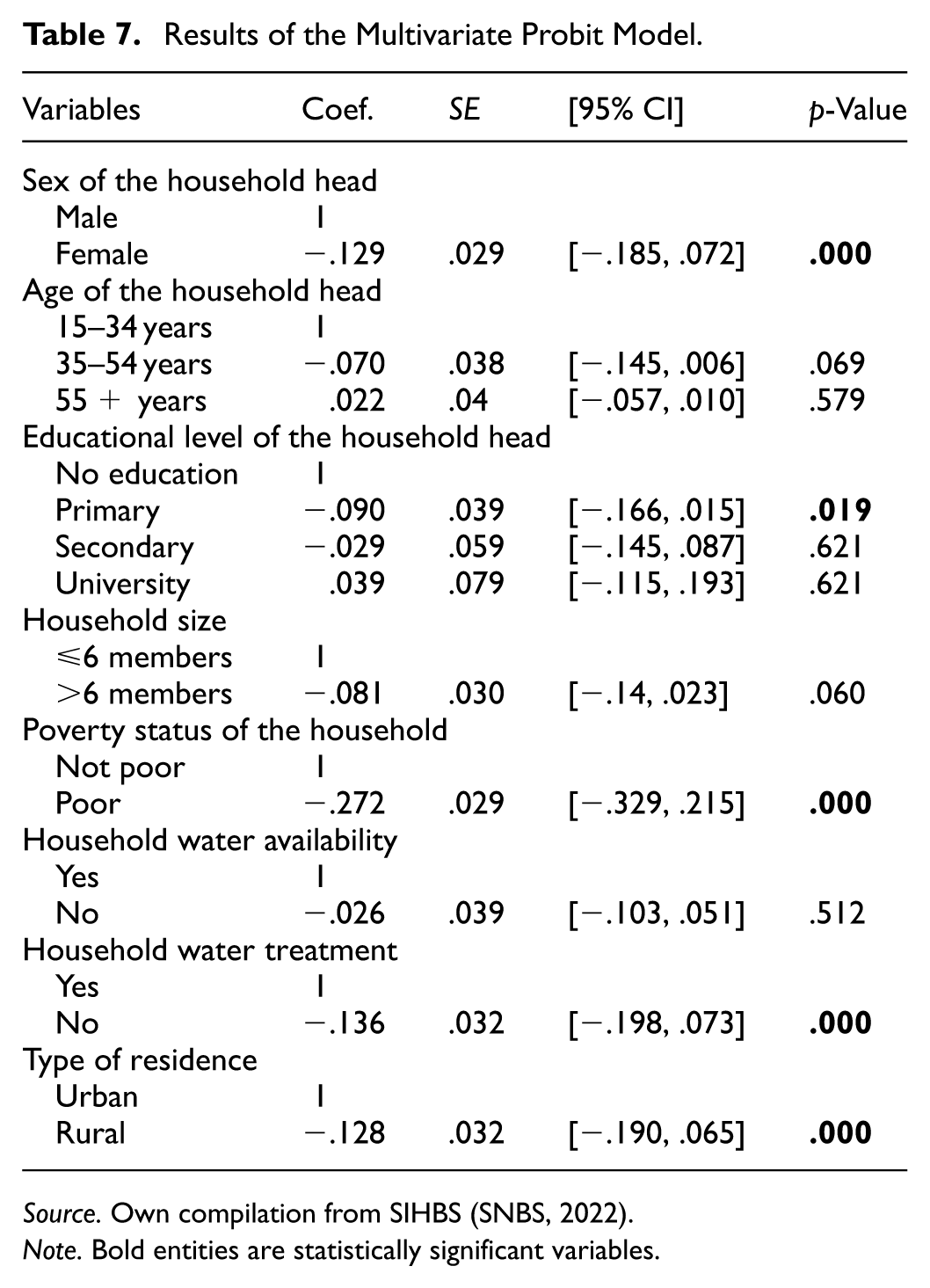
Source. Own compilation from SIHBS (SNBS, 2022).
Note. Bold entities are statistically significant variables.
Footnotes
Acknowledgements
We would like to thank the Somalia National Bureau of Statistics for enabling us to access to their microdata portable so that we may download the SIHBS 2022 Dataset for our research study.
Ethical Considerations
Ethical clearance was obtained from the Jamhuriya University Research Ethics Committee (certificate number JUREC0107/CGS321/052024). The committee confirms that the research complies with the ethical standards and guidelines established by Jamhuriya University of Science and Technology, as well as applicable national and international regulations. So, there were no risks associated with participation, and the collected data were utilized only for this study purpose, with complete anonymity.
Informed Consent to Participate
Written consent was obtained from the household heads in order to gather the data in a manner that was in conformity with the relevant rules and standards.
Author’s Contribution
Hassan Abdi Ahmed was responsible for writing idealization, introducing the manuscript, literature review, methodology, data extraction, manipulation, descriptive analysis, interpretation, model design and analysis full draft preparation. Dahir Abdi Ali performed Chi-square test, multivariate logit analysis interpretation, and review of the manuscript. All author’s read final draft and approved. Nelson Jerry Ndifwa, did Fairlie decomposition analysis, interpretation of findings and the critical review of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.