
Abstract
This study examines the sociodemographic and personal factors influencing e-cigarette use. In this study, the microdata set was obtained from the Türkiye Health Survey conducted by the Turkish Statistical Institute in 2019. Gompit regression analysis was employed to identify the factors associated with individual e-cigarette use. The study included data from 17,084 participants aged 15 or older. Findings indicate that 68.9% of e-cigarette users in Türkiye are male, and 60.8% are married. Among e-cigarette users, 62.8% also use tobacco, while 37.2% consume alcohol in addition to e-cigarettes. The results suggest that females are less likely to use e-cigarettes compared to males, but married individuals are more likely to use e-cigarettes than single individuals. Furthermore, the probability of e-cigarette use decreases with age but increases with higher levels of education. Individuals exposed to tobacco smoke, as well as those who consume both alcohol and tobacco, have a higher likelihood of using e-cigarettes. E-cigarette use poses significant societal challenges, including increased rates of disease, mortality, and workforce losses. Identifying the factors associated with e-cigarette consumption can highlight critical areas of concern, guiding efforts to reduce its use and supporting the development of effective control policies. This study underscores the importance of targeting specific groups for intervention, particularly young people, men, individuals exposed to tobacco smoke, alcohol users, individuals seeing a psychiatrist, those whose treatment is not covered by the Social Security Institution (SSI), and tobacco users. Addressing these groups can contribute significantly to reducing the prevalence and harmful effects of e-cigarette use.
Introduction
Smoking is responsible for millions of deaths worldwide and remains one of the leading causes of disability and premature mortality (Alkan et al., 2023). Despite its well-documented adverse effects, smoking is a notoriously difficult addiction to overcome (Alkan & Demir, 2019). In response to smoke-free laws and steadily increasing tobacco prices, many consumers have sought alternatives to traditional cigarettes (Schober et al., 2014). Electronic cigarettes (e-cigarettes) have emerged as popular substitutes, marketed as devices that enable users to smoke anywhere. These products are often promoted as potentially helpful tools for quitting smoking or reducing cigarette consumption. Through television, internet, and print advertisements, e-cigarettes are frequently advertised as a healthier alternative to traditional tobacco products (Felberbaum, 2013; Grana & Ling, 2014).
E-cigarettes were first introduced as “smokeless cigarettes” by Herbert A. Gilbert in 1963 (Gorukanti et al., 2017). Later, in 2003, electronic nicotine delivery systems (ENDS) were developed in China as devices designed for broad consumer use, and they have since gained global popularity, primarily through online platforms (Adkison et al., 2013). The e-cigarette market, described as fragmented and rapidly growing, now includes hundreds of brands (Dawkins et al., 2013).
E-cigarettes, which typically use a battery-powered heating element to produce an aerosol from a nicotine-containing solvent (e-liquid), are becoming increasingly popular (Vardavas et al., 2015). They are marketed as tools that can help smokers quit or reduce smoking by mimicking smoking-related rituals, such as hand-to-mouth movements and nicotine delivery (Polosa et al., 2011). However, there is limited information on their safety for dual users—those who use both traditional cigarettes and e-cigarettes—for exclusive e-cigarette users. Despite this, e-cigarettes have gained a significant market share as tobacco use has been increasingly restricted in public places worldwide (Schober et al., 2014). Many smokers turn to e-cigarettes to support their smoking cessation efforts. The rapid rise in e-cigarette sales has even led some analysts to predict that they may soon surpass traditional cigarettes sales (Purkayastha, 2013).
The literature contains various studies on e-cigarette use (Chen-Sankey et al., 2024; Swiatkowska et al., 2024; Ünver, 2024). Many of these studies have explored the relationship between e-cigarette use and perceived risks associated with their use (Manzione et al., 2020).
The three most commonly cited reasons for using e-cigarettes in prior research include aiding smoking cessation, reducing exposure to tobacco smoke, and their perceived appeal (Biener & Hargraves, 2015). One study reported that approximately 27% of e-cigarette users cited enjoying e-cigarette flavors as their primary reason for use, followed by protecting their families from secondhand smoke (23%) and reducing or quitting smoking (21%). These findings suggest that many users may view e-cigarettes as alternatives to traditional smoking rather than as tools for complete cessation (Alhajj et al., 2022).
Other studies have identified additional motivations for e-cigarette use, such as their status as a popular trend (Martínez et al., 2019; Puteh et al., 2018) and their use by friends and family members (Lotrean, 2015; Martínez et al., 2019). The growing popularity of e-cigarettes as a trend can be attributed to the influence of extensive marketing campaigns, particularly on the internet. In contrast, the role-modelling effect of friends and family highlights the social influences driving e-cigarette use (Alhajj et al., 2022).
A study conducted in the USA reported an e-cigarette usage prevalence of 11.5% among individuals aged 18 to 24 years (Nagel et al., 2022). This high prevalence aligns with earlier findings, highlighting the rapidly growing popularity of e-cigarette use among young adults (Saddleson et al., 2015; Tanriover et al., 2022). The e-cigarette industry’s marketing strategies often target adolescents and young adults (Ünver, 2024).
In contrast, a study involving university students from Belarus, Lithuania, Poland, Russia, and Slovakia found that only 1.1% of participants reported using e-cigarettes (Brozek et al., 2019). Similarly, in China, the prevalence rates among vocational high school students were reported at 2.1% and 3.6%, respectively (Wang et al., 2016). Among university students, e-cigarette usage rates were 0.6% in Hungary (Pénzes et al., 2016), 2.7% in Romania (Lotrean, 2015), and 13.3% in France (Rakotozandry et al., 2016).
In the United States, e-cigarette use among high school students rose significantly from 1.5% in 2011 to 19.6% in 2020 (Çetinkay et al., 2022). By 2016, e-cigarettes had become the most popular tobacco product among middle and high school students in the United States (Tsai et al., 2018).
Although e-cigarette use among young people has undeniably increased, an ongoing debate persists regarding the extent of harm it may cause (Kong et al., 2015). Concerns have been raised that e-cigarettes could serve as a gateway to tobacco products, potentially encouraging nicotine addiction or dual tobacco use (Riker et al., 2012). Given that most tobacco use begins during adolescence and young adulthood, it is crucial not to underestimate the potential harm of e-cigarettes to this vulnerable demographic (Cullen et al., 2019).
In addition to their negative impact on younger generations, passive remains a global health concern, despite the implementation of comprehensive smoke-free regulations in many countries (Öberg et al., 2011). Moreover, e-cigarettes are not emissions-free and may adversely affect indoor air quality (Schober et al., 2014).
E-cigarettes are marketed as offering a potentially reduced exposure to the harms of smoking. While these products resemble traditional cigarettes in design or function, they are not cigarettes and are often promoted as being “safer” alternatives (Goniewicz, Knysak, et al., 2014). However, the scientific evidence supporting claims that e-cigarettes have no adverse effects remains inconclusive and subject to debate.
E-cigarettes are believed to avoid emitting the toxins typically found in traditional cigarette smoke, as they do not contain or burn tobacco (Cobb & Abrams, 2011). Nevertheless, some public health experts express concern that the use ENDS could undermine laws promoting smoke-free indoor environments and perpetuate the use of nicotine and tobacco-containing products among smokers who might otherwise consider quitting (Regan et al., 2013).
Given the diverse range of diseases associated with e-cigarettes in the literature, it is notable that cases in Wisconsin and Illinois presented similar clinical findings, disease progression, and suggested a comparable pathophysiological mechanism of lung injury (Layden et al., 2020).
Relatively few side effects have been reported in connection with e-cigarette use. Mouth irritation was the most frequently reported, followed by throat irritation. Among those who experienced side effects, fewer than 16% reported any meaningful impact, and less than 3% reported severe side effects. Furthermore, there was no significant difference in reporting side effects between individuals who had quit smoking and those who continued to smoke (Dawkins et al., 2013).
Some studies indicate that smokers perceive e-cigarettes as tools for smoking cessation (Etter, 2010). These products have been reported to reduce the urge to smoke after quitting (Bullen et al., 2010), help prevent relapse among former smokers, and potentially lower overall cigarette consumption (Etter & Bullen, 2014; Polosa et al., 2011; Siegel et al., 2011).
While e-cigarettes may help conventional smokers reduce harm, they also pose the risk of increasing nicotine addiction among new users (Primack et al., 2015). Results indicate that nicotine intake from e-cigarettes can be 1.5 times greater than that from traditional cigarettes (Flouris et al., 2013). Empirical studies suggest that completely switching from tobacco cigarettes to e-cigarettes could lower the risk of illness and that using e-cigarettes may be less harmful than smoking (Shahab et al., 2017). However, despite the potential advantages, definitive conclusions about their overall impact on human health remain elusive due to limited data (Callahan-Lyon, 2014).
In recent years, several countries, including Türkiye, have imposed various bans and restrictions on the use and sale of e-cigarettes. In Türkiye, e-cigarettes, which were introduced for sale in 2007 to 2008, were later subjected to regulations and restrictions imposed by the Ministry of Health. Restrictions were imposed on the advertising, official sale, and marketing of e-cigarette products, with an official declaration stating that they were not classified as medical products (Börekçi et al., 2015). In 2013, e-cigarettes were brought under the scope of Law No. 4207 on Preventing the Harms of Tobacco Products and their Control. This legislation made it illegal to advertise e-cigarettes, use them indoors, or sell them to individuals under the age of 18. The ban was justified by the “high risk of nicotine intake at a high dose, addiction potential, and the hindrance to smoking cessation efforts” (ResmiGazete, 1996).
Furthermore, Presidential Decree No. 2149 prohibited the import of all products—whether they contain tobacco or not—intended for the consumption of tobacco-like products. This includes e-cigarettes, electronic hookahs, as well as electronic devices, their components, and solutions, due to their potential to imitate tobacco products (ResmiGazete, 2020).
When addressing e-cigarette use, it is crucial to understand the factors contributing to its prevalence. This study adopts the Theory of Planned Behavior (TPB) as its framework (Ajzen, 1991). According to TPB, behavior is determined by the intention to perform it, which in turn is influenced by three constructs: attitudes (perceived advantages and disadvantages of the behavior), subjective norms (social influences on the behavior), and perceived behavioral control (facilitators and barriers to the behavior) (Doherty et al., 2022).
TPB has been widely applied to identify factors influencing behavioral intentions, explain cognitive processes related to smoking, and examine cessation behaviors (Hukkelberg et al., 2014; Su et al., 2015). More recently, TPB has been used to investigate factors driving e-cigarette use among adolescents and young adults (Scheinfeld et al., 2019; Simpson et al., 2022; Trumbo, 2015). For instance, using a shortened version of the theory, Trumbo and Kim found that positive responses to advertisements and beliefs about lower addiction potential were predictors of students’ intentions to use e-cigarettes (Trumbo, 2015). Another recent study focused on undergraduate students and employed TPB to examine e-cigarette use, identifying attitudes and norms as key factors associated with usage. The findings suggested that challenging positive attitudes and social norms could reduce e-cigarette use among students (Scheinfeld et al., 2019).
This study explores e-cigarette use among individuals living in Türkiye by addressing the following research questions:
The remainder of this paper is organized as follows: Section “Methods” discusses the data, variables, and analytical methods used in the study. Section “Results” presents the results in detail. “Discussion” discusses the findings in the context of the existing literature. Finally, “Conclusion” offers macroeconomic policy recommendations to raise awareness of the adverse health effects of e-cigarette use.
Methods
Data
This study utilized data from the Türkiye Health Survey, which the Turkish Statistical Institute conducted in 2019. The purpose of the study is to gather data on health indicators, which are critical components of development indicators, reflecting the level of a country’s development. Within the context of the Türkiye Health Survey, this study aims to bridge existing knowledge gaps in the current health landscape.
The Türkiye Health Survey aims to assess the overall health profiles of individuals and collect data on health indicators, which are critical measures of a nation’s level of development. This study not only identifies national health needs but also facilitates cross-national comparisons. The sampling framework for this study is based on the “National Address Database (UAVT)” which underpins the “Address-Based Population Registration System (ADNKS),” established in 2007. The survey covers all settlements within the borders of the Republic of Türkiye.
The data was collected using a stratified two-stage cluster sampling method. In the first stage, blocks (clusters) with an average of 100 household addresses were randomly selected proportionally to their size. In the second stage, household addresses were randomly chosen from each selected cluster. This sampling approach was designed to provide a representative estimate for Türkiye (TurkStat, 2020).
For this investigation, data from 17,084 individuals aged 15 and older, included in the Türkiye Health Survey, was analyzed.
Measures and Variables
In the Türkiye Health Survey, participants were asked, “Do you currently use electronic cigarettes or similar electronic products? (yes, no)” to determine their current e-cigarette usage during the survey. The response to this question was used to generate the dependent variable for the study. Individuals who reported using e-cigarettes were coded as 1, while those who did not were coded as 0.
The independent variables in the study are the variables available in the Türkiye Health Survey and emerge from the literature review. Factors related to the sociodemographic and personal characteristics of the participants include gender, marital status, age, educational level, occupation, reimbursement of treatment expenses by the Social Security Institution, receiving psychological support, tobacco use status, exposure to tobacco smoke, and alcohol use status.
Many studies reported that e-cigarette use is associated with various factors (Laverty et al., 2018; Nagel et al., 2022; Tanriover et al., 2022; Ünver, 2024). Previous studies consistently identified gender differences as a significant factor influencing e-cigarette use (Alhajj et al., 2022; Laverty et al., 2018). Similarly, age was determined in earlier studies as a factor associated with individuals’ e-cigarette use (Brozek et al., 2019; Wills et al., 2015).
In previous studies, education level was a significant determinant of e-cigarette use (Cullen et al., 2019; Kong et al., 2015; Ünver, 2024). Moreover, a previous study reported that the coverage of treatment expenses by social security (SSI), receiving psychological support, and exposure to tobacco smoke are factors associated with e-cigarette use (Ünver, 2024). Given the results reported before, tobacco and alcohol use are also factors associated with e-cigarette consumption (Primack et al., 2015; Ünver, 2024). Additionally, professional occupation was shown to be an important determinant of e-cigarette use (Pénzes et al., 2016; Rakotozandry et al., 2016).
Ordinal and nominal variables were defined as dummy variables to observe the effects of the categories of all variables to be taken into the gompit regression model (Alkan & Abar, 2020).
This study’s independent and dependent variable are linked according to the research model presented in Figure 1. The variables in the research model are hypothesized as follows:
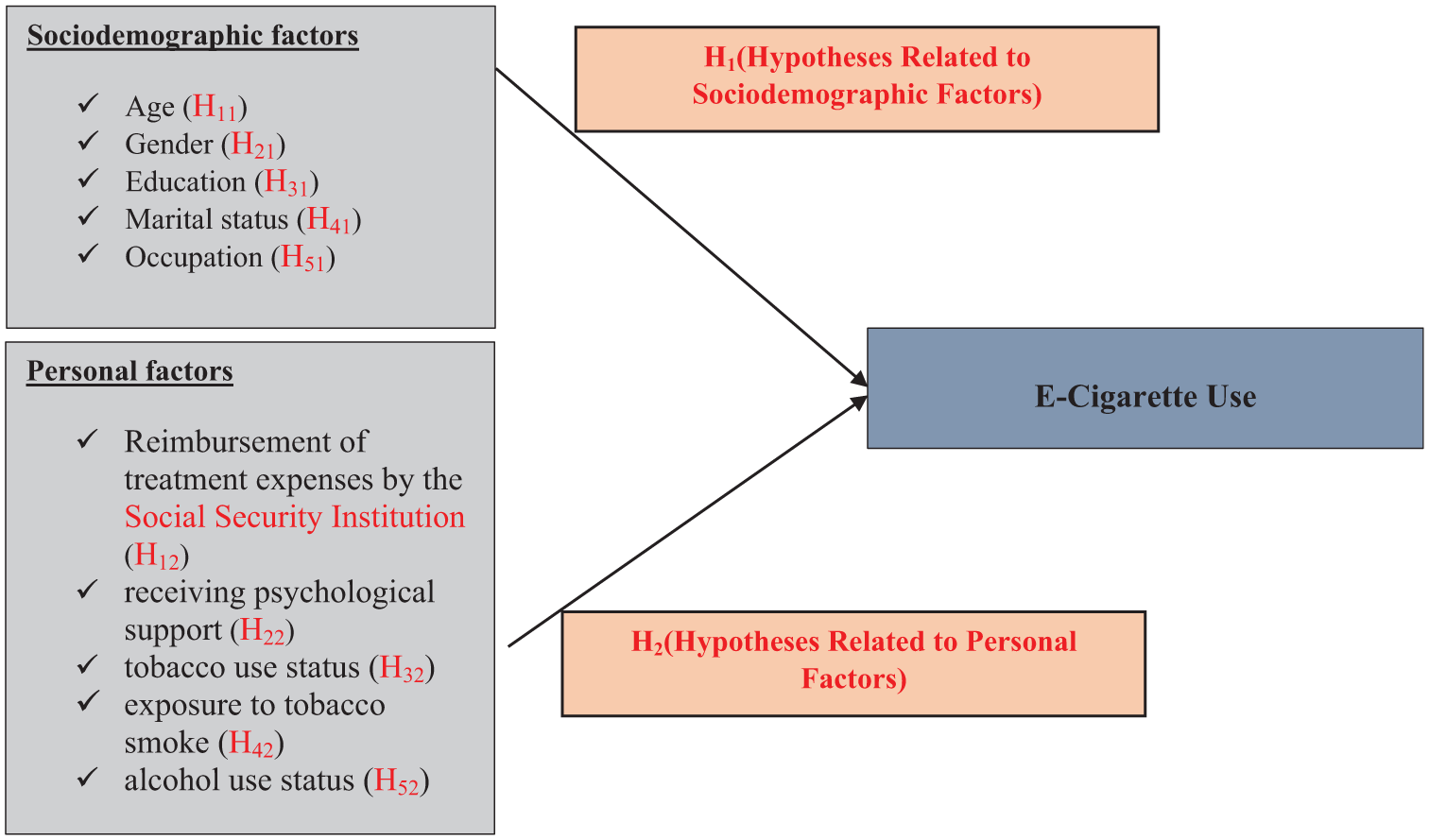
Research Model.
Hypotheses Related to Sociodemographic Factors
Differences in e-cigarette use among demographic groups constitute an interesting area of research because demographic characteristics influence individuals’ actions before engaging in a specific behavior (Ünver & Alkan, 2021, 2022). Thus, the following hypotheses are offered:
Hypotheses Related to Personal Factors
According to the Theory of Planned Behavior (TPB), personal factors are among the most significant determinants influencing individuals’ behavioral intentions and actual behaviors (Ajzen, 1991; Unver, Aydemir, et al., 2023).
Thus, the following are offered:
Research Method
Firstly, frequencies and percentages were calculated to describe the participants’ e-cigarette use status. The association between independent variables and e-cigarette use was investigated using a chi-squared independence test. Subsequently, factors associated with individuals’ e-cigarette use status were determined through a Gompit regression analysis. Gompit regression studies have become more prevalent in the literature in recent years (Güney et al., 2023; Karaaslan & Karaaslan, 2022; Laila et al., 2021). Binary qualitative choice models are regression models in which the dependent variable is discrete with binary values. In other words, in these models, the dependent variable is a binary dummy variable, representing either the probability of an event occurring or the likelihood of choosing one of two options. The Logit and Probit models are the most commonly used binary qualitative choice models. These models use different functional forms to model probabilities based on independent variables. While the Logit model is based on the Logistic Distribution, the Probit model is based on the Standard Normal Distribution. Both distributions are symmetric around zero.
In some cases, one of the two binary states in the dependent variable occurs at a much higher frequency than the other. Zeros or ones in the dependent variable are disproportionately more frequent. In such cases, using an asymmetric distribution instead of symmetric ones becomes more appropriate. The Gompit model can be an alternative to the Logit and Probit models in these scenarios. The Gompit model is based on the Gompertz Distribution, an asymmetric distribution around zero that is more effective than symmetric distributions in capturing extreme values. The Gompit model is defined using the cumulative distribution function of the Gompertz Distribution as follows:

The parameters of this model are estimated using the Maximum Likelihood Estimation method (Cameron & Trivedi, 2005; Güriş et al., 2011).
Results
Descriptive Statistics
It was determined that, in Türkiye, 68.9% of e-cigarette users are male, and 60.8% are married. The results achieved here indicate that 62.8% of e-cigarette users also use tobacco (dual users), and 37.2% of e-cigarette users also consume alcohol. The results related to factors associated with e-cigarette use in Türkiye are presented in Table 1.
Findings on the Variables Associated with e-Cigarette Consumption.

According to Table 1’s Chi-Square independence test findings, there is statistically significant evidence linking e-cigarette use to sociodemographic and personal factors.
Model Estimation
Table 2 lists the estimated outcomes of the Gompit regression. The independent variables in the Gompit regression model were examined for multicollinearity in the current study. At least five variance inflation factor (VIF) values indicate moderate multicollinearity. Values of 10 or more, on the other hand, suggest a significant degree of multicollinearity (Baskan & Alkan, 2023; Unver, Aydemir, et al., 2023). In this study, no variable causes multicollinearity among the variables.
Estimated Gompit Model Results for Variables Associated with e-Cigarette Use.

When Table 2 is examined, it can be observed that the factors of gender, age (45-54, 55-64), educational status (high school, university), occupation (skilled agriculture/forestry/fishery workers), coverage of treatment expenses by the Social Security Institution (SSI), receiving psychological support, tobacco use, exposure to tobacco smoke, and alcohol use are statistically significant. Table 3 displays the marginal effects of the variables impacting e-cigarette use.
Marginal Effects for Factors Associated with e-Cigarette Use.

The likelihood of women using e-cigarettes is 69.3% lower than men’s, per the Gompit regression model shown in Table 3. These results are consistent with previously observed gender differences in smoking and e-cigarette use in Europe (Laverty et al., 2018; Vardavas et al., 2015). Compared to those aged 15 to 24, people are 128% and 193.6% less likely to use e-cigarettes in the 45 to 54 and 55 to 64 age groups. Previous studies also reported that e-cigarette use is particularly prevalent among adolescents and young adults. Moreover, the proportion of young individuals experimenting with e-cigarettes has doubled over the past 5 years (Filippidis, Laverty, Fernandez, et al., 2017; Filippidis, Laverty, Gerovasili, et al., 2017; Laverty et al., 2018).
Compared to non-users, tobacco users are 93.6% more likely to use e-cigarettes. Contrarily, those exposed to tobacco smoke are 71.7% more likely than others to use e-cigarettes. As shown, compared to non-drinkers, people who use alcohol have a 67.4% higher likelihood of using e-cigarettes. As stated in a previous study, individuals who consume alcohol are 0.9% more likely to use e-cigarettes in comparison to non-drinkers (Ünver, 2024). Furthermore, in another study, 11.10% of tobacco users reported starting to use e-cigarettes because they perceived them to have fewer side effects than traditional cigarettes (Göney et al., 2019).
Compared to the others, those who receive psychological help are 63.8% more likely to use e-cigarettes. A previous study carried out in Türkiye revealed that individuals who visited a psychiatrist in the past 12 months were 0.5% more likely to use e-cigarettes in comparison to those who did not (Ünver, 2024).
Compared to those who have never attended school, people with a high school or university degree are 85.2% and 105.7% more likely to use e-cigarettes, respectively. Another study on high school students aged 15 to 18 in three cities in the Russian Federation reported that 2.2% of students used e-cigarettes. In contrast, the present study revealed that Russia’s overall e-cigarette usage rate was 4% (Kong et al., 2017). Compared to the unemployed, qualified agriculture, forestry, and aquaculture workers are 131.3% less likely to use e-cigarettes. Compared to the general population, persons whose medical expenses are paid for by SSI are 66% less likely to use e-cigarettes. It was found in another study that individuals whose medical expenses were covered by social security were 0.4% less likely to use e-cigarettes compared to those without coverage (Ünver, 2024).
Discussion
This study explored the variables associated with individuals’ e-cigarette use in Türkiye using Gompit regression analysis. The findings indicate that gender, age, educational status, occupation, Social Security Institution (SSI) coverage of treatment expenses, psychological support, tobacco use, exposure to tobacco smoke, and alcohol consumption were all associated with e-cigarette use.
Gender
The analysis revealed that gender plays a significant role in e-cigarette use. Consistent with previous studies, this study found that women are less likely to use e-cigarettes compared to men (Alhajj et al., 2022; Ali et al., 2021; Laverty et al., 2018).
Age
Age is another critical factor. The results demonstrated that advancing age decreases the likelihood of e-cigarette use. Prior research has shown that regular cigarette and e-cigarette use is most prevalent among the youngest age groups, particularly those aged 15-19 years (Filippidis, Laverty, Gerovasili, et al., 2017; Goniewicz, Gawron, et al., 2014). Another study focusing on young people identified psychosocial risk factors, parental support, smoking expectations, peer influence, and thrill-seeking behavior as contributing factors to e-cigarette, cigarette, alcohol, and marijuana use (Wills et al., 2015).
Educational Status
Educational attainment was found associated with e-cigarette use significantly. Higher levels of education were associated with an increased likelihood of e-cigarette use. A previous study revealed that college students are more likely than high school students to use e-cigarettes (Kong et al., 2015), while another study found that high school students use e-cigarettes more frequently than middle school students (Cullen et al., 2019). Additionally, research conducted among U.S. teenagers and young adults indicated a correlation between parental education levels and e-cigarette use (Primack et al., 2015).
Social Security Institution (SSI) Coverage
SSI coverage of treatment expenses was another variable linked to e-cigarette use. Individuals whose treatment expenses were covered by the SSI were less likely to use e-cigarettes compared to those without such coverage. A Turkish study similarly reported that people whose medical expenses were paid for by the SSI were less likely to smoke (Alkan, 2017). This highlights the importance of preventive healthcare services, which are critical in combating health issues, reducing healthcare costs, and mitigating workforce losses (Alkan & Abar, 2020).
Psychiatric Support
The study found that seeking psychiatric care within the last 12 months was associated with e-cigarette use. Individuals who had consulted a psychiatrist during this period were more likely to use e-cigarettes than those who had not.
Exposure to Tobacco Smoke
Exposure to tobacco smoke emerged as a significant factor associated with e-cigarette use. As a primary public health concern, tobacco smoke exposure has been extensively studied through various methodologies (Do et al., 2021; Groner et al., 2015; Ulbricht et al., 2015). This study corroborates previous findings, showing that individuals exposed to tobacco smoke are more likely to use e-cigarettes than those who are not (Mbulo et al., 2021; Unver, Tekmanli, et al., 2023).
Alcohol and Tobacco Use
Finally, alcohol and tobacco use were strongly linked to e-cigarette use. The findings indicated that individuals who consume these substances are more likely to use e-cigarettes compared to non-users. Moreover, a study conducted among U.S. teenagers and young adults reported a connection between parental tobacco consumption and e-cigarette use (Primack et al., 2015).
Conclusion
This study aims to determine the sociodemographic and personal factors associated with e-cigarette use by analyzing data obtained from 17,084 individuals aged 15 and older who participated in the Türkiye Health Survey.
The results indicate that women are less likely to use e-cigarettes than men. Individuals aged 45 to 54 and 55 to 64 are less likely to use e-cigarettes than those aged 15 to 24. High school and university graduates are more likely to use e-cigarettes than those with no formal education. Individuals employed in skilled agriculture, forestry, or fisheries are less likely to use e-cigarettes than those unemployed. Those whose medical expenses are covered by social security are less likely to use e-cigarettes than others.
Individuals receiving psychological support, tobacco users, and those exposed to tobacco smoke are more likely to use e-cigarettes. Similarly, alcohol consumers are more likely to use e-cigarettes than non-consumers.
The usage of e-cigarettes is a significant global health issue. The development and rigorous implementation of e-cigarette control policies can reduce e-cigarette use. Identifying factors that affect e-cigarette use can help guide the implementation of e-cigarette control policies by highlighting the areas of concern for reducing e-cigarette use. This study particularly emphasizes the need to address young individuals, males, those exposed to tobacco smoke, alcohol users, individuals seeking psychiatric help, those not covered by social security, and tobacco users.
E-cigarette use poses a significant public health concern. The increasing prevalence of e-cigarette advertisements and online sales contributed to its widespread use. Consequently, public health measures must be implemented to address this issue. Due to the substances they contain, e-cigarettes threaten public health. Furthermore, identifying effective marketing techniques and channels that alter young people’s perceptions of harm and influence their progression toward e-cigarette use is critical for designing effective prevention campaigns aiming to reduce e-cigarette use among youth. It is well-known that e-cigarette use harms society, including disease, death, loss of workforce, and more. Combating e-cigarettes should become a component of the broader tobacco control efforts. Society must be educated about the harms of e-cigarettes, and political authorities should raise awareness and take necessary precautions. To increase awareness of the harmful effects of using e-cigarettes, appropriate strategies should be developed to reduce e-cigarette consumption by paying attention to the determinants that affect e-cigarette use and considering public health strategies. Moreover, the study’s findings can inform the creation of programs and regulations to reduce the adverse effects of e-cigarette use.
Limitations of the Study
This study has several limitations. First of all, secondary data were employed in this investigation. The dataset’s variables make up the variables needed for statistical analysis. Second, because the data are cross-sectional, it cannot draw firm conclusions about the causal links between socioeconomic characteristics and e-cigarette use (Erdogan et al., 2022; Tutar et al., 2024). A cross-sectional study is a study design used to collect information and analyze data at a specific point in time. Such studies gather data from various groups of individuals or subjects representing different populations, age groups, or other relevant categories. However, cross-sectional studies cannot establish causal relationships between variables. Since the data is collected at a single time point, it is difficult to determine the temporal order of events or whether one variable directly influences another. Finally, this study’s findings were gathered based on respondents’ responses. As a result, the data gathered using this form of data collection could be biased.
Footnotes
Acknowledgements
The authors would like to thank the Turkish Statistical Institute for its data. The views and opinions expressed in this manuscript are those of the authors only and do not necessarily represent the views, official policy, or position of the Turkish Statistical Institute.
Authors’ Note
Additionally, the authors had full access to all the data in the study and took responsibility for the integrity of the data and accuracy of the data analysis.
Ethical Considerations
We declare that all ethical guidelines for authors have been followed by all authors. Ethical approval is not required.
TurkStat is an institution that compiles, evaluates, and presents statistical information to decision-makers to prepare development plans and programs, make economic decisions, and address all other issues needed. TurkStat carries out internationally comparable statistical production activities according to the standards of organizations such as the European Union Statistical Office, the United Nations, OECD, ILO, etc. TurkStat collects data within the scope of the Official Statistics Program. The Official Statistics Program is prepared for 5-year periods based on the Turkish Statistics Law No. 5429 to determine the basic principles and standards regarding the production and publication of official statistics and to ensure the production of up-to-date, reliable, timely, transparent and impartial data in areas of need at national and international levels. The individuals included in the sample in the surveys conducted by the Turkish Statistical Institute are legally obliged to participate in the survey. According to the Turkish Statistics Law, those who do not provide the information requested within the scope of the research in the specified form and time without a valid excuse or who provide incomplete or incorrect information are warned once and asked to provide the information or correct the deficiencies and errors within 7 days. An administrative fine shall be imposed on natural persons or organs and representatives of private legal entities who, despite this warning, do not provide the information or correct the deficiencies and errors as requested. TurkStat also conducts the Türkiye Health Survey within the scope of the Official Statistics Program put into effect by law. Since the Türkiye Health Survey is conducted within the scope of legal responsibility by the state, ethical approval is not required.
The data were obtained through the joint teamwork of both the Turkish Statistical Institute (TurkStat) and the European Union Statistical Office (SOEU). We obtained this data from TurkStat in return for a contract without needing an ethics committee document and used it in our study.
For this study, secondary data were employed. Official approval was received from the Turkish Statistical Institute to use the microdata set from the Türkiye Health Survey. The Türkiye Health Survey provides many indicators in the field of health, including the utilization of health services by individuals aged 15 and over, the degree of difficulty they experience in performing their daily activities, and their smoking and alcohol use habits. The Turkish Statistical Institute also received a “Letter of Undertaking” authorizing it to use the study’s data.
The letter of undertaking for the use of micro data without restrictions in dissemination:
Article 1- This letter of undertaking determines the rules, principles and obligations of the use of micro data, which are safe to disclose apart from the Presidency.
Article 2-This letter of undertaking regulates the use of micro data sets of Türkiye Health Survey in 2019, within the framework of the Directive on Access and Use of Micro Data in line with the purpose specified in Article 1.
Article 3- The following provisions apply for the use of micro data:
a) Findings obtained by the researcher as a result of incorrect calculation only bind the researcher.
b) The researcher refers to the micro data of the Institution that he uses while disclosing the results obtained from the study.
c) The researcher is obliged to send a copy of the published report, article, publication etc. to the Institution Library within 3 months at the latest. Subsequent micro data usage requests of the researcher who is found not to fulfill this obligation are not covered.
d) The researcher cannot reproduce, give to third parties, sell or transfer the micro data set he obtained.
Article 4-The researcher, by taking into account the principles of confidentiality defined in 13. and 14. articles of Turkish Statistical Institution numbered 5429 and Regulation on Procedures and Principles Regarding Data Confidentiality and Confidential Data Security in Official Statistics, is deemed to guarantee hereby that he shall not disclose the information, table, etc. violating this principle and shall only use micro data for statistical purposes.
Consent to Participate
In compliance with the national legislation and the institutional standards, written informed permission from the patients/participants or patients/participants’ legal guardian/next of kin was not necessary.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this study is subject to third-party restrictions by the Turkish Statistical Institute. Data are available from the Turkish Statistical Institute (