
Abstract
Intimate partner violence (IPV) is common and is associated with deleterious mental health outcomes. Less research has focused on the impact of lifetime IPV exposure on pregnancy-related outcomes and postpartum mental health symptoms, especially anxiety symptoms. As such, the current study examined the impact of lifetime IPV exposure on birthing experiences and postpartum anxiety symptoms. Participants were a sample of 1,912 females enrolled in a multi-site randomized control trial (i.e., “Mamma Mia”) of an internet and mobile-based intervention for preventing and reducing perinatal mental health symptoms. Although IPV history did not predict subsequent birth experience, findings demonstrated significant main effects of IPV history on both anxiety and depressive symptoms, and differences regarding main effects between intervention groups. A strengths-based approach, with a focus on posttraumatic growth, may improve postpartum mental health symptoms in trauma-exposed females specifically.
Keywords
Introduction
Intimate partner violence (IPV) includes physical violence, sexual violence, stalking, and/or psychological abuse by a current or former partner or spouse (Breiding et al., 2014). The World Health Organization declared IPV a major public health issue in 1996, and it remains one of the most prevalent forms of violence against women with lifetime estimates reaching upwards of ∼45% (Thompson et al., 2006). IPV is associated with a range of deleterious mental health consequences such as alcohol dependence, generalized anxiety disorder, and posttraumatic stress disorder (Bryngeirsdottir et al., 2022; Okuda et al., 2011). While IPV is a notable public health burden, both in frequency of exposure and severity of co-morbid mental health concerns, broadly speaking, less research has focused on the harmful effects of IPV exposure on pregnancy-related outcomes and post-partum mental health symptoms specifically. This is a key population of interest regarding IPV exposure given that the adverse health effects of IPV are amplified in pregnancy (Chisholm et al., 2017).
Stress-response models provide a useful framework for understanding how exposure to interpersonal violence (IPV) can negatively affect pregnancy and postpartum outcomes. These models suggest that chronic or severe stress—such as that resulting from IPV—can dysregulate the hypothalamic-pituitary-adrenal (HPA) axis, leading to heightened physiological arousal, altered cortisol patterns, and inflammation, all of which have been linked to adverse perinatal outcomes (Yim et al., 2015). Prolonged activation of the body’s stress-response system in the context of IPV may contribute to increased risk for complications such as preterm birth, low birth weight, and postpartum mood and anxiety disorders (Agarwal et al., 2023). Moreover, IPV-related trauma may sensitize individuals to future stressors, amplifying emotional and psychological responses during the perinatal period (Lancaster et al., 2010). This conceptualization supports the need for early identification of IPV and integration of trauma-informed care into prenatal and postpartum services to mitigate the physiological and psychological toll of chronic stress during this critical time.
Although it is well-established that experiencing IPV during pregnancy has an adverse impact on birth outcomes and mental health sequelae, there is a dearth of literature examining the longitudinal effects of pre-pregnancy IPV on birth outcomes and subsequent postpartum mental health symptoms. One potential way in which IPV history may impact postpartum mental health symptoms is through its impact on birthing experience and outcomes. To the best of our knowledge, extant research has not examined antenatal/lifetime IPV’s impact on birthing experiences, but existing research demonstrates that those experiencing IPV during their pregnancy were more likely to experience low birth weight and preterm birth as compared to those women who did not experience IPV during their pregnancy (Berhanie et al., 2019). A better understanding of how antenatal IPV exposure impacts birth and postpartum outcomes could inform prevention strategies for negative birthing outcomes and postpartum mental health symptoms.
Relatedly there has been an increase in attention on postpartum mental health intervention, with these efforts largely focused on postpartum depression. Several promising interventions have been proposed for both the prevention and management of perinatal depressive symptoms including but not limited to pharmacological treatment (Ali et al., 2021; Deligiannidis et al., 2021), cognitive behavioral intervention (Branquinho et al., 2020), and complementary approaches such as yoga and physical activity (Reza et al., 2018). However, with a heavy focus on postpartum depression, postpartum anxiety symptoms have largely been ignored in this literature base which is a notable weakness given that postpartum anxiety symptoms are common (Fawcett et al., 2019), especially after experiences of IPV (Navarrete et al., 2021). Further, little is known about how these interventions impact symptoms for those with a history of IPV compared to those without. More research is needed on the generalizability of postpartum mental health interventions across trauma-exposed persons, particularly with regard to anxiety symptoms. Trauma-informed postpartum mental health interventions should be the standard of care, given the frequency of both antenatal trauma histories as well as those who experience traumatic childbirth (Alcorn et al., 2010).
As such, the present work had three aims: (1) Examine the impact of a lifetime history of IPV exposure assessed at baseline (i.e., during pregnancy, prior to 25 weeks’ gestation) on birthing experience, hypothesizing that those with a pre-pregnancy history of IPV will have a more negative birthing experience than those without, (2) Examine IPV history at baseline as a moderator of the relationship between negative birthing experience and postpartum anxiety symptoms, hypothesizing that those with an IPV history will report worse anxiety symptoms in the postpartum period following a negative birth experience than those without an IPV history, and (3) Compare the effects of an intervention, spanning across the course of pregnancy, (i.e., Mamma Mia/Mamma Mia Plus) on anxiety symptoms in those with a history of IPV versus those without. Aim three was exploratory and thus no hypothesis was specified given the lack of prior literature examining postpartum mental health interventions in trauma-exposed populations. Although postpartum anxiety symptoms were our primary outcome of interest, we tested these same aims with depressive symptoms as an outcome as well.
Methods
Procedures
Data for the current study come from a multi-site randomized control trial (i.e., “Mamma Mia”) of an internet and mobile-based intervention for preventing and reducing perinatal mental health symptoms (Kinser et al., 2021). The full study protocol, including ethical safeguards for participants, is described in detail elsewhere (Kinser et al., 2021). As a brief overview, Mamma Mia recruited pregnant women less than 25 weeks’ gestation in the United States who were then randomly assigned to one of three conditions: “Mamma Mia,”“Mamma Mia Plus,” and usual care, whereby the “Mamma Mia” group received only the mobile-based intervention modules and the “Mamma Mia Plus” group received the mobile-based modules as well as brief guided support from a registered nurse. Participants were also required to have regular access to the Internet, a working email address, and a working phone since the intervention was delivered solely via the Internet and mobile device. All data for the parent study, and the current study, was collected via the internet-based platform, REDCap. Primary assessments for the present study were collected at the baseline (pre-birth), 3-month post-delivery, and 6-month post-delivery time points.
Measures
Demographic Covariates
All demographic variables were assessed at the baseline time point (i.e., during pregnancy; prior to 25 weeks gestation). For all demographic variables, dummy codes were created comparing the groups endorsed most by participants to allow for comparisons between groups.
Race/Ethnicity
Participants endorsed which racial/ethnic category they identified with from the following options: Latino/Hispanic, African American/Black, Asian/Pacific Islander, Native American/Alaska Native, Caucasian/White, or Other. Dummy codes were created for this variable allowing for comparisons between the following groups: White versus African American/Black, White versus Latino/Hispanic, and White versus Other with Other including all participants identifying as Asian/Pacific Islander, Native American/Alaska Native, and Other. These groups were collapsed into the “Other” dummy code given the relatively small number of participants endorsing these categories precluding the ability to make statistically powered comparisons.
Education Level
Participants endorsed whether their highest level of education completed was elementary school, high school, some college (at least 1 year), college degree, or graduate degree. The dummy codes created for this variable were: College degree versus high school, college degree versus some college, and college degree versus graduate degree. No participants included in the present study endorsed elementary school as their highest level of education completed.
Marital Status
Current marital status was assessed by asking participants to endorse one of the following: Single, living with a partner, married, divorced/separated, widowed, or other. The dummy codes created from this variable were: Married versus single, married versus living with a partner, or married versus other which included those that endorsed divorced/separated, widowed, and other given that all three of these categories were minimally endorsed by participants.
Income Level
Participants reported on their current annual family income by endorsing one of the following options: Less than $15,000, $15,000 to 34,999, $35,000 to 49,999, $50,000 to 99,999, or $100,000 or more. Most participants endorsed having an annual family income of $100,000 or more, $50,000 to 99,999, or $35,000 to 49,999 and thus the dummy codes created for this variable were $100,000+ versus $50,000 to 99,999, $100,00+ versus $35,000 to 49,999, and $100,000+ versus. Other including those endorsing an annual family income of less than $15,000 or $15,000 to 34,999.
Baseline Measures
Intervention Group
To compare outcomes between the three intervention groups, dummy code variables were created to allow for the comparison of the control group versus Mamma Mia and the control group versus Mamma Mia Plus. As previously noted, the specifics of these interventions are described in detail elsewhere (Kinser et al., 2021).
Intimate Partner Violence Exposure
A history of lifetime exposure to IPV was assessed via two self-report items. The first asked whether the participant had ever been in a relationship with someone who had “pushed, hit, kicked, or otherwise hurt [you]”? The second asked if the participant had ever been in a relationship with someone who “[you] are afraid to disagree with because they might hurt [you]”? Response options for both items were “0” for no and “1” for yes. In the present analyses, the two items assessing IPV exposure were summed to create an IPV “total” with possible values ranging from zero to two.
Follow-up Measures
Birth Experience
Birth experience was assessed at around 3 weeks postpartum using items from the Childbirth Experience Questionnaire (CEQ; Dencker et al., 2010). The CEQ is a 22-item self-report measure that assesses a woman’s perception and feelings about their childbirth experience. It includes items such as: “Labor and birth went as I had expected” and “I felt strong during labor and birth.” Items are scored on a Likert scale ranging from 1 (“totally disagree”) to 4 (“totally agree”). For the present analyses, all items were summed to create a total birth experience score with higher scores indicating a more positive birth experience. This questionnaire has demonstrated good sensitivity and in the present sample, demonstrated excellent reliability (α = .90).
Anxiety Symptoms (Primary Outcome)
The primary outcome of interest in the present paper, anxiety symptoms, were assessed at the 3 and 6-month follow-up timepoints using a subset of questions from the Edinburgh Postnatal Depression Scale (EPDS; Cox et al., 1987). Specifically, items three, four, and five (EPDS-3A) were summed to create a total anxiety score with higher scores indicating higher levels of anxiety as has been done in previous work in the field (Smith-Nielsen et al., 2021). These items ask how often in the past 7 days a participant has “blamed [myself] when things went wrong,” has felt “anxious or worried,” and has “scared or panicky.” The EPDS-3A has shown acceptable validity and reliability, with internal consistency being strong in the present sample at both time points (α3 months = .76; α6 months = .77)
Depressive Symptoms (Secondary Outcome)
The secondary outcome of interest, depressive symptoms, were assessed at the 3 and 6-month follow-up timepoint using ten items from the EPDS (Cox et al., 1987), as is standard in the field. Although anxiety is our primary outcome of interest, we tested similar models for depressive symptoms given the notable focus on postpartum depression within the field of women’s mental health. All 10 items from the EPDS were summed to create a total depressive symptom score. Items on the EPDS ask participants how often in the past 7 days they have felt symptoms such as: “Sad or miserable,”“So unhappy that I have been crying,” etc. The EPDS demonstrated strong reliability in the current sample at both time points (α3months = .85; α6 months = .86).
Data Analytic Plan
Before conducting primary study analyses, descriptive statistics and correlations among study variables were calculated (see Tables 1 and 2). All analyses were performed using SPSS 29 software (IBM Corp, 2022).
Demographic and Clinical Characteristics of Study Sample (n = 1,912).

Correlations Among Primary Study Variables (n = 1,912).
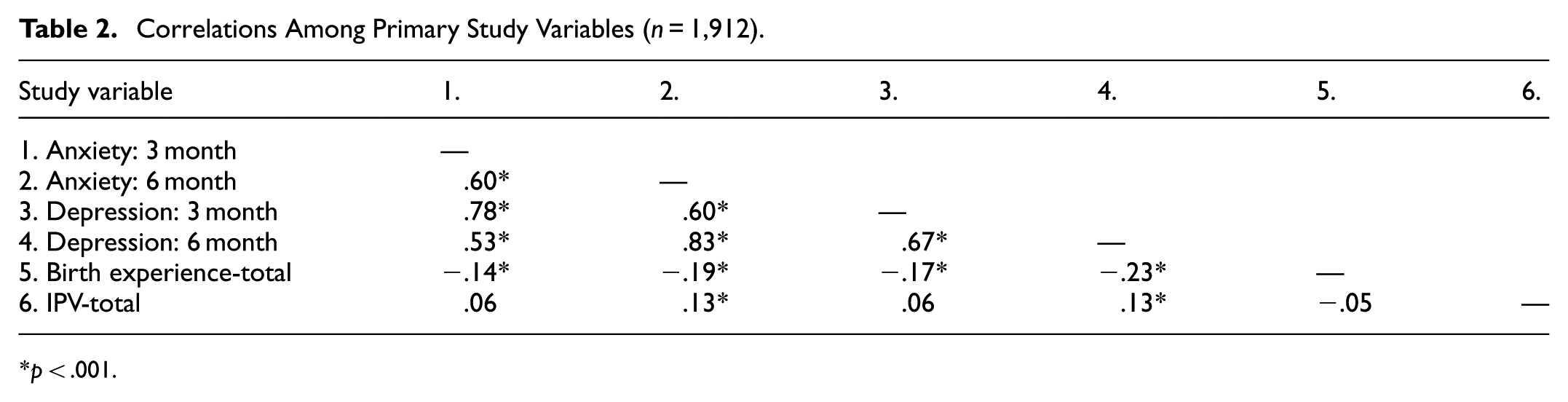
p < .001.
Aim 1
Our first aim was to examine if a history of IPV at baseline was related to one’s birthing experience as reported at the 3-week postpartum time point while controlling for key covariates (i.e., race/ethnicity, education level, income level, and marital status). A linear regression model was tested to assess IPV on subsequent birthing experience.
Aim 2
The second aim of the present paper was to examine total IPV exposure as a moderator of the relationship between birth experience and postpartum anxiety symptoms at both the 3-month postpartum and 6-month postpartum follow-up time points. While anxiety symptoms were our primary outcome of interest, we also tested these models with postpartum depression at 3 and 6 months as an outcome as well. To do so, we used the PROCESS (Hayes, 2022) macro in SPSS 29. Four models were tested with birth experience as the independent variable, IPV total as the continuous moderator, and 3-month anxiety, 6-month anxiety, 3-month depression, and 6-month depression as the outcome variables respectively. These models controlled for key covariates (i.e., race/ethnicity, education level, income level, and marital status).
Aim 3
Our third aim was to compare the effects of a perinatal intervention (Mamma Mia/Mamma Mia Plus) on anxiety symptoms in those with a history of IPV versus those without. For aim three analyses, IPV exposure was re-coded into a dichotomous variable (vs. used as a continuous variable for aims 1 and 2) whereby “0” indicated no IPV exposure and “1” indicated lifetime history of IPV exposure given the requirements of a two-way ANOVA. As noted previously, these models were also tested with postpartum depression as an outcome. We conducted two-way ANOVAs with intervention group status and IPV status as the two factors and anxiety symptoms at both 3 and 6 months as the outcome variable. When effects were significant, we conducted pairwise comparisons to examine at what level differences were meaningful.
Results
Sample Descriptives
Participant characteristics and descriptive statistics are presented in Table 1. In the total sample (n = 1,912), participants were 30.7 (±4.6 SD) years old on average. Generally, participants had a college degree (38.9%) or a graduate degree (33.9%), reported making less than $100,000+ annually (45.3%), and reported having been pregnant once before the current pregnancy (33.2%). The majority (60.7%) identified as non-Hispanic white and as currently married (72.2%). There were no significant differences on study variables between intervention groups.
Zero-Order Correlations
Table 2 provides the zero-order Pearson correlations among primary study variables. Associations amongst the variables of interest were generally as would be predicted. More specifically, anxiety at both time points was positively associated with depression at both time points and negatively associated with birthing experience as higher scores on the CEQ indicate a more positive birth experience. IPV was associated with anxiety and depressive symptoms at six-months only and not significantly correlated with birthing experience.
The Impact of IPV on Birthing Experience
Findings from our first aim, examining the impact of IPV history on one’s subsequent birthing experience are presented in Table 3. Results demonstrated a significant covariate effect whereby those identifying as “other” race/ethnicity were more likely to report a more negative birth experience as compared to those identifying as white. Lifetime IPV exposure at baseline did not significantly predict one’s birthing experience score at the three-week postpartum follow-up time point. None of the key covariates were associated with subsequent birth experience.
Linear Regression Predicting Birthing Experience at 3 Weeks Postpartum.

Note. For all race variables, White = 0, African-American, Latina, or Other is coded as 1. W to B refers to those identifying as White as compared to those identifying as Black and/or African American. W to L refers to those identifying as White versus those identifying as Latina. W to O refers to those identifying as White as compared to those identifying as “Other.” Edu = education; HS = high school; Some = some college; Grad = graduate degree; Inc = income level. 100 to 50 refers to those making 100 k+ annually versus those making 50 k+ annually. 100 to 35 refers to those making 100 k+ annually versus those making 35k+ annually. 100 to O refers to those making 100 k plus annually versus all other income levels. Mar = marital status; Living = living with; O = all other marital status options; IPV = interpersonal violence history.
IPV as a Moderator Between Birthing Experience and Mental Health Symptoms
Our second aim examined IPV as a moderator of the relationship between birthing experience and anxiety and depressive symptoms at the 3 and 6-month timepoints, respectively (see Table 4). Significant covariate effects were evidenced for anxiety and depression at the 3-month time points. Identifying as Black/African American as compared to white was associated with greater anxiety symptoms. Those with a college education as compared to those with a high school education reported more anxiety symptoms, and those endorsing a marital status as “other” as compared to those identifying as married reported more anxiety symptoms as well. Those identifying as Black/African American or Latina reported more anxiety symptoms as compared to those identifying as White. With regard to depressive symptoms, those with a high school degree as compared to those with a college education were more likely to experience depressive symptoms.
Moderation of Birthing Experience on Anxiety and Depressive Symptoms by IPV at 3 and 6-Months.

Notes. For all race dummy codes, White is coded as “0”. B = Black/African American; L = Latina; O = other; Coll = college; HS = high school; Some = some college; Grad = graduate degree; Inc = income; Mar = martial status; Birth exp. = birth experience; IPV = interpersonal violence.
p < .05. **p < .01. ***p < .001.
Similar patterns were found across both outcomes. For anxiety and depressive symptoms at both time points, the interaction between IPV total and birth experience was non-significant. Thus, the interaction terms were dropped to allow for the examination of significant main effects. These main effects are presented in Table 4. Birth experience significantly predicted anxiety symptoms at the 3-month time point with a worse birth experience predicting greater anxiety symptoms. Anxiety at 6 months was significantly associated with birthing experience and lifetime IPV history such that a worse birth experience and a history of IPV were associated with greater anxiety symptoms. Birth experience was significantly associated with depressive symptoms at both 3 and 6 month such that a worse birth experience was related to a higher level of depressive symptoms, as would be expected. Lifetime IPV exposure was associated with depressive at 6 months only whereby those with a history of IPV reported higher depressive symptoms.
Differences in Mental Health Symptoms by IPV Status and Intervention Group
Aim three sought to examine differences in anxiety and depressive symptoms by IPV history status and intervention group using a series of two-way ANOVAS. Table 5 presents findings from comparisons between the control group and the Mamma Mia group. Table 6 presents findings from comparisons between the control group and the Mamma Mia Plus group. For all outcomes, the interaction between IPV and the intervention group was non-significant and thus, main effects were examined. When the main effects were significant, pairwise comparisons were conducted to identify where the significant difference was.
Findings from the Two-Way ANOVA Assessing Anxiety and Depressive Symptoms by IPV and Intervention Group (Control vs. Mamma Mia) at 3 and 6 Months.

Notes. SS = sum of squares; df = degrees of freedo; Sex: 1 = males, 0 = females; Race: 0 = White, 1 = Blacks, Asians, or other for each of the three dummy codes; TE = traumatic event; Peer = peer deviance; Parent = parental involvement; PTSD = probable PTSD; INTX = Y4 interaction term between new onset TE and resilience.
p < .05. **p < .01. ***p < .001.
Two-Way ANOVA Results Assessing Anxiety and Depressive Symptoms by IPV and Intervention Group (Control vs. Mamma Mia Plus) at 3 and 6 Months.

Notes. B = standardized regression coefficient; SE = standard error; Sex: 1 = males, 0 = females; Race: 0 = White, 1 = Blacks, Asians, or other for each of the three dummy codes; TE = traumatic event; Peer = peer deviance; Parent = parental involvement; PTSD = probable PTSD; INTX = Y4 interaction term between new onset TE and resilience.
p < .05. **p < .01. ***p < .001.
Control Versus Mamma Mia
The main effect of IPV on three-month anxiety symptoms was significant. More specifically, there were significant differences between those endorsing an IPV history versus those without an IPV history on three-month anxiety symptoms in the intervention group only. Those endorsing a history of IPV (M = 2.24, SD = .22) had a higher mean anxiety symptom level than those not endorsing an IPV history (M = 1.74, SD = .11). Findings for six-month anxiety symptoms were similar such that there was a significant difference between those endorsing an IPV history versus those not reporting an IPV history in the control group only, with those endorsing IPV having a higher mean level of anxiety symptoms (M = 3.53, SD = .21) than those without (M = 3.00, SD = .12).
Main effect analyses demonstrated that IPV history had a significant effect on six-month postpartum depressive symptoms. There was a significant main effect of IPV demonstrating that mean depressive scores differ based on IPV history in both the intervention group and the control group. In the intervention group, those with an IPV history (M = 7.67, SD = .78) have a higher mean depression score than those without (M = 5.64, SD = .40). A similar pattern was observed in the control group such that those with an IPV history (M = 7.32, SD = .50) have a higher mean depression score than those without (M = 6.37, SD = .28).
Control Versus Mamma Mia Plus
For analyses examining those in the control group vs. those receiving Mamma Mia plus with and without an IPV history, there were no significant interactions between the intervention group and IPV status. Thus, main effect analyses, including pairwise comparisons, are reported below.
There was a significant main effect of IPV on 3-month anxiety symptoms. However, pairwise comparisons demonstrated no significant difference between groups (intervention nor IPV status) on 3-month symptoms. In the control group only, there was a significant difference in 6-month anxiety symptoms between those endorsing a history of IPV (M = 3.53, SD = .23) versus those without (M = 2.97, SD = .12).
There was a significant main effect of IPV on depressive symptoms at the 6-month timepoint only. Pairwise comparisons showed significant mean differences between IPV versus no IPV in the control group only such that those with a history of IPV (M = 7.87, SD = .54) had a higher mean depression score at 6 months than those without an IPV history (M = 6.16, SD = .28).
Discussion
The present study had three aims focused on examining the relationships between IPV history, birth experience, and postpartum mental health symptoms. Although IPV history did not predict subsequent birth experience, findings demonstrated significant main effects of IPV history on both anxiety and depressive symptoms, and differences regarding main effects between intervention groups. These findings will be discussed in turn.
The Impact of IPV on Birthing Experience
Results from our first aim demonstrated that IPV experience at baseline did not significantly predict birthing experience assessed at 6 weeks postpartum. Although a non-significant finding, this adds to the small literature examining IPV history and birthing experience as the majority of the extant work in this area focuses on IPV exposure during pregnancy (e.g., Mazza et al., 2021). Our work meaningfully contributes to this area by examining the effects of lifetime IPV on the birthing experience. The IPV measure used in the present study assessed lifetime exposure; although a strength in expanding the existing literature, it may be that our finding was non-significant given that one’s exposure to IPV could have been any number of years before becoming pregnant and giving birth. It is possible that there is not an enduring effect of IPV exposure earlier in life on subsequent birthing experiences, and any effect likely depends on if and how the trauma was processed prior to pregnancy. Elderton et al. (2017) conducted a meta-analysis of 16 studies that examined post-traumatic growth (PTG; Tedeschi & Calhoun, 1996) among IPV survivors, and found that 71% of all IPV survivor participants reported growth. While experiencing PTG does not invalidate or minimize the deleterious impacts of IPV, growth experiences could interrupt the impact of IPV exposure on birthing outcomes. Therefore, additional work is needed with a more precise measurement of IPV exposure in terms of the type and timing of exposure, as well as potential PTG experiences, to fully understand how IPV history impact subsequent birth experiences and if PTG mediates that relationship.
IPV as a Moderator Between Birthing Experience and Mental Health Symptoms
In aim two we examined IPV as a moderator of the relationship between birth experience and subsequent anxiety symptoms (primary outcome) and depressive symptoms (secondary outcome). For anxiety at the 3-month timepoint, there was a main effect of birth experience on anxiety symptoms whereby a more negative birth experience was related to increased anxiety symptoms. At the 6-month timepoint, there were main effects of IPV history and birth experience on symptoms such that IPV exposure and worse birth experience were associated with more anxiety symptoms. The existing literature on postpartum mental health largely focuses on depressive symptoms and has historically isolated those symptoms from others. However, it is becoming increasingly clear that depression, anxiety, distress, obsessive-compulsive behaviors, and other similar symptoms are typically comorbid during the perinatal period and should not be evaluated in isolation (e.g., Farr et al., 2014; Shen et al., 2024, etc.). Thus, examining the impact of these harmful experiences on anxiety symptoms specifically is a meaningful contribution to the existing literature.
Our finding that birth experience is related to postpartum anxiety symptoms is consistent with the small existing literature that demonstrates that a lack of control during labor, low self-confidence for the delivery and the delivery staff, and premature delivery are all risk factors for the development of postpartum anxiety (Field, 2017). Lifetime IPV exposure being related to postpartum anxiety symptoms in this data was unsurprising given that IPV exposure is heavily associated with posttraumatic stress disorder (Hegadoren et al., 2006), generally speaking, and PTSD and anxiety are closely related with PTSD previously being categorized as an anxiety disorder in the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2000). Even still, results demonstrating that IPV history predicts later postpartum anxiety symptoms suggests a pertinent risk factor for providers to screen for when considering postpartum mental health prevention and intervention efforts.
A similar pattern of findings emerged for depressive symptoms such that birth experience predicted depressive symptoms at 3 months, and birth experience and IPV history predicted depressive symptoms at the 6-month time point. These findings are consistent with the expansive literature examining risk factors for postpartum depression (e.g., (Malta et al., 2012; Moyer & Kinser, 2021; Tani & Castagna, 2017), though again, much of this literature examines IPV in the perinatal period specifically, whereas we examined lifetime IPV history. Taken together, our findings from aim two may help to identify women at risk for postpartum psychopathology allowing for the effects of screening and treatment in the prenatal period to persist on postpartum mental health, benefiting new mothers and families in the longer term.
Differences in Mental Health Symptoms by IPV Status and Intervention Group
Our third aim sought to examine if 3- and 6-month anxiety and depressive symptoms differed significantly by both IPV status and intervention group. Results from this aim suggest differences in psychopathology between control versus intervention groups, indicating that the intervention(s) positively impact symptoms. Second, findings demonstrate that there are differences by IPV status, suggesting that lifetime IPV may have a lasting impact on postpartum mental health and that the two interventions tested here may have different implications for those with an IPV history versus those without.
Control Versus Mamma Mia
When comparing the control group to the individuals who received the Mamma Mia intervention, there was a significant difference in mean anxiety symptoms at 3 months between those endorsing IPV versus those without a history of IPV in the intervention group only. This finding suggests that the Mamma Mia intervention was effective in reducing anxiety symptoms for those without IPV but not for those with an IPV history. However, at 6 months postpartum, IPV was significantly associated with greater anxiety symptoms in the control group, but not in the intervention group. This suggests the intervention may have buffered the impact of IPV on maternal anxiety, reducing the risk typically observed in control participants. To the best of our knowledge, there is no existing research assessing the effectiveness of a perinatal mental health intervention for anxiety symptoms in a trauma-exposed population making it difficult to contextualize these findings. The majority of the existing research has focused on the impact of interventions for posttraumatic stress disorder symptoms and in individuals who have experienced birth trauma specifically (Taylor Miller et al., 2021), thus our findings add to this small literature by examining anxiety symptoms specifically and focusing on those with an IPV history. Our results provide early evidence that a trauma-focused intervention for postpartum anxiety may be warranted.
There was a significant difference between groups on 6-month depressive symptoms for both the control and intervention groups. These results suggest that the Mamma Mia intervention and standard of care procedures impacted six-month depressive symptoms in both groups (i.e., IPV vs. no IPV) in the same capacity. This may be due to the longer period between birth and assessment of symptoms (i.e., 3 vs. 6 months) such that intervention programming for postpartum mental health may be more effective if delivered over a longer period following one’s birth experience. However, resources are often limited given the demands on new mothers, which must also be considered when balancing intervention effectiveness with practicality and feasibility for this population. This finding, in comparison to the anxiety symptom finding, may also suggest that the Mamma Mia intervention targets anxiety symptoms more effectively as compared to depressive symptoms when delivered to women who have experienced IPV.
Control Versus Mamma Mia Plus
Findings from the present study evidenced a significant difference between those with an IPV history and those without on 6-month anxiety symptoms in the control group only indicating that the Mamma Mia Plus intervention reduced symptoms for those with and without an IPV history equally. As noted previously, there is a dearth of literature examining postpartum mental health intervention on anxiety and/or depressive symptoms in a trauma-exposed population. The Mamma Mia Plus intervention expands upon the Mamma Mia intervention by adding brief guided support from a registered nurse (Kinser et al., 2021). This extra support and guidance may increase the effectiveness of the Mamma Mia intervention for trauma-exposed populations who have an increased need for active intervention ingredients. For example, social support has been shown to improve symptoms in trauma-exposed populations (e.g., Calhoun et al., 2022). The additional contact from a registered nurse may provide this social support increasing the effectiveness of Mamma Mia Plus for trauma-exposed individuals. For depressive symptoms, there was a significant mean difference at the 6-month time point for those with an IPV history versus those without in the control group only, again suggesting that perhaps the “Plus” part of the Mamma Mia intervention is increasing the effectiveness of the intervention on depressive symptoms for trauma-exposed individuals. While PTG is possible post-trauma, PTG, post-traumatic stress, and depression can co-occur (Cobb et al., 2006). In fact, according to the dual-factor model of posttraumatic responses (Hamby et al., 2022), promoting high PTG may be more beneficial than simply decreasing mental health symptoms following trauma.
Implications, Limitations, and Future Directions
Attention to the role of PTG and resilience in people with a history of traumatic life experiences is critical and must be considered when evaluating the effectiveness of Mamma Mia and Mamma Mia Plus. PTG is defined as positive psychological change experienced because of a struggle with stressful, traumatic, or challenging life events or circumstances (Calhoun & Tedeschi, 2001). A strengths-based, growth-oriented perspective is necessary when working with people who have trauma histories. Post-traumatic growth, by definition, suggests that while trauma has negative impacts there is potential for positive impacts on self-perception of personal strength, new possibilities, relationships with others, spiritual strength, and appreciation of life. Both the Mamma Mia and Mamma Mia Plus interventions may have improved participant’s postpartum symptoms via addressing a number of these areas and thus exerted a moderating impact on symptoms following IPV exposure. However, additional work is needed to dismantle the impact of intervention components on levels of PTG and subsequently, how a potential increase in PTG may buffer against symptoms. Importantly, post-traumatic growth is not just returning to the pre-trauma status quo, rather it is a cognitive process that reflects a transformative and lasting change to one’s baseline levels of adaptation to adversity (Tedeschi & Calhoun, 2004). PTG is a critical factor in mental health recovery including the reduction of mental health symptoms and increased wellbeing (Barskova & Oesterreich, 2009), which may have played a role in the effects of the intervention. Further insight into which specific components of the Mamma Mia and Mamma Mia Plus trials facilitated PTG, though outside of the scope of the current work, is critical in informing future intervention design for postpartum women with an IPV history.
Indeed, there are important implications from the current work for clinical practice in OB-GYN settings. The findings of this study underscore the critical need for routine screening for IPV exposure during the perinatal period. Given the significant association between IPV history and heightened postpartum anxiety and depressive symptoms, healthcare providers should be trained to recognize and assess trauma histories in birthing individuals. Integrating trauma-informed care into perinatal and postpartum mental health services is essential, particularly as traditional interventions may be less effective for those with trauma exposure.
The differential outcomes observed between intervention groups highlight the effectiveness of tailored, trauma-informed interventions—specifically, the Mamma Mia Plus program—in improving postpartum anxiety among those with an IPV history. This supports the implementation of strengths-based, posttraumatic growth-oriented approaches that acknowledge the unique needs and resilience of trauma-exposed individuals. In clinical practice, interdisciplinary teams should prioritize individualized care plans that incorporate trauma-informed mental health interventions and provide ongoing support throughout the postpartum period. Establishing clear referral pathways and access to digital mental health tools like Mamma Mia Plus could serve as a scalable strategy to address the mental health burden among postpartum individuals with IPV histories.
Although the present work makes a meaningful contribution to the existing literature, it is not without limitations. First, IPV history was assessed using two questions in the interest of reducing participant burden with regard to the required surveys. However, a more comprehensive assessment of IPV history including the exact timing of the event, if the exposure was ongoing versus one single incident, the specific type of event (i.e., physical vs. emotional vs. sexual), etc., would allow for a more nuanced understanding of exactly how IPV impacts postpartum mental health outcomes. Relying on a dichotomous (yes/no) measure of IPV may oversimplify the complexity and variability of these experiences, potentially masking important differences in frequency, severity, and chronicity that are critical for understanding psychological outcomes. A more nuanced understanding would then allow for more targeted screening procedures and subsequent prevention efforts before one’s birth experience, ultimately reducing the rates of postpartum psychopathology in those who are most at risk. Relatedly, the current study did not include a measure of PTSD symptoms, limiting any inferences that can be made about how lifetime IPV exposure may also influence subsequent PTS symptoms as the hallmark psychiatric disorder following trauma exposure.
The majority of the sample included in the present analyses identified as white, well-educated, married, and of relatively high socioeconomic status. Existing research shows that individuals identifying as racial or ethnic minorities experience more negative birth experiences and higher rates of subsequent postpartum psychopathology, largely due to persistent systemic health disparities, discrimination, and differential access to quality care (e.g., Su et al., 2021). Therefore, the homogeneity of the current sample significantly limits the generalizability of the findings. Specifically, these results may not accurately capture the experiences or needs of individuals from underrepresented or marginalized groups, including Black, Indigenous, and other people of color, as well as those with lower educational attainment, unmarried status, or limited financial resources. These populations are not only at increased risk for adverse postpartum mental health outcomes but are also often excluded from research, perpetuating a cycle of inadequate representation and poorly tailored interventions. As such, future research should prioritize the recruitment and inclusion of diverse populations to ensure that prevention and intervention strategies are equitable, culturally responsive, and widely applicable across various demographic groups.
Lastly, all surveys were self-report in nature, introducing biases inherent in self-report measurement (e.g., Furnham & Henderson, 1982). However, self-report measures allow for more comprehensive assessments with fewer resources. Future research that assesses trauma history, anxiety symptoms, depressive symptoms, and PTSD symptoms with gold-standard clinical interviews by a trained clinician may provide a more accurate depiction of the influence of IPV history and birth experience on postpartum anxiety and depressive symptoms. The present study focused on symptoms in the 3- and 6-month postpartum period. Future research would benefit from assessing the evolution of anxiety and posttraumatic stress symptoms over time after childbirth (e.g., up to 12-months postpartum).
Despite these limitations, findings from the present study suggest that IPV history is an important risk factor for the development of postpartum anxiety and depressive symptoms and that Mamma Mia Plus, an online-based intervention for postpartum depressive symptoms, may be uniquely effective for trauma-exposed populations.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by 5R01HD100395-04 (PI: Kinser) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. SC's time was supported by 4T32MH020030-24 from the National Institute of Mental Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.