
Abstract
The high incidence and mortality rates of cervical cancer are global health concerns. Families of cervical cancer patients often encounter difficulties and face great pressure. Family resilience can assist them handle the crisis. This study aimed to explore the influencing factors of family resilience in patients with cervical cancer, providing a reference for healthcare staff to carry out targeted interventions. Data were collected from 280 individuals in two tertiary Class A hospitals in Jiangsu province, China between September 2022 and October 2023. Using a self-created general information questionnaire and several scales (Family Resilience Questionnaire, 10-item Conner-Davidson Resilience Scale, Herth Hope Index, Family APGAR scale, and Social Support Rating Scale), 258 patients completed the questionnaire with a participation rate of 92.1%. Linear regression analyses were used to examine the predictive variables of family resilience. The average family resilience score was 113.70 ± 16.30. Communication and cohesion scored highest, while religiousness and spirituality scored lowest, Predictors of family resilience included monthly per capita household income (β = .142, p = .011), religiousness (β = .281, p < .001), degree of hopefulness (β = .173, p = .001), psychological resilience (β = .190, p = .002), effectiveness of family functioning (β = .142, p = .008), and social support (β = .267, p < .001). Those diagnosed with cervical cancer have a relatively high family resilience. Family income and religious belief are the main factors. Improving psychological resilience, hope, family function, and social support can also promote it.
Introduction
Cervical cancer, the second most prevalent gynecological cancer globally, has a significant impact on developing countries, leading to high morbidity and mortality (Guo et al., 2021; Singh et al., 2023). According to the International Agency for Research on Cancer. (IARC), around 604,000 women were diagnosed with cervical cancer in 2020, and approximately 342,000 women lost their lives to this disease (Viveros-Carreño et al., 2023). Despite the availability of vaccines and screening programs that aid in early detection and effective treatment, the occurrence and fatality rates of cervical cancer remain alarmingly high in developing nations (Liu et al., 2021; Nguyen et al., 2022). This is particularly true in central and western regions of China, as well as rural areas, where population size, geographic location, and economic conditions contribute to the inability to achieve desired reductions in mortality rates (Hu et al., 2023; Li et al., 2021; Qin et al., 2022).
Currently, the primary approach to treating cervical cancer involves surgical procedures, radiation treatment, chemotherapy, and pharmaceutical intervention. Nevertheless, postoperative complications are highly prevalent (Han et al., 2021). In the case of patients with cervical cancer, they encounter symptoms associated with reproductive function, including issues with urination dysfunction, vaginal discharge, and decreased sexual function. Therefore, the family is not just the main provider of physical, psychological, and societal assistance, but also plays an active role in the healing and recuperation process (Goldberg-Looney et al., 2017; Rat et al., 2021). Furthermore, researchers have documented that enduring pain caused by treatment and resulting patient complications places the burden of caregiving on the family (Yeh et al., 2021). During this phase, families experience significant psychological consequences and stress due to multiple factors, while simultaneously having to ready themselves for future rehabilitation. Hence, greater focus ought to be directed towards individuals suffering from cervical cancer as well as their families. More and more researchers have observed that dealing with adversity is an intricate procedure and necessitates adjusting the whole family system (Henry et al., 2015).
According to Patterson, family resilience refers to the positive behavior and functional competence displayed by a family unit during challenging or unfavorable situations (Park et al., 2022; Walsh, 2016). It highlights the family as an entire and confirms its potential to recover and thrive in the face of adversity, which is crucial for maintaining the physical and mental well-being of family members and the normal functioning of the family (Huang et al., 2019; Kuang et al., 2023). Patients with cancer experience symptoms directly related to the disease, while family members also bear the burden of providing care due to psychological and financial instability (González-Blanch et al., 2010). Family resilience is present in every family activity, but not every family member can overcome obstacles in dealing with crises and stimulate the potential of family resilience. This also explains why some families can adapt to pressure and challenges while others cannot withstand similar ones. As the medical care model continues to transform, an increasing number of scholars have recognized that nursing services are not merely about promoting the health of individual patients but also require the expansion of services to the family and society. The process of dealing with adversity is not a simplistic one where an individual exploits his or her advantages in isolation. Rather, it is a process that involves the entire family system [29]. Scholars have also gradually taken individuals, families, and society as a whole to carry out research.
Review of Literature
Hope can guide patients to correctly understand the disease and establish health beliefs, deal with pressure with a positive and optimistic attitude, and promote the improvement of family resilience (Haugan et al., 2013). Psychological resilience refers to the ability of an individual to effectively adapt and maintain or restore mental health when facing adversity or experiencing setbacks. It is a positive internal coping resource (Luo et al., 2020). As an internal resource for coping with stress, individual psychological resilience is a protective factor in stressful situations and can effectively regulate the relationship between negative life events and individual stress responses (Tao et al., 2023). In the multilevel model analysis of family resilience in advanced cancer patients by Cui et al. (2023), it was confirmed that individual psychological resilience is a better internal adjustable factor for family resilience. Family function is used to describe the characteristics and structure within the family, including emotional connections among family members, family rules, communication methods, and the degree of care and emotional expression towards each other, these factors all affect the health status of family members and the effectiveness of dealing with external events (Serrano et al., 2023). In an intervention study on family resilience of children with cancer by Park et al. (2023), it was mentioned that good family function can generate positive emotional experiences for patients, weaken the pressure on the family caused by difficult situations, be conducive to family communication and problem-solving, and promote the improvement of family resilience. Social support usually refers to the material or spiritual help that an individual obtains from the outside world, mostly from the support of friends, the community, and society. Some studies have shown that social support is significantly positively correlated with family resilience and is a positive predictive factor for family resilience (W. Zhang et al., 2023) [64]. In the study by Mao et al. (2021) on evaluating the psychosocial path of family adaptation in liver cancer patients, it was confirmed that social support, as an external resource, can provide information and emotional assistance to the family, promote communication and mutual support among family members, and enhance their perceived internal family support.
Faccio, Renzi, Giudice, et al.’s (2018) research indicate that family resilience can assist family members in activating recovery when confronted with cancer diagnosis and treatment, and facilitate the family function to attain a new equilibrium and harmony. Family resilience not only influences the adaptability of family members to cancer but also impacts the treatment outcome of cancer patients and the entire cancer progression (Faccio, Renzi, Crico, et al., 2018). Although foreign studies on the factors affecting the family resilience of gynecological cancer patients exist (Kim & Ahn, 2022), the research results are not representative due to the heterogeneity of the study population and significant regional and cultural differences. Moreover, previous research has shown a significant association between family resilience and the family functioning of patients with liver cancer and their caregivers in China (Mao et al., 2021). In addition, similar studies have demonstrated a positive association between family resilience in lung cancer patients and their caregivers (Wang et al., 2021). Domestic scholars have explored the family resilience of patients with other types of cancer. However, different disease types may exhibit variations in family resilience. Currently, there is a lack of research on the factors affecting the family resilience of cervical cancer patients in China. Prior research has validated that many factors, ranging from social and interpersonal aspects to individual aspects, are predictors of family resilience (Saetes et al., 2017). However, few studies have investigated the influence of these factors on family resilience in individuals diagnosed with cervical cancer. Thus, what is the level of family resilience of Chinese cervical cancer patients? What are the influencing factors? And how can we improve the family resilience of cervical cancer patients to help them resist pressure, overcome difficulties, and achieve family adjustment? These questions are worthy of consideration and in-depth investigation.
Aim
This study is designed to explore the level of family resilience in patients with cervical cancer and the factors influencing it. Specifically as follows: First, investigate the current situation of demographic characteristics, family resilience, hope level, psychological resilience, family function, and social support among Chinese patients with cervical cancer. Second, clarify the correlations between hope level, psychological resilience, family function, social support, and family resilience. Third, analyze the influencing factors of family resilience in patients with cervical cancer from multiple angles.
Theoretical Basis
McCubbin and McCubbin (1996) Resiliency Model of Family Stress Adjustment and Adaptation (RMFSAA) mainly focuses on the dynamic adaptation process of families when confronted with stress and crises. It is a comprehensive model divided into the adjustment stage and the adaptation stage, used to understand how families adjust and adapt in stressful situations to maintain their function and health. (1) Adjustment Stage: When facing mild or short-term stress, the family reevaluates its goals, values, and behavior patterns, and reestablishes a good balance via fine-tuning. It may experience emotional fluctuations, communication difficulties, etc., but through mutual support and cooperation, can gradually adjust its internal structure and function. (2) Adaptation Stage: If a major stress event causes maladaptation, the family changes its operation mode. It first needs to comprehensively and specifically assess itself and the stress source, stimulate resilience to cope with stress, regain balance and harmony, and then achieve family recovery through specific methods. The key in this stage is whether the family can effectively adjust its structure and function to adapt to external environment changes. RMFSAA emphasizes the importance of both internal resources (support, communication, and cooperation skills among family members, as well as the family’s values and beliefs, etc.) and external resources (social support, professional help, and other social resources), which can help families to cope with stresses and challenges, and facilitate their adaptation and resilience. Based on the theoretical model, fully utilizing internal and external resources can enhance the adaptive resilience of families to better face stresses and challenges (Henry et al., 2015). The reason for selecting this model is that it places greater emphasis on concentrating on the dynamic adaptation process of families in the face of stress and crisis, incorporating the analysis of distinct adjustment and adaptation phases, and highlighting the significance of internal and external resources. It is capable of helping to understand the family’s coping mechanism and offering theoretical and practical guidance for strengthening the family's adaptive resilience and dealing with stress and challenges.
McCubbin and McCubbin (1996) proposed that family resilience is a process of positive interaction among individuals, families, and the external environment. The stimulation and adjustment of family resilience is a process from the individual to the family level. Family factors jointly cope with the adverse effects of stress events through interaction, promoting the family to reach an excellent adaptive state. According to a review of prior research on various sample groups, the potential elements affecting family resilience consist of personal aspects (individual resilience and the hope of patients and family members [Card & Barnett, 2015; Wen et al., 2022]), interpersonal aspects (family function, defined as the perceived support and care among family members, indicating the contentment of family members with the family [Mao et al., 2021]), and societal aspects (social support, referred to the assistance, care, and resources that individuals received from their social networks, such as family, friends, and community organizations [Y. Zhang et al., 2023]). Based on RMFSAA as the theoretical model, we selected variables from internal and external resources to explore the influencing factors of family resilience for cervical cancer patients. Internal resources include individual resilience, the level of hope, and family functioning. External resources include social support.
Materials and Methods
Study Design
This study was conducted in two tertiary Class A hospitals located in Jiangsu Province, China. Adopting a cross-sectional survey with a correlational design methodology, it sought to explore the interrelationships among family resilience, psychological resilience, hope level, family function, and social support. Furthermore, it analyzed the influencing factors of family resilience in patients with cervical cancer.
Participants
Based on the cluster sampling method of hospitalized cases, we selected cervical cancer inpatients from two tertiary Grade A hospitals in Jiangsu Province between September 2022 and November 2023. To be eligible for the study, participants had to meet the following criteria: (1) Patients with cervical cancer diagnosed through clinical and pathological histology; (2) Age of 18 years or older; (3) Individuals who are aware of and have received the disease diagnosis; (4) Those who provide informed consent and voluntarily participate in the study; (5) Alert individuals capable of understanding the questionnaire content, without communication barriers and able to cooperate with the investigator. The exclusion criteria were: (1) Unstable condition or in critical condition; (2) Combined with other malignant tumors or other serious chronic diseases; (3) Patients with previous serious psychological disorders or mental illness.
According to the sample size method (Wang & Ji, 2020), it is recommended that the sample size be increased by 5 to 10 times compared to the number of variables. The number of independent variables in this study was 28, and considering the 20% loss-to-follow-up rate, the ideal range of sample size would be 168 to 336. Therefore, the estimated sample size for this study was 250.
Measures
The general information questionnaire, compiled by the researchers on their own, it includes demographic data (age, marital status, educational level, occupation, place of residence, mode of payment for medical expenses, per capita monthly family income, living conditions, main caregiver, and presence or absence of religious belief, etc.) and disease data (disease course, clinical stage, treatment method, presence or absence of metastasis or recurrence, and presence or absence of other chronic diseases). Among them, the disease data are collected by the researchers from the patient’s electronic medical records.
The family resilience questionnaire (FaREQ) was developed by Italian scholar Faccio, Gandini, et al. (2019). After Li et al. (2022) translated it into Chinese. It is mainly used to dynamically assess the family resilience and adaptability of cancer patients. The questionnaire consists of four dimensions: communication and cohesion (items 1–8), perceived social support (items 9–16), perceived family coping (items 17–20), and religiousness and spirituality (items 21–24), making a total of 24 items. The scale employs the Likert 7-level scoring method. A score of 1 means “strongly disagree,” and a score of 7 means “strongly agree.” The total score ranges from 24 to 168. The higher the score, the stronger the resilience level of the patient’s family. This questionnaire has been confirmed to have good reliability and validity, with a Cronbach’s α coefficient of .910. In this study, the Cronbach’s α coefficient is .851.
The Chinese version of the Herth Hope Index (HHI), was translated and modified by Zhao Haiping to evaluate the hope level of clinical patients, and its psychometric properties have been empirically tested (Zhao & Wang, 2000). Twelve items of the HHI belong to three dimensions (Cronbach’s α = .850) namely, temporality and future, positive readiness and expectancy, and interconnectedness. The rating of items was done using a Likert-type scale with four points (1 = strongly disagree, 2 = disagree, 3 = agree, 4 = strongly agree). The total score of Dimension 1 is the sum of scores of items 1, 2, 6, and 11. Dimension 2’s total score is that of items 4, 7, 10, and 12. Dimension 3 is the sum of scores of items 3, 5, 8, and 9. Hopefulness can be measured on a scale of 12 to 48, where higher scores reflect greater levels of hope. In this study, the Cronbach’s α coefficient is .734.
Psychological resilience was measured in the study using the Chinese version of the 10-item Conner–Davidson Resilience Scale (CD-RISC-10), a shortened version of the original 25-item CD-RISC consisting of a single-dimensional scale of 10 items (Ye et al., 2017). Items were rated using a five-point Likert-type scale (0 = not true at all, 4 = true nearly all the time; Cronbach’s α = .909). High levels of resilience were reflected by the total scores obtained by summing all responses, which ranged from 0 to 40, with high scores (Shin et al., 2018). In this study, the Cronbach’s α is .895.
To assess family function, the Chinese version of the Family APGAR scale (APGAR) was utilized, a tool translated by lv Fan, for measuring family members' satisfaction with the functioning of a family (Lv et al., 1999). This scale included five dimensions: Adaptation “A,” Partnership, “P,” Growth, “G,” Affection, “A,” and Resolve, “R.” A total of five items, each item represents one dimension. Each item was given points based on a Likert scale with three points (0 = never, 1 = sometimes, and 2 = often). The total score ranged from 0 to 10 with high scores indicating better family function (Cronbach’s α = .851). In this study, the Cronbach’s α is .841.
The research assessed social assistance by utilizing Xiao’s (1994) Social Support Rating Scale (SSRS). The scale consists of ten items categorized into three dimensions: subjective support (the total score of items 1, 3, 4, and 5), objective support (the total score of items 2, 6, and 7), and social support utilization (the total score of items 8, 9, and 10), which were evaluated using a four-point Likert-type scale, with 1 indicating never and 4 indicating fully met. High social support levels were indicated by high scores on a scale ranging from 12 to 66 (Cronbach’s α = .923). In this study, the Cronbach’s α is .717.
Data Collection Procedure
In August 2022, 60 cervical cancer patients were chosen following stringent inclusion and exclusion criteria for a preliminary investigation. To validate the rationality and feasibility of the survey design, the suitability of the research tools, and the duration of the study, and promptly adjust the problems arising during the investigation process to further refine the research plan.
The formal investigation was conducted from September 2022 to November 2023, and the participants who took part in the pre-test were excluded to guarantee the validity of the research results. The investigators collected disease data of patients from electronic medical records, including disease course, clinical stage, and treatment method. They established subject case profiles to understand the basic situation of patients’ families and made adequate preparations for the questionnaire survey. Two trained nursing graduate students issued paper questionnaires to each respondent in the oncology department and gynecology ward to collect other data. The study subjects were selected in strict accordance with the inclusion and exclusion criteria. According to the actual condition and status of the patients, the investigators chose a relatively stable time for investigation when the patient's condition was stable. In order to protect the privacy of participants, avoid external influences, and enhance generalizability, undisturbed wards or demonstration classrooms were selected as the survey locations. When collecting data face to face, the investigator used the questionnaire to explain the purpose of the survey to the respondents, informed them of the questionnaire filling method and matters needing attention, and ensured the anonymity and confidentiality of personal data; All the questionnaires were completed independently by the patients and collected on the spot. However, for older patients with limited education and difficulty in filling out the questionnaire, the investigator dictated the instructions, entries, and options to the questionnaire and filled it in for them to ensure objective records. Consistent answers were given to any questions raised by patients to ensure the accuracy of the data.
Each questionnaire is numbered. Two researchers input them into Excel files. Questionnaires with identical answers, inconsistencies or logic errors are eliminated one by one. All questionnaires are reviewed for logical consistency; invalid ones that can't be repaired are deleted. Finally, the study recruited 280 potential participants, out of which 258 were included in the study. Of these, 22 cases did not match the criteria and were excluded (response rate: 92.1%). See Figure 1 for details.

Flowchart of the screening process of study participants.
Ethics Consideration
This study followed the Declaration of Helsinki specified in 1975 by the World Medical Congress, with revisions made in 2000. It was approved by the Ethics Committee of the *** Hospital of *** City (Ethics number: KY-20221130001-01). Before the commencement of the study, the test protocol was approved. The purpose, procedure, and possible risks of the study were introduced, and a written informed consent was signed to inform the study subjects of their right to withdraw from the study at any time. The privacy of the study subjects and the data confidentiality during the study were protected.
Data Analysis
In this study, data were analyzed using SPSS 25.0. Descriptive statistics, including frequency (n), percentage (%), mean (M), and standard deviation (SD), were employed. The Independent sample t-test (or Mann–Whitney U test) and ANOVA (or Kruskal–Wallis H-test) were utilized. Additionally, Pearson correlation analysis (for normally distributed data) or Spearman correlation analysis (for non-normally distributed data) was used to test the correlation between continuous variables and family resilience and its dimensions. Through univariate analysis and correlation analysis, statistically significant variables were screened out as independent variables, with family resilience as the dependent variable. These variables were then included in the multiple linear regression model to analyze the factors influencing family resilience. Statistical significance was indicated by a p-value < .05 in all two-sided tests.
Results
Demographic Characteristics
The majority of individuals in the study were aged 40 to 60 years (n = 162, 62.8%), married (n = 222, 86.0%), and farmers (n = 165, 64.0%). The primary caregivers were mainly adult children (n = 126, 48.8%) and spouses (n = 116, 45.0%). Monthly per capita household income ranged from 1,000 to 3,000 RMB for approximately half of the participants (n = 108, 41.9%). Approximately half (n = 155, 60.1%) responded that the new rural cooperative medical insurance paid their medical expenses. Stage II cervical cancer accounted for the majority (n = 78, 30.2%), followed by Stages III (n = 72, 27.9%) and I (n = 64, 24.8%). Treatment duration was 1–3 months (n = 65, 25.2%) or >1 year (n = 60, 23.3%). For treatment, the number of patients who underwent surgery + radiotherapy was more than half (n = 152, 58.9%); the rest underwent radiotherapy + chemotherapy (n = 66, 25.5%). The results of the univariate analysis demonstrated that the respondent’s level of education (p = .002), occupation (p = .001), region of residence of family (p = .001), payment method (p < .001), monthly per capita household income (p < .001), and religious affiliation (p < .001) were independently correlated with family resilience (Table 1).
Characteristics of Participants and the FaREQ Score (n = 258).

Notes. N = number; M = mean; SD = standard deviation; FaREQ = family resilience questionnaire.
Scores of Family Resilience and Other Related Variables
In this study, The FaREQ scores in patients with cervical cancer were consistent with a normal distribution, it achieved 113.70 ± 16.30 out of 168 points, surpassing the midpoint. The communication and cohesion score was 48.61 ± 5.65, out of a total of 56 points. The level of perceived social support was 35.96 ± 9.02 indicating a high level on a scale of 28 points. The level of perceived family coping was 20.02 ± 4.74 on a scale of 56 points, indicating a moderate to high level. The level of religiousness and spirituality scored 9.11 ± 6.94 out of 28 points, indicating relatively low levels. The scores of the CD-RISC-10 conformed to a normal distribution. The total score was 25.76 ± 5.89, and it was a single-dimensional scale. Likewise, the HHI score also conformed to a normal distribution. The total score was 37.66 ± 4.14, and the average score per item was 3.14 ± .35. Among the three dimensions of the Herth Hope Index, the dimension of positive readiness and expectancy had the highest mean score of 3.25 ± .44, whereas the dimension of temporality and future had the lowest mean score of 3.02 ± .36. As for the SSRS score, it fitted a normal distribution. The total score was 41.69 ± 5.88, and the average score per item was 4.17 ± .58. The subjective support was the highest at 6.26 ± .97, while the support utilization was the lowest at 2.17 ± .63. In contrast, the AGPAR score did not follow a normal distribution. Employing M (P25, P75), the score range was from 0 to 10 points, with a score of 9.00 (7.00, 10.00) points (Table 2).
Level of Family Resilience and the Dimensions in Cervical Cancer Patients (n = 258).
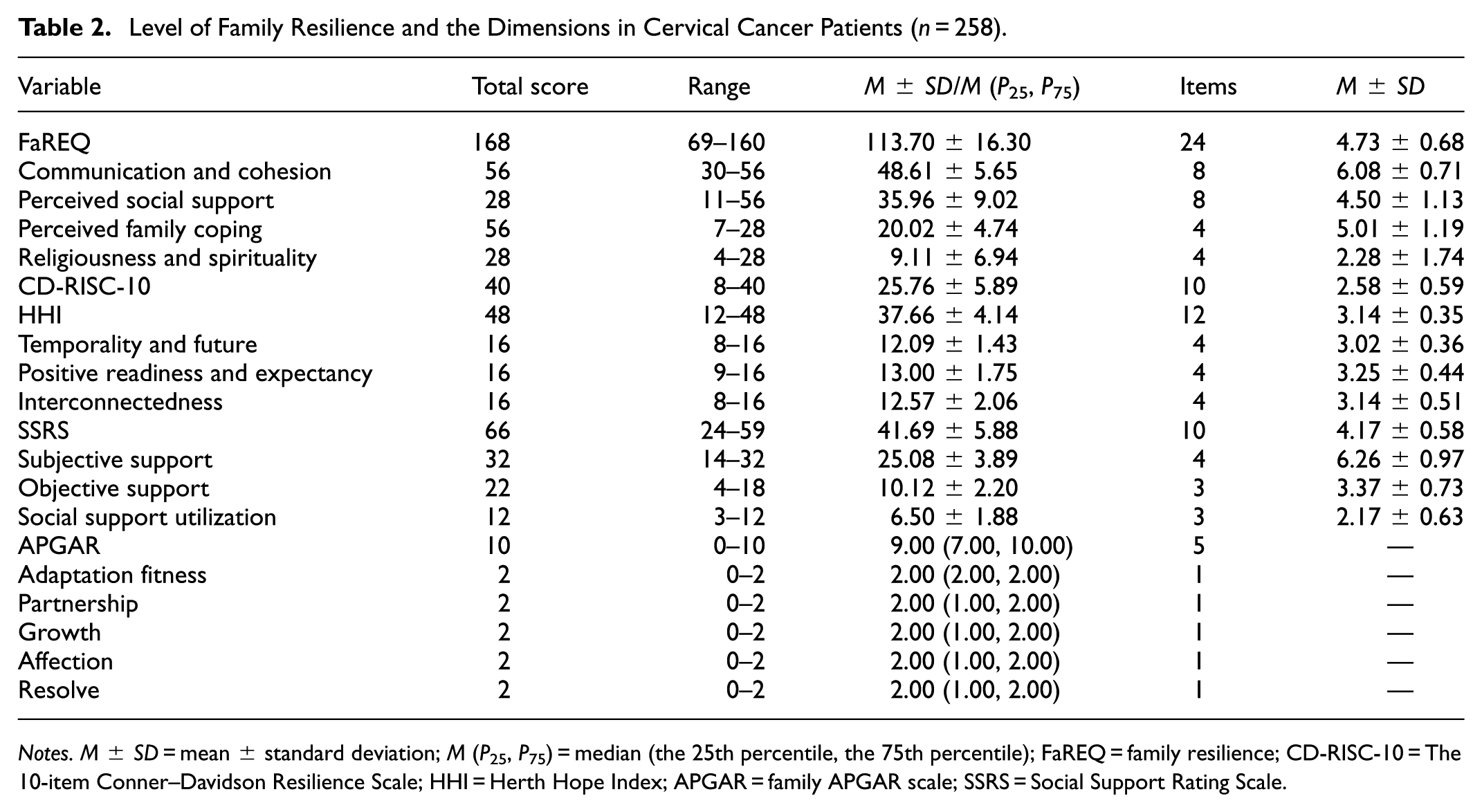
Notes. M ± SD = mean ± standard deviation; M (P25, P75) = median (the 25th percentile, the 75th percentile); FaREQ = family resilience; CD-RISC-10 = The 10-item Conner–Davidson Resilience Scale; HHI = Herth Hope Index; APGAR = family APGAR scale; SSRS = Social Support Rating Scale.
Description and Correlation Between Family Resilience and Other Study Variables
Among all variables, family function scores were non-normally distributed and other variables were normally distributed, so Spearman correlation analysis was used in this study. The analysis results revealed that Family resilience in patients with cervical cancer was positively associated with communication and cohesion (r = .535, p < .01), perceived social support (r = .763, p < .01), perceived family coping (r = .604, p < .01), religiousness and spirituality (r = .510, p < .01), level of hope (r = .434, p < .01), individual psychological resilience (r = .557, p < .01), family function (r = .480, p < .01), and social support (r = .546, p < .01). Nevertheless, religiousness and spirituality were not significantly related to communication and cohesion or perceived family coping and exhibited a slight positive correlation with perceived social support (r = .136, p < .05). In addition, religiousness and spirituality were not significantly related to the level of hope, individual psychological resilience, or family care. Among the subcomponents of family resilience, perceived family coping showed a positive moderate correlation with communication and cohesion (r = .341, p < .01) and perceived social support (r = .209, p < .01; Table 3).
Correlations Between Family Resilience and Other Study Variables.
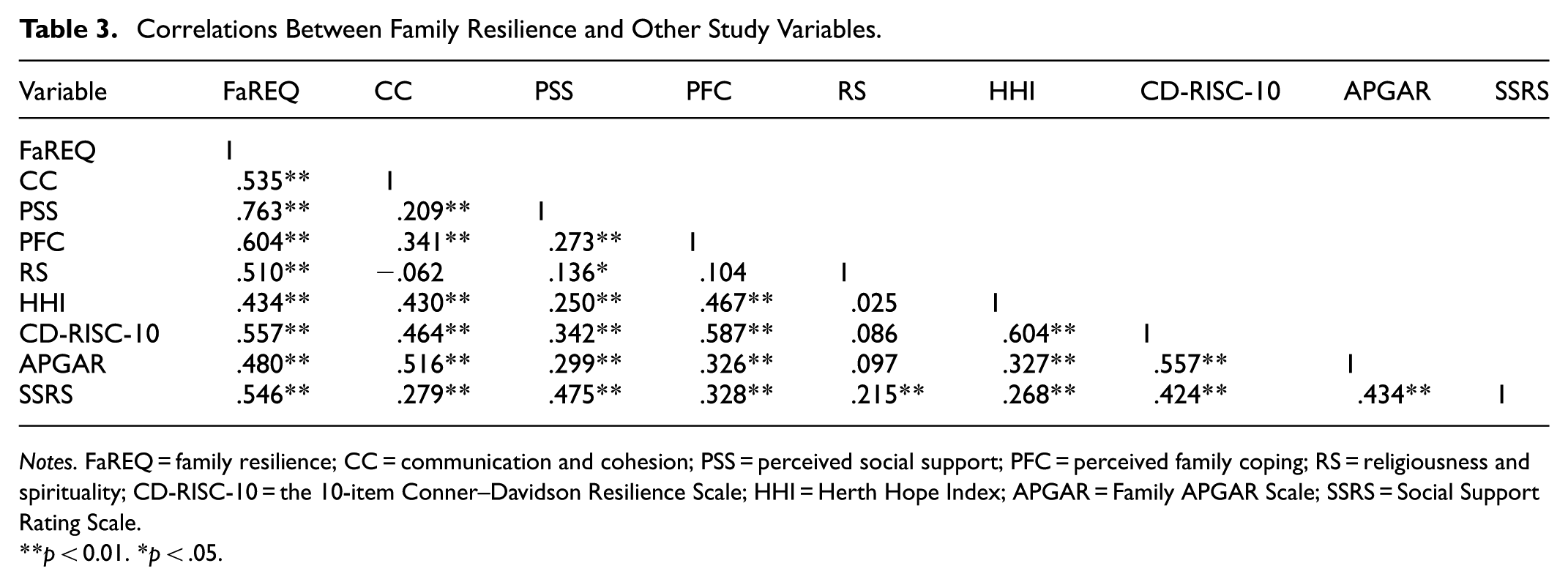
Notes. FaREQ = family resilience; CC = communication and cohesion; PSS = perceived social support; PFC = perceived family coping; RS = religiousness and spirituality; CD-RISC-10 = the 10-item Conner–Davidson Resilience Scale; HHI = Herth Hope Index; APGAR = Family APGAR Scale; SSRS = Social Support Rating Scale.
p < 0.01. *p < .05.
Multiple Linear Regression Analysis of Family Resilience
In multiple linear regression analysis, taking the total score of family toughness as the dependent variable, the independent variables from univariate analysis (educational level, occupation, family living region, payment method, monthly per capita household income, religious affiliation) and the variables correlated with family resilience (HHI, CD-RISC-10, APGAR, and SSRS) were incorporated into the regression model. Assuming linear relationships between the independent and dependent variables and no complete or high linear correlation among the independent variables. Multicollinearity was detected by employing the variance inflation factor method. The specific assignments are provided in Table 4.
Variable Assignment Methods.
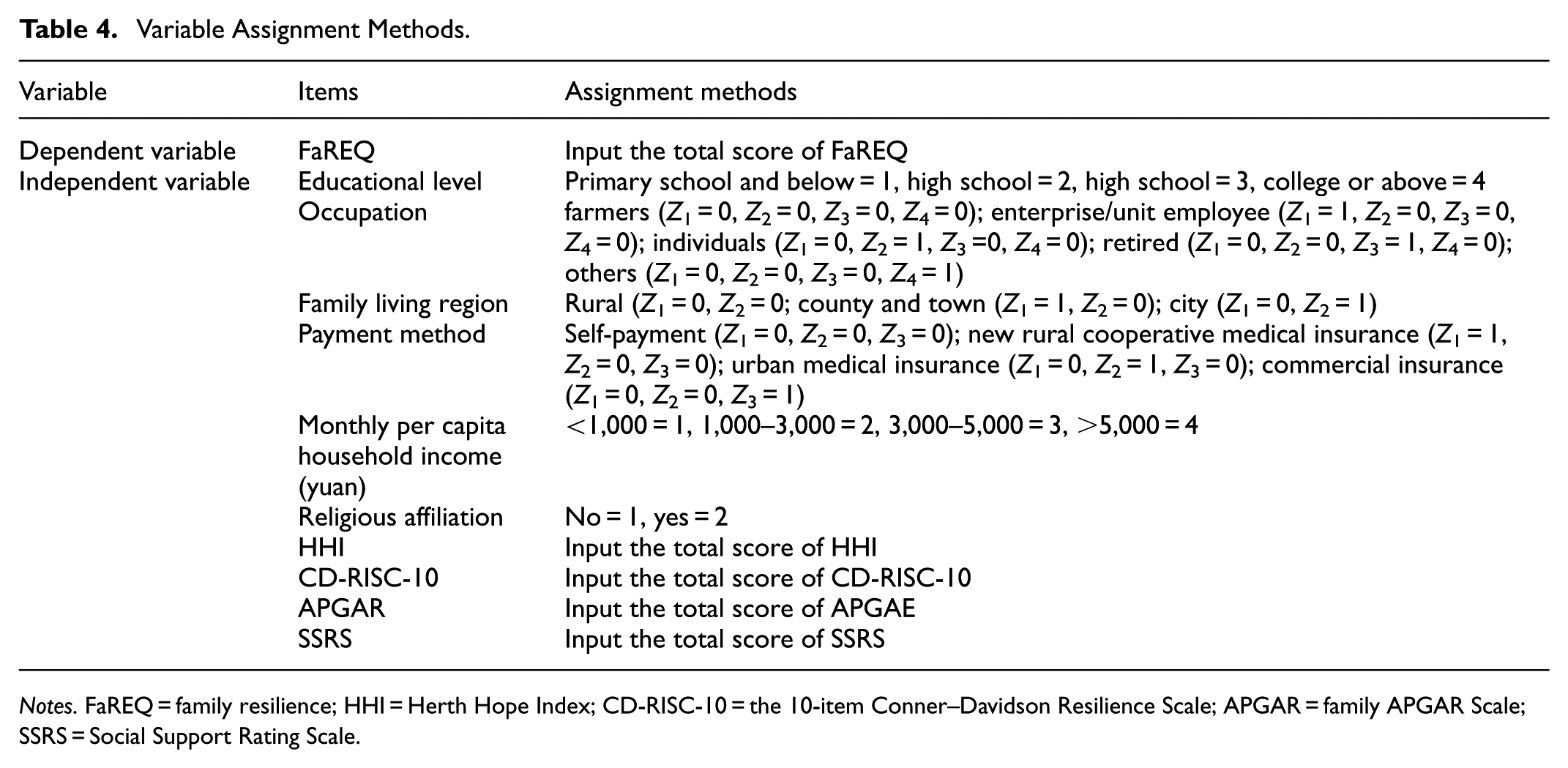
Notes. FaREQ = family resilience; HHI = Herth Hope Index; CD-RISC-10 = the 10-item Conner–Davidson Resilience Scale; APGAR = family APGAR Scale; SSRS = Social Support Rating Scale.
Before conducting the multiple linear regression analysis, the study validated the appropriateness of the data by checking the regression equation assumptions (normality and linearity multicollinearity) and examining the residuals (normality of residuals, independence of errors, and equal variance). To ensure the error’s independence, the regression model's inclusion criterion was set at α = .05. The range of tolerance (.458–.898) and the variance inflation factor, varying between 1.113 and 2.182, suggest that there are no issues with multicollinearity among the independent variables.
The factors that were significant for family resilience were monthly per capita household income (β = .142, p = .011), religiousness (β = .281, p < .001), HHI (β = .173, p = .001), CD-RISC-10 (β = .190, p = .002), APGAR (β = .142, p = .008), and SSRS (β = .267, p < .001). In other words, family per capita monthly income, religious belief, level of hope, psychological resilience, family function, and social support were entered into the regression equation. These six variables play a significant role in determining the level of family resilience in patients with cervical cancer, explaining 56.6% of total variation, as shown in Table 5.
Multiple Regression Analysis of FaREQ Among Cervical Cancer Patients (n = 258).

Notes. R 2 = .593, adjusted R2 = .566, F = 21.946, p < .001. B = unstandardized coefficients; β = standardized coefficients; FaREQ = family resilience; CD-RISC-10 = the 10-item Conner–Davidson Resilience Scale; HHI = Herth Hope Index; APGAR = family APGAR scale; SSRS = Social Support Rating Scale.
Discussion
Analysis of the General Demographic Characteristics of Cervical Cancer Patients
A total of 258 cervical cancer patients were involved in this study. The majority of them were aged between 40 and 60 years old, constituting 62.8% (162 cases). A preponderance of these patients hailed from rural areas, accounting for 58.1% (150 cases). This is largely in accord with the epidemiological data on cervical cancer in China. Survey results indicate that the incidence of cervical cancer in China peaks in the 50 to 54 age group, and the incidence in rural areas is higher than that in urban areas (Cai et al., 2023). In this study, 50.4% (130 cases) of cervical cancer patients had an educational attainment of primary school or below. Some had junior high school and high school education, comprising 44.2% (114 cases). There were relatively few patients with college/bachelor’s degrees, occupying only 5.4% (14 cases), suggesting that the educational level of cervical cancer patients is relatively low. This situation may be related to the age structure and the era in which the research subjects lived. Insurance-paying patients accounted for 96.9%, which is attributable to the national policy of popularizing medical insurance. Among them, the new rural cooperative medical insurance accounted for 60.1% (155 cases), and urban medical insurance accounted for 36.8% (95 cases). The majority of patients’ occupations were farmers, making up 64.0% (165 cases). This is relatively consistent with the proportion of the new rural cooperative medical insurance in the payment method at 60.1%. This may be because this survey pertains to provincial and municipal tertiary hospitals, and cervical cancer patients are more inclined to seek treatment in local large hospitals. The per capita monthly income of patients was concentrated in the range of 1,000 to 3,000 yuan, accounting for 41.9% (108 cases), which may be related to the region surveyed in this study. The main caregivers were adult children, constituting 48.8% (126 cases), and spouses, accounting for 45.0% (116 cases). The reason may be that the vast majority of cervical cancer patients in this study were married (86%, 222 cases). Caregivers, mostly children and spouses, regard caring for family members as an obligation or responsibility, which is closely related to Chinese cultural traditions (C. Li et al., 2023) In this study, 30.2% (78 cases) of patients had stage II cervical cancer, and 27.9% (72 cases) had stage III. A small proportion of patients with stage IV accounted for 17.1% (44 cases). Among them, 98 cases (38.0%) of patients had metastasis, indicating that most patients were already in the middle and advanced stages when diagnosed with cervical cancer and failed to detect tumors in the early stage in a timely manner. This may be related to the patient’s lack of attention to or understanding of early screening for cervical cancer.
Current Status of Family Resilience in Cervical Cancer Patients
The objective of this research was to examine the degree and contributing factors of familial resilience among individuals diagnosed with cervical cancer. The findings indicated that patients experience significant emotional distress, including anxiety, fear, and feelings of loss, as a result of the disease's impact on their physical functioning (Düzgüneş et al., 2019; Smith, 2015). Depression and anxiety in individuals with cervical cancer have a significant impact on the process of healing, mental well-being, and overall life satisfaction. These conditions can disrupt the functioning of families, resulting in reduced levels of family resilience. In the current sample, the scores for family resilience were moderate or high for communication and cohesion (48.61 ± 5.65), perceived social support (35.96 ± 9.02), and perceived family coping (20.02 ± 4.74). This finding resembled that of a different research, which indicated higher than average scores for support from families of cervical cancer patients compared to gynecological cancers like breast, uterine, and ovarian cancer (Chen et al., 2022).
Communication and cohesion were positive predictors of family resilience. The latest discovery indicated that individuals diagnosed with cervical cancer who have spouses and children exhibited elevated levels of family resilience and improved communication for solving problems. Patients may communicate their thoughts or needs to their closest family members, such as spouses and children, while receiving care, which promotes family communication and problem-solving. Family resilience was positively predicted by perceived social support. In prior research, it was discovered that when confronted with stress and family emergencies arising from gynecologic cancer, the families of patients possess the means to seek assistance from nearby communities and society (Kim & Ahn, 2022). This current study revealed that social support was correlated with family resilience and the subdimensions of problem-solving communication and family coping. Hence, to enhance family resilience as a source of social support, society must offer increased assistance to the families of such individuals. This would facilitate the patient’s understanding of the accessible social support and encourage their proactive utilization of the support already in place. The coping level of the families of these participants was higher than the midpoint, similar to the coping level reported for families of individuals with different types of cancers like digestive, respiratory, and genitourinary (Postolica et al., 2017; Yeh et al., 2023). These findings have implications for enhancing family resilience in cervical cancer survivors.
Analysis of Influencing Factors of Family Resilience in Cervical Cancer Patients
According to the results of multiple linear regression analysis in this study, family per capita monthly income, religious belief, psychological resilience, hope level, and family function and social support, are all factors that affect the family resilience of cervical cancer patients (p < .05). The following is the discussion.
We discovered a positive correlation between the level of family resilience and monthly per capita household income. Specifically, as the monthly per capita household income increases, so does the score of family resilience. On the contrary, it is also stated that higher levels of poverty are associated with lower family resilience. The findings were in line with Matos et al.’s (2021) research. The researchers mentioned that affluent families do not have to face overwhelming financial burdens and can afford to prioritize long-term postoperative recovery, chemotherapy, and radiotherapy, as well as extended treatment duration caused by cancer recurrence, which enhances family resilience (Ghanouni & Hood, 2021). This indicates that medical staff should pay particular attention to the families of patients with relatively poor economic conditions. If necessary, they should seek medical aid and policy support to relieve the economic pressure on these families. Nevertheless, there are also studies suggesting that a family’s economic income has no influence on family resilience. Hence, more research is required to probe into the relationship between family resilience and socio-demographic characteristics.
Additionally, the results of multiple linear regression analysis showed that religiousness and spirituality were positive factors for family resilience in cervical cancer patients (p < .001), Put simply, the greater the religious devotion, the greater the degree of family resilience. The results add to the increasing amount of research that indicates the significant impact of religious beliefs and spiritual practices on the context and culture of individuals who have survived cervical cancer. According to earlier research, incorporating faith-based or spiritual care into the treatment of cancer patients has been found to improve their quality of life and health outcomes (Kamijo & Miyamura, 2020; Koenig, 2012). In the current study, patients with religious affiliation and spirituality had high levels of family resilience, which indicates that religiousness and spirituality are some of the major facilitators of family resilience among patients diagnosed with cervical cancer. It must be admitted that in this study, the number of cervical cancer patients with religious beliefs was small (20.2%, 52 cases), which may cause result bias. The influence of religious belief on family resilience may vary due to factors like culture and personal faith intensity. In this research, despite the small number of people with religious beliefs, it is a significant influencing factor for family resilience, possibly related to the family resilience scale introduced by Chinese scholars. Due to cultural differences, it may affect the assessment results. In China’s political and cultural context, there are many types of religious beliefs, including Buddhism, Christianity, Islam, Taoism, Tudigong, Confucianism, Catholicism, Bodhisattva, etc. Chinese religious beliefs not only include beliefs in superhuman entities but also encompass worship and respect for ancestors, families, and blood ties, which help generate positive emotions and a sense of self-well-being in patients, such as love, forgiveness, comfort, and reduced stress. The above research findings indicate that medical personnel should respect patients’ beliefs and perspectives, encourage them to find strength and hope within religious beliefs, and seek appropriate spiritual support to alleviate mental pressure.
Furthermore, in this study, we classified variables according to McCubbin’s resilience model into internal variables and external variables. The internal variables included psychological resilience, hope level, and family function. The external variable was social support. Our analysis using multiple linear regression revealed that these variables were the key determinants affecting the family resilience of patients with cervical cancer.
As one of the internal variables, psychological resilience reflects the adaptability and recovery ability of patients when facing disease challenges. We examined the connection between family resilience and psychological resilience in the households of individuals diagnosed with cervical cancer and found a positive correlation, which indicates families of patients with higher scores show greater resilience. The results of this study align with previous research on the families of individuals diagnosed with cancer (Hwang et al., 2018; Kiani et al., 2020). The reason underlying this result was that patients with good psychological resilience were aware of cancer but continued to hold a strong desire for life, fully utilized the resources around them to seek help, and actively improved their health behavior, which may affect the level of family resilience (Mao et al., 2021). According to Card and Barnett (2015), psychological resilience plays a crucial role in enabling patients and their family members to effectively manage stress, foster family resilience, and achieve positive family adaptation. Higher psychological resilience can help patients better cope with stress and maintain a positive attitude, thereby enhancing family resilience.
The hope level also has an important impact on family resilience. Our study discovered a positive correlation between family resilience in individuals diagnosed with cervical cancer and their level of hope, indicating that those with higher levels of hope tend to have stronger family resilience. Patients full of hope are more likely to actively participate in the treatment and rehabilitation process, bring positive energy to the family, and promote the stability and harmony of family relationships. Having hope is particularly crucial for maintaining good mental health, as it serves as a safeguard against stress and illness and as a necessary condition for successful treatment outcomes (Yaghoobzadeh et al., 2019). NikoLoudi et al. (2021) discovered that by implementing strategies that boost hope, patients with heart failure can experience better physical health and psychological well-being due to the increased levels of hope. Similarly, for individuals with cancer, hope plays a crucial role in helping them face the challenges of cancer head-on and build resilience (Wu et al., 2021). Bando et al. (2018) noted that hope is seen as the core of caring for patients with lung cancer and providing appropriate support is important for alleviating treatment-related symptoms. Therefore, improving the level of hope could reduce stress responses and negative emotions toward cancer and surgery, which improves the coping style of patients, promotes postoperative recovery, and, thus, improves family resilience.
The findings demonstrated that family function had a positive correlation with the degree of family resilience. A possible reason is that a good family function can promote effective interaction between family members and help them establish a positive good role adaptation, which, thus, improves the degree of family resilience (Kukihara et al., 2020). The family function is also indispensable among internal factors. A family environment full of care and support can provide patients with emotional reliance, enhance their confidence, and further improve the overall resilience of the family. Individuals diagnosed with cervical cancer usually face multiple pressures such as the loss of reproductive organs after surgery, the distress caused by chemotherapy-related symptoms, disease progression and recurrence, and are prone to have negative emotions such as inferiority, depression, and anxiety, and cope with the disease in a negative way. Good family care and family warmth will encourage patients, help them feel their importance to their families, actively rehabilitate treatment, and successfully cope with the crisis (Jin, 2023). This current study contributed additional evidence to the existing literature on family function, emphasizing the relationship between great family function and high levels of family resilience in advanced cancer. Medical professionals can offer tailored health education based on the specific circumstances of the patient’s family, fostering a warm and harmonious environment that promotes the well-being of families dealing with cervical cancer.
Social support as an external variable is also an important factor affecting the family resilience of patients with cervical cancer. The current study uncovers compelling proof of the correlation between family resilience and social support, presenting a new and unique perspective. Social support can come from friends, neighbors, the community, and the medical team. A good social support network can provide practical help such as financial support and care services for patients and their families, and at the same time give emotional encouragement and comfort. This external support can reduce the burden on families and enhance their ability to cope with diseases. Positive behavior can be encouraged and negative emotions can be diminished through the provision of social support. A previous study found that social support is increasingly viewed as a priority area when supporting people experiencing mental distress (Ma et al., 2020). Additional studies have also shown the positive impact of social support on the psychological well-being and self-efficacy of individuals with prostate cancer (Weber et al., 2007). For these patients, both previous and current studies strongly indicate that social support indirectly improves mental health, such as alleviating symptoms of depression and anxiety, by enhancing internal mental resources (Q. Li et al., 2023). These studies highlight the significance of social support. Nevertheless, little research has thoroughly investigated the correlation between social assistance and family resilience in individuals diagnosed with cervical carcinoma. The findings pointed to a positive association between social support and family resilience, indicating the need for providing social support to families of individuals diagnosed with cervical cancer.
Implications
The exploration of factors influencing family resilience in cervical cancer has significantly contributed to the field. Theoretically, it has refined the application of family resilience theory specifically in relation to cervical cancer scenarios, enriching the theoretical framework with more detailed understandings. It has also delved deeper into the stress and adaptation mechanisms characteristic of cancer families, furnishing empirical evidence that enriches the existing body of knowledge. Practically, this study has helped identify specific targets for clinical interventions, allowing for the formulation of more targeted and effective measures. It has offered valuable guidance for developing comprehensive family support plans to ensure their practicality and effectiveness. Moreover, it has improved communication and collaboration between healthcare providers and families, promoting the well-being of patients. Methodologically, the study has presented paradigmatic examples for analogous research endeavors centered on family resilience in other diseases, thereby contributing to the refinement and evolution of research methodologies within this domain.
Limitations
We must acknowledge certain limitations of our study. First, this study only selected 258 cervical cancer patients from two public hospitals as research subjects. The number of participants is very small, and there are issues such as regional differences and insufficient sample representativeness, which may lead to bias in the research results and make the research conclusions very fragile. This means that the sample may not comprehensively capture the full spectrum of characteristics and variations present in the entire population of cervical cancer patients. Subsequent studies can expand the sample size and use stratified random sampling methods to conduct cross-regional, multi-center research.
Second, this research investigated the factors influencing family resilience in cervical cancer patients and determined the correlations between family resilience and variables such as psychological resilience, hope level, family function, and social support. However, we are unable to establish the causal relationship and specific action paths among these variables. In the future, a structural equation model can be constructed to deeply analyze the potential interaction mechanism between various variables and family resilience, thereby revealing the complex interrelationships among these factors and verifying their influence paths on family resilience.
Furthermore, as this study is a cross-sectional study, it merely examined the level of family resilience of cervical cancer patients at a single point in time and was unable to reflect the process and trend of its changes. Since the level of family resilience changes dynamically with time and environment, in the future, we will conduct longitudinal follow-up studies to explore the change trajectory of family resilience and construct and implement effective intervention programs for verification.
Conclusions
This research discovered that family resilience holds great importance for the families of cancer patients. The family resilience level of cervical cancer patients is relatively high. Family per capita monthly income and religious belief have a certain impact on the family resilience of cervical cancer patients. There is a significant positive correlation between the social support, psychological resilience, hope level, and family function of cervical cancer patients and family resilience. At the same time, they are also predictive factors affecting family resilience. To improve the family resilience of cervical cancer patients, it is necessary to assess the family resilience level by evaluating communication and cohesion, perceived support from social networks, family coping mechanisms, and religious and spiritual beliefs. Special attention should also be paid to low-income families and non-religious families. Medical staff should implement targeted interventions according to the specific circumstances of patients’ families and encourage cervical cancer patients to actively obtain supportive resources. By enhancing personal psychological resilience, being hopeful for the future, strengthening family functions, and expanding the social support network, the family resilience level can be comprehensively improved to help cervical cancer patients and their families better cope with various challenges brought by the disease.
Supplemental Material
sj-xls-1-sgo-10.1177_21582440251374438 – Supplemental material for Family Resilience and Its Influencing on Patients with Cervical Cancer in China: A Cross-Sectional Study
Supplemental material, sj-xls-1-sgo-10.1177_21582440251374438 for Family Resilience and Its Influencing on Patients with Cervical Cancer in China: A Cross-Sectional Study by Jin Wang, Fengqin Xu, Ling Yang, Na Lv and Yuting Zhu in SAGE Open
Footnotes
Acknowledgements
We express our gratitude to all the individuals who volunteered and participated in the current research.
Ethical Considerations
This study followed the Declaration of Helsinki specified in 1975 by the World Medical Congress, with revisions made in 2000. It was approved and reviewed by the Ethics Committee of The First People’s Hospital of Lianyungang (Ethics number: KY-20221130001-01).
Author Contributions
Jin Wang contributed to paper design, managed data collection, analysis and compilation, drafted and revised key content; Na Lv handled data work, helped draft and significantly revised; Fengqin Xu oversaw the whole process, guided research design and paper drafting, ensured contributions met standards; Ling Yang helped collected data, drafted initial paper sections related to data work; Yuting Zhu involved in data collection, helped with paper revision. All authors approved the manuscript final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Aging Health Research Project of Lianyungang (L202207) and the Key Projects of the Scientific Research Topics Approved by Lianyungang Nursing Association (LHX-Z-202305).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.