
Abstract
Learning disabilities (LD) present substantial challenges for both affected individuals and society, often going under-recognized, leading to delays in diagnosis and inadequate interventions. These conditions are complex and caused by a mix of genetics, environment, and brain function. This can affect the sensory and mental information during processing, making learning more difficult. A systematic review of 19 selected studies was conducted using databases such as PubMed, Embase, Cochrane Library, and Web of Science. Studies were evaluated for risk of bias, and findings were synthesized to offer an integrated understanding of the etiology, pathophysiology, diagnostic complexities, and treatment strategies associated with LD. Key genetic and environmental risk factors were identified, and diagnostic challenges were explored, with an emphasis on the role of neurocognitive assessments and educational tools for accurate identification. The effectiveness of different treatments, such as educational programs, cognitive therapy, and novel technologies, was also assessed in terms of how well they help improve learning outcomes. The information processing theory was examined in depth, illustrating how disruptions in the processing of sensory and cognitive stimuli contribute to the learning difficulties observed in LD. The review also emphasizes the need for a team effort, bringing together parents, teachers, healthcare workers, and communities. This might provide vital support for people with LD. Advances in educational technology and cognitive training offer promising avenues for improving information processing and, consequently, educational outcomes. A holistic approach to diagnosis and intervention is essential for optimizing the quality of life and educational success of individuals with LD.
Plain language summary
Learning disabilities (LD) are conditions that make it harder for some people to learn, remember, or understand things the same way as others. These challenges affect not just the person but also their families and communities. Sadly, LD often goes unnoticed, so many people don’t get the help they need early in life. LD can happen because of a mix of reasons, like genetics (what we get from our parents), the environment we live in, and how the brain works. To learn more about LD, researchers looked at 19 reliable studies. They found that LD is linked to how the brain takes in and understands information, which makes learning harder for those affected. Diagnosing LD isn’t always easy, but tools like brain tests and school assessments can help spot it earlier. The good news is that there are ways to support people with LD. These include special teaching styles, brain training exercises, and new learning tools. One important idea the review highlighted is called the “information processing theory.” It explains how the brain handles information. When this process doesn’t work well, learning becomes more difficult. But new technologies and brain training methods are helping people with LD learn better. In short, the review shows that with the right support from parents, teachers, doctors, and the community, people with LD can do better in school and have brighter futures.
Introduction
Disability has evolved through various phases of development, but a universally accepted definition has yet to be established. Before Samuel Alexander Kirk’s contributions to shaping the concept of disability, it was referred to by several different terms, such as minimal brain damage, brain dysfunction, and perceptual disorders (Carman & Lim, 2025). The concept of disability, particularly in the context of learning disabilities (LD), has been loaded with controversy, especially due to the lack of a globally accepted definition. Conceptually, learning disability is understood as a broad term that refers to a diverse group of disorders. It is marked by significant difficulties in acquiring and using skills such as listening, speaking, reading, writing, reasoning, or mathematical abilities (Stamp et al., 2025). These difficulties are inherent to the individual and are thought to stem from dysfunctions in the central nervous system (CNS), with effects that may persist throughout a person’s life (Fletcher & Miciak, 2024).
While this definition seems universally accepted, it contains complexities that are often challenging to understand, especially from a layman’s perspective. Issues such as how to measure “significant difficulties,” the presumed link to CNS dysfunction, and terms like “heterogeneity,”“intrinsic,” and “concomitant occurrence” contribute to confusion in understanding LD (Goodley, 2023). The uniqueness of this disability arises from its diversity, the significant nature of the difficulties, the inherent causes within the individual, the frequent co-occurrence with other disabilities, and the exclusion of external influences. To help clarify these challenges, different models, such as the element model, have been proposed to simplify the understanding of LD (Tzortsou, 2023).
Learning disability, as a special needs condition, has been around for as long as humans have been learning. The historical teaching methods rooted in cultural heritage and gender-based roles are believed to be associated with LD (King et al., 2023). While it was not initially recognized as a disability, there were individuals in traditional societies who faced difficulties learning, following instructions. Besides this, recognizing objects, counting, differentiating sounds, interpreting cultural symbols, or understanding rhythms from traditional drumming patterns used in various social contexts are linked to LD (Stone et al., 2023).
Unlike other disabilities, LD is primarily associated with learning and education, which implicates the brain and CNS. As emphasized by the National Joint Committee on LD (NJCLD), LD is believed to result from dysfunctions in the CNS (Griffiths, 2024). Given that learning is fundamentally a cognitive process, any disruption in brain function can damage this process. This is observed in hemispheric lateralization, the idea that different parts of the brain handle different tasks. For example, the left hemisphere is mainly responsible for language-related skills like reading (Lage et al., 2024). If the area of the brain responsible for a particular task is dysfunctional, it can affect the person’s ability to perform that task. Studies have confirmed that hemispheric lateralization plays a critical role in the learning process of children with LD (Savegnago et al., 2024).
The nature of LD is heterogeneous and often accompanies other disorders. This means that individuals with LD can experience a range of symptoms, including perseveration, perceptual difficulties, and problems with visual, auditory, and kinesthetic discrimination (learning through physical movements). Other symptoms include organizational issues, distractibility, cognitive disorders, motor deficits, and figure-ground disorders (Kendeou & Johnson, 2024). People with LD often experience significant difficulties in different academic areas, including writing, solving mathematical problems, reading comprehension, and reasoning skills (Savegnago et al., 2024). These challenges are illustrated in Figure 1.

Important symptoms of learning disabilities.
Brain imaging has shown that problems in the central nervous system can disrupt how neurotransmitters work, affecting how the brain processes and understands information. This disruption can lead to perceptual difficulties, such as a child confusing letters like “p” and “b,” or numbers like “6” and “9.” How can such a child learn to spell words when letters are perceived incorrectly? Problems with discrimination skills can make learning even more challenging. Research suggested that around 80% of children with these difficulties experience major problems in school (Granato et al., 2024).
Recent advancements in research have proposed various theories explaining the multiple risk factors associated with LD (Liu et al., 2024). Furthermore, researchers have identified different markers for diagnosing the disorder (Ciulkinyte et al., 2025). While progress has been made in the classification, etiology, diagnosis, and treatment of LD, much of the information is scattered across various sources. This study systematically reviews 19 recent articles on diagnosing, classifying, and treating learning disabilities, aiming to aid early detection and targeted interventions for improved quality of life among affected individuals, caregivers, and professionals.
Methods
This review followed PRISMA guidelines and Elsman et al. (2024) procedures to ensure a transparent, rigorous, and credible approach to identifying, selecting, and synthesizing relevant studies. The PEOS framework used for this review is outlined below:
Literature Search Method
The search strategy for this systematic review was meticulously designed to ensure transparency and accuracy in identifying relevant literature. It included a combination of Medical Subject Headings (MeSH) and free-text keywords, enabling a comprehensive search that captured both standardized terminology and variations in how concepts are described in the literature. Boolean operators were strategically utilized to enhance both the sensitivity (maximizing the number of relevant studies retrieved) and specificity (minimizing irrelevant results) of the search process. In particular, the Boolean operator “AND” was employed to link core concepts, ensuring that retrieved articles addressed all aspects of the research question.
To enhance the scope and depth of the literature review, a comprehensive electronic search was performed across multiple major databases, including BIOSIS, Embase, the Cochrane Library, ProQuest, SCOPUS, Web of Science, and PubMed. This elaborate database selection assisted to capture a wide range of peer-reviewed articles reported in the literature. The search was performed over a five-month period, from August to December 2024. The primary focus of the search was on studies associated with LD, drawing upon foundational and recent works in the field, as referenced by Fletcher and Miciak (2024), Savegnago et al. (2024), and Olusanya et al. (2023).
Study Selection
Each author independently reviewed literature on LD etiology, pathophysiology, diagnostics, and treatment to ensure a balanced appraisal. Study selection occurred in two stages: title/abstract screening, followed by full-text review. Discrepancies were resolved collaboratively or with expert input, per Bucaille et al. (2022), to minimize bias and enhance reliability.
Eligibility Criteria
To ensure the relevance and quality of the evidence included in this systematic review, a set of predefined inclusion and exclusion criteria was applied. The inclusion criteria were as follows:
Language and Consent: Only articles written in the English language were considered, and all selected studies involved populations that had been formally diagnosed with LD and had ethically approved informed consent for participation.
Study Design and Time Frame: The review was restricted to cross-sectional studies published between 2021 and 2024 to ensure contemporary relevance and methodological consistency.
Focus of Research: Selected studies specifically addressed the classification of LD and the diagnosis of its symptoms, offering insights into the clinical identification and categorization of the disease.
Etiology and Treatment: Research that examined the underlying causes (etiology) of LD and proposed or evaluated treatment options was prioritized.
Data Quality and Source: Only articles published in indexed, peer-reviewed journals that presented comprehensive statistical analyses, including measures of significance, were selected to maintain the scientific rigor of the review.
Studies were omitted if they did not meet these eligibility criteria. Additional exclusion factors included the availability of duplicate publications, overlapping datasets that could compromise data integrity, and studies with non-extractable or incomplete data. These exclusion parameters were aligned with established best practices for systematic reviews, as described by Mikola et al. (2023).
Data Extraction Protocol
Data were extracted from each study using a standardized data extraction form to ensure consistency. The extracted data included the following:
Basic study details (author names, year of publication, study location)
Study design and methodology (including patient diagnosis)
Outcome measures (safety, prognosis, and symptomatic improvement)
Key findings and conclusions.
Bias Assessment
To ascertain the quality and reliability of the included studies, a formal bias assessment was performed using the Revised Cochrane Risk-of-Bias tool for Randomized Trials (RoB 2.0), as described by Xie et al. (2022). This widely applicable instrument offers a standardized and systematic approach for assessing potential bias across several key domains, including the randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of the reported result. By applying RoB 2.0, the review aimed to ascertain a thorough and objective appraisal of the internal validity of each study. This rigorous evaluation protocol contributed to a more nuanced interpretation of the findings, strengthening the credibility and transparency of the systematic review.
Quality Assessment
To assess cross-sectional studies, the Newcastle-Ottawa Scale (NOS) was applied per Chen et al. (2022), evaluating selection, comparability, and outcome assessment. Reviewers conducted blinded, independent evaluations; disagreements were resolved through discussion or expert consultation. Of 431 retrieved articles, 125 unique ones were screened. After excluding 62 articles for missing key information or statistical inconsistencies, 19 met all eligibility criteria and were included (see Figure 2).

PRISMA flow diagram to select scientific studies from the literature.
Ethical Considerations
The objective of this study was to systematically compile and present information from publicly available sources to benefit the scientific community and promote further research in the emerging field of LD. Ethical guidelines and procedures, as outlined in the literature, were followed during the data collection process (Gliniecka, 2023). Data were obtained from public domains, including official websites and peer-reviewed publications. Efforts were made to ensure the privacy of individuals and organizations involved in the research.
Only open, reusable, and redistributable data were used, with no restrictions on their use. Data that were incomplete, controversial, or lacked ethical clearance were excluded. Additionally, research employing improper statistical methodologies or biased approaches was not included. All sources used in the data collection process were properly cited.
Data Representation
The collected data were organized in an Excel sheet, analyzed, and represented in either tabular or graphical form for clarity. Key information is presented in the following figures and tables: Table 1: Major classes of LD; Figure 1: Important symptoms of LD; Figure 2: PRISMA flow chart; Figure 3: Possible risk factors for LD; Figure 4: Etiological models of LD; Figure 5: Highlights of information processing theory linked to LD; Figure 6: Common forms of LD; Figure 7: Challenges in handling children with LD; Figure 8: Standardized protocol for teaching children with LD; Figure 9: Recommendations for managing children with LD
Major Classes of Learning Disabilities.


Possible risk factors for learning disabilities.

Important etiological models of learning disabilities.

Important highlights of information processing theory linked to learning disability.
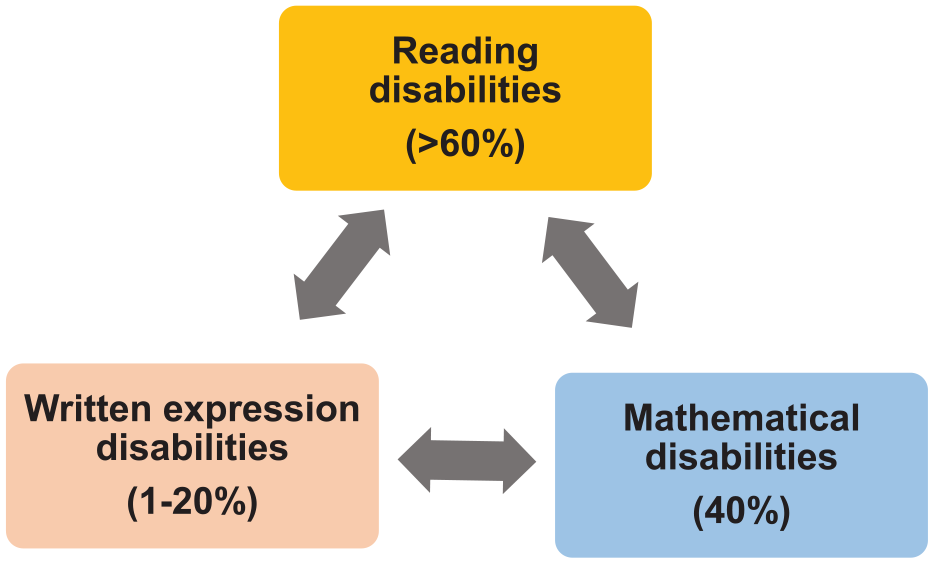
Common forms of learning disabilities with percentage.

Challenges in handling children with learning disabilities.

Standardized protocol for teaching children with learning disabilities.

Recommendations for managing children with learning disabilities.
Learning Disabilities
Learning disabilities (LD) are neurobiological disorders that primarily affect children’s ability to acquire academic skills. Understanding LD is essential for providing effective interventions and support in both diagnostic and educational settings. Teachers, caregivers, and other professionals requires a strong understanding of LD, including their signs, characteristics, types, and symptoms (Granato et al., 2024). Despite the numerous attempts to define LD, over 40 definitions have been proposed, but none have achieved universal consensus. Various models, such as the definitive approach, the descriptive approach, and the discrepancy model, have been suggested to explain the disorder (Sarid et al., 2024).
Nature of LD
LD is a neurobiological disorder that disrupts the brain’s ability to coordinate and process information, which in turn affects a child’s ability to learn fundamental academic skills. Samuel Alexander Kirk defines LD as delays or disorders in domains like speech, language, reading, writing, and math, caused by brain dysfunction rather than intellectual disabilities or cultural factors (Tien et al., 2024). According to the American Psychological Association (APA) in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), LD is categorized as a Neurodevelopmental Disorder. This disorder impedes the ability to learn specific academic skills such as reading, writing, and arithmetic. These difficulties are considered “unexpected,” as other developmental areas are typically unaffected (Leroy et al., 2024).
Early signs of LD may emerge as early as preschool when children struggle with basic skills such as recognizing letters or counting. However, a formal diagnosis is typically made once the child begins school (Savegnago et al., 2024). Importantly, LD is often a lifelong condition, particularly specific LD (SLD), which may persist into adulthood. Additionally, learning disabilities can show up vividly depending on the language and cultural context, shaped by different education systems and cultural influences (Song et al., 2024).
People suffering from LD exhibit some of the following conditions (Rana et al., 2025);
Heterogeneity of LD
LD is not a single condition but a heterogeneous disorder, meaning it presents in various forms and can affect different academic areas (Ciulkinyte et al., 2025; Shukla, 2024). Therefore, definitions of LD must consider several key parameters:
There are several LDs, each impacting different aspects of learning. The most common include:
Heterogenicity of data is important for the following reasons (Bildiren et al., 2025);
Conceptualization of LD
The National Joint Committee on LD (NJCLD) defines LD as a significant discrepancy between a child’s potential to learn and their actual level of achievement. Children with LD often demonstrate various characteristics (Fathi Azar et al., 2024), including:
Hyperactivity and impulsivity
Perceptual-motor impairments
Memory and cognitive challenges
Emotional instability
Academic difficulties
Coordination issues
Language deficits
Attention disorders
Neurological signs that may be unclear or inconsistent
While LD primarily impacts academic learning, it can manifest in a range of developmental and cognitive issues. These issues can slow a child’s learning at school, so identifying them early is essential to offer timely support tailored to the child’s needs (Ocklenburg et al., 2024).
LD are complex, multi-dimensional conditions that require a thorough understanding of their various manifestations, characteristics, and types. Although no single definition has been universally accepted, the importance of early detection and intervention cannot be overstated. Educators, parents, and healthcare professionals need to work together to support children with LD by using diagnostic tools, personalized education plans, and tailored teaching methods to help them succeed (Kuriakose & Amaresha, 2024).
Recent conceptual themes of LD (Liu et al., 2025) are;
Important issues identified in conceptualization of LD (Strübbe et al., 2025):
Prevalence of Learning Disabilities
LD is not a single, uniform condition; rather, it encompasses a range of difficulties in processing information that can affect learning in different ways. As a result, children and adults with LD may experience multiple challenges, referred to as comorbidity (Semchishen & Colman, 2025). For example, one child might have difficulties with reading and spelling, another may be better at reading but struggle with math, and a different child might find it hard to understand spoken language or express their thoughts clearly. Though the manifestations of LD differ, they all share a common thread of learning difficulties (Yan et al., 2024).
Research indicates that the lifetime prevalence of specific learning disorders among children aged 3–17 years is 9.7%. Among children with special health care needs, the prevalence is significantly higher, at 28%, compared to 5.4% in typically developing children. Reading disorders alone account for 80%–90% of all LD (Li et al., 2023). In the United States, for example, the Centers for Disease Control and Prevention (CDC) reports that about 1 in 5 children has a learning or attention problems such as dyslexia, dyscalculia, or ADHD, though not all qualify as LD under educational law (Müller-Axt et al., 2025). Studies have shown that the prevalence of specific learning disorders in primary school-aged children is around 15%. Within this group, dysgraphia affects 12.5%, dyslexia 11.2%, and dyscalculia 10.5%. Additionally, 7% of children were found to have all three types of LD (Li et al., 2023).
LD commonly happens alongside other conditions like ADHD, anxiety, and motor skill disorders. The most common co-occurring condition is ADHD, with an estimated 33% of children with LD also being diagnosed with ADHD. Anxiety disorders are present in about 28.8%, mood disorders in 9.4%, and language disorders in 11% of children with LD (Cristofani et al., 2023).
LD as a Neurodevelopmental Disorder
LD is considered a neurodevelopmental disorder, meaning it typically appears early in childhood before school entry and leads to difficulties in social, academic, and/or occupational functioning. These disorders are marked by dysfunctions in various cognitive areas, including attention, memory, perception, language, problem-solving, and social interaction. Other neurodevelopmental disorders include ADHD, autism spectrum disorder (ASD), and intellectual disabilities (Katyal et al., 2024).
Neurobiological evidence suggested that individuals with LD often show structural and functional differences in specific brain regions responsible for language processing, memory, and executive functions. Genetic factors, prenatal influences, and early childhood brain injuries can result in these developmental differences (Gentry et al., 2025). As neurodevelopmental conditions, LDs are not the consequence of low intelligence, lack of motivation, or inadequate instruction, but rather stem from inherent neurological variations that impact how the brain processes information (Katyal et al., 2024).
Several risk factors are associated with LD, and some are considered primary causes of the disorder. Among the most significant are genetic factors and birth defects. Additionally, substance abuse and exposure to environmental toxins may contribute to the development of LD. Head injuries and diseases of the central nervous system (CNS), including infections, are also known to play a role. Furthermore, complications during pregnancy can increase the risk of LD (Ciulkinyte et al., 2025; Katyal et al., 2024), as illustrated in Figure 3.
Unlike other neurodevelopmental disorders, children with LD have average or above-average intelligence. Their learning difficulties are specific to acquiring, organizing, retaining, comprehending, or using verbal and non-verbal information. This sets LD apart from other cognitive or developmental disorders, which may be more generalized (Ciulkinyte et al., 2025).
Etiology
The exact cause of learning disabilities (LD) remains not fully understood, but research strongly suggests a neurobiological origin. LDs are believed to result from abnormalities in brain structure or functioning that interfere with the acquisition and use of academic skills. Both genetic and environmental factors are implicated in their development. For instance, children with a family history of LD have an increased likelihood of developing similar challenges (Granato et al., 2024). Specific genetic components, such as mutations in the CDK13 gene, have also been associated with LD. Furthermore, maternal education has been identified as a contributing factor—children born to mothers with less than 12 years of schooling are at a greater risk of developing LD (Bourgois et al., 2024).
Traumatic brain injuries may also precipitate the onset of LD later in life. Overall, the development of LD is shaped by an interplay of genetic, environmental, and neurobiological contributors (Buchfellner & Ross, 2024). Several etiological models attempt to explain the underlying mechanisms of LD, each offering a different perspective and informing tailored diagnostic and therapeutic approaches (Bourgois et al., 2024; Buchfellner & Ross, 2024; Li et al., 2023). These models are summarized in Figure 4.
According to Strock et al. (2025), understanding LD requires a multifactorial approach that integrates various etiological perspectives. Emerging research (Eroğlu et al., 2025; Chong, 2025) highlights the following key domains:
LDs are linked to atypical brain structure and function. Functional imaging studies (e.g., fMRI, PET) have identified altered activation in brain regions critical for reading, math, and writing, for instance, the left temporo-parietal region in individuals with dyslexia.
LDs often run in families. Twin studies show a high heritability rate, particularly for dyslexia. Although no single gene causes LD, several—such as DYX1C1 and KIAA0319—have been implicated, pointing to a polygenic influence.
Risks include premature birth, low birth weight, prenatal substance exposure, birth trauma, and hypoxia—all of which may affect brain development.
Early childhood deprivation, toxic exposures (e.g., lead), and malnutrition may increase LD risk or affect symptom expression.
While not causal, emotional trauma or chronic stress can co-occur with LD and exacerbate coping difficulties. Children with undiagnosed LD often experience frustration, leading to secondary mental health concerns.
Pathophysiology
Neurophysiological and neuroanatomical studies on the brains of individuals with dyslexia have revealed structural abnormalities, particularly in the left cerebral cortex. Similar to other neurodevelopmental disorders, such as obsessive-compulsive disorder, schizophrenia, attention-deficit/hyperactivity disorder (ADHD), and Tourette syndrome, a dysfunction of the corticosteroid system has been proposed as a contributing factor in the pathogenesis of LD (Ciulkinyte et al., 2025; Odegard et al., 2024).
Information Processing Theory
The information processing theory, developed by cognitive psychologists, seeks to explain how individuals process information. This theory focuses on how humans receive, interpret, and transform stimuli from their environment into meaningful responses. George Armitage Miller was among the first to introduce the concept of information processing, which was later developed further by John William Atkinson and Richard Shiffrin (Decarli et al., 2023). Their research aimed to elucidate the cognitive mechanisms of the brain and its functions for learning. They proposed that these processes are relatively simple, but the complex and vast network of neural connections can cause significant learning disruptions if any part of the system fails (Savegnago et al., 2024).
According to this theory, the process begins with the brain receiving external stimuli through the senses. The brain then processes and stores this information in memory, from where it can be retrieved when needed. The brain is often compared to a computer that takes in, processes, stores, and retrieves information when required. This comparison helps describe how learning happens (Decarli et al., 2023).
The theory suggests four stages of information processing: sensory memory, short-term memory (or working memory), long-term memory, and processing, which are further described by four levels: acquisition, storage, transformation, and transmission. These stages are interconnected, and any disruption at one stage can impair the overall learning process (Xie et al., 2022). The four stages are explained below:
Information processing depends on various strategies that are systematically arranged, integrated, and adapted to support effective occupational performance. The effectiveness of this process depends on adopting the most suitable strategies that enable efficient handling of information (Bucaille et al., 2025). Cognitive strategies refer to methods of thinking and the ability to process thoughts in a purposeful, goal-oriented fashion. Using cognitive strategies means effectively applying known techniques in real-time situations, selecting and implementing the most appropriate strategy to meet the requirements of a specific context (Alsaadi et al., 2025).
One method used to augment these capabilities is cognitive strategy training. This approach aims to assist individuals in acquiring and implementing effective strategies to process information more efficiently, thereby improving academic or functional performance. In addition to cognitive strategy training, the systematic instruction method can also assist in developing occupational functioning by targeting the improvement of specific task-related skills (Jain et al., 2024).
Systematic instruction is a method commonly associated with functional or behavioral task approaches. It follows a top-down model similar to strategy training and includes structured interventions such as task assessment, cueing, prompting, chaining, and guided support (Gallego-Molina et al., 2024). These methodologies align with learning theory frameworks that stress skill acquisition. The core objective is to enable learners to perform tasks step-by-step, thereby promoting mastery of essential skills within a therapeutic setting (Kuriakose & Amaresha, 2024).
Damage to the left hemisphere of the brain can result in language deficits, while damage to the right hemisphere can impair emotional expression and discourse understanding. Those with right hemisphere damage may struggle to make inferences, understand main concepts, or process alternative meanings (Remaud et al., 2024). Information processing theory is closely associated with LD. A key aspect of this theory is the central role of cognitive skills in learning. According to the theory, dysfunction at any stage of the information processing sequence, whether it be input, integration, storage, or output, can hinder the learning process. Notably, interventions aimed at improving or correcting deficits in information processing mechanisms have exhibited promising results in reducing the symptoms of LD (Remaud et al., 2024), as illustrated in figure 5.
The hidden nature of LD, coupled with the lack of visible signs or sensory evidence, makes it difficult to identify and address, unless accompanied by other conditions. This frequently causes misunderstandings about LD, even though it affects a child’s ability to learn important academic subjects and life skills. These challenges impact not only the children but also their parents, teachers, and society as a whole (Ahn and Park, 2025). Parents may struggle to understand why their children face learning difficulties, while educators strive to provide effective learning strategies. Meanwhile, the public often fails to recognize the realities of the disability, and governments face the responsibility of creating inclusive learning environments (Gabay et al., 2024).
Researchers have focused a lot on the challenges children with LD face in learning and expressing knowledge, even in subjects they have already mastered. These challenges have been explored from three perspectives: the disability-based perspective, the individual profile perspective, and the general perspective. LD is a condition that affects individuals across all demographics, regardless of gender, race, age, socioeconomic status, or religious background, and it is prevalent in many schools and communities (Kuriakose & Amaresha, 2024). Given the complexity of this disability, it is essential to continue simplifying its understanding through theories like the information processing theory, which attempts to explain how the brain processes stimuli during learning activities (Santoni et al., 2024).
Impact of Brain Damage on Learning and Behavior
Damage to different areas of the brain can impact learning in various ways. For example, damage to the left hemisphere typically affects language processing, while damage to the right hemisphere can impair emotional tone in speech, understanding discourse, and the ability to make inferences. This shows how complex brain processing is and explains why children with LD can have a variety of learning challenges (Alexander et al., 2022).
LDs are complex and multifaceted, affecting individuals in different ways. The prevalence of LD is significant, with many children facing challenges in various academic areas, such as reading, writing, and mathematics. Learning disability is a neurodevelopmental defect caused by a mix of genetic, environmental, and neurobiological factors (Kalmar et al., 2022). The information processing theory offers valuable insight into how LD affects children, focusing on how information is received, processed, and used. Understanding these factors is essential for developing effective interventions and support systems to help children with LD succeed academically and beyond (Ayar et al., 2022).
According to recent discoveries, the following are the major types of brain damage that affect learning abilities (Kantathanawat et al., 2025; Martin et al., 2025)
● Causes: Lack of oxygen (hypoxia), traumatic birth, neonatal stroke, infection (e.g., meningitis) ● Impact: May result in LD-like deficits in language, attention, memory, or executive functioning.
● Injury post-birth, typically due to accidents or falls. ● Can cause acquired learning disabilities, including: ○ Problems with attention and memory ○ Slowed processing speed ○ Difficulties in reading, writing, or math
● Damage to specific brain areas can result in targeted learning problems: ○ Left hemisphere (language areas) → dyslexia-like symptoms ○ Right parietal lobe → difficulties in visual-spatial tasks or dyscalculia-like symptoms ○ Frontal lobe → executive dysfunction affecting organization, planning, and behavior
● Conditions like cerebral palsy, epilepsy, or hydrocephalus can lead to secondary learning disabilities depending on the extent and location of brain involvement.
Classification of LD
LD can be classified based on two primary factors (Aro et al., 2022):
The important categories of LD can be classified based on stages of information processing and the associated functional impairments. For instance, a deficit in the input stage of information processing is commonly linked to dyslexia. Similarly, impairments in the integration stage may contribute to conditions such as dysgraphia. Deficits in the storage stage can lead to disorders like auditory-visual processing impairments, nonverbal learning disabilities, dyspraxia, and dysphasia (Aro et al., 2022; Bruefach & Reynolds, 2022). These associations are summarized in Table 1.
Common Forms of LD
LD encompasses a variety of challenges in acquiring specific academic skills. The most common types of LD are difficulties with reading, math, and writing. These types differ in their manifestations and the specific areas of learning they affect. People with LD most commonly exhibit difficulties in reading (60%), followed by challenges in mathematical problem-solving (40%) and writing (ranging from 1% to 20%) (Aro et al., 2022), as illustrated in figure 6.
a. Reading Disabilities
Reading disabilities, particularly dyslexia, are the most prevalent type of learning disability. Dyslexia is characterized by difficulties in recognizing words accurately and fluently, despite having normal or even above-average comprehension abilities. People with dyslexia usually have issues with phonological awareness, the skill to recognize that speech can be split into smaller sounds like words, syllables, and phonemes. This might lead to difficulties recognizing words (Fumero et al., 2022).
In contrast, students with specific comprehension deficits do not have trouble recognizing words, but they struggle with understanding the meaning of what they read. These difficulties often stem from issues such as weak vocabulary knowledge, trouble processing grammar, or poor listening comprehension (Brueafach & Reynolds, 2022).
Some students may have both dyslexia and specific comprehension problems, which makes it difficult for them to recognize words and understand what they read. Prevalence estimates show that 5%–17% of the population has dyslexia, and 10%–15% of primary school-aged children experience specific reading comprehension deficits (Cristofani et al., 2023; Li et al., 2023).
Reading problems in LD typically involve impairments in one or more of the following areas (McLeod et al., 2025; Kim et al., 2025):
b. Mathematical Disabilities
Mathematical LD involves two primary areas: computations and problem solving.
c. Written Expression Disabilities
Writing disabilities make it cumbersome for people to express themselves clearly in writing. These students may have difficulties with various components of writing, such as handwriting, spelling, and composition (Ewoldt & Byme, 2023).
Students with written expression disabilities may find it particularly challenging to complete written tasks in an organized, clear, and accurate manner (Re et al., 2023).
Diagnostic Evaluation of LD
The diagnostic process for identifying LD typically requires a multidisciplinary team approach and involves several stages of evaluation (Aldharman et al., 2023; Fletcher & Miciak, 2024; Semchishen & Colman, 2025; Tv et al., 2025):
● Woodcock-Johnson-III ● Wide range achievement test
● Adaptive behavior assessment system-III ● Vineland adaptive behavior scale-II
● Conners rating scale ● ADHD rating scale-III ● NICHQ Vanderbilt percent and teacher scale
● Wechsler Intelligent scales for children
● Achenbach child behavior checklist
● Clinical evaluation of language fundamentals
● Beery test of integration
The Response to Intervention (RTI) model is a growing substitute to traditional methods for diagnosing LD. It focuses on how a child responds to a particular teaching strategies and support. It starts with a standard instruction that targets the child’s specific areas of difficulty. If the child continues to struggle despite interventions, further assessments are conducted to determine whether a learning disability is present. This method can help differentiate between LD and performance issues caused by lack of instructions (Gilmour et al., 2024).
Diagnosing LD includes a thorough, team-based approach. It's vital to understand the different types. Some of them include reading problems like dyslexia, problems with math, and challenges in writing, to offer the right support and interventions. Formal evaluations, which include cognitive, academic, and behavioral assessments, are necessary to accurately identify and measure the extent of the disability. By recognizing LD early and implementing appropriate interventions, children can receive the support they need to succeed academically and in life (Gilmour et al., 2024; Ramos-Carrillo & Moreno-Perez, 2023).
Trends in the diagnosis of LD (Devitt et al., 2025; Fathi et al., 2025; Musumeci et al., 2025
● EEG-based biomarkers: Researchers are using EEG rhythms and machine learning to find neural markers of learning disorders, showing early promise for accurate, non-invasive detection of related brain patterns ● MRI and functional imaging: These tools reveal unique brain patterns in dyslexia, dyscalculia, and other LDs, assist early detection and subtype differentiation.
● Mobile and desktop AI screening apps: Pattern recognition tools recognizing handwriting and speech can screen for dyslexia, dysgraphia, dyscalculia, and ADHD with ∼90% balanced accuracy. ● Deep learning on handwriting samples: Custom CNNs detect dysgraphic handwriting with ∼91.8% accuracy. ● Generative Adversarial Networks + transfer learning: A novel framework in Al Kharj, Saudi Arabia, uses SRGANs and transfer learning to analyze handwriting for dyslexia screening, achieving ∼92.5% accuracy. ● AI analyzing VR task performance: VR tasks combined with AI predicted support essential in university students with dyslexia with ∼90% accuracy.
● Comprehensive apps now screen for multiple LDs together with promising pilot data showing accurate detection and notable student improvement.
● Provisional diagnoses post-COVID: Amid pandemic learning losses, experts advocate flexible criteria utilizing clinical history, provisional IDs, and prioritizing assessments to flag at-risk students early.
Identification of LD in students
Learning disabilities (LD) are typically identified through models focusing on discrepancies in academic performance or responses to interventions. Two key methods are the IQ-Achievement Discrepancy and Response to Intervention (RTI) models.
a. IQ-Achievement Discrepancy
Traditionally, LD identification relied on the gap between a student’s intellectual potential (IQ) and academic achievement. For instance, a student with an average IQ (e.g., 100) but significantly low academic scores (e.g., 70 in reading) may be diagnosed with LD (Alabbad et al., 2023). However, a student with low IQ and below-average achievement (e.g., IQ 85, math 80) wouldn’t qualify due to lack of discrepancy (Granato et al., 2024).
This model is often criticized as a “wait-to-fail” approach, as it delays diagnosis until a substantial gap emerges and overlooks the quality of instruction received. Consequently, some students may be misidentified, delaying timely support (Kuriakose & Amaresha, 2024).
b. Response to Intervention (RTI)
RTI addresses these limitations through a proactive, three-tiered system emphasizing early detection and tailored interventions (Gilmour et al., 2024):
Tier 1: High-quality, evidence-based instruction for all students, with regular progress monitoring. About 20%–30% not progressing advance to Tier 2.
Tier 2: Targeted small-group interventions led by specialists, with frequent progress checks. Students who improve may return to Tier 1; others proceed to Tier 3.
Tier 3: Intensive, individualized support often one-on-one, leading to LD identification and possible special education eligibility. RTI provides early, customized support, preventing students from falling behind (Ramos-Carrillo, 2023; Horridge et al., 2023).
c. Characteristics of Students with LD
Students with LD often have average or above-average intelligence but show specific cognitive deficits affecting learning (Mattison et al., 2023; Nehra et al., 2024; Kang et al., 2023):
Attention difficulties, often co-occurring with ADHD, impair focus and increase distractibility.
Memory weaknesses impact working and long-term memory, affecting tasks like instruction recall.
Slower information processing delays task completion and understanding of complex instructions.
Metacognitive challenges hinder self-monitoring and applying prior knowledge to new learning.
Low self-esteem and motivation arise from repeated failures, often worsening social skills.
Nature and Challenges of LD
The nature of LD is complex and involves both cognitive and environmental factors. It's essential to understand that LD are often hidden and don’t show obvious signs like blindness or deafness. This can make it challenging to diagnose and support students with LD. Identifying and supporting people with learning disabilities (LD) presents several challenges. Important issues include negative attitudes, an unsupportive learning environment, a lack of adequately trained staff, insufficient attention to individual needs, prevailing myths about the disorder, and usual cases of improper diagnosis (Bölte et al., 2023; Briggs et al., 2023; Khademi et al., 2023), as shown in figure 7.
The identification and support of LD are critical to providing students with the tools they need to succeed academically. However, the hidden nature of LD and the various cognitive challenges it involves make it difficult to accurately identify and support students. By improving diagnostic models, increasing public awareness, and ensuring better training and resources for educators, we can better support students with LD and help them achieve their full potential (Briggs et al., 2023).
Co-morbidities Associated with LD
a. Cognitive Problems
Children with LD often face significant challenges in acquiring academic skills despite average or above-average intelligence. These difficulties extend beyond academics into everyday functioning. While poor teaching or limited training can impact progress, research shows these are not primary causes of LD (Abd-Alrazaq et al., 2023). Instead, LD involves neurological disorders affecting the brain’s ability to receive, process, store, and respond to information, impacting key psychological processes:
Input: Receiving and interpreting information,
Memory: Storing and retrieving information,
Integration/Association: Combining and expanding information,
Output: Using information meaningfully (Gabay et al., 2023). Deficits in these processes explain the academic struggles seen in children with LD (Abd-Alrazaq et al., 2023).
b. Person-Centered Related Factors
LD often brings psychological challenges. For instance, dysgraphia can cause frustration and low confidence, potentially leading to school phobia and avoidance of writing tasks (Martin-Ruiz et al., 2023). Past failures may lead to a pessimistic outlook, learned helplessness, low stress tolerance, and emotional withdrawal, making school engagement difficult (Tv et al., 2025).
c. Behavioral Issues
LD affects not only academics but also social relationships and self-esteem. Children may misinterpret social cues and display behavioral problems such as:
Externalizing behaviors: Aggression, impulsivity, poor judgment,
Internalizing behaviors: Anxiety, withdrawal, depression (Harper et al., 2023).
Such behaviors can lead to peer rejection, risky conduct, and substance use (Peter et al., 2023). Approximately 30%–50% of children with LD exhibit behaviors interfering with learning and socialization. Repeated failure lowers self-worth and motivation, emphasizing the need for comprehensive support from families, schools, and communities (Thapliyal & Ahuja, 2023).
Summary of Key Co-morbidities (Polydoros & Antoniou, 2025; Shelton et al., 2025):
ADHD: Most common, 25%–60% prevalence in LD,
Anxiety disorders: 21%–30%, including school phobia,
Depressive disorders: 20%–28%,
Conduct disorder and oppositional defiant disorder: 20%–30%, often overlapping ADHD,
Language disorders and dysgraphia: 40%–70% in dyslexia,
Sensory processing and motor coordination issues (e.g., dyspraxia): 10%–15%,
Nonverbal learning disability: Overlaps with LD, ADHD, and Autism.
Treatment and Management of LD
1. Learning Strategies
Good teaching methods are vital for helping children with LD succeed, but true success comes when students learn, improve, and overcome challenges. Children with LD often struggle with cognitive and metacognitive skills needed to process, store, retrieve, and apply information, which hinders acquiring new concepts without appropriate learning strategies (Thériault et al., 2024).
Lev Vygotsky’s Zone of Proximal Development (ZPD) provides key insight into learning. It defines three zones: tasks a learner can do independently, tasks requiring assistance, and tasks beyond current ability. Misalignment between assigned tasks and a child’s ZPD can cause cognitive overload and frustration (Malapela & Thupayagale-Tshweneagea, 2024).
Despite these obstacles, LD does not mean failure. With proper support, therapeutic environments, and technology, children with LD can achieve success, as demonstrated by figures like Einstein and Edison (Esquivel et al., 2024).
2. Instructional Strategies
a. Explicit Instruction
Explicit instruction is a clear, structured teaching approach using simple language to foster effective teacher-student interaction (Bundock et al., 2024). It involves:
Focused lessons breaking complex skills into smaller parts,
Clear explanations of skills,
Teacher-led demonstrations (“I do”),
Guided practice with feedback (“We do”),
Independent practice with immediate feedback (“You do”).
This method helps students with LD by making learning steps manageable (Rao et al., 2024).
b. Strategy Instruction
Strategy instruction teaches specific methods to help students learn, work independently, and apply skills broadly. It includes:
Study skills like note-taking and summarizing,
Mnemonics for memory,
Content-specific strategies such as Self-Regulated Strategy Development (SRSD) for writing.
This is especially effective for students with LD who struggle to develop such strategies naturally (Brown & Marsh, 2024; Ryan et al., 2024).
c. Scaffolding Instruction
Scaffolding provides gradual, stepwise support that is slowly removed as learners gain independence (Mossige et al., 2023). It consists of:
Content scaffolding with accessible material,
Material scaffolding using prompts and cues,
Task scaffolding breaking tasks into smaller steps and modeling the process.
This approach builds confidence and independence in students with LD. The standardized protocol is shown in Figure 8 (Theriault et al., 2024; Malapela & Thupayagale-Tshweneagea, 2024; Esquivel et al., 2024; Bundock et al., 2024; Rao et al., 2024; Brown & Marsh, 2024; Ryan et al., 2024).
These strategies together create a comprehensive approach to supporting students with LD, helping them not only in academic tasks but also in developing the skills needed to thrive in different areas of life.
Emerging trends in the therapeutic interventions of LD (Bayram et al., 2025; Connors et al., 2025; Wang et al., 2025)
● AI Assistive Tools: Chatbots, word prediction, and text-to-speech tools are motivating supporting students with dyslexia and writing challenges, enhancing engagement and autonomy ● Digital Therapeutics for ADHD: The FDA-approved game app AKL-T01 (EndeavourRx) significantly enhances attention and inhibitory control in children and adults with ADHD. ● VR (virtual reality) + AI Screening and Support: VRAIlexia uses VR tasks and AI to examine dyslexia and tailor interventions with ∼90% predictive accuracy.
● Rhythmic Reading Training (RRT) : A music and rhythm program improves reading speed and working memory in kids with dyslexia after 20 sessions. ● Serious Games and VR Exposure: VR modules like oVRcome help decrease anxiety in medical settings for students with learning disabilities and autism. ● Serious Games for Literacy: Early data shows that gamified apps and video protocols result to meaningful reading gains.
● Transcranial Direct Current Stimulation (tDCS) : Used for dyscalculia, this stimulates the parietal lobe and augments numerical skills for up to 6 months post-treatment. ● Non-Invasive Brain Training: Neurofeedback devices and cognitive-enhancement wearables target executive function and attention in LDs but are effectively still in development.
● Equine-Assisted Therapy: Programs like Enabling Through the Horse in Namibia improve motor skills, coordination, and socio-emotional development in kids with LDs, ADHD, and neurodiversity.
● Adaptive Literacy and Math Apps: Tools like CogniFit’s AI dyslexia app (boosting reading accuracy ∼34%) and Meister Cody’s adaptive math game improve personalized interventions. ● Integrated Approaches for LD+ADHD: Combined interventions address shared cognitive deficits like working memory and verbal comprehension, mainly in comorbid cases. ● Remote Neuropsychodynamic Platforms: Tools like Tachidino enable active online dyslexia intervention across all ages and severity levels.
Future Implications, Recommendations and limitations
This review highlights the multifaceted impact of learning disabilities (LD) on children, beyond academics, affecting emotional well-being and social development (Saleh et al., 2024). To effectively support children with LD, several future directions and practical recommendations are proposed.
A. Early Identification and Intervention
Early recognition of LD is critical for improving academic and psychosocial outcomes. Timely interventions can reduce long-term effects and prevent emotional or behavioral issues stemming from frustration, low self-esteem, or isolation. Effective screening requires coordinated efforts among schools, parents, and healthcare providers (Aldharman et al., 2023; Han & Wang, 2023; Mather & Schneider, 2023; Semchishen & Colman, 2025; Tv et al., 2025).
B. Addressing Emotional and Behavioral Challenges
Children with LD often experience anxiety, depression, and social withdrawal due to fear of failure or rejection. This increases their risk of academic dropout and mental health issues. A holistic approach is necessary, including:
Psychological support: Counseling to build resilience and manage emotions.
Behavioral interventions: Programs to develop social skills and reduce aggression.
Early intervention can break the cycle of failure and promote emotional well-being (Abd-Alrazaq et al., 2023; Gabay et al., 2023).
C. Accurate Diagnosis and Avoiding Misidentification
Misidentifying LD as intellectual disability is a frequent issue due to limited awareness. Inaccurate diagnosis can lead to inappropriate interventions and hinder progress. Professional assessment is essential to differentiate LD from other conditions, ensuring children receive appropriate educational and psychological support (Aldharman et al., 2023; Ramos-Carrillo & Moreno-Perez, 2023).
D. Parent and Teacher Education and Collaboration
Effective management of LD requires informed and cooperative involvement from both educators and caregivers.
Teacher training: Educators should be equipped to identify LD, understand its impact, and apply tailored strategies, including addressing socio-emotional needs (Theriault et al., 2024).
Parent education: Families should be taught to recognize early signs and support learning at home in a positive environment.
Collaboration between teachers, parents, and mental health professionals is vital for building strong support systems that enhance both academic performance and social integration for children with LD (Bundock et al., 2024). Key recommendations are visually summarized in Figure 9.
Finally, the review emphasizes the importance of maintaining a positive attitude towards children with LD. Instead of viewing their struggles as a permanent limitation, it is essential to recognize their potential and provide ongoing support (Ryan et al., 2024). This includes:
The review shows that with effective help, support, and a positive attitude, children with LD can overcome difficulties, succeed in school, and enjoy a good quality of life (Mossige et al., 2023).
While this study utilized a scientifically recognized method for collecting data from different articles, it is essential to acknowledge several limitations. These include the probability of bias in how studies were chosen and how data were retrieved. Evaluating the quality of each study also poses challenges, as inconsistencies in design and reporting can make evaluation cumbersome. Furthermore, variations among the studies, such as differences in methods, populations, and outcomes, can complicate the analysis. The applicability of the assessment to broader contexts may also be limited. Therefore, the analysis and conclusions of this review are based solely on the data extracted from the included studies.
Emerging trends in the therapeutic interventions of LD (Bayram et al., 2025; Connors et al., 2025; Wang et al., 2025)
Learning disabilities are multi-factorial conditions that require precise, individualized treatment based on their underlying causes. Personalized approaches such as genetic and neurobiological profiling, together with machine learning techniques, can be utilized to develop customized learning paths. Targeted neurostimulation and cognitive training have shown promising effects in enhancing working memory. In some individuals, rhythm- and music-based interventions have improved phonological processing and memory retention.
Immersive learning environments and social recognition training have been effective in enhancing interpersonal skills among individuals with LD. Additionally, a focus on mental health and emotional resilience has proven beneficial in managing anxiety and depression. Parent training programs and peer-mediated interventions support learning at home and contribute to increased motivation and improved social skills, respectively.
Given the diverse clinical presentations of LD, various interventions should be initially trialed and then adjusted based on their effectiveness in alleviating specific symptoms.
Conclusion
Learning disabilities have existed for centuries, but their complex nature makes them difficult to fully understand. Learning disabilities primarily impact academic performance, even in children with above-average intelligence. The information processing theory indicates that learning disabilities may occur when there are problems with how information is received, processed, or shared. Cognitive psychologists emphasize that smooth information transfer is crucial for learning, and any disruption hampers this process. Recent advancements have significantly improved the early detection of LD, even during the initial stages of development. Specific learning disabilities are now better understood in terms of their underlying causes, associated risk factors, and affected brain areas. Emerging technologies such as neuroimaging, biomarker analysis, artificial intelligence (AI), and machine learning tools, as well as multifunctional mobile examinations, have transformed the diagnostic process for LD. Additionally, digitally powered therapeutics, technology-enhanced interventions, neurostimulation techniques, and personalized treatments targeting comorbid conditions have shown promising results in suppressing the symptoms of LD. To better support children with learning disabilities, it is important to disseminate recent research findings in the form of seminars, workshops as well as training programs to educators, healthcare professionals, and the general public, thereby promoting greater awareness and more effective intervention strategies.
Footnotes
Acknowledgements
The authors extend their appreciation to the King Salman Center for Disability Research for funding this work through Research Group no KSRG-2024-027.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors extend their appreciation to the King Salman Center for Disability Research for funding this work through Research Group no KSRG-2024-027.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data is within the article.