
Abstract
The COVID-19 pandemic has triggered many psychological concerns on nurses, such as anxiety and compassion fatigue. This study aimed to examine the relationship between compassion fatigue and anxiety levels of nurses after working in COVID-19 isolation wards in Kirkuk, Iraq. In this study, descriptive correlational design was used and the nurses after working in the COVID-19 isolation wards were selected by purposive sampling (n = 170) between 10 and 17 September 2022. Sociodemographic Information Form, Compassion Fatigue Scale, and State Anxiety Inventory were used in data collection through face-to-face interviews with nurses. Descriptive statistics, Levene test, Kruskal-Wallis test, Independent sample t-test, One-way ANOVA, Pearson correlation, and Ordinal Logistic Regression analyses were used to analyze data. The mean score of the Compassion Fatigue Scale and the State Anxiety Inventory for nurses working in the COVID-19 isolation wards was 39.53 ± 8.76 and 50.97 ± 7.45, respectively. This study determined that nurses working in the COVID-19 isolation wards had moderate compassion fatigue and anxiety levels. The results also showed a statistical significance between compassion fatigue and gender, age, and nursing experience, while anxiety levels and educational level. According to the results of ordered logistic regression analysis, men had a level of compassion fatigue than 0.07 times less than women; anxiety levels of nurses with 11 to 15 years of experience are 0.13 times less than those with 20 to 25 years of experience. There was no statistically significant relationship between compassion fatigue and anxiety levels of nurses working in the COVID-19 isolation wards. Given these risk factors, it is critical to implement targeted interventions to mitigate compassion fatigue and anxiety among nurses in COVID-19 isolation wards in Iraq. There should establish dedicated units to address the mental health needs of nurses, provide regular counselling, and stress management programs.
Introduction
Coronavirus or severe acute respiratory syndrome (SARS-cov-2) called Coronavirus Disease (COVID-19) was first detected in Wuhan, China, in December 2019 (Okereke et al., 2020). COVID-19 was declared a pandemic and a public health emergency by the World Health Organization (WHO) on March 11 (Xiong et al., 2020). According to a report issued by the WHO in December 2020, the number of infections among health care providers reached 10% globally (WHO, 2020). In the world, especially health care workers such as nurses, has been affected due to their direct contact with patients and their critical role in limiting the spread of infection (Nemati et al., 2020). Studies have shown that nurses working directly with COVID-19 patients are more likely to experience psychological problems than other nurses (Alshekaili et al., 2020; Arpacioglu et al., 2021). In addition, several studies have indicated increased levels of mental health problems among nurses during COVID-19 (Alshekaili et al., 2020; Arpacioglu et al., 2021; Keogh et al., 2020). Research indicates that nurses on the front lines are significantly more affected, with a 1.5 times higher likelihood of experiencing anxiety. Additionally, they report greater stress and insomnia compared to their colleagues who are not directly involved in COVID-19 care (Alshekaili et al., 2020).
The nursing profession is characterized by its demanding and heavy nature. The demands of the nursing profession make nurses stressful and thus put them at risk of anxiety. According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5, 2015), anxiety is “anticipation of future threat” (p. 189; American Psychiatric Association [APA], 2015). Anxiety also causes multiple problems for nurses, affecting their well-being and mental health, affecting the quality of care provided and impeding the nursing process (Maharaj et al., 2018). Nurses were expected to experience crises, exposure to risk of anxiety compared to other professions (Labrague & De Los Santos, 2020; Waris et al., 2020). Through previous studies, it was found that the most common psychological disorders caused by direct work with COVID-19 were anxiety, compassion fatigue, post-traumatic disorder, dissatisfaction, and tension (Luo et al., 2020; Murat et al., 2021). A long-term study Grasmann et al. (2025) showed a significant increase in anxiety symptoms and their levels were much higher among nurses than the general population. Tao et al. (2024) also noted anxiety among nurses during the COVID-19 pandemic and it was more common than other psychological disorders. In addition, compassion fatigue also had the highest expected effect value. In a comprehensive meta-study conducted by Al Maqbali et al. (2024), it was found that nurses were more prone to anxiety than other groups, at 30.8%.
The term compassion fatigue was first coined in 1992 by Nurse Figley then developed the concept and defined it as “a state of exhaustion and dysfunction-biologically, physically, and socially-as a result of prolonged exposure to compassion stress and all that it evokes” (Bride et al., 2007; Joinson, 1992). Nurses often must share their emotions with their patients suffering from trauma to facilitate the healing process; through this sharing, the nurses are placed in the face of the traumatic events of their patients (Bride et al., 2007). An empathetic nurse can fall victim to the constant pressure of meeting patients’ needs and experiencing the same feelings as their patients, so the cost of this care can be the nurse’s health (Figley, 2013; Lombardo & Eyre, 2011). Nurses are also exposed to compassion fatigue when feeling despair resulting from a feeling of inability to change the patient’s health status (Sacco et al., 2015). Compassion fatigue affects the health and well-being of nurses and leads to their feelings of despair, frustration, boredom and sadness. Compassion fatigue also causes nurses to fear their workplace and unwillingness to communicate with some patients, which leads to a shortage of nurses or to provide substandard care (Showalter, 2010).
Nurses’ exposure to the suffering and constant patient requests during COVID-19 generates sympathy for patients, which in turn causes anxiety and compassion fatigue (Gustafsson & Hemberg, 2021). One of the reasons compassion fatigues occurs is the shortage of nurses, who are forced to work long hours and sometimes overtime because there are not enough numbers to care for patients (Pfefferbaum & North, 2020). It is known that compassion fatigue leads to multiple adverse effects (Sung et al., 2012). These negative effects are anxiety, depression, stress and sleep disturbances (Whitebird et al., 2013). It also makes it difficult for nurses to provide emotional care and thus leads to patient mistreatment, neglect, and work-related errors (Cross, 2019). There could be a positive relationship between anxiety and compassion fatigue. People with compassion fatigue show higher levels of anxiety, also (Kim & Na, 2017). Anxiety is considered a risk factor for compassion fatigue, as people with high anxiety levels have a higher risk for compassion fatigue (Craigie et al., 2016; Gustafsson & Hemberg, 2021). According to a report issued by the WHO during the period (June-August 2020), showed 93% of 130 countries witnessed a delay in providing mental health services and education about crisis management at times when these services were most needed (WHO, 2020). The demand for psychological services is increasing due to the continuing pandemic. Therefore, preserving and supporting nurses’ mental health is essential to maintaining the continuity of the nursing process and providing high-quality health care (Chen et al., 2021). Psychological care interventions can prevent the emergence of various and multiple psychological effects. From here, the important role of psychiatric nurses during the spread of the epidemic and their influential role in supporting the mental health of nurses working in direct contact with COVID-19 and reducing stress and psychological symptoms can be important (Walton et al., 2020). The Consultation Liaison Psychiatric (CLP) nurses aim to provide a safe and comfortable environment for nurses by helping them adapt to the new environmental conditions considering the circumstances of COVID-19, providing encouragement and education regarding mental health, providing advice and guidance (Kuzman et al., 2020).
The importance of the current study includes studying the levels of anxiety and compassion fatigue in the long term after the third wave of the COVID-19 pandemic, which is rare among the available references because most studies included studying the psychological problems mentioned above during the first and second waves, which showed high rates of psychological problems (Azoulay et al., 2020; Grasmann et al., 2025; Heesakkers et al., 2023; Luceño-Moreno et al., 2021; Umbetkulova et al., 2024). The nurses in Iraq had to deal with the aggressive behavior of some patients and their families inside the hospital. In addition, nurses not to mention the nurses feeling excluded and stigmatized because of their work with the virus and people fearing that the nurses could infect them. Working with the pandemic has created a lot of anxiety, stress, and fear for nurses about getting infected and transmitting the infection to their families (Shah et al., 2021). Despite the global research on anxiety and compassion fatigue in nurses during the COVID-19 pandemic, studies specific to Iraq remain scarce. Given the unique challenges faced by Iraqi nurses, including exposure to aggressive patient behavior, social stigma, and fear of infection, this study aims to bridge the gap by examining the relationship between compassion fatigue and anxiety levels among nurses in Kirkuk, Iraq. Understanding this relationship is crucial for developing targeted interventions to support nurses’ mental well-being. This study is important to understand the compassion fatigue and anxiety-related variables during COVID-19, and to develop preventive and interventional programs. This study is also important in terms of contributing to psychiatric nurses’ planning of Consultation Liaison Psychiatry (CLP) services for their colleagues in the context of their duties and responsibilities in this area.
Methods
Aim and Design
In this study, descriptive correlational design was used. This study aimed to examine the relationship between compassion fatigue and anxiety levels of nurses after working in COVID-19 isolation wards in hospital, Kirkuk, Iraq. At the time of the research, 295 nurses worked in the isolation ward (N = 295). Nurses who working in the isolation ward are divided as follows: 22 nurses work part-time from 8 a.m. to 3 p.m., 5 days a week, and the rest of the nurses’ work in a shift system 1-day a, 24 hr a week, 1 day for every 6 days.
Sample
The sample calculation formula with known universe was used to determine the sample size in the current research (Alpar, 2016). The total number of nurses who working in the isolation wards is (N = 295), with an error rate of 0.05, the minimum number of nurses to be included in the sample was determined as 168 nurses using the sample calculation formula with a known population. In this study, 170 nurses were reached (n = 170). Data for the current study were collected from September 10 to 17, 2022. Criteria for including nurses in the current study included willingness to participate, ability to speak and understand Arabic, are working as a nurse in the related hospital COVID-19 ward at least 1 year and being present during the study. The nurses undergoing psychological treatments were excluded.
Data Collection Tools
Sociodemographic Information Form
The researchers developed Sociodemographic Information Form through a literature review and this form include questions related to age, gender, marital status, occupation, educational level, and nursing experiences. It also included information about the duration of work in the COVID-19 isolation ward (Al-Razaq et al., 2018).
Compassion Fatigue Scale
The Compassion Fatigue Scale (CFS) is a self-reported measure to determine the level of fatigue resulting from empathy and was developed by Adams et al. (2008). Al-Razaq et al. (2018) adapted the CFS to Arabic and used 10 questions from the original scale, and the remaining questions were not used in the Arabic version because they were not in harmony with the Arab community. The final form of the Arabic version had 14 questions, and there were no sub-dimension or inverse questions. The CFS was rated on a 5-point Likert-type scale “never = 1, rarely = 2, sometimes = 3, most of the time = 4, and always = 5.” The level of compassion fatigue among nurses is determined based on the total scores of the items. The minimum score obtained from the scale is 14, and the maximum is 70. Compassion fatigue increases with the increase in the number of points, so the score is considered as 14 to 32 mild level, 33 to 51 moderate level, and 52 to 70 severe level. The Cronbach Alpha coefficient of the CFS was measured at .73, and in the present study, it was found to be .82.
State Anxiety Inventory
State-trait anxiety inventory (STAI) consisted of state and trait of anxiety dimensions and was developed by Spielberger (1972). This study used only the State anxiety inventory (SAI) dimension of STAI. The scale is a self-report measure used to diagnose individuals with anxiety, and it can be used with patients and the normal population. The SAI measures the state of anxiety and consists of 10 positive (1, 2, 5, 8, 10, 11, 15, 16, 19, 20) and 10 negative questions (3, 4, 6, 7, 9, 12, 13, 14, 17, 18). The SAI requires the participants to answer what they feel “at present” and respond to each item without thinking about it. The SAI was adopted into Arabic by Kadiem and Hamzah (2004). The SAI was rated on a 4-point Likert-type scale “never = 1, sometimes = 2, most of the time = 3, always = 4.” The minimum score that can be obtained from the scale is 20, and the maximum is 80. State anxiety increases with the increase in total scores. Thus, the score is considered as 20 to 40 mild level, 41 to 60 moderate level, 61 to 80, severe level. The Cronbach Alpha coefficient of the SAI was measured at .79, and in the present study, it was found to be .76.
Data Collection
Data was collected from nurses working in the COVID-19 isolation ward at a hospital in Kirkuk, Iraq, between 10 and 17 September 2022. Data was collected face-to-face, using data collection tools by the researcher, and it took approximately 30 min for a nurse to fill out the data collection tools.
Statistical Analysis
Analysis of the data SPSS (Statistical Package for Social Sciences) program version 22 was used. The data were analyzed by an independent statistician outside the research. Descriptive data were analyzed as numbers, percentages, mean, and standard deviation. Cronbach alpha was used for reliability. The homogeneity of variance was tested using Levene’s test. The t-test was used to examine differences in CFS and SAI scores for demographic characteristics consisting of two categories, such as gender. The Kruskal-Wallis test was used for the rest of the variables consisting of more than two categories because there was no normality and homogenesis condition. In the presence of three or more categorical variables, pairwise comparison analysis was performed to determine which group the significance originated from. Pearson Correlation test was used to find the relationship between CFS and SAI scores (Polit & Beck, 2004). The correlation coefficient (r) is the statistical value that numerically expresses the amount of the relationship. The value of the correlation coefficient is between −1 and +1 indicates the r value as small, medium and large, respectively, because of the correlation analysis (≥.10; ≥.30; ≥.50; Cohen, 1988). The Ordinal Logistic Regression analyses was used to determine the factors that affect the compassion fatigue and anxiety levels of nurses working in COVID-19 isolation wards in terms of various variables. A confidence interval of 0.95 was considered, with a significance level less than .05 (Polit & Beck, 2004).
Ethical Consideration
In this study, ethical approval was obtained from the relevant university of ethical committee (date: April 21, 2022, decision no: 25) before starting data collection. Then, institution approval was obtained from the Iraq Ministry of Health, from Kirkuk Health Department Training and Development Department, and relevant hospital. Permission to use the scales used in the study was obtained from the relevant authors via e-mail. The confidentiality and confidentiality informed the participants of the research, and the Informed Consent Form was signed, stating that all information will be used only for research purposes and cannot be accessed by anyone other than the researchers. The questionnaire did not include personal information or names. The research was carried out according to the rules of the Declaration of Helsinki (World Medical Association, 2013).
Results
In this study aimed to examine the relationship between compassion fatigue and anxiety levels of nurses after working in COVID-19 isolation wards in hospital, Kirkuk, Iraq, the mean age of the nurses working in the COVID-19 isolation wards was 31.47 ± 7.57 (minimum 21-maximum 48). In addition, 48.8% of nurses were 20 to 29 years old, 64.7% were male, 69.4% were married, and 42.9% were bachelor graduates. The mean nursing experience of nurses working in COVID-19 isolation wards was 8.42 ± 7.14 years, and the period of working in the COVID-19 isolation wards was 1.84 ± 0.84 years (Table 1).
The Distribution of the Socio-demographic Data of Nurses Working in the COVID-19 Isolation Wards (n = 170).

The mean score of CFS for nurses was 39.53 ± 8.76. The mean score of SAI for nurses was 50.97 ± 7.45. Thus, it was determined that nurses working in the COVID-19 isolation wards had moderate levels of compassion fatigue and anxiety (Table 2).
Mean Scores of Nurses Working in the COVID-19 Isolation Wards from CFS and SAI (n = 170).

In this study, CFS score of nurses working in the COVID-19 isolation wards according to age was found to be a statistically significant difference (H = 7.369; p < .05). Pairwise comparison analysis was performed to determine which group the significance originated from. The analysis showed statistically significant differences between 20 to 29 years and 40 to 49 years (p = .007). The compassion fatigue level of nurses in the 20 to 29 age group was found to be higher than the 40 to 49 age group. CFS score of nurses working in the COVID-19 isolation wards according to gender was found to be a statistically significant difference (t = −6.050; p < .05). It was found that female nurses had compassion fatigue more than male nurses. CFS score of nurses working in the COVID-19 isolation wards according to nursing experiences was found to be a statistically significant difference (H = 14.179; p < .05). Pairwise comparison analysis was performed to determine which group the significance originated from. The analysis showed statistically significant differences between 1 to 5 years and 20 to 25 years (p = .003). The compassion fatigue level of nurses has 1 to 5 years nursing experience was found to be higher than the 20 to 25 years nursing experience. A statistically significant difference was not found between the CFS scores of nurses working in the COVID-19 isolation wards with marital status, educational level, and period of working in the COVID-19 isolation wards (p > .05; Table 3).
Distribution of CFS Scores by Socio-demographic Characteristics of Nurses Working in the COVID-19 Isolation Wards (n = 170).
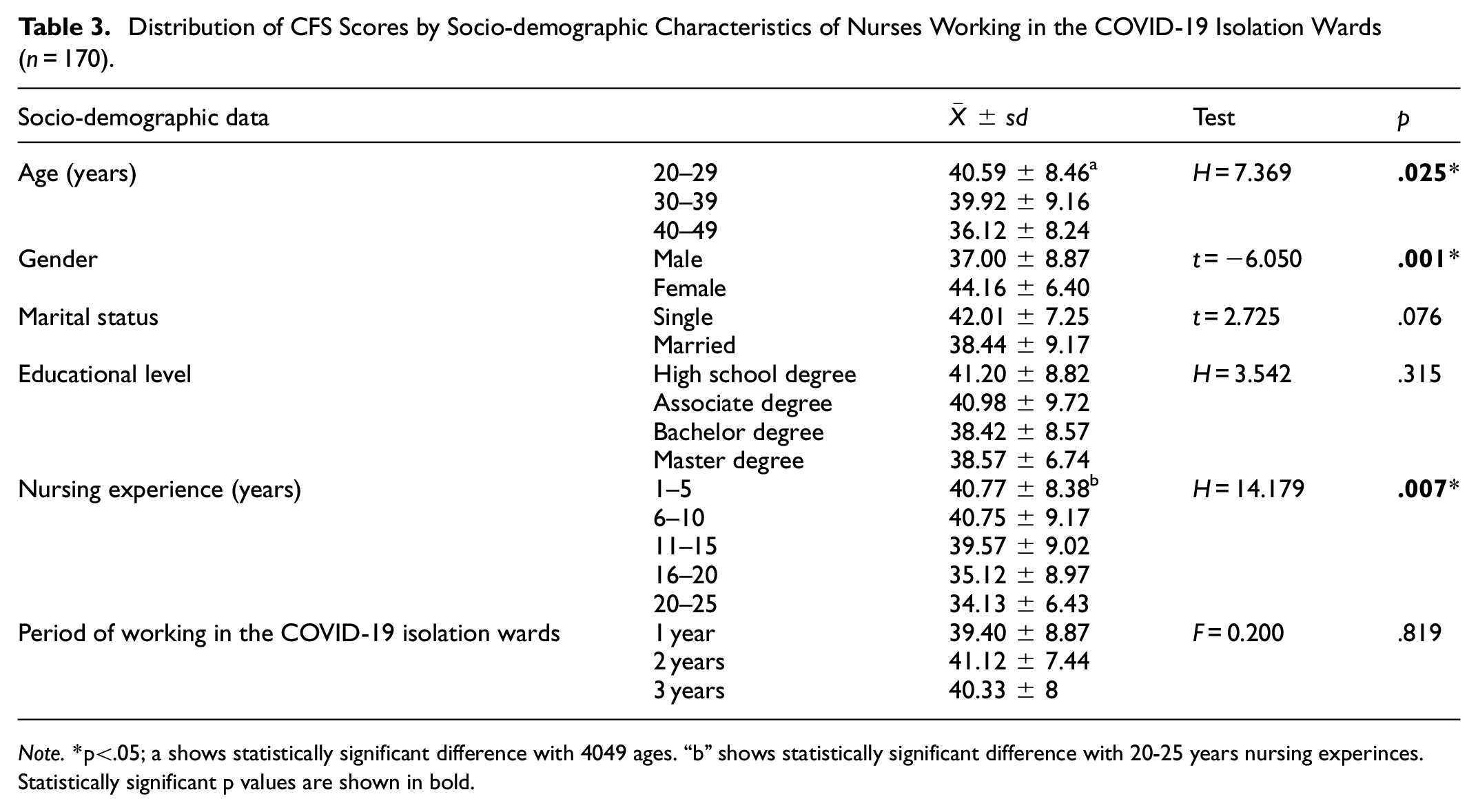
Note.*p<.05; a shows statistically significant difference with 4049 ages. “b” shows statistically significant difference with 20-25 years nursing experinces. Statistically significant p values are shown in bold.
In this study, SAI score of nurses working in the COVID-19 isolation wards according to educational level was found to be a statistically significant difference (H = 15.715; p < .05). Pairwise comparison analysis was performed to determine which group the significance originated from. The analysis showed statistically significant differences between associate degree and bachelor’s degree working in COVID-19 isolation wards (p = .001). The anxiety level of nurses has bachelor’s degree was found to be higher than associate degree. Between the SAI scores of nurses working in the COVID-19 isolation wards with age, gender, marital status, nursing experience and period of working in the COVID-19 isolation wards was not found a statistically significant difference (p > .05; Table 4).
Distribution of SAI Scores by Socio-demographic Characteristics of Nurses Working in the COVID-19 Isolation Wards (n = 170).

Note. Statistically significant p values are shown in bold. “a” shows statistically significant difference with associate degree.
As a result of the analysis, there was not a statistically significant between CFS scores and SAI scores of nurses working in the COVID-19 isolation wards (p > .05; Table 5).
The Relationship Between CFS Scores and SAI Scores of Nurses Working in the COVID-19 Isolation Wards (n = 170).

The Ordinal Logistic Regression Model was created to determine the factors that affect the compassion fatigue levels of nurses working in COVID-19 isolation wards in terms of various variables. It was found that the parallel assumption of this model was determined (p > .05) and the model compliance was good (p > .05). 29% of the dependent variable of compassion fatigue in the model is explained by independent variables. It was found that one of the five independent variables in the model were statistically significant according to certain categories (p < .001) and others were meaningless. This result was found to have a statistically significant relationship between gender and compassion fatigue. It was found that men had a level of compassion fatigue than 0.07 times less than women (Table 6).
Ordinal Logistic Regression Results of CFS (n = 170).

Note. β = regression coefficient; SE = standard error; Exp (β) = odds ratio, 0a = reference variable, LB, and UB are the 95% lower and upper bonds of confidence intervals for β or Exp (β). Gender coded as “0 = severe,”“0 = female,”“0 = married,”“0 = master,”“0 = 20 to 25 years nursing experience.” Statistically significant p values are shown in bold.
The Ordinal Logistic Regression Model was created to determine the factors that affect the anxiety levels of nurses working in COVID-19 isolation wards in terms of various variables. It was found that the parallel assumption of this model was determined (p > .05) and the model compliance was good (p > .05). 6% of the dependent variable of anxiety in the model is explained by independent variables. It was found that one of the four independent variables in the model were statistically significant according to certain categories (p = .034) and others were meaningless. This result was found to have a statistically significant relationship between nursing experiences and anxiety. Accordingly, anxiety levels of nurses with 11 to 15 years of experience are 0.13 times less than those with 20 to 25 years of experience (Table 7).
Ordinal Logistic Regression Results of SAI (n = 170).

Note. β = regression coefficient; SE = standard error; Exp (β) = odds ratio, 0a = reference variable, LB, and UB are the 95% lower and upper bonds of confidence intervals for β or Exp (β). Gender coded as “0 = severe,”“0 = female,”“0 = master,”“0 = 20 to 25 years nursing experience.” Statistically significant p values are shown in bold.
Discussion
This study found that nurses COVID-19 isolation wards had moderate levels of compassion fatigue. This study agrees mostly with the studies of where most of the sample showed moderate compassion fatigue (Christianson et al., 2023; Sahin et al., 2023). And differed from the results of it was likely that the results of the studies differed due to the stage of the epidemic at the time the study was conducted. Studies showed the same results in the third stage of the pandemic, where sufficient information and vaccines were available, with fewer infections and a decrease in pressure on nurses (Amir & Okalo, 2022; Labrague & de Los Santos, 2021). The studies whose results varied, they could be conducted in the early stages of the epidemic considering the lack of information, the unavailability of vaccines, and the continued rise in the number of infections. This comparison could indicate that compassion fatigue among nurses was affected by work pressure, the number of infected patients, and working in a safe environment. Additionally, depending on the studies being conducted in different cultures and countries, this could be due to nurses’ different working conditions, workloads, and psychological resilience.
This study found that the compassion fatigue level of nurses in the 20 to 29 age group was found to be higher than in the 40 to 49 age group. Also, it was found that female nurses had compassion fatigue more than male nurses. Men had a level of compassion fatigue than 0.07 times less than women. The compassion fatigue level of nurses has 1 to 5 years nursing experience was found to be higher than those in the 20 to 25 years nursing experience. The results of the current study were consistent with the results of the Amir and Okalo (2022), Labrague and de Los Santos (2021) and differ from the study of Sahin et al. (2023) and Alharbi et al. (2019). The results of the current study were also consistent with the results of many studies before the epidemic, where age, years of experience, and gender affected levels of compassion fatigue (Alharbi et al., 2020; Figley, 2013; Xie et al., 2021). Perhaps women were more susceptible to compassion fatigue than males due to the female’s physiological and emotional make up, in addition to her other duties and responsibilities such as childcare and other responsibilities and household chores and perhaps take care of a family member. The results showed a correspondence between age and years of experience, which exhibited an inverse consistency with compassion fatigue. The fewer years of experience and age, the greater the levels of compassion fatigue among nurses. These results were attributed to a lack of experience in the field of work and life, or perhaps not yet adapting to the conditions of work and not having gone through similar experiences before. Additionally, as nurses’ experience increases, they constantly encounter many patients. Accordingly, nurses could have become automatic in their nursing skills, and their awareness and empathy skills toward patients may have decreased.
This study found that nurses working in the COVID-19 isolation wards had moderate levels of anxiety. The level of anxiety in the current study was consistent with studies conducted by in Pakistan and Italy, respectively (Nadeem et al., 2021; Simonetti et al., 2021). A study conducted by Hadi and Mohammed (2022) showed a statistically significant relationship between anxiety and the spread of COVID-19. Foodani et al. (2023) to study nurses’ anxiety from COVID-19 and its relationship to the quality of professional life, the results showed that nurses had moderate anxiety, and there was a statistically significant relationship between anxiety and quality of professional life. The current study was inconsistent with studies conducted by Roberts et al. (2021) and Wong et al. (2020). The difference in results may be due to the demographic composition of the sample in terms of personal reasons, such as physical activity and diet, or reasons related to the work environment, such as the presence of an outlet and a place to rest between shifts, or behavioral and cognitive reasons for the nurse, such as psychological state, expressing feelings, and maintaining social contacts. The difference in results could also be due to the population density of infections in each study, the time the study was conducted concerning the stage of the epidemic, the extent of the availability of protective equipment, and sufficient information related to the pandemic.
The current study showed that the anxiety level of nurses has bachelor’s degree was found to be higher than associate degree. This study agrees with the Hadi and Mohammed (2022) results of in terms of the effect of the scientific level on levels of anxiety, but it differs in that the current study did not show any relationship with demographic variables. The current study did not agree with the results of several studies (Çelmeçe & Menekay, 2020; Nadeem et al., 2021; Roberts et al., 2021). The fact that bachelor’s degree nurses working in the COVID-19 isolation wards experience more anxiety shows the effect of bachelor nursing education in Iraq. It may have caused them to experience much anxiety as their level of knowledge of nurses about the diseases increased.
In this study, anxiety levels of nurses with 11 to 15 years of experience are 0.13 times less than those with 20 to 25 years of experience. Similar results were found in the studies discussed in the literature. It is stated that there are significant differences between the anxiety levels of nurses working in COVID-19 services and nursing experience (Cho & Kim, 2021; Morgado-Toscano et al., 2023; Shen et al., 2021). Nurses with longer careers (20–25 years) may experience greater burnout and fatigue from sustained exposure to high-stress environments. The cumulative effect of chronic stress, compassion fatigue, and workload can make them more vulnerable to anxiety. In addition, senior nurses (20–25 years of experience) might face greater physical strain and fatigue, which can exacerbate anxiety. Senior nurses are more likely to have familial responsibilities (e.g., caring for children or elderly parents), increasing fear of infection and transmitting the virus to loved ones. This concern might be more pronounced in nurses with longer careers, leading to higher anxiety levels.
As a result of the analysis, there was no statistical significance between compassion fatigue and state anxiety scores of nurses working in the COVID-19 isolation wards. The results of a study by Lluch-Sanz et al. (2022) showed an increase in the rate of compassion fatigue, and the main risk factor associated with it was anxiety. To the best of our knowledge, no study was conducted to study anxiety and compassion fatigue under the conditions of the spread of COVID-19 in Iraq. Thus, it was difficult to compare the current study with similar studies under the same conditions, but many studies examined the relationship between compassion fatigue and anxiety before the pandemic (Cross, 2019; Hegney et al., 2014; Jo et al., 2020; Whitebird et al., 2013). The current study did not show any relationship between compassion fatigue and anxiety. The reasons may be due to other factors that affect the relationship, such as the person’s personality, resilience, and level of social support from the institution and family.
Conclusion
The analysis revealed no statistically significant relationship between compassion fatigue and state anxiety scores among nurses working in COVID-19 isolation wards. However, nurses in these wards exhibited moderate levels of both compassion fatigue and state anxiety. Further findings indicate that younger nurses (20–29 years old) reported higher levels of compassion fatigue compared to those aged 40 to 49. Female nurses experienced higher levels of compassion fatigue than their male counterparts. Specifically, the compassion fatigue level in men was 0.07 times lower than in women. Nurses with 1 to 5 years of experience had higher compassion fatigue levels than those with 20 to 25 years of experience, suggesting that early-career nurses are particularly vulnerable. Nurses with 11 to 15 years of experience had anxiety levels 0.13 times lower than those with 20 to 25 years of experience, indicating that more seasoned nurses may experience heightened anxiety over time. Given these risk factors, it is critical to implement targeted interventions to mitigate compassion fatigue and anxiety among nurses in COVID-19 isolation wards in Iraq. There should establish dedicated units to address the mental health needs of nurses, provide regular counseling and stress management programs. In addition, screening protocols to identify nurses at high risk of compassion fatigue and anxiety should develop and proactive strategies, including peer support programs and resilience training should implement.CLP nurses should play a central role in raising awareness, enhancing coping mechanisms, and supporting self-care among nurses. Hospitals should formally incorporate CLP nurses into their strategic planning to reduce psychological distress among frontline nurses. The Ministry of Health should establish guidelines for managing psychological stress and structured mental health education and crisis management training for nurses working in high-stress environments should develop. By implementing these strategies, healthcare institutions in Iraq can reduce the long-term psychological impact on nurses, improve workplace well-being, and enhance the overall quality of patient care.
Limitations of the Study
The results of the current research cannot be generalized because the data were taken from nurses working in isolation wards for COVID-19 patients in a hospital in Kirkuk, Iraq, where the results represent the current sample only.
Footnotes
Acknowledgements
All authors are grateful to all the participants for their useful contributions to this study.
Ethical Considerations
In this study, ethical approval was obtained from the relevant university of ethical committee (date: April 21, 2022, decision no: 25) before starting data collection. Then, institution approval was obtained from the Iraq Ministry of Health, from Kirkuk Health Department Training and Development Department, and relevant hospital. Permission to use the scales used in the study was obtained from the relevant authors via e-mail. The confidentiality and confidentiality informed the participants of the research, and the Informed Consent Form was signed, stating that all information will be used only for research purposes and cannot be accessed by anyone other than the researchers. The questionnaire did not include personal information or names. The research was carried out according to the rules of the Declaration of Helsinki (World Medical Association, 2013).
Author Contributions
SJMM: Conceptualization, formal analysis, investigation, writing and editing. HAD: Conceptualization, formal analysis, investigation, supervision, writing and editing. All authors have read and approved the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.