
Abstract
The deteriorating physical and mental health of the rural elderly has become a common problem in developing countries and demands immediate attention. This article investigates the overall impact of China’s policy of community-based home care on rural elderly’s health, reveals the underlying mechanisms, and examines specific types of elderly care services. Based on the theoretical analysis of the mechanisms, we carried out an empirical analysis using the PSMDID method with data from the China Health and Retirement Longitudinal Study (CHARLS) for 2013, 2015, and 2018. We find that community-based home care not only reduces the scores of Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) among the rural elderly but lowers their scores of negative emotions and levels of depression, therefore enhancing their physical and mental health. These effects remain robust against sensitivity analyses, regression by year, and interferences of previous policies. Distinguishing different types of services, we find that daily care reduces individuals’ scores of ADL and negative emotions, and therefore enhances physical and mental health; while regular medical and recreational services lower ADL or IADL scores and thus improve physical health, their impact on mental health is not significant. This article concludes that community-based home care significantly improves the physical and mental health of rural elderly, and hence advises rural pension policy-making.
Introduction
The declining physical and mental health of the rural elderly has become a common problem in developing countries, demanding immediate attention. In rural China, a scarcity of healthcare resources and social safety nets has given rise to a host of health challenges among the elderly, including chronic diseases of the “three highs” (Jiang & Liu, 2023; Ma et al., 2022), major illnesses, loneliness, anxiety, and depression, which in some cases have resulted in impoverishment and suicide.
By the end of 2022, two-thirds of Chinese people aged 65 and above had been suffering from multiple diseases, 78% had at least one chronic illness, and the number of disabled had been increasing (AANEWS, 2023). Research also indicates significant disparities in access to healthcare between urban and rural residents in developing countries like China (Zhang et al., 2017), resulting in poorer health of the rural elderly. The health conditions of the elderly in other developing countries, such as India, are worse than in China, according to the Study on Global Ageing and Adult Health by the World Health Organization (WHO; Kowal et al., 2012).
In recent years, China has been implementing home-based elderly care to address the health problems caused by the lack of family care. However, this policy remains to be systematically evaluated. Community-based home care originates from “community care,” which aims to provide care for elderly people with declining physical functions, enabling them to live at home or in a home-like environment. The recipients of community-based home care services, which include dining, laundry and household chores, medical care, recreational activities, etc., are elders (aged 60 or above) who need care because of age, illness, or other reasons. The criteria for receiving the services vary from one region to another. In 2016, pilots of community-based home care were implemented by China’s Ministry of Civil Affairs and Ministry of Finance (Ma, 2022). The number of elderly care facilities in China has rapidly increased from 18,000 in 2014 to 360,000 in the first quarter of 2022 (Li, 2022). Community-based elderly care, as an effective way to accommodate an aging population, has gained rapid development (Feng et al., 2020; Shao et al., 2021; Shi, 2020).
Existent literature on the performance of community-based home care mainly focuses on the services per se, including existing problems and solutions (Sabetsarvestani et al., 2021), the efficiency of service supply (Büscher et al., 2022), service quality (McDonald & Russell, 2019; Ning et al., 2022), and service accessibility (Li et al., 2023; Nässén et al., 2023). Notably, a contribution analyzes the housing problem of the elderly in Hong Kong in the context of the community-based ageing-in-place model, examines the supply and demand, and reveals the phenomenon of economically motivated housing downsizing and the government’s response (Li et al., 2022). But there is only limited empirical research on the impacts of community-based home care on the physical and mental health of the rural elderly. Does community-based home care have positive impacts on the physical and mental health of rural elderly individuals? Do the impacts vary with different types of community-based home care services? These questions remain to be answered.
The purpose of this paper is to analyze the multidimensional impact of community-based home care and their different functions on the health of rural elderlies by drawing on the empirical facts of the implementation of community-based home care services, with specific factors including Activities of Daily Living (ADL), Instrumental Activities of Daily Living (IADL), depression level and so on. The ADL score, a tool used to assess an individual’s ability to perform activities of daily living (ADL), can assist healthcare professionals in providing patients with appropriate rehabilitation guidance and support. The IADL score refers to the assessment of instrumental activities of daily living, that is, activities performed by a person to maintain an independent life, including shopping, using transport, preparing food, doing household chores, managing finances, etc. Depression level measures the severity of an individual’s depressive symptoms.
Compared with similar studies, this article makes contributions in three dimensions. First, it systematically analyzes the mechanisms and the varying impacts of distinct types of community-based home care. Second, this article uses PSM-DID to identify the effects of community-based home care on rural elderly’s health. This approach effectively addresses the endogeneity arising from self-selection, eliminates the influence of unobservable factors that remain constant over time, and enhances the accuracy and reliability of the conclusions. Last, this article uses large-sample balanced panel data from the China Health and Retirement Longitudinal Study (CHARLS) for 2013, 2015, and 2018 to improve the representativeness and external validity of our research findings.
By investigating community-based home care services, we aim to improve the quality and efficiency of service provision, safeguard the physical and mental health of the rural elderly, and provide theoretical support for the effective integration of social service resources.
This article proceeds as follows. Section “Research Hypotheses” raises our research hypothesis. Section “Research Methods and Data” introduces the research methodology and data sources, which is followed by a descriptive analysis in Section “Descriptive Statistics.” Section “Results of Econometrics Analysis” presents the econometric analysis and the robustness tests. Section “Conclusion” concludes the article.
Research Hypotheses
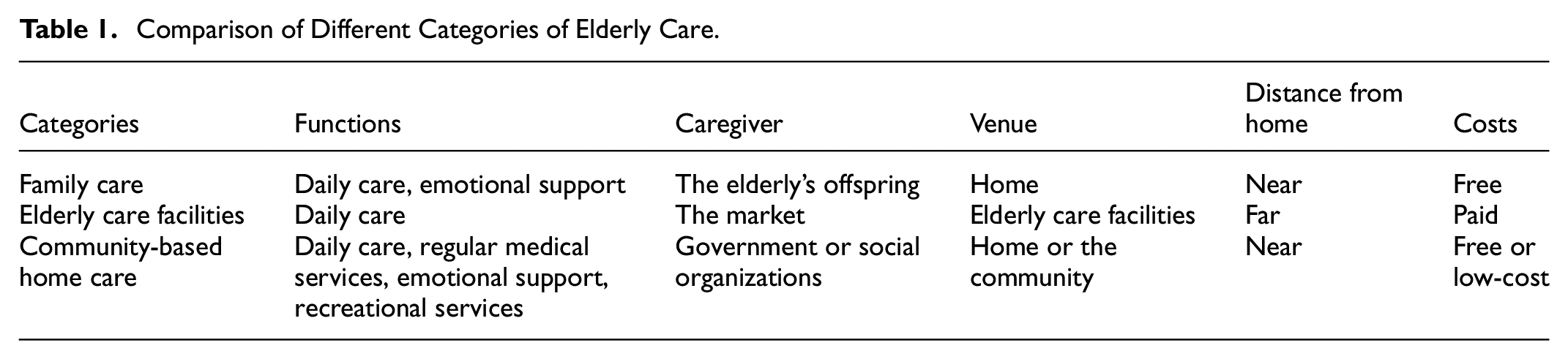
China’s elderly care can be roughly divided into three categories based on the venue and form: family care, elderly care facilities, and community-based home care. In traditional family care, financial support, daily care and emotional comfort for the elderly almost completely rely on family members (Ouyang et al., 2018), and the caregiving burden is even heavier in rural areas. Family members, mostly elderly people’s offspring, are caregivers in their daily life or in diseases, and devote time, effort, and money to fulfill this role, which subjects the elderly to stress (Fast et al., 1999) and has adverse effects on their mental and physical well-being.
Lack of family care is considered a significant contributing factor to the rural elderly’s declining health. The seventh national census suggests that the average household size in China decreased from 3.10 in 2010 to 2.62 in 2020. This, joined by a lowered birth rate and an aging population, reduces elderly care resources within families (Wang et al., 2023). Besides, social development moves a large number of young and middle-aged laborers from rural areas to cities for non-agricultural work (Pan, 2018; Pan et al., 2021; Xie & Jiang, 2016), changing the traditional pattern of multigenerational living. As many as 63.9% of Chinese rural elderly live separately from their children, with reduced opportunities to receive intergenerational support, such as family care and emotional support (Zhao et al., 2023). Moreover, they may even take on the responsibility of caring for their grandchildren. Studies show that this caregiving role may limit their time and opportunities to take care of themselves, and leads to physical and emotional stress (Hong et al., 2023). Therefore, the role of family care is weakened (Li et al., 2022), diminishing its positive influence on the rural elderly.
Apart from challenges in family care, elderly care facilities in China are underdeveloped with limited management capacity (Chu & Chi, 2008). Nursing homes are scarce in rural areas, and most of them only provide accommodation and basic care, often with limited outreach to surrounding areas. Also, the cost of nursing homes is high (Grabowski et al., 2023; Welford et al., 2010) and unaffordable to low-income elderly people in rural areas (Xu et al., 2022). Living in elderly care facilities means that the elderly have to leave their family and familiar environments. This weakens the support they can receive from loved ones, friends, and society, and imposes significant pressure on them to develop new connections in nursing homes (Gautam et al., 2021).
Community-based home care has the following advantages vis-à-vis the above two forms. Firstly, it optimizes resource allocation. It allows rural elderly to live in their communities where they maintain their original lifestyle (Chyr et al., 2020; Mei et al., 2020), and receive care from the communities and their families. Second, it meets the elderly’s personalized needs. Nursing homes provide identical or similar services to elderly people based on uniform standards. In contrast, community-based home care is more personalized, gratifying, and targeted, and therefore capable of improving the elderly’ life and satisfaction (Davitt et al., 2016). Third, it effectively reduces the costs of elderly care. The temporary residential care provided by community-based home care can relieve the burden of family care and meanwhile tap community and household resources (Wu et al., 2023), reducing the government’s burden and lowering elderly care costs (Dyer et al., 2020).
Community-based home care works in the following ways. The daily care services provided by community-based home care enable rural elderly people to enjoy services in their familiar communities without leaving their homes. For example, in their daily life, when they encounter problems with cleaning and hygiene, cooking, etc., the elderly can contact community service staff by telephone. Community-based home care also provides regular medical services that are more affordable and convenient by treating minor ailments close to home and providing home-based medical and nursing care. This approach strengthens the emotional relationship with elderlies and reduces their psychological pressure. Regular medical check-ups screen out hidden diseases and risks in advance and improve the rural elderly’ physical health. Recreational services for aging in place provide rural elderly with venues for leisure, recreation, and fitness activities, which can effectively reduce their social isolation and negative emotions.
Existent research finds that community-based home care can significantly improve the health and welfare of the elderly. These services not only alleviate the financial burden on the elderly (Maruoka et al., 2023), but satisfy their emotional needs, which is crucial for their mental well-being (Polacsek & Woolford, 2022). Community-based home care maintains a basic standard of living for the elderly, engages them in physical activities, and thus improves their physical and mental health; it also increases the elderly’s social participation (Joyce et al., 2020), encourages interactions, fosters their interest and passion for life, thereby achieving positive aging (Shu, 2021). Additionally, it is found that community-based home care has a more pronounced effect on the rural elderly (Ma & Shen, 2023). Compared with family care, community-based home care employs specialized personal to provides the elderly with daily care and regular medical services. This reduces their children’s burden and offers more professional services. Compared with elderly care facilities, community-based home care enables the elderly to purchase services at a lower cost without leaving the familiar environment of their village. The differences between community-based home care, family care, and elderly care facilities are shown in Table 1.
Comparison of Different Categories of Elderly Care.
Based on the comparison, this article proposes the following hypotheses for empirical testing:
Community-based home care for the elderly can be categorized by functions, namely daily care, regular medical services, and recreational services, and each has a varying influence on the physical and mental health of the elderly.
Furthermore, existent research finds that engaging the elderly in community activities or providing home care and nursing services can enhance their life quality and satisfaction (Bölenius et al., 2017; Karlsson et al., 2013; Kim et al., 2020); providing them with medical and rehabilitation services at home helps maintain their functional capacities and prevents depression (Grillo et al., 2010; Kahrazei & Akbarizadeh, 2020). Scholars also analyze survey data on factors influencing the Chinese elderly’s health and find that the nursing services of community-based home care play a positive role in the elderly’s depression prevention, life satisfaction, cognitive function, and social participation (Su et al., 2023). Therefore, this article proposes the following hypotheses for subsequent empirical testing.
Research Methods and Data
Propensity Score Matching Difference-in-Differences (PSMDID) Method
Community-based home care was launched in 2016, but which areas would be the first to adopt it remains unknown. In places where it is implemented, the elderly can choose whether to participate or not, leading to the “self-selection” problem. Therefore, this article employs PSM-DID to investigate the impact of community-based home care on the health of the rural elderly to address the potential estimation bias caused by self-selection (Heckman et al., 1998). PSM-DID combines the advantages of the DID and the PSM methods.
This methodology is widely applied. For instance, the PSM approach is employed to find that social engagement has a positive impact on physical functioning and depression in Chinese empty-nester older adults (Su et al., 2020), and that the implementation of a smart city program has a favorable impact on mitigating the prevalence of developmental delays and wasting (Xu et al., 2024). In this article, we use the double difference method based on PSM proposed by Heckman et al. (1998) to explore the impact of community-based home care services on the health of rural elderlies. Suppose the dummy variable Di represents whether individual i receives community-based home care, where Di = 1 indicates receiving such services and Di = 0 indicates not. Let yi denote the health of the rural elderly. For each individual i, their health of yi may have two states, assumed to depend on whether they receive community-based home care, that is,

where y0i represents the health status of individual i who has not received community-based home care, while y1i represents that of individual i who has received community-based home care. (y1i–y0i) represents the causal effect of individual i receiving this service, or the “treatment effect.” Assuming individual i belongs to the experimental group, identify an individual j from the control group whose observable variables are as similar as possible to those of individual i (matching), that is, xi ≈ xj. There is no consensus in the academic community on the matching method. Therefore, this article adopts kernel matching and adjusts its brandwidth in robustness tests.
The treatment effect (y1i–y0i) is a random variable, and hence we are interested in its expected value, known as the average treatment effect (ATE), or the “average causal effect.”

The ATE represents the expected treatment effect of an individual randomly selected from the population, regardless of whether that individual receives the services. This definition, however, does not factor in the fact that some areas have not adopted community-based home care. This problem can be addressed by redefining the population. But the average treatment effect on the treated (ATT) may be more important to policymakers, as it measures the gross benefits of the care receivers. Therefore, this article only considers the ATT of individuals who receive community-based home care.

Based on the matched sample, the DID estimation runs as:

In this model, i represents rural elderly individuals; t represents time; Health it is the dependent variable that denotes the health of rural elderly individuals; Treat i is a dummy variable, which reports 1 if individual i belongs to the treatment group, and 0 if it belongs to the control group; Post t is a time dummy that equals 1 if the time is after 2016 and equals 0 if otherwise. Community-based home care was carried out in 2016, so the 2015 data was collected before the implementation, and the 2018 data after the implementation. This article focuses on the estimated value of the coefficient β, which represents the net effect of community-based home care on the health of the rural elderly. Xit is a control variable; ε it is the random error term; β0 is the constant term; μ i represents individual fixed effects; λt represents time fixed effects.
Data and Variables
The data used in this article is from the CHARLS. This survey was conducted by the Institute of Social Science Survey of Peking University to collect representative data from Chinese people aged 45 and above. The CHARLS data is a crucial microdata set for studying population aging in China. In addition to basic sociodemographic and socioeconomic information, the CHARLS collects comprehensive information on individual health, facilitating multidimensional and multilevel analyses (Zhao et al., 2014).
This article uses micro-panel data publicly available from the CHARLS for 2013, 2015, and 2018. We retain samples of individuals aged 60 and above from rural areas, exclude samples with missing data in key variables, and get a total of 7500 penal samples for the three surveys. It should be noted that the CHARLS questionnaire investigated the elderly’s reception of community-based home care services only in 2018. Of the 2500 respondents, 629 received the services, and 1871 did not. We use the 2013, 2015, and 2018 data to examine the effects of community-based home care on the health of the rural elderly. The year 2018 serves as the experimental period, 2015 as the base period, and 2013 as the base period for robustness testing. The 2013 and 2015 samples are grouped according to individuals’ reception of community-based home care in 2018.
Dependent Variables: Building on the existing research, both the physical and mental health states of the rural elderly are assessed. Physical health consists of ADL and IADL, while mental health includes levels of depression, positive emotions, and negative emotions.
ADLs are the fundamental measurement of the elderly’s health status, including 6 activities: dressing, bathing, eating, transferring (getting in and out of bed), toileting, and continence. IADLs refer to the 6 activities: housekeeping, preparing meals, shopping, making phone calls, taking medications, and managing finance. The answer “not difficult” to the scale questions scores 0 points; “difficult but can still manage” scores 1 point; “difficult and in need of assistance” scores 2 points; “unable to complete” scores 3 points. The scores of the 6 ADL questions and 6 IADL questions are then summed to measure the elderly’s physical health.
Positive emotions are measured by two questions, “hopeful about the future,” and “feeling happy.” The answer “rarely or never” scores 0 points; “not often” scores 1 point; “sometimes or half the time” scores 2 points; “most or all the time” scores 3 points.
Negative emotions are measured by eight questions, “worried by trivial things,”“trouble concentrating on what I was doing,”“feeling depressed,”“feeling that everything was difficult,”“feeling fearful,”“bad sleep,”“feeling lonely,” and “feeling unable to continue my life.” The answer “rarely or never” scores 0 points; “not often” scores 1 point; “sometimes or half the time” scores 2 points; “most or all the time” scores 3 points.
Depression level is measured by the two questions for positive emotions and three questions for negative emotions combined. These 10 questions come from the Center for Epidemiologic Studies Depression Scale (CES-D scale). When calculating the depression level, we reverse the scale of the 2 positive questions “hopeful about the future,” and “feeling happy,” so that the answer “rarely or never” scores 3 points; “not often” scores 2 points; “sometimes or half the time” scores 1 point; “most or all the time” scores 0 points. The scale of the 8 negative questions remain unchanged, and the depression level is the sum of the scores of the 10 questions.
Core explanatory variable: Participation in community-based home care. It is a dummy variable based on the question “Have you enjoyed the following community-based home care ?” The community-based home care includes daycare, nursing homes, meals, regular health check-ups, home visits by medical staff, home hospitalization, community nursing, health management, and recreational activities. If a respondent has received one or more of the services, the variable is assigned the value of 1; otherwise, the value of 0 is assigned.
Additionally, we further categorize explanatory variables based on individual responses. Selecting options of “daycare, nursing homes, meals,”“community nursing,” or “health management” indicates receiving daily care services of community-based home care; choosing options of “regular health check-ups,”“home visits by medical staff,” or “home hospitalization” means receiving regular medical services; choosing the option of “recreational activities” indicates receiving recreational services.
Control Variables: Besides the socio-demographic variables, this article also controls for individuals’ family characteristics. Socio-demographic variables include age, gender, education, ADL, IADL, and the number of chronic illnesses. Family characteristics refer to living with a spouse, household income, pension insurance, medical insurance, distance of children’s residence, family caregiving, and province. Descriptive statistics for the variables used in this article are presented in Table 2.
Descriptive Analysis of Variables.

Source. Compiled by the authors from official data.
Descriptive statistics
Overview
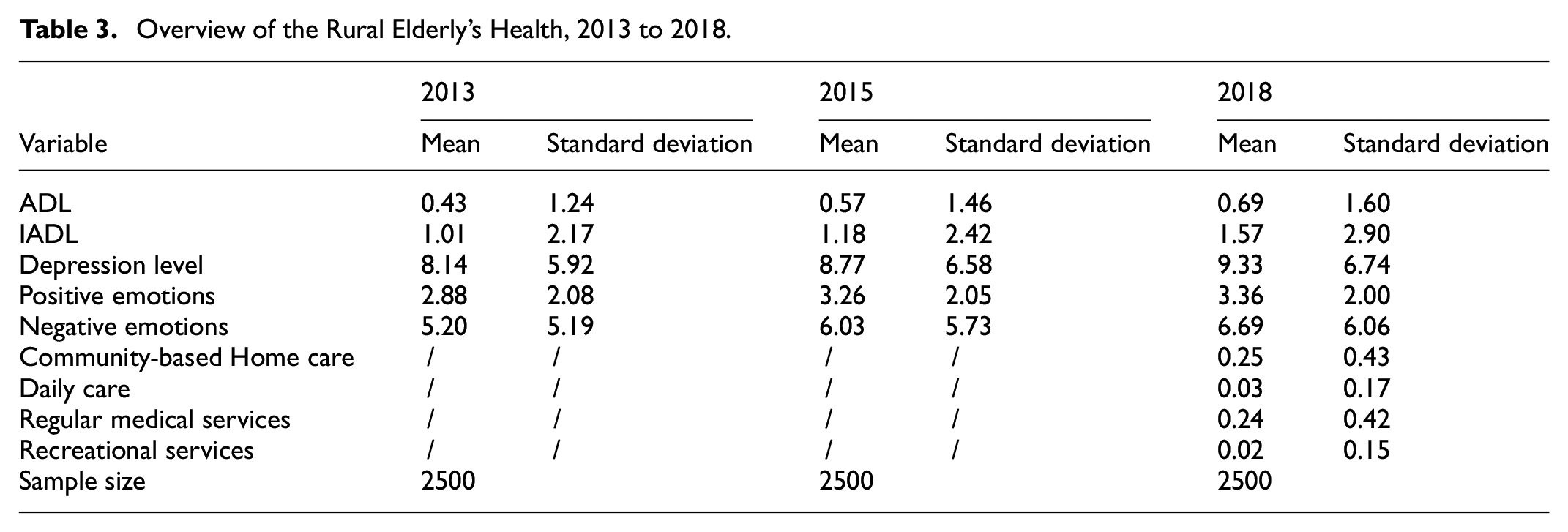
Table 3 describes the health status of the rural elderly in 2013, 2015, and 2018, and their participation in community-based home care in 2018. Their ADL, IADL, depression level, positive emotions, and negative emotions all reflect a rising trend over the years. Specifically, from 2013 to 2018, their ADL increased from 0.43 to 0.69, IADL from 1.01 to 1.57, depression level from 8.14 to 9.33, positive emotions from 2.88 to 3.36, and negative emotions from 5.20 to 6.69. In the sample, 25% of the elderly received community-based home care. To be specific, the elderly receiving daily care, regular medical services, and recreational services account for 3%, 24%, and 2% of the total sample, respectively. That reflects the worrisome health condition of the rural elderly, and the limited coverage of community-based home care, especially in the case of daily care and recreational services.
Overview of the Rural Elderly’s Health, 2013 to 2018.
Description of key variables
We classify the rural elderly into two groups based on their reception of community-based home care. Table 4 provides a statistical analysis of the health of the two groups, for the years 2013, 2015, and 2018. The table demonstrates the disparities between these two groups and how these disparities change before and after participation in community-based home care. For the group that receives community-based home care, its scores for ADL, IADL, depression level, and negative emotions are significantly lower than those of the other group, and its score for positive emotions is significantly higher than that of the other group. All parameters reach a significance level of 1%. This indicates that community-based home care has a positive impact on the rural elderly’s health.
Description of Key Variables, 2013 to 2018.

Note. 1. The table reports means and standard deviations. Values in parentheses are standard deviations. 2. The asterisks (*) denote the significance level of the t-test for a specific variable between the two sample groups for the corresponding year. ***, **, and * represent significance levels of 1%, 5%, and 10%, respectively.
Results of Econometrics Analysis
The Impact of Community-based Home Care
Table 5 shows the influence of community-based home care on the rural elderly’s physical and mental health. Control variables are added in turn to the regression analysis in this article to see whether they lead to changes in results. In the first column, only individual characteristics, family characteristics, and province dummy variables are controlled for, and in the ensuing three columns, institutional safeguards, physical characteristics, and family caregiving variables are added in turn. Table 5 shows that the regression results in the four columns do not differ significantly. Therefore, this article primarily observes the regression results in the fourth column.
The Impact of Community-Based Home Care on the Rural Elderly’s Health, 2015 to 2018.

Note. 1. In parentheses are t-values. 2. ** and * represent significance levels of 5%, and 10% respectively. 3. Physical/mental health refers to the control for mental health influence in the regressions of ADL and IADL, and the control for physical health influence when analyzing depression level, positive emotion, and negative emotion. The same applies in our subsequent analysis. 4. The same control variables are applied to the regressions in the same column. 5. Yes/no indicates whether the variable is controlled for.
Community-based home care results in a significant decrease of 0.16 points/person and 0.33 points/person in the ADL and IADL of the rural elderly, and the corresponding parametric tests reach a significance level of 5%. Additionally, community-based home care significantly reduces the rural elderly’s depression level and negative emotions by 0.66 points/person and 0.56 points/person, respectively, both passing parametric tests at a significance level of 10%. The results show that community-based home care allows the rural elderly to receive daily care, emotional support, and recreational services without leaving the familiar environment. This improves both their physical health and mental well-being. Hypothesis 1a and Hypothesis 1b are validated.
Robustness Tests
Robustness tests aim to assess whether a statistical model remains relatively stable in case of changes or disturbances. In particular, the balance test of PSM is designed to ensure no significant differences in key covariates between the treatment and control groups, thus avoiding bias due to poor sampling. It helps to ensure the reliability and validity of the experimental results. Besides, sensitivity analysis is used to observe the changes in the results and identify the factors that have the greatest impact on the results by altering multiple uncertainties that may affect the results during the analysis process. The model may also be affected by external disturbances, such as policy changes. The robustness test simulates these disturbances factors to evaluate the model’s resilience in response to these changes. Therefore, this paper ensures the reliability of the research by the balance test of PSM, sensitivity analysis, and the exclusion of interferences of preexisting policies.
Balance Test of PSM
Figure 1 illustrates the distribution of absolute deviations before and after matching for the base and experimental periods. It shows that the variables’ standardized deviations decrease after matching. We run a balance test on the matching results and find all of the deviations are less than 10%.

Balancing variables after matching.
Sensitivity analysis
When running PSM-DID, the outcomes of kernel matching may be influenced by the choice of bandwidth intervals, for different intervals may lead to varying estimation results. We perform a sensitivity analysis using intervals of (0.02, 0.04, 0.08, 0.1) and find that the estimations are robust (see Table 6).
A sensitivity Analysis of the Impact of Community-based Home care on the Rural Elderly’s Health.

Note. 1. In parentheses are t-values. 2. ** and * represent significance levels of 5% and 10% respectively.
Regression by year
To explore the impact of community-based home care on the health of the rural elderly, this article applies Ordinary Least Squares (OLS) estimation to data for 2015 and 2018 respectively. The results are presented in Table 7.
OLS Results by Year.

Note. 1. In parentheses are t-values. 2. ** represents significance level of 5%. 3. Yes/no indicates whether the variable is controlled for. 4. The table presents the two OLS regression results for 2015 and 2018.
Row 1 and Row 2 of Table 7 present the estimated impact of community-based home care on the rural elderly’s health in 2015. The reception of community-based home care in 2015 has no significant influence on the physical and mental health of the rural elderly. Rows 3 and 4 report the estimated impact of community-based home care on the health of the rural elderly in 2018. In the 2018 estimations, receiving community-based home care leads to a significant decrease of 0.14 points/person in ADL, 0.28 points/person in IADL, and 0.59 points/person in depression level among the rural elderly, with parametric tests reaching a significance level of 5%; it also results in a significant increase of 0.21 points/person in positive emotions, with the parametric test reaching a significance level of 5%; but it has no significant impact on the negative emotions of the rural elderly. At this point, community-based home care has enhanced the rural elderly’s physical and mental health. There was no difference in the health of individuals who received the care and those who did not before the policy was implemented, and the gap emerged only after the policy implementation. This justifies the choice of 2015 as the base period.
Interferences of Preexisting Policies
In 2013, the State Council released Opinions on Promoting the Development of the Elderly Care Industry, which promises policy support to elderly care facilities and companies around this industry, so as to meet the demand of an aging population (The State Council, 2013).
Table 8 demonstrates the impact of community-based home care services on the rural elderly’s health, using 2013 as the base period and 2018 as the experimental period. The services result in a significant decrease of 0.21 points/person in ADL, with the parametric test reaching a significance level of 1%. Therefore, receiving the services has a significant impact on their physical health. The effect of community-based home care is mitigated by other related policies.
PSM-DID Results Excluding the Interferences of Other Policies.
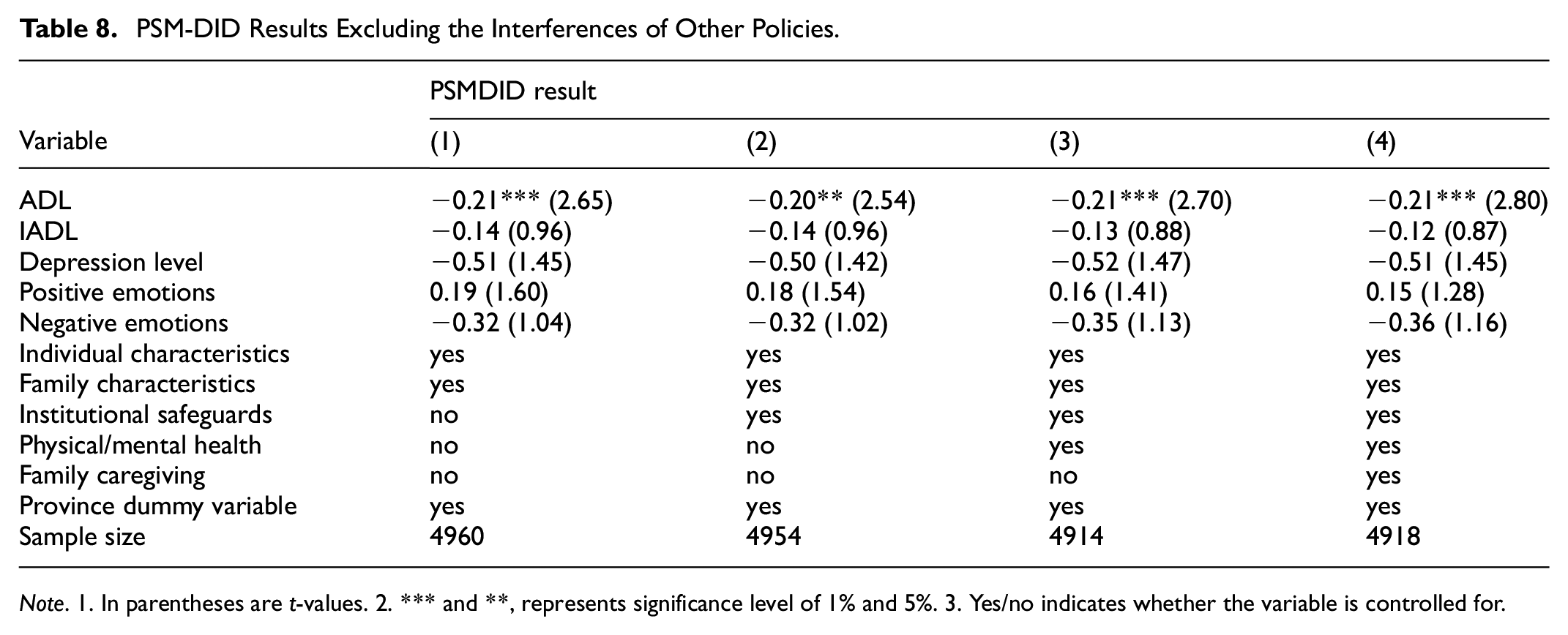
Note. 1. In parentheses are t-values. 2. *** and **, represents significance level of 1% and 5%. 3. Yes/no indicates whether the variable is controlled for.
Impact of Different Types of Community-based Home Care
Our above analysis indicates that community-based home care significantly improves the health of the rural elderly. In this section, we further our investigation to identify the specific types of community-based home care that influence the health of the elderly. The results are shown in Table 9.
PSM-DID Results by Types of Care.
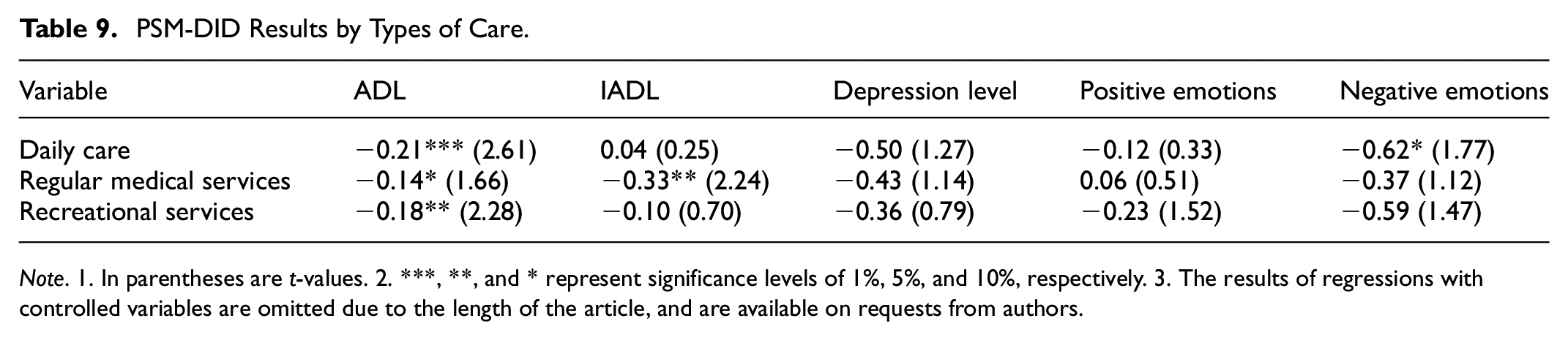
Note. 1. In parentheses are t-values. 2. ***, **, and * represent significance levels of 1%, 5%, and 10%, respectively. 3. The results of regressions with controlled variables are omitted due to the length of the article, and are available on requests from authors.
The first two rows of Table 9 report the estimated impact of daily care on the physical and mental health of the rural elderly in the first two rows. Daily care reduces the ADL by 0.21 points/person, with the parametric test reaching a significance level of 1%; it also lowers negative emotions by 0.62 points/person, with a parametric test reaching a significance level of 10%. This indicates that daily care assists the elderly in their daily life, and also offers them emotional support, thereby enhancing their physical and mental health. Hypothesis 2a is validated.
Rows 3 and 4 of Table 9 reflect the estimated impact of regular medical services on the physical and mental health of the rural elderly. Regular medical services reduce the ADL by 0.14 points/person and the IADL by 0.33 points/person, with parametric tests reaching significance levels of 10% and 5%, respectively. This indicates that regular medical services such as regular health check-ups, and home visits by medical staff enhance the physical health of the elderly, but have no significant impact on their mental health. Hypothesis 2b is partially validated.
Rows 5 and 6 of Table 9 present the estimated impact of recreational services on the physical and mental health of the rural elderly. Recreational services reduce the ADL by 0.18 points/person, with a parametric test reaching a significance level of 5%. The elderly’s participation in recreational activities organized by the community, such as playing chess and reading, along with interactions with neighbors, effectively trains their mental and physical agility, thereby improving their physical health. Hypothesis 2c is partially validated.
This paper utilizes CHARLS data to explore in depth the positive effects of community-based home care services on the health of rural older adults, and finds that its diversified service model is effective and robust in improving older people’s physical and mental health. This provides empirical evidence for further optimizing the content and improving the quality of community-based home care services, and emphasizes the importance of customizing services for different health needs.
Conclusion
In recent years, more and more scholars have been focusing on community-based home care services. Some scholars have found that community-based home care services can improve the life satisfaction of Chinese older adults, and that the positive effects of spiritual and cultural services and reconciliation and legal services are more obvious than those of life care services and medical care services. However, that article lacks an in-depth discussion and analysis of how community-based home care services specifically affect the physical health of older adults (Zhang et al., 2022). Other scholars have found that community-based home care services can significantly improve older adults’ self-reported health, and this effect is more pronounced for older adults who are under the age of 80, have functional impairments, do not have chronic illnesses, have never attended school, live in low-income households, are single, and have few interactions (He et al., 2023).
This article uses the CHARLS data to investigate the impact of community-based home care on the rural elderly’s health, and delves into specific types of community-based home care to reveal their mechanisms and variations in influence. Empirical results indicate: (a) Community-based home care significantly improves the physical health of the rural elderly, for after receiving the services, ADL and IADL scores decrease significantly. (b) Community-based home care significantly improves the mental health of the rural elderly and reduces their likelihood of depression. (c) Daily care improves both the physical and mental health of the rural elderly; regular medical and recreational services enhance the physical health of the rural elderly, but do not show a significant impact on their mental health.
Based on the abovementioned conclusions, this article provides the following advice. First, local civil departments should improve China’s community-based home care policy. This includes improving collective planning, strengthening national policy support, and providing services to the rural elderly tailored to the local economic and social conditions, to optimize resource allocation and avoid waste. Second, local publicity departments should promote community-based home care in rural areas using various media such as television, the Internet, and WeChat official accounts, to acquaint the rural elderly with the content and value of community-based home care. This would enhance their trust in and acceptance of the services, and thereby the effectiveness of implementation. Third, encourage more social actors, such as cooperatives, mutual assistance organizations, and special enterprises incorporated to promote rural development, to participate in the establishment and operation of elderly care facilities. Meanwhile, the government should provide subsidies for facility construction, financing, operation, and taxation to support the development of community-based home care services.
This article has academic value and policy significance. Theoretically, this article analyzes the impact of community-based home care services on the health of the rural elderly and its mechanism and discerns the influence of each functional service. Besides, the results of this article advise public policy to integrate the rural old-age resources and provide the rural elderly with more targeted elderly services.
However, this article has the following limitations. As the data used in this article comes from the public database CHARLS, they only investigated the participation of the elderly in community-based home care services in 2018, unable to assess the long-term effects. More data sources will be explored in the future, and more flexible and dynamic criteria will be considered to classify village elderly care facilities to reflect their changes over time and accurately assess the long-term effects.
Footnotes
Ethical Considerations
An ethics statement is not applicable to this research, because it uses publicly available data, and does not carry out experiments or surveys.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Natural Sciences Foundation of China (72003177); Philosophy and Social Science Planning Special Project titled “Youth of Zhijiang Program” of Zhejiang Province (24ZJQN045YB)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.