
Abstract
As the prevalence rates of eating disorders and disordered eating behaviors continue to rise worldwide, it is crucial to make psychometrically validated tools available for clinical use. The current study examined the psychometric properties of the Arabic versions of the Eating Disorder Examination Questionnaire (EDE-Q) and the Clinical Impairment Assessment (CIA) using a sample from the clinical population. The sixth edition of the EDE-Q and the third edition of the CIA were translated into Arabic and administered to 260 Arab participants (203 diagnosed with eating disorders and 57 from the general population) who are natives of various countries in the Middle East and North Africa (MENA) region. Convenience sampling method was used to recruit the participants with a 97% response rate. Participants from the non-clinical group also filled out the Arabic version of the EAT-26 questionnaire to rule out underlying disordered eating behaviors. Data was collected between June 2018 and August 2023. Internal consistency for the global scores of both the EDE-Q and CIA were high, while the coefficients for the four subscales of the EDE-Q and the three subscales of the CIA were moderate. Confirmatory factor analysis on the EDE-Q revealed a good fit for the abbreviated seven-item measurement with three factors, and the same was true for the CIA’s three-factor model. Convergent validity results showed significant correlations between the EDE-Q and the CIA with high coefficients. Known groups validity tests revealed significant differences based on eating disorder behaviors, where those who reported vomiting episodes and laxative misuse scored significantly higher on the EDE-Q than those who did not, and those who reported excessive exercising behavior scored significantly higher on the CIA than those who did not. There were no significant differences observed based on eating disorder diagnoses, nor were there differences among individuals with secondary diagnoses. Test-retest reliability and discriminant validity tests were not carried out. Strengths, limitations, and future directions are thoroughly discussed. The study investigated the reliability, validity, and factor structure of these tools. The findings corroborate previous studies’ support for the EDE-Q’s abbreviated seven-item measurement with three factors and the CIA’s three-factor model. With a comparatively modest sample size, the findings should be considered preliminary for Arabic versions of the tools using a clinical sample, and future studies with larger sample are warranted to confirm them.
Plain language summary
In this study, the authors wanted to see if two questionnaires commonly used to understand eating disorders work well when translated into Arabic and used with Arabic-speaking people. They tested the questionnaires on 260 Arab participants, some diagnosed with eating disorders and some from the general population. They found that the questionnaires generally showed good validity, meaning that they measure what they are supposed to measure. However, the study had some limitations, including a relatively small sample size, so more research with larger groups is needed to be sure these findings are accurate. Overall, the study suggests that these translated questionnaires could be useful tools in Arabic-speaking communities for identifying and understanding eating disorders.
Keywords
Introduction
Despite the prevalent assumption that the Western concept of the thin ideal does not exist in other cultures, review studies on the point prevalence and incidence rate of eating disorders (EDs) and disordered eating behaviors (DEBs) show an estimated rate between 2% and 54.8% in different parts of the Arab world (Alsheweir et al., 2023; Melisse et al., 2022; Safiri et al., 2022). Globally, the lifetime prevalence rate of EDs among females is 4% and 0.3% among males (Alsheweir et al., 2023). Studies also show that the prevalence of DEBs among Arab adolescents is comparable to that of Western countries (Azzeh et al., 2022). Considered as the native language of this region and as of the year 2023, Arabic is spoken by around 274 million people worldwide (Dyvik, 2023). To make sure that clinical assessments are carried out accurately and appropriate interventions are effectively implemented, translated and validated tools in Arabic are essential (Hamed et al., 2012). This study was designed with the aim of fulfilling this need by translating and validating the Eating Disorder Examination Questionnaire (EDE-Q) and the Clinical Impairment Assessment (CIA). Moreover, this study is the first one in the literature to include a clinical sample when validating the EDE-Q in Arabic as well as the first one ever to validate the CIA in the same.
The EDE-Q is a self-administered questionnaire based upon the full-length investigator-based interview known as the EDE, used to assess eating disorder psychopathology (Fairburn & Beglin, 1994, 2008; Fairburn et al., 2008). Several studies have demonstrated a significant relationship between the EDE and EDE-Q (Fairburn & Beglin, 1994; Mond et al., 2004a; Sysko et al., 2005). The EDE-Q is widely used across the world due to its practicality and has also been validated for online use (Chan & Leung, 2015).
The EDE-Q has four subscales contributing to a global score: Restraint, Eating Concern, Shape Concern, and Weight Concern. It is designed to assess the severity of eating disorder psychopathology including behavioral features such as binge eating, self-induced vomiting, laxative misuse, and excessive exercising. The psychometric properties of EDE-Q have been investigated across several studies, whereby significant differences between clinical groups and their non-clinical counterparts were detected (Aardoom et al., 2012; Berg et al., 2011, 2012; Elder et al., 2006; Englelsen & Laberg, 2001; Mond et al., 2004b; Ro et al., 2015). The EDE-Q has also shown high internal consistency (Luce & Crowther, 1999; Reas et al., 2005; Rose et al., 2013), temporal stability (Bardone-Cone & Bond, 2007; Mond et al., 2004a; Peterson et al., 2007), convergent validity (Mond et al., 2004a; Reas et al., 2010) and sensitivity to change over time (Sysko et al., 2005).
The EDE-Q has been translated into several languages and validated for use in Swedish (Mantilla et al., 2017), Spanish (Villarroel et al., 2011), Italian (Calugi et al., 2017), Greek (Giovazolis et al., 2012), German Aardoom et al., 2012), Fijian Becker et al, 2010a), Norwegian (Reas et al., 2011; Ro et al., 2010, 2015), Malai (Taib et al., 2021), Turkish (Yucel et al., 2011), Portuguese (Machado et al., 2014), Mexican (Penelo et al., 2013), and Korean (Bang et al., 2018). Most recently, two studies from Saudi Arabia (Aldubayan et al., 2023; Melisse et al., 2022) were published using sample from the general Saudi population. The study by Aldubayan et al. (2023) included 549 Saudi nationals from the general population and conducted confirmatory factor analysis (CFA) using the entire sample first, and exploratory factor analysis (EFA) and a second CFA after splitting the data for convergent validity. Their findings revealed a good fit for a three-factor model with 14 items, similar to the Malai (Taib et al., 2021), Korean (Bang et al., 2018), and Swedish (Mantilla et al., 2017) versions. The study by Melisse et al. (2022) on the other hand, had a larger sample of 2,690, also from the general Saudi population. Their model did not reveal a good fit for the original four-factor model, but the primary contribution of their study was obtaining discriminant validity for the EDE-Q as a screening tool for Saudi nationals at risk of having an ED. There are several factors that make the current study unique; firstly, it is the first from the region to validate the EDE-Q in Arabic by involving samples from both the general as well as the clinical population, consisting of individuals diagnosed with an ED. Secondly, unlike the studies by Aldubayan et al. (2023) and Melisse et al. (2022), which included a homogenous sample of Saudi nationals and only from the general population, the current study involved a heterogeneous sample from several countries in the Middle East and North Africa (MENA) region, in both the clinical sample and the general population. Furthermore, the current study carried out known-groups validity test to assess differences among the sample based on eating disorder related behaviors, which the two studies from Saudi did not. To our knowledge, no previous studies have validated the EDE-Q in Arabic using a clinical sample representing various countries from the MENA region.
The CIA is a 16-item self-report questionnaire that focuses on the health status of a person in a given 28-day period and measures the severity of psychosocial impairment caused by eating disorders (Bohn et al., 2008). It is used in the clinical assessment of patients before and after treatment for eating disorders, evaluating impairment in domains of life that are typically affected by eating disorder psychopathology: mood and self-perception, cognitive functioning, interpersonal functioning and work performance. The CIA provides a single index of the severity of psychosocial impairment and is used alongside measures of eating disorder features such as the EDE-Q, typically completed immediately after filling out the latter. This protocol is put in place by Fairburn and Beglin (1994) to ensure that patients are actively contemplating their eating disorder features while filling out the CIA.
Several studies have documented using the CIA in clinical settings and it has also been translated into different languages across the world, including in Persian (Mahmoodi et al., 2016), Fijian (Becker et al., 2010b), Italian (Calugi et al., 2018), Spanish (Martin et al., 2015), Swedish (Welch et al., 2011), and Norwegian (Dahlgren et al., 2017). Moreover, a study using a UK sample demonstrated good psychometric properties of the CIA (Jenkins, 2013), and in women at high risk of eating disorder onset (Vannucci et al., 2012). To our knowledge, no previous studies have translated and validated an Arabic version of the CIA.
Due to the universal prevalence of eating disorders, the tools’ applicability in screening and diagnosis of eating disorders, and their potential usage for clinical and research purposes, the current study was designed to translate and validate the EDE-Q and CIA in an Arabic-speaking population, assessing the psychometric properties of the two questionnaires.
Method
Forward-Backward Translation Process
An expert team was set up to carry out the translation and psychometric validation process, utilizing procedures recommended by the World Health Organization (WHO, 2020). It was ensured that the procedure used is consistent with developed guidelines and standards (Saklofske et al., 2013). The team was comprised of the following members:
(1) The original developers of the tools (consulted for permission to translate and validate the tools)
(2) Four healthcare professionals familiar with the tools within clinical settings
(3) Two research professionals with background in psychology and research methods
(4) One professional translator not familiar with the tools
Steps
The EDE-Q and CIA underwent careful forward-backward translations. The team ensured the translators’ mother tongue was the target language, and the literary standard across the MENA region known as Modern Standard Arabic (MSA) was chosen as the single Arabic dialect. All steps of the translation process were documented, and are summarized below:
(1) Forward-translation—This was done by two translators with Arabic as their mother tongue and who are also familiar with the contents of the tools, and a third translator from a professional translating service who is not familiar with the contents.
(2) Backward-translation—The three sets of translations were synthesized by three translators, two of whom have Arabic as their mother tongue, and one fluent in MSA, to produce one final version out of the three. One of the translators was blinded to the original versions of the tools.
(3) Cognitive interviews—To ensure content validity, five randomly-selected individuals were asked to complete the questionnaires and were interviewed about the meaning of each item. This was done to ensure the respondents interpreted the items in the manner intended by the developers/translators of the instruments. These participants have Arabic as their mother tongue. They were debriefed and asked what they thought the questionnaires were asking, whether they could repeat the questions with their own words, what came to their mind when they heard a particular phrase or term, and how they chose their answers.
Participants
The study was reviewed and granted ethics approval by the Institutional Review Board at the private clinic where participants for the clinical group were recruited. A total of 260 participants were included in the study, comprising of individuals with an eating disorder diagnosis and from the general population. Data was collected between June 2018 and August 2023. For the clinical group, a total of 203 individuals (183 females, mean BMI 26.7 ± 8.8) meeting the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM–5; American Psychiatric Association, 2013) diagnostic criteria for eating disorders were recruited from a private outpatient clinic for psychiatric and neurological disorders in the United Arab Emirates (UAE). The clinic caters for citizens and foreign residents diagnosed with various neuropsychiatric disorders.
The participants from the clinical group were approached for consent to participate during their first consultation visit to the clinic. For individuals under the age of 18, written informed assent of the participants and written informed consent of their parents/guardians were obtained prior to the start of participation. The youngest participant in the clinical group was 16 years of age. Clinical psychologists carried out clinical interviews to screen for underlying disordered eating behaviors and to perform the diagnoses. There were four categories under primary diagnoses, for which 48 (18.5%) of the participants met the criteria for anorexia nervosa, 97 (37.3%) for binge eating disorder, 33 (12.7%) for bulimia nervosa, and 25 (11.5%) for other unspecified eating disorders. Ninety three out of the 203 individuals in the clinical group had secondary diagnoses of mainly psychiatric disorders; 34 (16.7%) were diagnosed with major depressive disorder, 39 (19.2%) with general anxiety disorder, 11 (5.4%) with obsessive compulsive disorder, 5 (2.4%) with bipolar disorder, 2 (0.98%) with adjustment disorder, and 2 (0.98%) with obesity. Table 2 displays more details on the characteristics of the clinical group.
Using convenience sampling strategy and with a 97% response rate, a total of 164 individuals (F = 149) were approached for participation from the general population for the non-clinical group. These individuals were approached at various community settings, such as universities, shopping malls, and public parks. They were first provided with the Arabic version of the EAT-26 questionnaire (Haddad et al., 2021) to rule out any underlying (undiagnosed) eating disorders. After screening, only 57 individuals (43 females, mean BMI 24.9 ± 5.1) met the criteria for inclusion in the final analysis, as the remaining 107 scored ≥20 on the EAT-26 questionnaire, indicating an underlying (undiagnosed) disordered eating behaviors. There were no participants below the age of 18 in the non-clinical group.
The majority of participants in both groups were female (Total: 226; clinical group: 183; non-clinical group: 43) while there were 20 males in the clinical group and 14 in the non-clinical group. Tables 1 and 2 have further details on the demographic characteristics of both groups as well as the clinical characteristics of the clinical group.
Demographic and Baseline Characteristics of the Clinical and Non-Clinical Groups

Clinical Diagnoses and Eating Disorder Behaviors of the Clinical Group.

Inclusion Criteria
Clinical group:
(a) Diagnosis of eating disorder using the DSM-5 (5th ed.; American Psychiatric Association, 2013) diagnostic criteria
(b) Age 16 and above
(c) Assent/consent to participate in the study
Non-clinical group:
(a) A score of ≤20 on the Arabic EAT-26 questionnaire
(b) Age 16 and above
(c) Assent/consent to participate in the study
Measures
The Eating Disorder Examination Questionnaire (EDE-Q)
The Arabic translation of the original EDE-Q (v.6.0, Fairburn & Beglin, 2008) was administered to both groups. The EDE-Q is a 28-item self-administered questionnaire used to assess eating disorder psychopathology in the last 28 days from the date of administration. It also assesses the frequency of binging and purging behaviors associated with an eating disorder diagnosis. The scale generates one global score and four subscale scores, namely, restraint, eating concern, weight concern, and shape concern. The scores range from 0 to 6, where higher scores indicate greater psychopathology.
The Clinical Impairment Assessment Questionnaire (CIA)
The Arabic translation of the original CIA (v.3.0, Bohn et al., 2008) was used to assess impairment due to an eating disorder psychopathology using three specific subscales, namely, personal, social, and cognitive. The 16-item self-administered questionnaire generates one global score using a 4-point Likert scale, with scores ranging from 0 to 48, where higher scores indicate greater severity of impairment.
The Eating Attitudes Test (EAT-26)
The Arabic version of the EAT-26 (Haddad et al., 2021) was administered only to the non-clinical group to screen for any underlying eating disorder. Items 1 to 25 are scored with values of 3 for “Always,” 2 for “Usually,” 1 for “Often” and 0 for other responses. Item 26 is scored in the opposite direction of the former. The total score is obtained by adding the scores for all items. Possible scores on the scale range between 0 and 78, and a cutoff score of ≥20 was used as an exclusion criterion, indicating a suspected underlying eating disorder.
Statistical Analysis
Data analyses were carried out using IBM SPSS v.22 (IBM Corp, 2013) and MPlus (Muthén & Muthén, 2015), and a significance level of α = .05 was adopted to interpret the results. Internal reliability tests were carried out to calculate the McDonald’s Omega values (ω) for the EDE-Q as well as the CIA. The relationship between the four subscales of the EDE-Q and the three subscales of the CIA were assessed using Spearman’s correlation coefficients. The same was done to observe the relationship between the EAT-26 and the CIA among the non-clinical group. Factor structure was calculated using Confirmatory Factor Analysis (CFA) in the clinical group. CFA was calculated using MPlus (Muthén & Muthén, 2015). For the CIA, a general factor model including one factor was tested first, followed by a three-factor model using the proposed subscales: personal, social, and cognitive (Bohn et al., 2008) was tested. For the EDE-Q, three different models were tested, in accordance with previous research. Firstly, a general factor model with all items loading on one factor was tested. Secondly, a four-factor model using the proposed subscales (Fairburn & Beglin, 1994) restraint, eating concern, shape concern and weight concern was tested. Third, an abbreviated seven-item measurement with three-factors (dietary restraint, shape/weight over evaluation, body dissatisfaction) was tested, as proposed by previous research using the EDE (Grilo et al., 2010). The seven-item measurement was chosen because it showed an acceptable model fit in a previous translation study (Calugi et al., 2017). For model estimation WLSMV (weighted least-squares means and variance) was used for the CIA and MLMV (maximum likelihood estimator, mean- and variance-adjusted) for the EDE-Q. Since the CIA only involved a 4-point-Likert-Scale rating for each item, an estimator for ordered categorical items was deemed more suitable. The EDE-Q on the other hand uses a 7-point-Likert-Scale rating, so a mean and variance adjusted maximum likelihood parameter, which is robust to non-normality, was used. For model evaluation recommended model fit indices were used (Hu & Bentler, 1999): CFI (comparative fit Index) and TLI (Tucker-Lewis index) > 0.90, RMSEA (root-mean-square error of approximation) < 0.06 and SRMR (standardized root mean square residual) < 0.08. After running normality tests and observing assumptions of normality were not met, convergent validity was assessed using Spearman’s correlation coefficients to evaluate the association between the four EDE-Q subscales and the three CIA subscales. Discriminant validity was not carried out due to the disproportionate distribution of participant numbers in the two groups. Test-retest reliability was also not carried out since only nine individuals from the clinical group completed the two questionnaires at two intervals of time.
Results
Table 1 displays the baseline demographic characteristics of participants from both the clinical (203) and non-clinical (57) groups. Table 2 has details on the clinical group’s diagnoses and eating behaviors.
Assumptions of Normality Distribution
Normality tests were carried out for both groups, and the results showed that the data for both groups were not normally distributed (Kolmogorov–Smirnov test, p < .05, Shapiro–Wilk test, p < .05). Based on these results, we carried out non-parametric tests wherever applicable, as shown below.
Internal Reliability
For the EDE-Q, the McDonald’ Omega values showed excellent internal consistency (ω = .919) for the global EDE-Q and moderate to high internal consistency for the subscale scores. The Spearman’s correlation coefficients between the four subscales were all highly significant (p < .001). The Omega (ω) values ranged from .61 between subscales 1 and 2 to .81 between subscales 1 and 4.
The same was true for the CIA, with excellent internal consistency overall (ω = .973). The Spearman’s correlation coefficient scores were all significant (p < .001) and the scores ranged from .78 between the personal and cognitive domain to .93 between the social and cognitive domain. Table 3 shows further details on the Omega (ω) values for both the EDE-Q and the CIA.
Internal Reliability Test Scores of the Clinical Group on the EDE-Q and CIA (n = 203).

Confirmatory Factor Analysis
The CFA for the EDE-Q general factor model (χ2(189) = 430.332, p < .001) showed poor model fit in all goodness-of-fit indices: CFI = 0.324, TLI = 0.270, RMSEA = 0.085, SRMR = 0.148. Similarly, the four-factor model (χ2(185) = 251.345, p < .001) using the proposed four subscales showed poor model fit: CFI = 0.610, TLI = 0.557, RMSEA = 0.073, SRMR = 0.130. The seven-item abbreviated measurement with three-factors (χ2(11) = 12.325, p = .34) on the other hand showed good model fit: CFI = 0.985, TLI = 0.971, RMSEA = 0.042, SRMR = 0.048. Intercorrelations between the three subscales were allowed in the model. The standardized factor loadings and the p-values for the seven-item abbreviated measurement model are shown in Table 4.
Factor Loadings for EDE-Q Abbreviated Seven-Item Measurement Model.

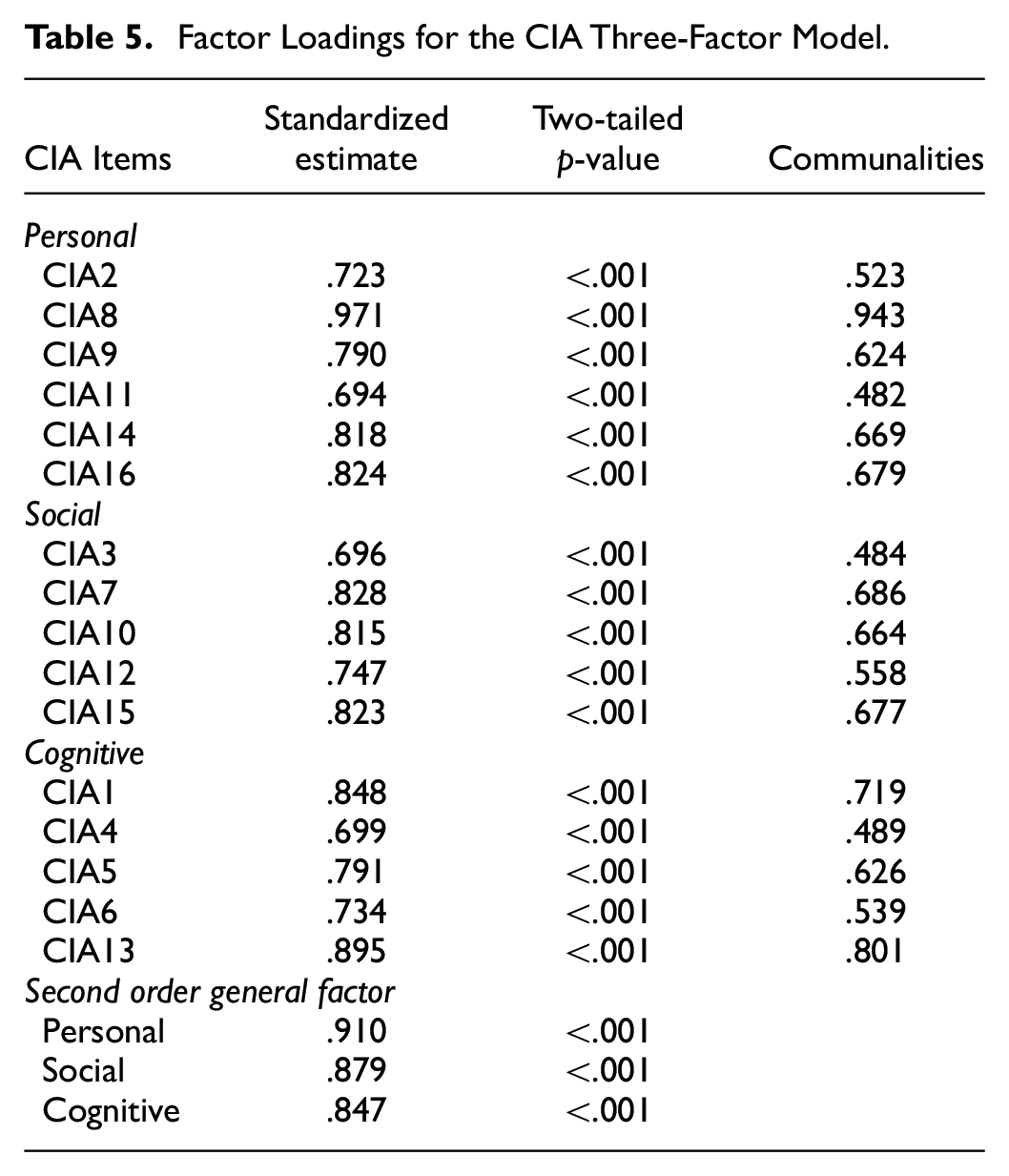
The CFA for the CIA one factor model (χ2(104) = 191.108, p < .001) showed considerably good model fit for the CFI and TLI: CFI = 0.926, TLI = 0.915. The RMSEA, on the other hand, did not show good model fit: RMSEA = 0.114. The three-factor model (χ2(101) = 143.901, p < .01) including the subscales, showed considerable improvement in the fit indices (CFI = 0.964, TLI = 0.957, RMSEA = 0.081). The standardized factor loadings and the p-values for the three-factor model are shown in Table 5. The SRMR is not available for the WLSMV parameter. Table 6 has the fit indices for the different factor structures.
Factor Loadings for the CIA Three-Factor Model.
Factor Structure and Fit Indices (CFI, RMSEA, TLI) of CFA for the General Factor Model, the Four-Factor Model, and the Seven-Factor Model of the EDE-Q and for the One and Three-Factor Models of the CIA.

Convergent Validity
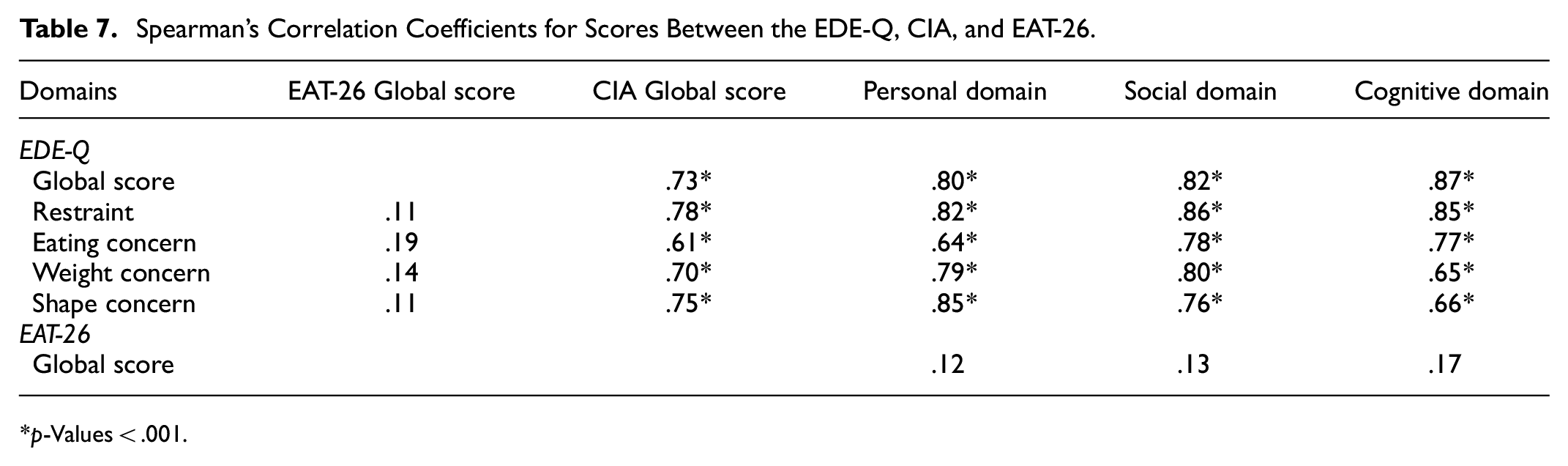
As shown in Table 7, Spearman’s correlation between the EDE-Q and the CIA scores for the entire sample group were all highly significant, with the coefficients ranging from .59 (between the EDE-Q Shape Concern subscale and the CIA Social domain) to .86 (between the EDE-Q Restraint subscale and the CIA Social domain).
Spearman’s Correlation Coefficients for Scores Between the EDE-Q, CIA, and EAT-26.
p-Values < .001.
The same was not true for correlation between the EAT-26 and the CIA among the non-clinical group, where the results were not significant and the coefficients were very low across the three subscales of the CIA (Personal, Spearman’s rho = .12; Social, Spearman’s rho = .13; Cognitive, Spearman’s rho = .17). Similarly, correlation between the EAT-26 subscales and the EDE-Q among the non-clinical group was not statistically significant (Restraint, Spearman’s rho = .11; Eating concern, Spearman’s rho = .19; Weight concern, Spearman’s rho = .14; Shape concern, .11).
Known-Groups Validity
To observe differences among the clinical group in global scores of the EDE-Q and CIA, two Kruskal–Wallis H tests were carried out using primary and secondary diagnoses. For the EDE-Q, although the mean rank for those diagnosed with bulimia nervosa were comparatively higher, there were no statistical differences between the sub-groups, (H (3) = 4.849, p = .183) with a mean rank of 31.1 for those with a diagnosis of anorexia nervosa, 41.62 for those with bulimia nervosa, 37.37 for those with binge eating disorder, and 27.50 for those with unspecified eating disorder. The same was true for the CIA where the results were not significant (H (3) = 1.689, p = .639) with a mean rank of 37.75 for those with a diagnosis of anorexia nervosa, 35.81 for those with bulimia nervosa, 33.16 for those with binge eating disorders, and 29.59 for those with unspecified disorders.
While comparing the global EDE-Q scores based on eating disorder behaviors among the clinical group, the scores were significantly higher (z = 305.0, p < .05) among those who reported vomiting episodes (Mean rank = 42.6) than those who did not (Mean rank = 31.6). There were also significant differences (z = 31.0, p < .05) between those who reported laxative misuse (Mean rank = 56.7) and those who did not (Mean rank = 33.5). There were no significant differences between the groups who engaged in objective bulimic episodes and those who did not, as well as those who practiced excessive exercising and those who did not. On the other hand, when comparing the global CIA scores based on eating disorder behaviors, we found significant differences (z = 167.0, p < .05) only between those who practiced excessive exercising (Mean rank = 47.8) and those who did not (Mean rank = 31.9).
Since the categories for the secondary diagnoses in the clinical group were not proportional in size, we ran a Mann-Whitney U test comparing only two groups: those diagnosed with major depressive disorder and generalized anxiety disorder. The results for the EDE-Q were not significant (z = 70.5, p = .206) indicating no significant difference between those with major depressive disorder (Mean rank = 16.46) and those with generalized anxiety disorder (Mean rank = 12.54). The same was true for the CIA, (z = 84.0, p = .519) indicating no significant difference between those with major depressive disorder (Mean rank = 13.50) and those with generalized anxiety disorder (Mean rank = 15.50).
Discussion
Studies looking at the incidence and prevalence of eating disorders have reported changing trends in recent years, with increasing rates being reported in the Arab region (Hoek, 2016; Pike et al., 2014). The current study was the first to translate into Arabic and test the psychometric properties of the EDE-Q and the CIA using a heterogenous sample from the MENA region involving both clinical and non-clinical groups. We tested the two measures’ internal reliability, construct validity, and factor structure in a real-world setting. The results using data from 260 participants showed strong internal consistency for the global scores of both the EDE-Q and CIA, while the coefficients for the four subscales of the EDE-Q and the subscale for the CIA showed acceptable consistency. These findings are in partial agreement with previous studies for the EDE-Q in Fijian (Becker et al., 2010a), Italian (Calugi et al., 2017), and in a college sample (Rose et al., 2013); for the CIA, the same is true with the Italian version (Calugi et al., 2018), the Spanish (Martin et al., 2015) and on a sample population in the United Kingdom (Jenkins, 2013).
Convergent validity results showed significant correlations between the EDE-Q and the CIA with high coefficients for each correlated item, supporting previous findings for EDE-Q (Aardoom et al., 2012; Mond et al., 2004a; Reas et al., 2011; Welch et al., 2011) as well as the CIA (Calugi et al., 2018; Vannucci et al., 2012). These findings are an indication that the Arabic version of both tools assess similar constructs in determining levels of psychopathology in eating disorders as well as functional impairment resulting from eating disorder psychopathology. Unlike previous studies (Calugi et al., 2018), our findings did not find significant correlations between the CIA and EAT-26 as well as between the EDE-Q and EAT-26 constructs for the non-clinical group, possibly because of insufficient sample size for the group. It is pertinent to mention that 107 out of the initial 164 that filled out the EAT-26 were excluded from the analysis due to high scores indicating suspected underlying disordered eating behaviors.
Similar to previous findings (Allen et al., 2001; Barnes et al., 2012; Calugi et al., 2017) the one-factor and four-factor structures for the EDE-Q showed poor model fit, while the abbreviated seven-item measurement with three factors demonstrated acceptable model fit (Calugi et al., 2017; Grilo et al., 2013, 2015; Welch et al., 2011). Calugi et al. (2017) had similar outcomes in the fit indices for the one and four-factor structures, attributing their results to the fact that the original EDE-Q was not developed using factor analysis. It needs to be addressed at this point that model fit indices are influenced by the amount of items used in the measurement (Cook et al., 2009). Hence, this could be a possible explanation for the comparably better fit of the seven-item measurement compared to the 22-item one. However, given the significant results we achieved on convergent validity using the Arabic abbreviated seven-item measurement with three factors, and seeing how its use would be time-efficient in a clinical setting, it would be of great benefit for future researchers to rerun confirmatory factor analysis using a larger sample from the region to further corroborate our findings.
The CIA factor analysis had significant results demonstrating improved model fit when the three-factor model was used. These results were consistent with previous studies which used the three-factor model (Calugi et al., 2018; Martin et al., 2015) as well as the original study (Bohn et al., 2008). Based on this, we encourage future researchers to investigate this further by using the three subscale scores as opposed to a single global score. If corroborated, these findings could provide clinical practitioners with more nuanced results of psychosocial impairment resulting from eating disorder psychopathology.
An interesting finding from the current study was the higher mean values for weight and BMI reported in both groups, with a relatively higher values for the clinical group. This is accounted for by the fact that the clinical group was predominantly made up of individuals diagnosed with binge eating disorder, bulimia nervosa, and other unspecified eating disorders while only 23.6% of individuals in the group had a diagnosis of anorexia nervosa, of which, 77.1% were of the restricting type. Studies have shown that bulimia nervosa and especially binge eating disorder are more commonly reported in overweight and obese individuals (Kolar et al., 2022). This finding is also consistent with Melisse et al.’s (2022) conclusion, which associates their samples’ higher BMI scores with high obesity rates and maladaptive weight loss strategies among the Saudi population. It is important to note that countries in the Arab Gulf region have one of the highest rates of obesity in the world (Al-Nohair, 2014). Furthermore, although a recently published (Okati-Aliabad et al., 2022) review of obesity prevalence in the Middle East reported a slightly declining trend between 2000–2006 (34.83%) and 2014–2020 (32.85%) for excess weight and a steady rate of 23% for obesity, these rates are still considered too high by global standards. Moreover, reviews of the literature highlight that there is generally poor knowledge and awareness about what constitutes as a healthy diet in the general population (de Ridder et al., 2017) as well as the significant association between impaired eating behaviors and psychosocial health (Cardi et al., 2018; Jones et al., 2020; Murray, 2023). Such findings underscore the importance of spreading awareness and educating the general population on healthy eating habits, dietary control, and emotional and psychological wellbeing.
Another observation was the mean age for both the clinical and non-clinical group were slightly higher than previous reports in similar studies (Calugi et al., 2017, 2018). This is not surprising given the higher incidence rates of bulimia nervosa and binge eating disorder often being reported in overweight and obese individuals, typically occurring later in life than does anorexia nervosa (Bertoli et al., 2016; Marcus & Wildes, 2014; Melisse et al., 2022; Okati-Aliabad et al., 2022). Furthermore, throughout the data collection process, we found that the younger population from Arabic-speaking nations were apprehensive about filling out the questionnaires in Arabic. Reports indicate that there is a noticeable decline in Arabic usage amongst Arab youth, especially in the Gulf region (Al Ramahi, 2017; Bell, 2015). Although the younger generation generally showed preference for the English versions of the tools in clinical settings, it is our hope that Arabic versions will be of use across all ages in the MENA region where Arabic remains the primary language. The higher mean values for age in our groups are also a good compliment to the previously published Saudi-based studies (Aldubayan et al., 2023; Melisse et al., 2022), whose mean values for age were notably lower, hence representing a younger sample population that ours did not.
In terms of cross-cultural differences, symptom recognition of an eating disorder among Arab populations may differ from that of Western populations, upon which the construct was initially defined, and this may potentially obfuscate accurate detection among individuals from different cultures. For example, while food restriction may be atypical among those from primarily secular Western culture or occur at limited times of the year for Western Judeo-Christians (i.e., restricting particular foods during Passover/Lent or on Fridays), complete abstinence from eating and drinking from sunrise to nightfall may be adopted by some observant Muslims as frequently as 2 days per week, with an additional emphasis on minimizing food intake considered normative by some as well. Participants may have spontaneously excluded the report of excessive fasting behaviors that they and/or their families would view as religiously or culturally acceptable, thereby reducing their detection as eating disordered behaviors on some scales. The risk of such Type II error was attenuated in the present study by the inclusion of clinical diagnosis on the basis of DSM-5 (5th ed.; American Psychiatric Association, 2013) criteria by a clinical psychologist, and by the use of the EAT-26 questionnaire among the non-clinical group to rule out any underlying disordered eating behaviors.
The primary strength of this study is the inclusion of a diverse group of individuals representing several nations from the Arab world. Although the sample size was relatively modest and not proportionally distributed across the two groups, quite a few of the 19 countries (Kiprop, 2019) in the MENA region were represented in the sample. Another strength of the study is testing the psychometric properties of both the EDE-Q and the CIA concurrently which showed significant correlations, indicating a strong convergent validity. In practice, potential users of the tools who are interested in switching to the Arabic versions in their clinical practice can now do so, which would not have been the case had they been translated and validated separately at different intervals of time. The study’s confirmatory nature for using the EDE-Q’s abbreviated seven-item measurement with three factors and the CIA’s three-factor model is also another strength, adding to the existing literature of translation and validation of the two tools. While recent studies (Aldubayan et al., 2023; Melisse et al., 2022) have validated the EDE-Q using samples from a homogenous group from the general Saudi population, this study is the first to validate the tool using a sample group from a clinical population comprising of Arab nationals from different parts of the MENA region. As for the CIA, this is the first Arabic translation and validation study allowing for a convenient use of both tools at the same time, which was not previously possible.
There are some limitations to the current study. Firstly, the sample size was not large enough and may have led to detecting false negatives which may otherwise have been significant. This was especially true for the internal reliability tests using the subscales as well as when running known-groups validity tests between individuals with different primary and secondary diagnoses. We recommend future researchers improve on our findings using data from a larger group of participants. Secondly, the study did not carry out discriminant validity due to the disproportionate number of participants in the two groups. Moreover, test-retest reliability test was not carried out due to fewer number of individuals in the clinical group who managed to complete the two questionnaires at two different time intervals. We encourage future researchers to include both tests to confirm the Arabic tools’ discriminant validity and temporal stability by including a much larger sample size from both the clinical and general populations. Thirdly, translation of the tools was performed using the literary standard Arabic across the MENA region, known as Modern Standard Arabic (MSA). However, the Arabic language is highly diverse with utilized vocabularies and word meanings dramatically differing between dialects. The establishment of an Arabic version of these measures using a single dialect may inadvertently suggest to users with less familiarity with the diversity of Arab cultures and languages a uniformity that lacks objective validity. Therefore, briefing users regarding this limitation is incumbent upon clinical practitioners who prefer using Arabic versions of the tools. Fourthly, model fit indices are influenced by the number of items, and this could explain the improved model fit of the EDE-Q seven-item measurement compared to the 22-item one. Future research could compare other EDE-Q short measures regarding their model fit. Lastly, the sample was largely made up of females, and as such, the results cannot be generalized to the overall population of the region.
Overall, the study suggests the Arabic versions of the EDE-Q and the CIA can be useful instruments for screening and assessing disordered eating attitudes in both clinical and research settings. The study investigated the reliability, validity, and factor structure of these tools involving a modest sample size, and as such, the findings should be considered preliminary and should be interpreted with caution. In conclusion, future studies with a larger and more representative sample are warranted to confirm the results.
Footnotes
Acknowledgements
The authors would like to acknowledge and thank Ms. Leila Alsaleh Alabed for assisting with recruiting participants for the clinical group and entering data for analysis.
Author Contributions
All authors have contributed to the study and the preparation of this manuscript following the ICMJE authorship criteria. Carine el Khazen Hadati and Maya Fleifel Sidani contributed to translating and back-translating the tools and recruiting the participants for the clinical group. Seada A. Kassie contributed to the designing of the study, preparing the study protocol for submission to the IRB, recruiting participants for the non-clinical group, entering the data, running the analyses, reporting and interpreting the results, writing the manuscript including the initial and the revisied versions, and reviewing the manuscript. Bianca Bertl contributed to running the analyses and reporting the results. Meriam Atif Wadiy Melad contributed to drafting and reviewing the tools in Arabic and recruiting participants for the non-clinical group. Alia Ammar contributed to writing portions of the section on ethical considerations, reviewing the manuscript, and providing feedback.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was reviewed for maintaining ethical standards and ensuring the safety of humans in clinical research and was granted approval by the Institutional Review Board of American Center for Psychiatry and Neurology, UAE (Reference number: ACPN-IRB-PN-0021).
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to the requirement to uphold confidentiality in protecting sensitive (clinical) information of the participants. However, data are available from the corresponding author on reasonable request.