
Abstract
Giving birth at a young age and being a victim of intimate partner violence are adversities that affect the life course of women. However, some young mothers overcome these adversities and cope well, showing a dynamic resilience pathway. In this qualitative exploratory study, we examined a purposive sample of 10 resilient mothers who gave birth as adolescents in a situation of intimate partner violence. Their stories were gathered from individual in-depth interviews and on-site participatory observations. Data were collected and analyzed simultaneously, according to grounded theory. Inspired by Masten and Monn’s integrated framework of resilience, the resilience pathway of the participating mothers began with the occurrence of the adversities addressed in this study, namely, early pregnancy combined with intimate partner violence. To overcome these adversities, the participants deployed several protective processes: (a) establishing their maternal identity and the creation of a bond with the child as a turning point, (b) taking an active stance to respond to victimization, and (c) acting proactively and adjusting to motherhood. Promotive processes, positive adaptation indicators, and risks to positive adaptation complete the proposed resilience pathway. The results lead to the conclusion that increased recognition of the challenges that these young mothers face and greater emphasis on the importance of their social surroundings to support these protective processes would support them in their transition to motherhood and promote their well-being and that of their children.
Background
Violence against women is a significant public health issue and a fundamental violation of human rights: It is estimated to affect 30% of ever-partnered women worldwide, with a slightly lower prevalence of 23.2% in high-income countries (World Health Organization, 2012, 2013). Defined as “behaviour within an intimate relationship that causes physical, sexual or psychological harm, including acts of physical aggression, sexual coercion, psychological abuse and controlling behaviours” (World Health Organization & London School of Hygiene and Tropical Medicine, 2010, p. 11), intimate partner violence (IPV) can occur in formal partnerships, such as marriage, as well as informal partnerships, including dating relationships and unmarried sexual relationships since the age of 15 (World Health Organization, 2013). The data suggest that violence typically starts quite early in female adolescents’ relationships (Teenage Research Unlimited for Liz Claiborne Inc. & National Teen Dating Abuse Helpline, 2008), with an already high 29.4% prevalence of IPV in young women aged 15 to 19 (World Health Organization, 2013).
Although IPV may occur at any life stage, pregnancy is a period of particular concern due to its effects on women’s and babies’ health and well-being (Chambliss, 2008; Daoud et al., 2012; Taillieu & Brownridge, 2010). Results from a meta-analytic review showed that IPV is a widespread problem, with 28.4% of pregnant women reporting emotional abuse, 13.8% physical abuse, and 8.0% sexual abuse (James, Brody, & Hamilton, 2013). Estimates from a population study in Canada show that 10.9% of mothers interviewed postpartum for the Maternity Experience Survey (2006-2007) were abused by their intimate partner: 6% before pregnancy only, 1.4% during pregnancy only, 1% postpartum only, and 2.5% during any combination of these times (Daoud et al., 2012). Higher IPV rates during pregnancy are reported by young mothers: In women aged 15 to 19 years, the prevalence of abuse was 40.7%, decreasing with increasing maternal age (Agence de santé publique du Canada, 2009; Daoud et al., 2012). It is now well recognized that IPV during pregnancy may produce serious adversities and numerous negative health effects for both mothers and babies, including low infant birth weight, higher prematurity rates, low maternal weight gain, miscarriage, placental abruption, injuries, and infections, among others (Chambliss, 2008; Coker, Sanderson, & Dong, 2004; Krug, Dahlberg, Mercy, Zwi, & Lozano, 2002; Silverman, Decker, Reed, & Raj, 2006). Moreover, the consequences of violence during pregnancy are not restricted to a woman’s physical health. There are also consequences for her mental health, social environment, and life course. Possible adverse mental health effects include depression, stress, anxiety, posttraumatic stress disorder (PTSD), and suicide attempts. In addition, due to IPV, some mothers may find it more difficult to form an attachment to their child, or they might experience breastfeeding problems (Campbell, Garcia-Moreno, & Sharps, 2004; Chambliss, 2008; Krug et al., 2002; Leone et al., 2010; Martin et al., 2006; Sarkar, 2008; World Health Organization, 2013).
Early pregnancy, for its part, has been linked to a number of social, educational, and economic consequences (Lachance, Burrus, & Richmond Scott, 2012). Although the results are inconsistent in terms of the nature and extent of the consequences for women, there is general consensus that becoming a parent at a young age can limit educational attainment, increase the probability of being welfare-dependent, and substantially lower personal and family income later in life (Boden, Fergusson, & Horwood, 2008). Studies show that many young mothers become isolated when they experience violence, suffer depression, and have less contact with their social networks (Kulkarni, 2009; Sussex & Corcoran, 2005). Yet, some young mothers challenge the assumptions of hardship, poverty, and limited parental capacities that are often associated with this situation. They use various protective mechanisms as well as coping and adaptive strategies that are thought to contribute to resilience.
For decades, scholars in various disciplines have used a variety of theoretical perspectives to examine how some people have managed to escape the harmful effects of severe adversity, cope well, and bounce back or even thrive (Garmezy, 1993; Masten, 2014; Rutter, 1987). In a broad sense, resilience refers to “the capacity of a dynamic system to adapt successfully to disturbances that threaten its function, viability, or development” (Masten, 2014, p. 10). As theoretical models and evidence on resilience increased, there were calls for context- and culture-dependent research and theorization as well as more integrated frameworks (Luthar, Cicchetti, & Becker, 2000; Masten & Monn, 2015; Ungar, 2004, 2007, 2011; Wexler, DiFluvio, & Burke, 2009). Recently, Masten and Monn (2015) proposed an integrated theoretical framework for child and family resilience. It contains five core components that allow viewing resilience from the perspective of contemporary developmental systems theory (Masten, 2014), which assumes that many systems interact or co-act to shape the course of development. These components (Masten & Monn, 2015) are (a) definitions of positive adaptation (for a person, a family, or any other system) and the scalability of adaptive functioning across system levels, (b) a clear description of the pathways of adaptive function over time and their interplay, (c) the identification of promotive processes for adaptive development and the processes by which these effects spread across systems, (d) the identification of various risks to positive adaptation or development and of the processes by which risk spreads across systems, and (e) the identification of protective processes that prevent or mitigate the adverse effects of adversity and the identification of processes by which protective influences spread across systems.
Resilience in the Context of IPV and Early Pregnancy
In the context of IPV and pregnancy, specific events, called pivotal moments or turning points, may help women reject violence in their intimate relationships. Examples of these events are threats to their children’s safety, changes in the frequency or severity of violence, or improved access to necessary resources (Bhandari, Bullock, Anderson, Danis, & Sharps, 2011; Eisikovits, Buchbinder, & Mor, 1998; Koepsell, Kernick, & Holt, 2006). Other factors are related to women’s decisions to end the relationship, the two most consistent predictors being low-relationship commitment and economic independence (Koepsell et al., 2006). According to Bach, Weinzimmer, and Bhandari’s (2013) study, pregnancy may increase women’s self-esteem and agency, which would help them end a relationship. This concurs with another study that found that pregnancy could facilitate a woman’s decision to leave a relationship if she felt that her child was in danger. Furthermore, the fear of being murdered and plans for the future can motivate women to leave a relationship, even when her partner’s manipulation and coercion make it difficult (Moe, 2009).
Different resilience processes have emerged from studies of combined pregnancy, violence, and young age. In her study of urban low-income mothers-to-be, Lutz (2005) developed a theory on double binding in these women. She defines the processes that women undergo to bond with their baby and navigate the relationship with their abusive partner. The majority of the mothers she interviewed were hesitant to report the violence they experienced for fear of public scrutiny and stigmatization. To maintain their public image, they adopted different strategies that allowed them to present a positive image of a pregnant woman in a healthy relationship. Consequently, they were living “parallel lives” (Lutz, 2005). The interwoven and sometimes contradictory processes that these women experienced were categorized into five phases that ultimately ended in a decision to stay (or not) in the abusive relationship (Lutz, 2005).
Bhandari’s qualitative study in rural, low-income pregnant women demonstrates not only some of the negative consequences of IPV on self-image, such as feelings of shame and worthlessness, but also that IPV did not affect maternal identity. However, the decision to leave an abusive partner to protect an unborn fetus as well as other children contributed positively to the representation of a good mother (Bhandari et al., 2011). A minority of women in Bhandari and colleagues’ (2011) study pursued an abusive relationship, partly due to their desire for their children to have a father figure. Kulkarni’s (2006) ethnographic study of 30 adolescent mothers found that adult (mainly parental) guidance, material support, and a safe environment can help young mothers maintain safety in a romantic relationship (Kulkarni, 2006).
Lutz, Kulkarni, and Bhandari’s study indicates that ending an abusive relationship during the perinatal period requires a complex decision that is influenced by numerous factors. They also highlight the dynamic nature of this decision process and situate it within a larger social and cultural context. However, whereas risk factors such as physical and social isolation, lack of access to resources, poverty, and patriarchy, along with the consequences, have been well documented, a deeper understanding of how women cope in these circumstances is needed (Bhandari et al., 2011). To better examine the processes involved in coping with violence during the perinatal period, the present study aimed to explore resilience and IPV in early motherhood, defined as occurring before the age of 20. A constructivist posture was adopted, using qualitative research methods that included individual interviews and on-site observations. Qualitative research is a useful and appropriate way to derive explanations from individually reported experiences (Willig, 2001). It contributes to the knowledge by presenting qualitative findings on resilience pathways, and more specifically, it aims to answer the following question: How do women giving birth in a context of dual adversity, namely, young motherhood and IPV, overcome these adversities? A better understanding of resilience and coping with IPV during the perinatal period would have implications for practices and policies designed to support young mothers.
Method
Data Collection
Using an ethnographic perspective (Creswell, 1998), 10 French-speaking mothers living in the Montréal metropolitan area (Canada) were interviewed individually in this exploratory study. The participants (a) were older than 18 years at the time of the interview, (b) had given birth to their first child before turning 20, (c) had been in a violent relationship, and (d) had a positive self-assessment of overcoming adversity (e.g., they felt that their mental and physical well-being was satisfactory, and they were comfortable in their role as a mother). A semi-structured interview guide was used, containing 16 open-ended questions covering themes such as the participant’s representation of her intimate relationship, her pregnancy, the violence she had experienced, her coping skills, her social environment, her future goals, and the advice she would give to someone else in her situation. The guide could be adapted to the participant’s story. Changes were also made during the data collection period to capture relevant aspects that emerged from the interviews. The participants were encouraged to share as much as possible about their background, situation, and experiences. These data were complemented by on-site observations (Beaud & Weber, 2003), whereby the researcher participated in two community groups of young mothers (4 months with the first group, 5 months with the second; 2 days per week at each site) to identify the various sources of adversity that these women had faced and to gain a better understanding of their realities. The study sites were organizations that provide services to either young parents or specifically to young mothers. The services included, but were not limited to, counseling, support group meetings, educational activities on various topics, on-site babysitting, and referrals to external organizations for specific needs. The first author (S.L.) participated in the groups as a member, using overt participant observation, and kept a daily logbook of observations, comments, and questions following on-site observations to help contextualize certain events and perceptions (Miles, Huberman, & Saldana, 2014).
Procedure
Participants were recruited via referrals by a counselor at the community organization they were attending. The counselors acted as intermediaries between the researchers and participants. They were responsible for informing eligible mothers about the study and transferring their coordinates to the research team if they were interested in participating. We were not informed about potential participants who chose not to participate in this study. This recruitment procedure, which was specified by the ethics committee, had the advantage of maintaining regular contact between the participants and counselors, who were familiar with the various situations of the mothers in their organizations and had the clinical expertise to identify mothers who were doing well. The first author held individual telephone conversations with potential participants prior to the interviews to explain the study goals, describe the discussion topics, and confirm the presence of IPV, measured by the Revised Conflict Tactics Scale (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996). Interviews were conducted at a location selected by the participant, with options including the site of the participant’s organization, home, or a restaurant near her home. Interviews lasted from 45 to 90 min. All participants received a monetary compensation of C$20, and child care was provided if needed. Verbal and written consent was obtained before the interview. Participants’ accounts were recorded on audiotape with their permission, and pseudonyms were assigned. This study was approved by the ethics committee of the University of Montréal, Faculty of Medicine.
Data Analysis
The data analysis was based on grounded theory, which enables inductive identification of social processes and trajectories (Darvill, Skirton, & Farrand, 2010; Glaser & Strauss, 1967). In accordance with grounded theory principles (Creswell, 2007; Glaser & Strauss, 1967), data were collected and analyzed simultaneously. Thus, once an interview was completed, it was transcribed and reviewed for accuracy and completeness (Lincoln & Guba, 1985). Data collection from individual interviews ceased and saturation was considered achieved when themes were repeated and no new material emerged from the interviews (Morse, 1995). First, the transcripts were read (and re-read) for contextual meaning, and the material was coded. Codes were created inductively to reflect participants’ experiences (Glaser & Strauss, 1967), sorted by category, and examined in different contexts. As more interviews were added, the initially developed provisional thematic coding scheme was refined. The first author performed all the coding, and a second author and a qualitative expert reviewed a portion of the analyses for discrepancies. Coding issues were resolved by negotiated consensus and discussion (Bradley, Curry, & Devers, 2007). All analyses were performed with NVivo. After preliminary analyses, we consulted some of the participants about our findings in a group meeting. They were invited to comment on whether our interpretations accurately represented their pathways (Miles et al., 2014). Their feedback proved helpful, as they clarified some of the results of the preliminary analysis and confirmed others.
Demographic Characteristics and Pregnancy
The participants had given birth to their first child at from age 15 to 19. For all but one participant, the romantic relationship during the pregnancy was described as “important.” For many, the father of their child was their first boyfriend: They had been dating from a few weeks to about 3 years before they became pregnant. From their testimonies, it was apparent that they had all been strongly committed to the relationship with the father of their child. There was a range of family histories across mothers, and many reported troublesome events in their family sphere, such as violence between parents, mental health problems, drug abuse, separation or divorce, or frequent moving. Overall, their academic backgrounds were similar: They had average grades and were more or less invested or interested in school. The majority did not want to pursue post-secondary education. When their pregnancy was confirmed, very few participants had well-defined educational or career aspirations. At the time of data collection, participants were from 18 to 33 years old, with eight aged from 18 to 24 years and two aged from 32 to 33 years. Six of the 10 mothers had left their abusive partner, whereas four had chosen to pursue the relationship.
Circumstances surrounding the participants’ pregnancies varied from a total absence of contraception to a planned pregnancy. At one extreme, Alizée was shocked by her pregnancy: “It was definitely not planned. We were immature; we didn’t use any protection. We knew the risk was there but we didn’t care I guess.” At the other end of the spectrum, we find Marie-Sophie, whose pregnancy was fully planned, as a way to escape from parental authority and live with her boyfriend: For us, it was planned. Hum . . . we were going out together and my mother decided to move to another city. It would have been quite far. So, we decided that I would get pregnant and we would live together.
Most of the participants fell somewhere between these two extremes.
Results
Inspired by Masten and Monn’s (2015) integrated framework of resilience, the resilience pathway of the participating mothers was represented schematically (Figure 1), based on an analysis of their life course and their accounts. The pathway begins with the occurrence of the adversities addressed in this study, namely, early pregnancy combined with IPV. This is followed by the deployment of protective processes that enabled the participants to overcome these adversities. These protective processes were (a) maternal identity and the creation of a bond with the child as a turning point, (b) taking an active stance to respond to victimization, and (c) proactivity and adjustment to motherhood. Promotive processes, positive adaptation indicators, and risks to positive adaptation complete the proposed resilience pathway.
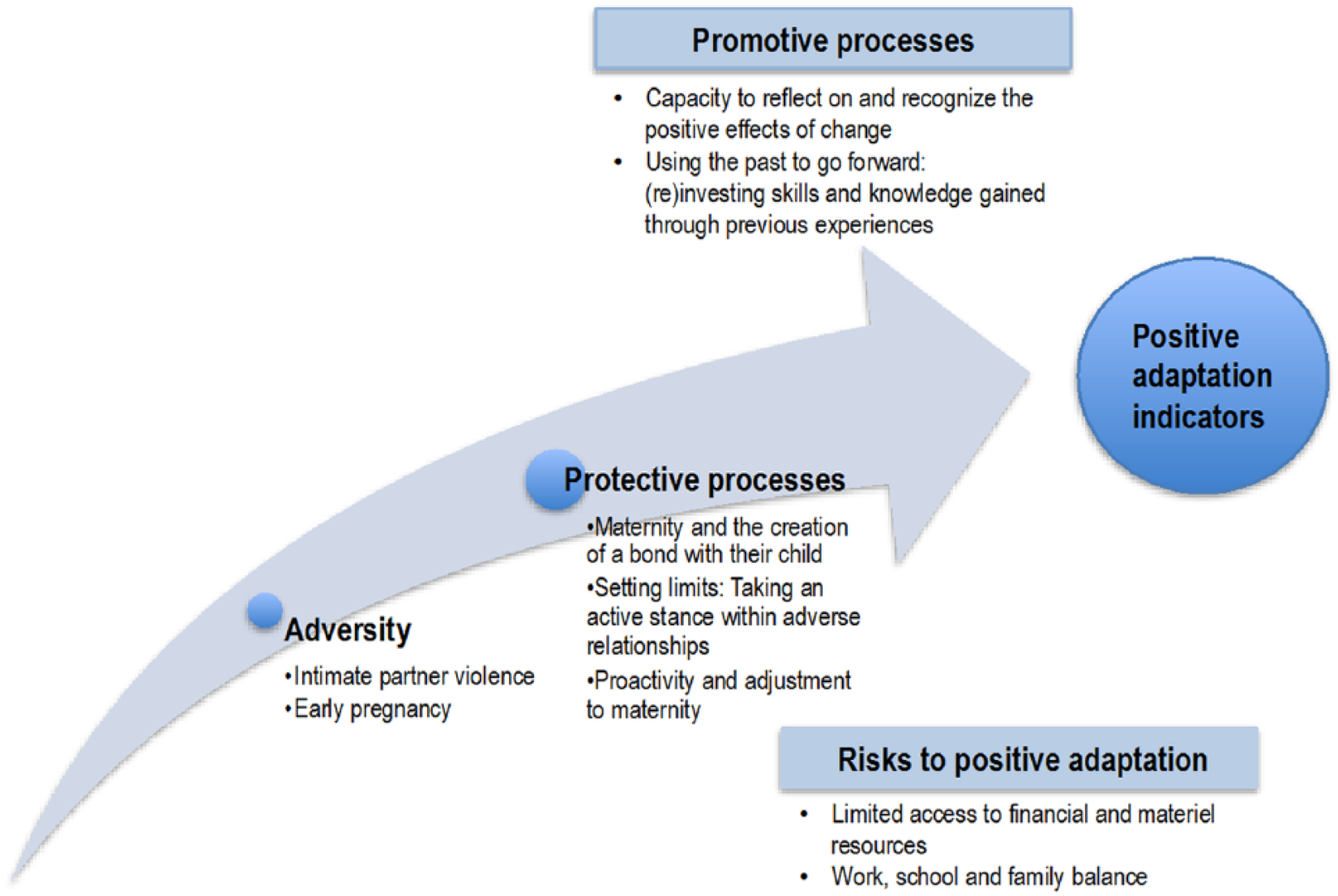
Schematic representation of the resilience pathway in a context of early pregnancy and intimate partner violence.
Each component is discussed in detail below. A conscious choice was made to avoid quantifying the data in terms of frequency. However, in certain situations, the singularity of some participants’ trajectories is noted. All participants are represented by pseudonyms.
Perceptions of Adversity
This study originally assumed that early pregnancy and IPV would constitute two simultaneously occurring sources of adversity. The results for early pregnancy show that motherhood was central for these women, surpassing all other aspects of their lives (professional, social, marital, personal). Furthermore, all participants agreed that IPV was a source of adversity, even if they had difficulty identifying the violent attitudes and actions associated with this term. Thus, although the maternal role was perceived as a difficult choice, it was assumed, and the IPV situation was viewed as a situation from which they could hardly escape. However, the majority of participants (n = 8) did not consider early motherhood as a source of adversity in, and of, itself. For some, it was simply the normal way of things, being the main model in their social and family environment. For others, it was a response to a lack of career plans or academic goals, as it gave their life purpose. Pregnancy was also the result of not knowing what lay ahead or an expression of a desire to let life decide, as illustrated by Shany’s comment: At that time, I think it was really to give my life a certain direction. It clearly was that. I’ve always loved children, but . . . it really was the idea that at last, I would do something with my life. It was selfish, just to get me anchored somewhere. You have a child, you don’t have a choice but to become a mother. In a way, we are proud to be mothers. It really was to find myself. (Shany)
The participants pointed out that maternity is not easy and that it requires a lot of learning, but they did not necessarily link these challenges to age. For example, during the on-site observations, they often talked about their child’s development, how it was within normal expectations for a growing child. Many of them pointed out that their child was following a regular psychosocial and physical development trend, meaning that they were doing their job correctly as mothers and were therefore not different from, or less competent than, older mothers. The participants also stated that what defines a good mother is not her age, but instead the skills and attitudes she deploys when caring for her child. In many informal discussions during the on-site observations, the participants talked about the inadequate parenting skills of older mothers that they knew. They also mentioned examples of young mothers with great parenting skills, the advantages of being younger for bonding with children and understanding them better, and so on. However, the two oldest participants, with longer delays between giving birth and being interviewed, presented early pregnancy as an adversity. Their comments about the role that young age played in their trajectory were more nuanced. For them, being a young first-time mother increased their vulnerability and made it more difficult for them to leave their abusive partner and take on single motherhood. Without exception, all the participants felt that their intimate relationship constituted a source of adversity. Whether due to control, threats, fearful atmosphere, repeated absences, or physical abuse, they considered their relationship to be adverse and linked to negative impacts on their lives and their maternal identity.
Protective Processes
According to Masten and Monn (2015), protective processes are factors that can be distinguished from promotive factors by their special role in facilitating adaptation in situations of adversity or crisis. Three main protective processes can be drawn from the participants’ accounts: (a) maternal identity and the creation of a bond with the child as a turning point, (b) taking an active stance to respond to victimization, and (c) proactivity and adjustment to maternity. Maternal identity consolidation and creation of a bond with the child occur first, whereas the last two occur more or less simultaneously, and not necessarily in a defined order. In this perspective, identity and bonding can be regarded as a turning point in the resilience pathway of young mothers who are victims of violence.
Maternal identity and the creation of a bond with their child
Pregnancy and childbirth changed the life trajectory of the participants. Some tried to change their lifestyle and situation as soon as they knew they were pregnant. For others, changes came when the baby arrived. Maternity brought an awareness of the impact of all their actions and decisions on another person’s life. As one participant stated, “When your baby arrives, I don’t know, you feel more mature, more responsible. You have someone to care for. You can’t leave him there and go to Timbuktu.”
The interviews indicated that confirmation of pregnancy planted the seeds for change and that the birth of the child combined with the creation of a bond with that child consolidated the desire to improve the situation. Whereas the time required to create an affective bond with the baby differed across participants, the analysis results showed that the awareness of that special bond motivated them to mobilize themselves, take on a positive parental role, and establish a violence-free environment. The affective attachment to their baby seemed to be based in part on their recognition of the child’s needs and of their own physical and emotional capacities to meet those needs. As such, their maternal identity, in the sense of the generated purpose and value, became central to their self-representation.
Setting limits: Taking an active stance within an adverse relationship
These resilient women were aware of the negative consequences of their romantic relationship: They knew that certain aspects could cause harm, to either themselves or their child. Impelled by this awareness, they used strategies that enabled them to meet their need for a safer environment in which they could raise their child. Although not all of them used the word “violent” to describe their relationship, the descriptions were unambiguous: So he tried to hit me but hit the wall besides me instead. Afterwards, he took his steel cap boot and knocked my friend over. He was . . . for him, there was nothing wrong in the way he was behaving. . . . He didn’t hit me afterwards, but you know the signs were there. I was now dumb, couldn’t do anything right, didn’t know how to take care of my baby, I was incapable of cleaning the house . . . Suppers, they were never good. (Élizabeth)
However, the participants did not all react the same way to their relational situation. The analyses revealed four types of coping strategies: (a) defense strategies, (b) couples therapy, (c) ultimatum linked to specific expectations, and (d) ending the relationship. These strategies were neither mutually exclusive, nor were they necessarily implemented immediately after the baby’s birth. Concretely, some participants (n = 3) developed defense strategies to reduce the harm caused by their partner and the relationship. One participant began therapy with her partner with the goal of developing a more egalitarian, control-free relationship. Another gave her partner a firm ultimatum regarding his attitudes and behaviors: If he changed, and those changes were maintained over time, they would pursue the relationship. Most participants (n = 6) chose to end the relationship: It started like that; he called me names and put me down. Once again, I froze and stayed inside for another whole month without going out or calling anyone. . . . I talked about it with X [counselor] and she was aware of the situation. She would come to my place for visits. She came for 3 or 4 months. And one day, I got up early in the morning, put all my belongings in a bag and left. From one day to another. (Élizabeth)
All the participants’ responses were characterized by major hesitation before ending the relationship for good. Indeed, the analyses revealed much back and forth, which can be attributed to two main motivations. First, there was a shared perception that early motherhood is judged more negatively when the mother is a single parent. For a large portion of our sample, the mother’s and spouse’s identities had to be combined so that the early parenthood would have legitimacy and credibility. They felt more respected as a young mother when they were in a relationship with the child’s father. Therefore, many participants chose to maintain their relationship even if it was unsatisfactory or did not meet their expectations. Similarly, most were strongly invested in the two-parent family ideal. All participants had a strong desire to form a united family, with the exception of one, who had wanted the father absent from their lives from the very beginning of her pregnancy. The second motivation for pursuing the relationship was a desire to maintain a united family for the sake of the child’s well-being. Another common element for many was the guilt they felt about their decision to split up the family, which consequently deprived their child of his or her father’s daily presence. (For a more detailed description of the challenges that IPV imposes on early motherhood, see Lévesque, 2015) Because for me not having a father growing up, I so wanted my daughter to have a father by her side. I really wanted him to play the part, to be a dad. . . . In my head, it was always with the idea that my two daughters would have their father. Mommy and daddy in the same house. I tried until the end. Until the end, I kept trying. (Shany) I was more . . . cause I felt I had to be a family. In my family’s eyes, for my son. And for J, cause that’s what he wanted. I just did it for those reasons. (Louise)
Proactivity and adjustment to maternity
Incidentally, becoming a mother brings many other major changes to a teenager’s life. One of the most significant may be the transition from the “I rely on someone” to “someone relies on me” status. When pregnancy was confirmed, the participants were not financially, materially, or personally prepared for parenthood. However, the interview analysis shows that they mobilized their external resources proactively and searched for new ones to help them overcome obstacles that they might encounter when they became mothers. As one participant puts it, You have a goal; you’re going to find what you need to achieve it. You can do it; you’ve taken the trouble to find the resources you need. To accomplish your goal. But it’s . . . going out and finding the resources. (Mimi)
These resources varied across participants and could include financial resources or material goods to prepare for the baby’s arrival, information and education about parenting, housing information, referral or access to public or cooperative housing or a more suitable apartment, educational and professional counseling, and ways to break social isolation and meet other new mothers. Family and social surroundings were important resources for the participants. Even if their family was not always supportive of the pregnancy at the beginning, they provided much-needed help when the baby arrived.
My mother helped me leave. She’s the one who found the apartment. If I hadn’t found a landlord who helped me find furniture in the first two weeks, and if I hadn’t found a person at the health center who was really concerned about my case, . . . I’m not sure I would’ve been able to get through it all. (Marie-Sophie)
This mobilization was driven by their desire to create a life setting that was better suited for maternity. Furthermore, the participants underscored the importance of establishing a life situation that was better suited for maternity and of creating an enjoyable life for their child. When asked about their motivations to make changes to their lives, the majority talked about their child’s well-being and taking responsibility for their children. As Shany puts it, “I want my daughters to be at peace, happy, and fulfilled. It’s the only thing that I want. It’s by showing them, by doing it myself. By being a role model for them.” To create that life setting, many participants had to end relationships with family, friends, and colleagues that they felt were toxic and had to create new social networks with people who shared the same values or lifestyle. Others had to end a habit that was unsuitable for maternity, such as drug or alcohol consumption. Many also had to establish a healthier lifestyle, for example, with a more regular schedule. Creating these healthy life settings required a capacity to discern what was adequate and what was not. Their inner strength also helped them make choices and stay committed to them. As one participant explained,
Me, I stood my ground until the end and got rid of the people who were harmful for me. What good was it to have them around me? . . . I think it’s normal that you do some “cleaning-up” of the people around you. Not keep all your friends. . . . All the people who were doing drugs for the kick and doing it every day, I flushed them out of my life. (Louise)
Promotive Processes
Promotive processes are factors and processes associated with adaptive success, independent of risk or adversity exposure, in that an interaction with risk is not necessary. Using the past to go forward by (re)investing skills and knowledge gained through previous experiences is a major process in the resilience pathway of the participants. As shown in Table 1, the participants had experienced many adversities before giving birth to their child. To overcome these previous experiences, they had to mobilize inner strength, draw on external resources, and make changes to central aspects of their lives. They gained strength by going through these processes, notably by acquiring knowledge and skills and reinvesting them to cope with new adversities. For example, for Shany, the various obstacles she encountered growing up gave her a strong sense of self and an unwavering resolve. Alizée’s life experiences were more helpful than any school lessons: using what she learned helped her avoid bad choices later on. Because Marie-Sophie moved frequently as a child, she had to deal with family instability: These experiences enabled her to develop good adaptation skills. Meanwhile, Mimi spoke about her strong character, which helped her cope with “what others think.” Elizabeth, who as a child was abandoned by her parents, had struggled for several years to make a living for herself and her younger sister. She developed autonomy, organization, and problem-solving skills, which she identified as useful in her current situation. Faced with the adversity of IPV, Elizabeth explained how she recalled actions and events from her past to help her in times of doubt: It was hard. Yes. At the apartment, I kept saying to myself: have I done the right thing? I had a house, a backyard . . . But I had no future because I was constantly controlled. It’s not normal to live like that and I wasn’t happy either. When I was in doubt, I would tell myself that it will go away with time. But I know that I will overcome it, because I have been through it. . . . You know, I have overcome obstacles worse than what I have to go through today. (Élizabeth)
Self-Reported Portraits of Participants’ Lives and Vulnerabilities.

Note. IPV = intimate partner violence.
Another promotive process is the capacity to reflect on and recognize the positive effects of change. An important aspect that kept the participants on a resilience trajectory was their capacity to reflect on the positive benefits and their new-found feeling of control as consequences of the changes they had made to their lives. This meant recognizing that they had made appropriate decisions to stop abuse, that they were gaining control over their own life (e.g., with an apartment in their name), and that they were able to provide their children with a stable and nurturing environment. These were some of the major incentives that kept them going. The opportunities to analyze what they went through, alone or with a counselor, to reflect on their coping skills and strategies, and to be aware that these actions had changed their life course appeared to be essential factors in their resilience pathway. Furthermore, recognizing that people around them were aware and supportive of their choices and actions appeared to be an important factor that kept the participants on a positive track. Some of them were able to recognize what they had done well, but for others, it was more difficult. For these young women, recognition by a peer, or someone else they valued, helped them become aware of the positive benefits of a resilience trajectory.
When people around me told me, “I can’t believe it. You are so good. I would never have been able to do everything you are doing. Thumbs up!” That, for me, was pride, but also a challenge to tell me I have to keep going. That people see me progress and go forward. I would also see it, but since I don’t have a lot of self-confidence, the fact that other people had trust in me allowed me to go through that. (Marie-Sophie) Seeing my family and my friends so proud of me helped me keep doing things better, so I guess support from the outside really helped doing good. Like once you are doing good, being told you are doing good really helps, you know. (Alizée)
Thus, being able to identify their qualities, apply acquired skills and knowledge to new situations, think about their situation, and view time as an important factor were all processes that promoted a resilience trajectory. The sum and interactions of these processes allowed these young mothers improve their life trajectory.
Risks to Positive Adaptation
Although the participants’ trajectories highlighted the processes they used to overcome adversities, namely, pregnancy at a young age combined with IPV, the fact remains that there were other problems along the way. The participants were aware of these limitations, which constituted risks to positive adaptation. Two main risks were identified in their accounts.
Limited access to financial and material resources
The two possible income sources for our study sample, government benefits and salary, are barely enough to live on. The end of the month comes quickly, and tight budgets generate stress. Housing accessibility, which depends on financial resources, is another factor that can weaken a resilience trajectory in many ways: by limiting the participants’ autonomy, forcing them to rely on their family, and sometimes forcing them to stay in abusive relationships. Although some participants were able to find cooperative or social housing, others had no choice but to live in an apartment that was too small, badly located, or unsuitable for their needs. They had to move frequently from place to place to improve their housing situation, which created instability.
Work, school, and family balance
Most of the participants did not want their children to be in full-time day care. They wanted to spend as much time as possible with their children, and they wanted to be there for them, at least until they started school. For them, the “good mother” value, the idea that a mother has to be present with her growing child, was central to their role as a mother. Participants who wanted to return to school or work outside the home wanted to have access to flexible day care, either part-time or accommodating for atypical work hours. However, according to the participants, the public day care system in Québec (Canada) does not offer these services. They were therefore faced with choosing to put their children in full-time day care or to stay at home with their children and set aside school and work plans.
Resilience Indicators
From the evaluation of the life trajectories of the participants and discussions held with the referring counselors, five criteria indicating positive adaptation to early motherhood in an IPV context were identified (see Figure 2).

Indicators of positive adaptation in a context of early pregnancy and intimate partner violence.
Presence of good parenting skills and concern for the child’s well-being
The counselors who contributed to this study referred mothers who they considered resilient to participate in the study. These participants had received previous support for parenting skills. In concrete terms, they had no history of intervention by the Department of Youth Protection. The participants were also questioned about what they felt constituted a good mother and on the ways in which they had acted as good mothers. Besides the label “good mother,” the participants demonstrated concern about their child’s well-being, whether by attending workshops on parenting skills or child development, or by their actions, attitudes, and interactions with their child.
Apparent absence of mental health problems
In the interviews with the participants and during the on-site observations, and as confirmed by the referring counselors, the participants did not present any signs of mental health problems. The majority of them had gone through more difficult experiences in the past, such as depression. However, these episodes appeared to have ended at the time of the study. We concluded that their current state of physical and mental health enabled them to accomplish what they felt was important: take care of their child, meet with other mothers, study or work, and so on.
Cessation of behaviors judged incompatible with motherhood
As mentioned above, a substantial proportion of the participants reported previous behavior patterns that they judged to be incompatible with motherhood. Therefore, they had decided to stop these behaviors when they found out that they were pregnant or after the baby arrived. The absence of these behaviors would also indicate a resilience trajectory.
Awareness of the adverse relationship and its consequences
The participants were aware that their relationship was not a positive element in their life. They knew that the behavior of their intimate partner had repercussions for themselves and their families. They were also aware that things could be different. This awareness of the relationship and its influence served as both a preliminary activating step to counter the violence within the relationship and an acknowledgment of the adversity of the relationship and its consequences. It was therefore considered an indicator of resilience.
Presence of plans for the future
The participants thought about their future and were not apathetic in this respect. They analyzed their situation and their options and made decisions to achieve goals that they had set.
I tell myself all the time that social assistance might not always be there. Me, my mother, she always had financial problems. My parents separated when I was six years old. At that time, my mother wasn’t working; she was a stay-at-home mom. . . . I told myself that I didn’t want that, in my life. So, I had to go to school. (Marie-Sophie)
These five indicators were identified by data triangulation and analysis and allowed distinguishing between mothers with and without a resilience trajectory. However, this distinction is fragile, due to the small sample size, the use of inclusion criteria based on the mothers’ and counselors’ judgment, and the absence of a control group for comparison (i.e., presenting the two combined adversities), and it should be interpreted with caution. It is also important to mention that these indicators were not necessarily immutable for the participants in this study. Instead, they should be considered as observations within a specific context and at a specific time in their life course.
Discussion
Based on the trajectories described by young mothers who participated in interviews and on-site observations, this article proposes an answer to the following question: How do resilient women who give birth at a young age and experience IPV overcome these adversities? The results of the qualitative analyses highlighted certain protective and promotive processes by which these women overcame these adversities. First, maternal identity and the creation of a bond with the child provided a turning point. Subsequently, they took an active stance to respond to victimization, acted proactively to adjust to motherhood, and used the past to move forward by reinvesting skills and knowledge they had gained from previous experiences. Only a few studies have addressed this specific context of dual adversity and the associated processes. The research has focused more on only one source of adversity. Despite the growing empirical data on protective and risk factors, little is known about the processes involved in coping strategies and resilience trajectories in an adversity context (Harrop, Addis, Elliot, & Williams, 2009; Reaching IN . . . Reaching OUT, 2010). The processes presented in this report advance the knowledge on relationships between early pregnancy, IPV, and resilience.
According to our results, the creation of a bond with their child is central to the lives of young mothers and constitutes a significant turning point. Maternal identity is a positive label that these women readily embraced. Our results are in line with the literature on the transition to motherhood in a challenging context, which postulates that the upcoming arrival of a child is an important catalyst for change in many pregnant women. For Charbonneau (2003), childbirth is an event that singlehandedly produces changes in the mother’s habits and daily life, generating a resource mobilization process that is distinct from those associated with other definitive events in the teenage years and emerging adulthood. Our results are also echoed in Bhandari and colleagues’ (2011) study, which concluded that the important life decisions made by mothers depend on the mother’s bond with their unborn or newborn baby as well as their other children. Regardless of the age at which maternity occurs, a notable characteristic of mothers who showed resilience was the development of an identity as a competent mother. Indeed, central to the issue of maternal identity is the idea that young mothers do not want to be labeled as “good mothers, considering their age.” Instead, they wanted to show that they met the criteria for a good mother, and they claimed their right to be categorized as good mothers. This suggests that age is inadequate and misleading as a normative criterion. Our results are also similar to the findings of McDermott and Graham (2005) and Mitchell and Green (2002), who found that young mothers tried to distance themselves from the idea that they were inadequate mothers because of their age, mainly by creating a division between the young mothers they judged as adequate or good and the ones they felt were irresponsible and who did not care enough about their child. Nevertheless, although this division allowed them to escape the social stigma of early motherhood, this perspective contributes to maintain prejudices against other young mothers.
Although they consistently recognized the negative impact of their relationship with the baby’s father, the participants in this study mentioned a number of strategies they used to respond to violent instances. These strategies were intertwined with other simultaneously occurring processes: proactivity, adjustment to maternity, and using the past to move forward. They differed qualitatively from the adaptive phases described by Lutz (2005). In the first phase, women pursue their ideal of family unity and a positive image of their partner, even if they experience IPV. In this phase, they play down signs of IPV. In the second phase, they put up with IPV for the sake of their child and to maintain the family unit. In the third phase, ambivalence toward the relationship with their partner increases: They oscillate between feelings of despair about their situation and a desire for change as well as better outcomes for themselves and their children. The fourth phase begins when the two worlds, public and private, are reconciled and the IPV is openly recognized. In the final phase, after the baby’s birth, the mother invests her energy into protecting her newborn from the abusive partner. A decision about the relationship has usually been reached by this time: If the woman wants to end the relationship, she makes appropriate plans. If she decides to pursue the relationship, she does so with conditions for the abusive partner (Lutz, 2005). Lutz’s (2005) results also demonstrated the importance of the paternal figure, the father’s presence being a key element for the study participants. Hence, none of them wanted to end their relationship during pregnancy, despite violence on the part of their partner. On the contrary, they reinvested in their intimate relationship, fuelled by the hope that the baby’s arrival would stop the violence (Lutz, 2005). However, Kulkarni (2007) proposed a different interpretation of the transition to motherhood in a context of IPV. She contends that when mothers are confronted with the multiple emotional demands of a conflictual relationship at a time where they are centered on the baby’s care, the partner is perceived as a burden.
Tidying things up by keeping unwanted people at a distance, creating a new circle of friends, inquiring about nurturing skills, and getting organized and equipped to welcome the baby are examples of the strategies that our participants used to create a more suitable life for maternity. This desire and its various manifestations have been reported in the literature on the transition to parenthood. As one of the most important transitions in the life course (Katz-Wise, Priess, & Hyde, 2010), it tends to stimulate improvements in one’s life habits and the creation of a safer environment for an expected baby (Klima, 2003; SmithBattle, 1995). This desire can be more pronounced in women who practice unconventional behaviors such as drug or alcohol abuse and in women with early pregnancy. In terms of social norms for maternity, these women are less often viewed as “good mothers” and are less psychologically and financially prepared for the child’s arrival (Klima, 2003; Venne & Morissette, 2009). Consequently, this transition period may provoke many of them to make rapid changes to improve their life conditions and life habits. For many adolescent mothers, pregnancy is a profoundly transformative experience that requires significant changes for them to become responsible parents (SmithBattle, 1995). SmithBattle (1995), who interviewed adolescent mothers during pregnancy and 4 years later, found that those who perceived their pregnancy as a positive, transformative experience blossomed into their parental role and reported that motherhood allowed them to envision a future filled with hope (SmithBattle, 1998).
The findings of this study must be considered in light of certain limitations. We investigated a small group of resilient women who had coped with specific types of adversity. Thus, our results cannot be generalized to all young pregnant women or all those who experience IPV. Second, all the participants in this study were referred by a counselor working at a community organization. Therefore, young, resilient mothers who had been victims of violence but were not involved in community groups or receiving services from a health clinic were not considered in this study. Third, as imposed by the ethics committee, we were prohibited from recruiting mothers younger than 18 years. This is an important limitation, because very young mothers’ trajectories may differ significantly. In addition, retrospective reports and time lag variations between events and interviews constitute additional limitations that could have influenced the mother’s self-reports.
Aside from these limitations, the results of this exploratory study raise intervention and research issues. The testimonies of the resilient young mothers demonstrate the complex circumstances of early pregnancy when intimate violence is also present, the many challenges involved, and the processes required to cope with them. Resilience is recognized as an beneficial feature of health promotion (Raeburn & Rootman, 2006), and this study provides a better understanding of the processes involved in the development of resilience pathway, as well as factors that promote or hinder its sustainability over time. Because these factors are subject to change, better-adjusted practices and targeted public policies could foster resilience pathway in a greater number of young mothers. Our results on young mothers’ definitions of adversity would also be useful for health and social service professionals. Their perspectives could help practitioners understand women’s subjective experiences and create spaces for dialogue, where common understandings of situations and intervention goals could be negotiated. Finally, this study underscores the importance of taking into account the positive elements in the lives of populations categorized as “vulnerable,” rather than targeting only risk factors or potentially negative aspects. Further studies are needed to fully explore the mechanisms of resilience and the associated coping processes in situations of early pregnancy and IPV. Mixed-methods research designs would improve the understanding of these issues (Sandelowski, 2000), and more qualitative studies could provide deeper contextual analyses of these dual adversities (Corbin & Straus, 2007).
Footnotes
Acknowledgements
The authors thank the women who participated in this study. The authors also thank the organizations that supported and helped recruit the volunteers for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.