
Abstract
This monograph reports the results of a three-year multiple case study of nine knowledge-to-action (KTA) initiatives mobilized in communities of practice (C0Ps) operating in Ontario's seniors' health system. A multiple case study design was used to conduct nine case studies through a combination of case study and ethnographic methods. Deductive analytical methods were used to answer two broad research questions about the KTA processes mobilized through the CoPs, and about the roles played by CoP members and other stakeholders. Inductive analytical methods were used to reveal the patterns of interaction characteristic of the CoPs. These CoPs acted as flexible and temporary social forms with specific characteristics and processes allowing them to integrate explicit and tacit knowledge to resolve the unique contextual challenges of health practices. Our findings suggest that these CoPs often developed a double-loop learning process that is well suited to responding to adaptive challenges and wicked problems. Conclusions from this qualitative study are not generalizable to all situations and contexts. Findings suggest that the concept of "knowledge-to-action" be supplemented by a concept of "action-to-knowledge" that recognizes that important initiatives are often incubated in the action of health care delivery when dedicated professionals come together to tackle intractable issues. This is the first multiple case study of CoPs in the Canadian health system. The study shows that CoPs can act as the junction for the rational epistemology of science and the narrative epistemology of practice.

Keywords
Introduction
Moving knowledge into frontline health practices is difficult. Greenhalgh and Wieringa (2011) commented that “…knowledge obstinately refuses to be driven unproblematically into practice” (p. 501). Many scholars and practitioners are trying to understand the source of this obstinacy and to identify interventions that could be scaled up for use by others.
Perhaps the intractability of the problem arises in part from the incommensurate nature of the worlds of science and frontline practice. For knowledge translation to occur, the rational, deductive epistemology of the scientific laboratory must integrate with the pragmatic and opportunistic epistemology of frontline practice. Decisions and actions must make sense within a complex array of systems that are bounded by norms, preferences and values rather than simple linear causality. An option is chosen not simply because science tells us that it ought to be, but also because human actors, facing the affordances and constraints of their practice, declare themselves willing and able to support and act on a new choice.
Early studies of knowledge translation attempted to identify the most successful approaches (Bero et al., 1998; Fixsen & Blasé, 1993; Grol & Grimshaw, 2003). Leaders and researchers have sometimes viewed organizational and system change as a process that is initiated and controlled by people at the top of organizational hierarchies or at the head of scientific research teams, with frontline workers and other stakeholders following instructions pushed down from above (Ashburner et al. 1996; Dunphy & Stace, 1988; Lavis, 2006; Ryan et al., 2008). While these efforts produced interesting results, including the suggestion that multifaceted interventions tend to be more successful, some scientists and practitioners began to wonder if new ways of conceptualizing knowledge translation might be needed (Greenhalgh & Wieringa, 2011; Kitson, 2009). Greenhalgh and Wieringa (2011), for example, have pointed out that some intellectual traditions emphasize the importance of having stakeholders at all organizational levels engage in a process of collective negotiation to bring new knowledge and innovations into practice. This is consistent with recent work in organizational change that sees transformation resulting from broad collective efforts to change mindsets, patterns of behavior, and the structuring of these patterns through culture, policy and technology (Appelbaum & Wohl, 2000; Bartunek et al., 2011; Bartunek & Jones, 2017; Cohn, 2009; Conklin, 2021; Fernandez & Rainey, 2006; Marshak, 2020).
In this monograph we argue that a community of practice (CoP) can be a social context in which this negotiation and mobilization takes place. We agree with the view that knowledge-to-action (KTA) is essentially a process of human interaction (Greenhalgh et al., 2004; Lavis et al., 2003; Shojania & Grimshaw, 2005). Knowledge has been seen to inform practice when people from different contexts and disciplines come together to discuss problems, gather data, and experiment with new approaches (Gabbay et al., 2003; Gabbay & le May, 2004; Kellie et al., 2012). Knowledge translation thus may be less like a top-down command, and more like a conversation among people who are grappling with complex problems in their practice. If this is correct, the shift in our understanding of knowledge translation resembles a contemporaneous shift in the field of organizational change, where top-down diagnostic approaches are being replaced by collaborative dialogic approaches (Bushe & Marshak, 2016).
For many years, scholars have been calling for research on factors that influence the uptake and use of innovations in local settings (Greenhalgh et al., 2004). Others have called for research to reveal the ways in which knowledge, frontline health delivery contexts, and implementation processes interact during efforts to move innovations across social boundaries (Kitson et al., 2008). For several decades, scholars and researchers have argued that organizational and social change is essentially a process of learning (Argyris & Schön, 1978; Hendry, 1996; Kegan & Lahey, 2016), and some have considered the social forms and activities that are best suited to support learning processes intended to bring about beneficial change (Stouten et al., 2018). We know that top-down change controlled by a cadre of managers is not always effective, but we continue to search for an understanding of the best ways to enable the collaboration and learning required to solve intractable problems and improve organizational performance (Conklin, 2021; Hastings & Schwarz, 2022). Our research is intended to help fill these gaps.
This monograph reports the results of a 3 year multiple case study into KTA processes mobilized through CoPs operating in Ontario’s seniors’ health sector. These CoPs operated within a knowledge network that relied on the following definition of a CoP: “A CoP is a community or group of people who have made a commitment to be available to each other, to offer support to participate in learning, and to create new knowledge. CoP members commit to advancing the field of practice and to sharing those discoveries with anyone engaged in similar work” (Chambers et al., 2010). The CoPs that participated in our research were therefore expected to act as contexts for learning and knowledge creation, and to use innovations and knowledge to improve an area of health care practice.
The study explored the following research questions:
Knowledge-to-action processes: (i) What KTA processes are initiated through the CoPs? (ii) To what extent does KTA involve an interaction between explicit knowledge and tacit knowledge?
The role of human agents: (i) What roles are evident among those who participate in these processes? (ii) How does the active involvement of knowledge users in the KTA process influence knowledge utilization? (iii) What factors support or hinder effective involvement in KTA processes?
Our study used deductive methods to describe and understand the KTA processes that were designed and implemented by CoPs operating in an Ontario knowledge network, and to identify the more prominent and important roles played by CoP members in these processes. The study also included an exploratory component that made use of inductive methods including open coding and thematic analysis, and that was explicitly intended to allow us to be open to discoveries that went beyond our explicitly stated research questions. We wanted to answer specific questions about KTA processes and the roles played by human agents, and we wanted to see if our large qualitative dataset could yield additional discoveries.
Over the course of our work it became evident that most CoPs were grappling with “wicked problems” (Rittel & Webber, 1973) characterized by high levels of uncertainty and a variety of forces acting at different levels in a complex provincial health system. The CoPs often began by identifying a seemingly bounded and straightforward issue that they would focus on, but as they moved forward with their work they found that this issue was held in place by a complex array of attitudes, interactions, and structures. Consequently, most CoPs developed exploratory processes that would provide them with access to diverse perspectives out of which might emerge innovative ways to handle complex challenges.
Indeed, our intention was to combine deductive and inductive methods in an effort to reveal the patterns characteristic of KTA processes in nine case studies, and we hoped that our cross-case analysis might produce a model depicting the manner in which most CoPs sought a way to move forward. The purpose of this monograph is to present these findings and discuss their importance.
Literature Review
To provide context for our research, we begin by reviewing research that considers the effectiveness of CoPs as vehicles for moving knowledge into action. We look at work that conceptualizes KTA as a social process enacted by CoPs that helps people to identify and use knowledge. We consider the various benefits that can be produced by CoPs, and the characteristics that distinguish CoPs. We look at the relative importance of tacit and explicit knowledge for CoPs, and at the critical success factors that have been associated with CoPs. We also review relevant aspects of the literature on social learning, and we consider the role that CoPs could play in solving intractable problems.
Knowledge-to-Action as a Social Process
The movement of knowledge across social boundaries is a complex and iterative process that includes interaction between and engagement of knowledge users and knowledge producers (Bero et al., 1998; Berta et al., 2005; Lavis et al., 2003; Shojania & Grimshaw, 2005). The complexity of KTA processes can derive from a clash of priorities or values, from the nature of the evidence that is being implemented, and from the unique features and characteristics of frontline health delivery contexts (Aylward et al., 2003; Dopson et al., 2003; Ginsburg et al., 2007; Greenhalgh et al., 2004; Kitson et al., 2008; Logan & Graham, 1998).
Moving knowledge into practice appears to require a conveyance or “bridge” across social boundaries, and scholars have considered what sort of bridge delivers the best results (Oborn et al., 2013). Pentland et al. (2014) have suggested that successful KTA in health care tends to involve either codification processes that connect people to useful documentary knowledge, or community processes that mobilize knowledge through human interaction. Some suggest that a change agent (e.g., a facilitator or thought leader) can overcome the gap between knowing and doing (McCormack et al., 2013). For example, knowledge brokers (KBs) have been seen to link knowledge users and researchers in ways that facilitate improvements in practice settings (Conklin et al., 2013; Hoens et al., 2013). Others argue that collaboration between knowledge users and researchers during the research process produces useful benefits (Kothari & Wathen, 2013). These arguments suggest that one way to bridge the knowing-doing gap is through collaborative relationships and social interaction (Bowen & Graham, 2013; Jansen et al., 2013).
Beneficial Social Processes Enacted Through CoPs
One organizational form that may facilitate the interaction processes needed for knowledge translation is the CoP. A variety of claims have been made about the role played by CoPs within an organization or system. Wenger (1998) argued that CoPs could help newcomers navigate a pathway from the role of an incoming novice to that of a fully competent practitioner, and could also help to foster a sense of inclusion and belonging. Wenger and Snyder suggest that CoPs seek creative solutions to problems, describing them as “…groups of people informally bound together by shared expertise and passion for a joint enterprise…[and who] share their experiences and knowledge in free-flowing, creative ways that foster new approaches to problems” (2000, pp. 139–140). CoPs are associated with theories that see learning as a process of social interaction and exchange rather than as a simple linear transfer of information (Dewey, 1938; Vygotsky, 1934). These insights led to experiential approaches to education and learning, which conceive of a learning cycle that includes action, reflection, and moments of disorientation along with ongoing interactions among practitioners as they encounter and solve problems (Kolb, 1984; Schön, 1983). Some scholars treat learning as a natural, situated phenomenon that can enhance the stability and adaptability of a group of practitioners (Brown & Duguid, 1998, 2000; Cummings & van Zee, 2005; Lave & Wenger, 1991; Orr, 1996; Wenger, 1998). These conceptions suggest that people who work together in a shared practice will create and sustain a pool of knowledge that can be accessed when needed (Boreham, 2004; Cook & Yanow, 1993; Orr, 1996).
This is the form of learning that Wenger (1998) believes lends coherence and resilience to a CoP. Members of the practice create routines and tools that offer stability. They interact with each other to accomplish tasks, and they socialize and train newcomers (Lave & Wenger, 1991; Wenger, 1998; Yanow, 2004). The knowledge arising from this dynamic is grounded in member experiences, is both tacit and explicit, and is sustained and spread through interaction (Brown & Duguid, 1998, 2002; Colville et al., 1999; Gherardi and Nicolini, 2000a; Leonard & Sensiper, 1998; Nonaka & Takeuchi, 1995; Yanow, 2004).
Researchers have identified a variety of ways in which CoPs have contributed positively to the organizations and systems in which they operate. CoPs have been seen to promote exchange between academic researchers and knowledge users, in part because they de-emphasize the power differentials that can act as barriers to exchange (Hart et al., 2013). Some see the main purpose of a CoP as improving the activities carried out by members of a practice through an ongoing negotiation of meaning that is well-suited to address complexity and uncertainty (Azan et al., 2017). CoPs have been shown to facilitate social learning, especially when the CoP: experiences democratic and empowering leadership; fosters intense collaboration that involves regular interactions through which experiences are shared; creates a sense of psychological safety and trust within the community; and has porous boundaries that allow for the ongoing creation of new relationships with people who could potentially contribute to the goals of the CoP (Durand et al., 2022; Fam, 2017; Sadiq, 2021; Salter & Kothari, 2016; Sibbald et al., 2022). Some conceptualize a CoP as a social form that enables the questioning of cherished assumptions and paradigms, making it possible for an organization to transform itself while operating in a complex and changing environment (Furlong & Johnson, 2003; King et al, 2023). A recent synthesis of the relevant literature suggests that CoPs are generally seen as serving one of three purposes: to promote learning, to promote innovation, or to protect and control existing interests (Nicolini et al., 2022).
In the domain of health care, CoPs have been used to engage practitioners in capacity building to achieve public health objectives (Bazyk et al., 2015). Health organizations have used virtual CoPs to support new training approaches (Champagne et al., 2014; McEwen et al., 2015) and to improve and inform healthcare practices by allowing geographically distributed peers to discuss issues arising from day-to-day practice (Ikioda & Kendall, 2016). CoPs have also been shown to facilitate the implementation of a new care paradigm involving early intervention services for mental health patients in France (El Oussoul et al., 2020). CoPs have helped teams and organizations to facilitate knowledge sharing, collective learning, and interprofessional collaboration (Gabbay et al., 2014; Mazer et al., 2015). CoPs have been shown to enact a shared learning process that involves “thinking together” about relevant and important problems such as dementia care and sepsis practice so that tacit knowledge is spread across occupational and institutional boundaries in ways that support positive change (Pyrko et al., 2017). Recently, CoPs have been seen to enable a learning process that has helped healthcare teams to better understand the ethical concerns that arise during some interactions with patients (Giske et al., 2022), and to manage distress and create moral resilience during the recent pandemic (Delgado et al., 2020, 2021). Another study has indicated that informal caregivers (mostly family members) of people with Alzheimer’s disease experienced an enhanced quality of life through their participation in a virtual CoP (Romero-Mas et al., 2021).
A study at the Center for Disease Control and Prevention in Atlanta found that CoPs produce benefits such as consistent communications, enhanced analytical competence, sharing of standards, promotion of initiatives, enhanced capabilities in specific domains, improved links among dispersed professionals, and greater efficiency (Mabery et al., 2013). These authors wrote: “Fostering trust and building relationships within a community is the first and most important work a community can do to build social capital within the domain” (Mabery et al., 2013, p. 234). CoPs have been found to satisfy members’ needs for social connection, belonging, and the sharing of experiences (Corso et al., 2009), and to be a useful way to overcome the learning barriers created by silos and hierarchies (Iaquinto et al., 2011). Some studies have found that CoPs are essentially a problem-solving mechanism (Pattinson & Preece, 2014), and others indicate that CoPs produce important unanticipated benefits through informal networking (Milne & Callahan, 2006).
CoPs as Diverse and Fluid Organizational Forms
Given the variety of benefits and contributions associated with CoPs, it is not surprising that observers have found that the CoP is a diverse and variegated social form. One study suggests that the diversity of CoPs arises out of the situations and contexts in which CoPs operate (Klein, 2008). Some CoPs may be interested in sharing knowledge, while others are more interested in nurturing the creation of new knowledge (Klein, 2008). One review of 82 studies of CoPs found that there is no single, ideal set of organizational arrangements suitable for all CoPs, and there also is no ideal CoP process or set of activities for achieving the goals of a CoP (Bolisani & Scarso, 2014). Specific social situations and contexts call for flexibility and experimentation.
Several studies have delved into the informal and fluid nature of CoPs, and have considered whether a CoP might be controlled or influenced by organizational or system leaders. Some researchers argue that CoPs generate and apply knowledge through a complex interaction of bottom-up or self-directed modes of operation and top-down or guided modes (Borzillo & Kaminska-Labbé, 2011). This argument posits that self-direction involves a search for relevant knowledge through cooperation and boundary spanning, while top-down dynamics involve an expansion of CoP knowledge resources through supportive and empowering leadership activities and a process of adaptive tension that allows the CoP to maintain stability while exploring and responding to new possibilities.
Others contend that research provides scant guidance on how organizational leaders might intentionally design and implement CoPs (Iaquinto et al., 2011). For example, one study found that science-based CoPs tend to take shape organically, without central planning, oversight, or control, and achieve incremental improvements or innovations through specific problem-solving activities (Pattinson & Preece, 2014). Other scholars suggest that it is possible to influence and support CoPs by fostering the conditions for a CoP’s emergence and success (Iaquinto et al., 2011).
A study of 47 CoPs in 21 organizations found that senior leaders can sponsor and manage CoPs without rigidly controlling them, and moreover that sponsorship by senior leaders can be a factor critical to the success of some organizational CoPs (Borzillo, 2009). Management sponsorship can be effected in three ways: by influencing the quantity and focus of CoP innovations; through governance committees that monitor and assess CoP activities; and by promoting the scaling up of CoP innovations throughout the broader organization (Borzillo, 2009). However, this study found that methods for influencing CoPs were implemented differently in different organizations, and that although sponsors exerted some control over CoPs, this is a loose form of control that was accomplished through collaboration with CoP leaders. More recent studies support this view, suggesting that leadership of CoPs that are meant to encourage social learning processes should facilitate collaboration by members rather than overtly direct activities and processes (Fam, 2017; Shaheen et al., 2021).
Other research adds credence to the proposition that a CoP is most often a fluid and informal organizational form. A study of public health CoPs, for example, found that the most successful CoPs were initiated and defined by the empowered members themselves, rather than formed by organizational leaders (Mabery et al., 2013). These findings suggest that strong or rigid hierarchies can be an impediment to an effective CoP. Successful CoPs cut across the boundaries separating programs, occupations, organizations, and geographic regions, and take on concerns that are broadly shared. These authors claim that CoPs “are fundamentally informal” (Mabery et al., 2013, p. 234) and are characterized by shared leadership and flexible roles.
Another study found that CoPs promote knowledge management and learning when the host organization exhibits high levels of commitment to the CoP and organizational members are highly involved and participate fully in the CoP (Corso et al., 2009). This study concludes that CoPs can be fostered and supported by organizational managers, but cannot be fully controlled. Another study found that the organizational or system context that hosts a CoP must provide reasonably stable conditions that allow for ongoing, uninterrupted informal interactions among CoP members (Schenkel & Teigland, 2008).
Mobilizing Tacit Knowledge
Another common finding in the research literature is that CoPs represent a human-oriented approach to managing knowledge, where knowledge is viewed as fundamentally tacit in nature (that is, arising and residing in the minds of knowers and created through complex processes of social interaction) (Azan et al., 2017; Bolisani & Scarso, 2014; Elliott et al., 2023). These studies suggest that the relatively loose and unconstrained social form of a CoP is suited to support knowledge flows through social interaction. Others have argued that the most significant benefit of CoPs is that they promote the creation and sharing of tacit knowledge that arises more from intuition than reason and that is highly contextual (Ardichvili et al., 2006; Castaneda et al., 2018). One study of CoPs in a public health context suggests that a CoP may offer a way to access useful tacit knowledge among members and to link this knowledge with explicit knowledge from the relevant scientific literature (Kothari et al., 2015). One would expect, then, that a CoP that exists in part to access scientific knowledge will also include interaction processes that allow for the sharing of tacit knowledge, and some studies have indeed found strong links between CoPs and collaboration, learning, and innovation (Castaneda et al., 2018).
Factors Associated with CoP Success
A variety of studies have attempted to identify characteristics common to successful CoPs. Some argue that CoPs are successful when their internal processes include networking, reflection on how members experience their practice, and structured problem investigation and resolution (Barbour et al., 2018). Others argue that CoPs do well when members are motivated by internal or personal factors, when organizational or system leaders are supportive, competent and active, and when the organizational culture supports and encourages knowledge exchange activities (Zboralski, 2009). One study attributed the success of a CoP within a postsecondary educational institution to the presence of a core team with one person acting as facilitator, the use of a common vocabulary, the openness of the CoP to new members, and the links between the CoP and existing organizational structures (Bastiaens & Heymann, 2023). Another found that when CoPs promote open communication, a common vocabulary, and mutual learning, members are likely to strive to enhance their personal competence (Matsuo & Aihara, 2022). A recent Canadian study found that CoPs are more successful when there is an active facilitation role supporting the work of the CoP (Kothari et al., 2015), while an Australian study suggests that CoPs benefit from supportive (rather than directive) leadership, fulsome collaboration by multiple CoP members, and continuous spanning of CoP boundaries to bring in new people with relevant knowledge and expertise (Fam, 2017).
Other researchers have looked at the constraints and impediments to CoP success. A review of four CoPs in public health found that time constraints and competing priorities impeded CoP effectiveness (Mabery et al., 2013). Some authors have found that knowledge exchange within a network requires formal support from network sponsors, and that organizational changes and restructuring can inhibit the ability of such a network to survive and be productive (Schönström, 2005).
Some recent literature explicitly explores factors that allow CoPs to move knowledge into practice. Gabbay et al. (2014) examined CoPs as learning communities and noted the importance of ensuring the presence of specific technical skills (e.g., Lean and PDSA methods), soft skills (e.g., conflict management, negotiation, stress management, and leadership), and learning skills (e.g., action learning and critical reflection). They found that a CoP requires institutional support and leadership, and the flexibility to adapt to changing circumstances.
CoPs encourage the interaction and collaboration that many see as essential to the implementation of research evidence (Berta, et al., 2013; Thomas et al., 2014). Collaboration allows for group learning and the leveraging of member expertise (Bonner & Baumann, 2012; Bucknall, 2012; Greenhalgh & Wieringa, 2011), and has been found to positively influence culture change (Dupuis et al., 2014).
The Problem-Solving Role of CoPs
The notion that CoPs play an important problem-solving role is widespread in the literature (Azan et al., 2017; Barbour et al., 2018; Hart et al., 2013; Pattinson & Preece, 2014; Pyrko et al., 2017). Some have argued that a recognition of important and (often) intractable shared problems is a basic reason for creating CoPs, and that a CoP can sometimes help members to share perspectives in ways that generate a new and more coherent understanding of these problems (Furlong & Johnson, 2003). A recent study shows that a CoP of change agents in an Italian university responded to the problems and disruptions brought on by COVID-19, in part through strengthened member relationships, an enhanced sense of belonging, and a clear sense of empowerment (Bolisani et al., 2021). The CoP was found to be well suited to deal with a situation in which faculty needed to share experiences and learn together about functioning during the crisis.
An Australian study of six CoPs considered the extent to which CoPs might offer an effective response to a “wicked problem” such as climate change (Iaquinto et al., 2011). They suggest that wicked problems are dynamic and involve numerous factors that make the dilemma seem intractable. These authors write, “A community of practice, with its emphasis on collaboration and knowledge exchange, could … foster the transdisciplinary approaches of systems science to overcome the compartmentalization of expertise within disciplinary and divisional boundaries (the so-called silo effect), and help … [government departments in] effecting future climate change adaptation” (p. 5).
Problem Solving Through Social Learning
Other scholars and practitioners have considered the dynamic of a human group that uses a situated, social learning process to solve shared problems that are stymieing a practice. The action science perspective suggests that the social learning arising in human groups such as CoPs can be depicted as having the form of a double-loop, or of two “orders” (Argyris, 2004; Bartunek & Moch, 1987). Familiar, well-understood problems are handled through a single loop of learning and problem solving, where actions and resources are designed and implemented and results monitored until the problem is resolved. More complex, poorly understood problems, on the other hand, often require a double-loop approach, where the stubbornness of the problem raises the need to reconsider assumptions, theories and mindsets.
These studies, which frequently combine social psychological and management science perspectives, often posit that double-loop learning tends to occur when team and organizational members are able to engage in honest discussions that are unimpeded by hierarchical power arrangements (Kegan & Lahey, 2016). When occurring within an organizational context, this form of learning can bring about a significant transformation that derives from discontinuous changes to the interpretive schemas or mindsets of organizational leaders and members (Bartunek & Jones, 2017). People encounter perspectives and situations that challenge their customary ways of understanding and acting, experience reflective and dialogic processes that lead them to alter their beliefs, and are then able to design and implement new behaviors that produce transformative changes in their organizational milieu (Argyris & Schön, 1978).
Some researchers and theorists have considered the characteristics of intractable problems, and how a group might enhance its ability to achieve double-loop learning when facing these sorts of dilemmas. The kinds of challenges that require a response informed by double-loop learning have been termed wicked problems or adaptive challenges. A wicked problem is a problem that eludes a definitive description, and is understood differently by different people who are motivated by differing or even incompatible values (Rittel & Webber, 1973). Others have referred to adaptive challenges that relate to unexpected and significant changes in the surrounding context that challenge existing beliefs or values and give rise to divergent opinions (Heifetz & Laurie, 2001; Heifetz & Linsky, 2002). There is no single, correct solution to a wicked problem, but rather a variety of possible solutions that are likely to be supported or opposed by different groups who have an interest in the solution. To solve such a problem, it is often necessary for the affected stakeholders to share perspectives, consider alternatives, and negotiate approaches that will satisfy as many concerns as possible. The response to a wicked problem might thus be thought of as a search for feasible solutions accompanied by testing and monitoring to determine if new approaches are producing the desired results.
Researchers and theorists have considered the most effective ways in which human groups might organize themselves to respond to wicked problems that require double-loop approaches. Some have focused on the leadership stances and approaches needed to resolve adaptive challenges (Heifetz & Laurie, 2001; Heifetz & Linsky, 2002). When facing an adaptive challenge, these authors stress the role of leaders in bringing stakeholders together to share perspectives and to receive new ideas with an open mind, creating the psychological safety needed for people to share controversial perspectives, and facilitating collaborative processes intended to produce concrete plans for action.
Others have suggested that to achieve the capacity to learn and improve it is especially important for organizational leaders to cultivate the condition of psychological safety in their teams (Edmondson, 1999; Edmondson & Lei, 2014). Psychological safety has to do with the beliefs of organizational members about what will happen if they take interpersonal risks as they interact with colleagues in the workplace. The presence of psychological safety has been shown to contribute to efforts to foster social learning processes in teams and organizations (Edmondson, 1999; Tucker, 2007). Others claim that an inability to implement desirable changes and improvements can result from the presence of competing goals that organization members are unaware of (Kegan & Lahey, 2009; Krousel-Wood et al., 2014). These authors recommend a coaching and learning process that allows people to uncover their competing priorities and consider ways of altering their assumptions and behavior.
Still others suggest that improvement is to be found through adopting certain structured processes or techniques that help organizational members to learn and improve as they respond to stubborn challenges. Developmental evaluation has been shown to encourage sensemaking and adaptive learning in the face of complex problems (Patton, 2011; Szijarto, 2019). Some scholars and practitioners in the UK have argued that action learning, with its focus on structured dialogue and the use of probing questions, is well-suited to helping people understand and respond to intractable challenges (Brook et al., 2012, 2015; Sharp, 2020). Many organization development practitioners and scholars recommend variants of the action research method as a useful way to integrate social learning with problem solving (Conklin, 2021; Jones & Brazzel, 2014; Schein, 1999), and the most recent approaches in this field of practice emphasize the importance of dialogic processes to bring multiple stakeholders into collective problem solving forums (Bushe & Marshak, 2015; Hastings & Schwarz, 2022).
These suggested stances and techniques to enhance a group’s capacity to learn, improve, and solve intractable problems rely on bringing people together in a loose social milieu, where power differentials are minimized, and where dialogue and relationship building might occur. A number of scholars have recently argued that CoPs facilitate organizational learning by encouraging people to carry out an inquiry and learning process that allows members to better understand and take action to ameliorate or resolve complex challenges (Friedman, 2006; Gherardi & Nicolini, 2000b; Kesavan, 2021; Raelin, 2008). In this monograph we suggest that a CoP, with its inherent social learning process and its propensity to create and expand networks of implicated or interested stakeholders, may represent a social form that is well positioned to create a double-loop learning and problem solving process.
Researchers also state that more work is needed to help us understand the specific factors associated with successful knowledge translation and to develop models, frameworks and strategies for successful implementation (Currie et al., 2014; Mazer et al., 2015; Nilsen, 2015). Some note that most CoPs studied by social scientists have been located in the private sector, and there is a need to look at CoPs in the public domain, particularly in healthcare (Bolisani & Scarso, 2014).
Main Points Derived from the Literature
The existing research evidence reviewed here suggests that CoPs can be an effective strategy for moving knowledge into action. We derive nine key points from this review. First, KTA is a social process of interaction and learning that helps people to access, appraise, create, and share relevant knowledge. Second, CoPs are a social form capable of enacting these social processes, and CoPs deliver a variety of benefits, including overcoming social barriers related to power, creating new organizational capacity, enhancing collaboration, and diffusing the tacit knowledge of expert practitioners. Third, CoPs tend to be diverse and fluid organizational forms that benefit from leadership support, but that generally are not amenable to tight management control. Fourth, much research emphasizes the overriding importance of tacit knowledge for most CoPs. Fifth, CoP success correlates with factors such as spanning organizational and geographic boundaries, internally motivated members, supportive leadership, supportive organizational culture, and a portfolio of important skills related to problem solving, relationship building, collaboration, and learning. Sixth, CoPs are fundamentally associated with social learning or learning in groups. This learning sometimes is concerned with learning to be part of a culture and to perform certain tasks, and it also is sometimes associated with encountering and responding to the shared problems of a practice. Seventh, the organizational learning literature has considered the dynamics of a human group that uses a situated, social learning process to solve shared problems that are stymieing a practice. One common way of representing these dynamics is in terms of two forms of learning: single-loop learning with a feedback loop that can target changes and improvements exclusively toward the problem solving actions of the group; and double-loop learning whose feedback loop can provoke transformative changes in mindsets, assumptions, and values as well as in their associated problem-solving actions. Eighth, some theorists and researchers have considered ways of enhancing a group’s ability to achieve double-loop learning when facing intractable problems, with a focus on leadership stances, psychological safety, and process techniques such as developmental evaluation or process consulting. And ninth, more work is needed to fully understand CoP success, and work is especially needed in public sector and healthcare contexts. The study reported here builds on the existing research base and focuses on public sector, health care CoPs.
Methods
The Context in Which Our Research Occurred
Our study looked at nine cases of KTA processes that were mobilized through CoPs operating in a knowledge network in the seniors’ health sector in Ontario, Canada.
The Seniors Health Research Transfer Network (SHRTN) collaborative, an Ontario-wide knowledge network, was established in 2005 with the aim of facilitating knowledge exchange between caregivers, researchers, and policymakers (Conklin et al., 2007). It was hoped that this enhanced level of knowledge exchange would benefit research, education, practice, and policy, and would ultimately improve the care of Ontario seniors. To facilitate knowledge exchange, SHRTN created CoPs that were seen as dynamic social contexts that would adjust to ongoing changes to their leadership and external environment (Provan & Milward, 2001).
To create the CoPs, each year SHRTN issued a call for proposals that invited interested individuals and groups to submit plans to operate a CoP whose purpose was to facilitate KTA processes in the seniors’ health sector. Typically, the proposals would aim to remove or reduce a knowledge gap that existed in Ontario long-term care (LTC) homes and other practice sites where care is provided to seniors. CoPs would often be formed by a small group of health professionals who worked in a specific area of care, such as oral health, dementia care, diabetes care, wound care, falls prevention, and so on.
Each CoP submitted a plan for one fiscal year, and if accepted by the SHRTN board of directors the CoPs received modest funds (generally not more than $20,000 CAD) to cover the cost of needs assessments, teleconferences, face-to-face meetings, and CoP-sponsored educational events and information products. CoPs were expected to submit quarterly reports to the SHRTN secretariat.
SHRTN also employed a team of information specialists (librarians) who helped CoP members to access resources available through the province’s institutional libraries, along with a team of knowledge brokers (KBs) who were assigned to assist the CoPs with strategic issues and operational tasks. SHRTN KBs facilitated learning processes based on both explicit and tacit knowledge to help CoP members to solve problems, and provided logistical, technical, and administrative support to CoP leaders (Conklin et al., 2013).
All SHRTN CoPs tended to follow the same basic steps. They began by identifying a need or gap that was affecting the ability of practitioners to provide appropriate care to Ontario seniors. They then attempted to assemble knowledge that could help to meet the need or reduce the gap. They then designed and implemented activities intended to move this relevant knowledge toward frontline practices, where it was hoped that practitioners would be able to implement improvements in their practice routines. In carrying out these steps, most CoPs engaged with a variety of knowledge users (who in SHRTN’s case would generally include health care providers, often in LTC homes, who make use of knowledge while performing their roles) and other stakeholders, inviting them to participate in the planning and design work and encouraging them to participate in educational and follow-on activities.
This approach resembles the learning cycle described by Wenger and colleagues that includes reflecting together on shared concerns, taking action in practice contexts, and then engaging in a process of social learning within the CoP (Wenger et al., 2002). However, SHRTN CoPs have two additional characteristics not included in Wenger’s model. First, their intent was to influence practice locations across the province (for example, all LTC homes), and not just those in which CoP members were directly employed. SHRTN believed that the CoPs might achieve this aim by hosting events that would be open to practitioners from throughout Ontario. Second, SHRTN CoPs were nested within and supported by the broader knowledge network that provided technical and financial resources. This meant that SHRTN CoPs were required to carry out the activities described in their proposal to SHRTN, were supported by a modest financial grant and by the expertise of their KB and information specialist, and otherwise were free to establish their own goals and action plans.
During the time of our research, SHRTN CoP members included health care practitioners, researchers, policy makers, educators, librarians, and others. These CoPs tended to form around a core group of leaders, with a larger group of members who participated in CoP activities. CoP leaders and members worked in many different health, educational, and government organizations throughout Ontario.
Our research began as the network operated under its third budget (funded by the province), running from 2009 to 2011. As this 3-years funding came to an end and the network attempted to secure new funding, SHRTN began to operate as two separate networks: the Seniors Health Knowledge Network (SHKN) and the Alzheimer Knowledge Exchange (AKE). The separation of SHRTN into two parallel networks was carried out in an amicable manner, and the leaders of SHKN and AKE described themselves as partners (Alzheimer Knowledge Exchange, 2012). Both networks continued to pursue their mandates by funding and supporting CoPs, and in the third year of our research we worked with two SHKN CoPs and one AKE CoP. During this time uncertainty arose concerning the resources required to sustain the network and complete projects that were underway.
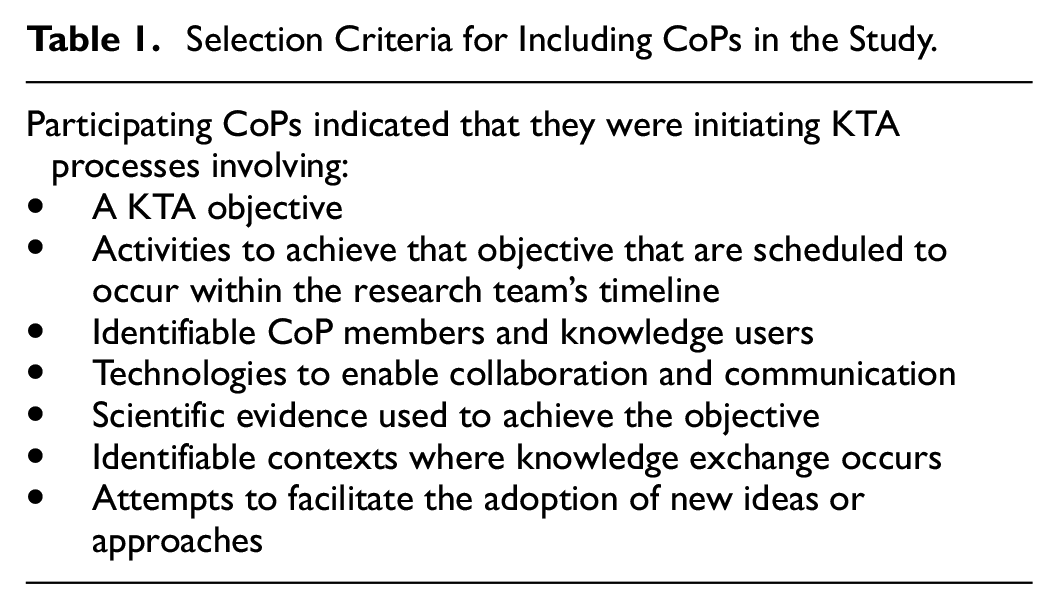
When we formed our research team, SHRTN was supporting 19 CoPs formed around topics such as persons with aphasia and communicative issues, activity and aging, continence care, elder abuse, and end of life care. Over the three years of our study we worked with eight different CoPs on nine case studies (in other words, we worked with one of the CoPs on two separate case studies), and each case study was carried out over a period of approximately twelve months. Purposive sampling was used to identify and select cases for inclusion in the study. All active SHRTN CoPs were invited to participate in our research as a case study. CoPs that indicated an interest were selected on the basis of the criteria described in Table 1.
Selection Criteria for Including CoPs in the Study.
Because of assurances that we provided to participants through the project’s ethics process, we are unable to provide the names of the CoPs or their initiatives that were included in the study. Instead, we identify the nine case studies (each focusing on a CoP and its KTA initiative) by an alphanumeric identifier, as shown in Table 2. The fourth character in the identifier indicates whether the CoP was studied during the first, second, or third phase of the investigation.
The CoPs and Their Interests.

Data Collection and Analytical Methods
A detailed methods protocol for this study was published in Implementation Science (Conklin et al., 2011). The following paragraphs provide a summary of these methods.
Our study was designed to allow us to understand the KTA processes that were enacted in nine CoPs operating in the Canadian health system, and how human agents brought those processes to life. When positive change occurs through the efforts of a CoP situated within a knowledge network, what precisely happens? Wenger and colleagues often discussed how CoPs helped to create and maintain the expertise in a practice, but here the SHRTN network sponsors hoped for an ongoing process of problem solving and innovation through which research knowledge would be translated into relevant, useful practical knowledge. Did this happen, and if so how did it happen? What affordances are opened up through the work of the CoP, and what constraints are encountered and overcome? What does the process of KTA look like? What patterns of human behavior bring the processes to life?
We used the Promoting Action on Research Implementation in Health Services (PARIHS) framework (Harvey et al., 2002; Kitson et al., 1998, 2008; Rycroft-Malone et al., 2002; Rycroft-Malone, Harvey, et al., 2004; Rycroft-Malone, Seers, et al., 2004) as a conceptual frame to guide our data collection. PARIHS sees KTA as an interplay between three dimensions: the evidence being transferred, the organizational context where evidence is implemented, and the facilitation processes used to achieve the implementation. According to PARIHS, KTA succeeds when evidence is relevant and coherent for the context where it is implemented, when local contexts are able to absorb useful new evidence, and when facilitation processes help practitioners to understand and use the new knowledge (Kitson et al., 2008).
PARIHS helped us to define the constituent elements of a case: the evidence being mobilized, the KTA processes and activities that were used, and the contexts in which KTA activities occurred. Case study research often makes use of a conceptual framework to inform the data-collection process (Collins & Stockton, 2018). Our use of PARIHS focused our attention on KTA processes and activities that were devised and implemented by the CoPs, and thus informed our data collection protocols. We observed and gathered data on the facilitative methods used by the CoPs that we studied. We looked for and identified the characteristics of the types of knowledge assembled or created by the CoPs, which led us to examine the use of tacit and explicit knowledge in the CoPs’ KTA processes. We identified and studied the locations where KTA processes took place, which frequently involved the collaborative planning activities of the CoPs, and the use of webinars to move knowledge into practice.
This study used a multiple case study design and qualitative methods. Case study design allows researchers to empirically explain complex social phenomena (Yin, 2009) such as the KTA processes that occur within and through CoPs. A multiple case study design was selected so we could examine a complex social phenomenon (KTA processes) that occurs differently in multiple situational contexts (Anaf et al., 2007; Baxter & Jack, 2008; Stake, 2006; Tellis, 1997). This design allowed us to describe and explain complex social phenomena occurring within and across organizational boundaries, such as the KTA processes that occur within and through CoPs and that extend to frontline settings (Connell et al., 2001).
Multiple case study designs can contain any number of cases, so long as the number is greater than two (Yin, 2009), and a total of nine cases is considered appropriate (Audet & d’Amboise, 2001; Marshall et al., 2013; Stake, 2006). With a team of three principal and three co-investigators supported by research staff, with funding to carry out data collection for three years, and with CoPs that were operating on the basis of twelve month plans, we had the capacity to undertake three case studies in each of three years, for a total of nine case studies. This meant that we would be able to triangulate results each year, and would also be able to triangulate the cross-case analysis produced in each of the three years. We thus divided the project into three phases, each of which included three case studies. Each principal investigator (PI) led one case in each phase, with one PI (the first author) leading the cross-case analysis at the end of each phase.
Each case involved a KTA initiative led by a CoP. A case consisted of the CoP’s KTA objectives and activities, the people, structures, and technologies used to support these activities, the evidence mobilized by CoPs to achieve objectives, and the places in which knowledge exchange and implementation occurred. By conceptualizing a case in this manner, we were able to identify and follow most KTA processes from beginning to end, and were able to identify the roles played by CoP members as they implemented their plans.
Data were collected through a combination of ethnographic observations, semi-structured interviews, and the gathering of key documents relevant to the case (Patton, 2015; Stake, 1995, 2006; Yin, 2009). Observers and interviewers were trained to ensure consistency in the data collection, and data were captured using structured templates.
Consistent with our ethnographic approach, observational data were gathered through observations at planning meetings, CoP interactions with potential knowledge users, and CoP interactions with SHRTN planners and managers. These data were recorded in field notes that made use of a template that separated observations from observer interpretations. Interview data were gathered through informal and semi-structured interviews. All cases began with semi-structured interviews of CoP leaders to gather contextual data. At this time CoP leaders were also asked to share relevant CoP documents, such as needs assessments, meeting minutes and SHRTN reports. As the case studies progressed and drew to a close, we conducted additional interviews with CoP leaders and knowledge users that helped us to understand the evidence that was being accessed and transferred, the contexts that were receiving the evidence, and the facilitative mechanisms that were being used, and that also highlighted the interplay of explicit and tacit knowledge in the CoPs’ activities. These interviews allowed participants to look back on their experiences and to reflect on their challenges and successes. Data gathering was concluded when saturation was reached. All observational field notes and interview transcripts were imported into an NVIVO database. Each case study used the same structure for their case study databases, to facilitate cross-case analysis at the end of each phase.
Analyzing qualitative data is often an exercise in pattern recognition. Analysts search for and recognize the patterns in the data relevant for the questions that were asked and, more broadly, relevant for the concerns that led them to ask those questions in the first place. They then draw inferences and make interpretations based on those patterns.
Our analytical strategy was to describe the people, knowledge, activities, and contexts that were involved in the KTA processes of each case study; to analyze how these KTA process unfolded by revealing interactive patterns; and to interpret these descriptions and analyses in ways that allowed us to suggest their meaning (Wolcott, 1994). This approach permitted us to understand the unique features of each case as well as how the social phenomenon we were studying (KTA processes in CoPs) manifested themselves across all cases (Stake, 2006).
Analysis for each case consisted of five steps: (i) review of all data sources and creation of a narrative description of the case; (ii) analysis of data using deductive or directed coding methods; (iii) formulation of answers to the research questions with iterative team discussion; (iv) re-analysis of the data with inductive or open coding and thematic methods; and (v) a cross-case analysis of findings for each phase and, at the end of the investigation, for the nine cases, again informed by team discussion (Braun & Clarke, 2006; Hsieh & Shannon, 2005; Stake, 2006).
In the first analytical step, one researcher read the data from beginning to end, making notations and analytical memos and reflecting on the research questions. During this review, the researcher created a detailed (or “thick”) narrative description of the case (Geertz, 1973). The narrative reports for each case study used a common table of contents, to facilitate the cross-case analysis. Throughout the course of the study the research team met via teleconference every 2 weeks to ensure that the work remained aligned. Drafts of the narrative reports were reviewed by all investigators, and suggestions for improvements were incorporated before the reports were finalized.
The second analytical step began after the narrative reports were complete, when each case study team undertook a comprehensive analysis of the data using deductive coding and categorizing procedures (Creswell, 1998; Hammersley & Atkinson, 1995; Lincoln & Guba, 1985; Merriam, 1988). The deductive coding process involved reviewing the data for a case in relation to the research questions that were asked. Using NVivo’s coding functions, codes that helped to elicit answers to the questions were created and defined. As the coding progressed, the analyst created a code book consisting of a numeric identifier for each code, the code name and description, cross references to the code’s location in the data set, and the number of data sources where the code originated.
When this coding exercise was complete we moved to the third analytical step. The analyst examined the codes that had been created for each research question and clustered the codes into categories. The analyst then read through this organized data in relation to each question, and drafted an answer to the questions that was consistent with and grounded in the data. This draft was then shared within the specific case study team and was revised and improved. Finally, the draft was shared with the full research team, and suggestions and improvements were considered before the answers were finalized.
The fourth analytical step involved a process of open, inductive coding that gave us a distinct way of deriving meaning from a large qualitative data set (Braun & Clarke, 2006). Instead of starting with a frame constructed from predetermined research questions, we invited the data to reveal its own underlying structure—the patterns that are inherent in the experiences recounted through interviews and observations. We began by identifying small units of meaning—distinct meanings that arise from what our informants saw, heard, felt, and thought. After completing the coding, we took note of the number of codes that had been created, the number of times that specific codes appeared in the dataset, and the number of data sources that specific codes were found in, and we then identified strong codes that were well-grounded in the data and weaker codes that appeared only a few times or in few data sources. Weaker codes could represent outlier perspectives on the KTA experience, and the qualitative paradigm calls for the retention of both strong and weak perspectives in a dataset (Lincoln & Guba, 1985); however in a few cases the weaker codes were found to be a rephrasing of an existing code, and in those cases we integrated the weaker code with stronger code.
We then reviewed and sorted the codes that resulted from this exercise into larger categories of meaning—forces, perspectives, issues, opportunities, and challenges that were evident in the nine case studies. Having considered and described the make-up of these larger themes, we then looked at how the themes co-exist within the bounded and open ecosystems that were constituted by the CoPs, the knowledge network in which they were nested, and the broader health system in which they functioned. To carry out this step we used a facilitation technique designed to allow a group of people to make sense of large amounts of written data (Oyler & Harper, 2007; Spencer, 1989; Stanfield, 2013). The investigators and research staff would review the codes and consider ways in which individual codes might represent units of larger thematic categories. When this clustering process was complete, the analysts would give a name to each thematic cluster, and write a narrative description of the broader theme that also was consistent with all of its constituent codes. Once this was done, the analysts would discuss how the different themes interacted with each other during the case study, creating a dynamic of the patterned thinking of CoP members and other stakeholders (for example, their goals, concerns, values, assumptions, etc.), their patterned behavior (the actions that they took to plan and implement their KTA initiative), and their structuring (the tools, technologies, policies, and procedures that they relied upon as they carried out their work). The results of these analytical steps were then recorded in the case study report, which by this time already included the sequential narrative of the case and the results of the deductive analysis.
The fifth and concluding analytical step saw the lead PI carry out a cross-case analysis at the end of each phase and at the conclusion of the overall project. The purpose of this step was to elicit an understanding of what the nine cases, taken together, reveal about the KTA processes mobilized through these CoPs and about the roles played by the people who participated in these processes. To accomplish this, the lead PI read through the outputs from the analytical processes for the case studies under consideration, and noted similarities and differences across the cases. This included a comparative analysis of the answers to the research questions produced by each case study. The inductive portion of this analysis involved looking at the themes generated through the open-coding process, and at the dynamic pattern of thought, behavior, and structuring evident in the case. The lead PI identified similar themes that spanned three or more cases, and wrote a cross-case theme name and description to indicate the meaning and importance of these higher-level groupings. These cross-case findings were circulated among the researchers, and a meeting was convened to allow for discussion and suggestions, after which the cross-case analysis was finalized. This process yielded answers to the research questions along with the thematic findings and tables presented in this article, along with the two illustrations (Figures 1 and 2) that depict an overall pattern of learning and action evident in most cases.

Theory of action evident in most cases.

Pattern of learning evident in most cases.
To ensure the trustworthiness of our findings, we relied on Patton’s suggestion that each researcher have the qualifications to carry out the study (Patton, 2015). Our team included skilled researchers with a combination of formal training and practical experience in the use of all methods in the study. We also provided annual, rigorous methodological training for all research personnel who participated in the data gathering and analysis. Lincoln and Guba have written that qualitative research must produce credible, transferable, dependable, and confirmable results (Lincoln & Guba, 1985). The credibility of our findings was assured through member checking, and through annual discussions of our emerging findings with SHRTN stakeholders. Transferability was assured through the creation of “thick descriptions” allowing readers to assess the applicability of the results to other contexts. Dependability involves our finding’s internal coherence, which we assured through member checking, reviewing and editing steps involving the full research team. Confirmability (requiring that conclusions be well-grounded in data) was assured through the coding and theming procedures described above. Many qualitative experts note that triangulating situations, informants, researchers, and methods helps to assure that qualitative research produces trustworthy results (Creswell & Miller, 2000; Denzin, 1978). Our study provides triangulation of situations, informants, researchers, and data-gathering methods. Moreover, Creswell and Miller (2000) suggest that validity in case study research is established by accurately representing the way in which participants view the phenomenon being studied, and by the extent to which participants see the findings as credible. We used eight of the validity procedures proposed by these authors: triangulation, member checking, disconfirming evidence, prolonged engagement, thick description, researcher reflexivity, collaboration, and peer debriefing. This study was funded by an Operating Grant from the Canadian Institutes of Health Research. The study received ethics clearance from the University Human Research Ethics Committee of Concordia University (reference number UH2010-115), the Bruyère Research Ethics Board (reference number M16-11-004), the University of Waterloo Office of Research Ethics (reference number 16894), and the University of Western Ontario Research Ethics Board for Health Sciences Research Involving Human Subjects (reference number 17879E).
Results
We now present the results that were produced by our analytical methods. We begin with a brief summary of the main points from the narrative descriptions of each case. We then present the findings from our deductive analysis, after which we present the findings from our inductive analysis. Finally, we offer our thoughts on the overall meaning of these findings.
Summaries of the Narrative Descriptions of the Case Studies
This section presents highlights from the narrative descriptions produced during the first analytical step. The full case reports were detailed and voluminous, sometimes running to over 100 pages including appendices. We include highlights here to help readers to understand the people and events that make up the cases we studied.
CoP1P: Designing LTC Homes for Residents with Alzheimer’s Disease and Related Dementias
CoP1P was concerned with the disorientation and agitation experienced by LTC residents living with dementia as they tried to find their way around the LTC home in which they lived. This issue was considered important because responsive behaviors (a term often used to describe the behavioral challenges characteristic of this patient population) can be triggered when people become confused as they make their way around the home.
This CoP addressed the problem by creating a set of design recommendations for LTC homes that included incremental improvements as well as more comprehensive design changes that could be incorporated in the LTC environment. The CoP disseminated the recommendations by designing and hosting a webinar.
CoP1P was composed of researchers, design experts, experts in dementia, and people with direct experience of LTC homes. The core group that carried out the initiative included a KB, two co-leads, a group of planners (ranging from five to nine people) that changed over time, and an information specialist who conducted literature searches. (All of the KBs and information specialists described in these case summaries were employed by SHRTN and were assigned to support the CoP.) The core group assembled research evidence and regulatory requirements concerning lighting, doorways, noise, and wayfinding (the term CoP members used for people finding their way around the LTC home), and also studied the needs of people living with dementia. This resulted in a set of recommendations for floor layout, hallways, landmarks, memory boxes, washrooms, and meaningful experiences.
This CoP’s collaborative planning process drew on explicit and tacit knowledge to develop the recommendations. The core team began with published qualitative and quantitative research studies, and members contributed practical insights based on their experiences while working in LTC homes. The core team’s composition changed over time as members reached out through their networks and brought in new expertise.
Despite the fluid and changeable composition of the core team, we were told that the team worked well. One member stated: “I have to say, the entire group is amazing to work with and one of the reasons why I like to call her a co-lead is because she’s always been somewhat of a silent partner, but she really is, and you can share this with her, I think she’s really a very important part of the backbone of the CoP…She’s brilliant. Oh, everybody is, honestly. We’ve got this librarian goddess who keeps us all on track and we’ve got these inspired passionate people that really enjoy coming together.” The group also welcomed and appreciated the contributions made by knowledge users (frontline LTC workers who were part of the core team). One participant commented, “The group is highly organized and supportive of one another. They ensure that each member has the opportunity to voice their opinions and ask questions. They also have several knowledge users on their core team which enables the knowledge from the literature to be supplemented by individual experience and expertise.”
When the guideline was complete, the team hosted a webinar in which a small audience reacted to the materials. About 25 people participated in the session. At the time of this initiative, the idea of wayfinding in LTC homes was relatively new, and team members hoped that their work would contribute to a shift in understanding among stakeholders about the importance of the topic. As awareness and interest increased, the CoP intended to take additional steps to share the recommendations with frontline care providers, administrators, and policy makers.
Although much of the CoP’s attention was taken up with achieving its immediate, short-term goals of developing a set of wayfinding recommendations, their long-term aim was to facilitate the development of new capacity in the LTC sector. They did this in part by building a larger network of people who were connected to the CoP. Through this growing network of practitioners, they wanted to develop innovative approaches to the problem of responsive behaviors by helping people to understand the incremental and transformative changes that could bring improvement.
CoP1P participants told us that they were aware of incremental improvements being made in some LTC homes based on their recommendations. However, they also indicated that broad uptake would not happen without the support of provincial policy makers. This highlights a point that we encountered in several case studies: the CoP investigates and attempts to fill a specific knowledge gap, and starts by believing that an incremental change, often involving education, will achieve the desired result; however, while attempting to design and implement an incremental change, often involving a knowledge product such as CoP1P’s design recommendations, the CoP leaders realize that the desired change will only occur if multifaceted interventions are targeted at multiple levels in the health system.
CoP1O: Improving Oral Health Care for LTC Residents
CoP1O was formed to address concerns that the oral health needs of LTC residents were often not receiving appropriate attention. They aimed to ameliorate this problem by raising awareness, providing education, and promoting collaboration and networking between the LTC and dental care sectors. To do this, the CoP assembled relevant knowledge and offered a webinar series to raise awareness of oral health issues in senior populations among professionals working in LTC (and hospital) settings. CoP members wanted to transfer step-by-step skill-based knowledge through webinars, and they archived the webinars for ongoing use. While our research team worked with the CoP, members built on earlier work by producing seven webinars that tackled practice-based skills relevant for specific populations (e.g., stroke survivors) or oral health conditions (e.g., halitosis).
With its specialized topic area, CoP1O was relatively small, with members linking the CoP to their own informal and formal networks of professionals who were interested in oral health care of frail older adults. One member acted as the group leader, and much of the work on this initiative was carried out by four CoP members as well as a SHRTN KB and information specialist, with occasional help from a small planning team.
The CoP used best practice guidelines and research syntheses to develop the webinar content, and they tailored the webinars to the needs of their intended audiences. In addition to explicit knowledge sources such as research studies and clinical guidelines, they accessed the tacit knowledge of CoP members to better demonstrate the practicalities of providing oral health care. One CoP member explained, “I think especially when people can see things being carried out, like you know for example being able to view what it looks like to, tooth brush technique or oral care, doing oral care with a behavioral kind of patient, it’s good I think for staff to be able to see the process of how things are being done…”
CoP1O’s collaborative planning process allowed access to a network of experts and potential participants. Much of the work involved designing and developing the webinar content. The live webinars used a 15-minute presentation followed by a 15 minute discussion session, and archived webinars were less than 15 minutes in length. The final recorded webinars were archived on a partner website.
Although this CoP focused on skill-based training, members came to realize that improving oral health care in LTC homes also required culture change and capacity building. Members came to realize that in addition to needing training, those on the frontlines who were doing oral health (mainly Registered Nurses [RNs] and personal support workers [PSWs]) needed mandates and support from their organizations’ senior management. In most organizations, however, this support was lacking. As CoP members designed and implemented their training webinars, they began to discuss the importance of creating a culture of awareness and support among senior leaders. Members realized that an intervention targeting senior leaders in LTC homes was an undertaking that differed substantially from their efforts to create webinars.
Like the CoP1P case, this oral health initiative shows a group of leaders and practitioners who find a way to address a knowledge and skill gap in the LTC system, and who come to realize that to fill the gap they must intervene at multiple system levels. It is not enough to improve the skills of frontline workers. They must also encourage policy makers and LTC leaders to recognize the importance of oral health care, and to set the appropriate priorities for frontline staff. This case study thus reveals the unexpected complexities of KTA activities within the context of CoPs, where best-practice evidence is accessed, adapted, and contextualized for use.
CoP1R: Meeting the Needs of People Living with Dementia Who Exhibit Responsive Behaviors
CoP1R brought together people, resources, and knowledge to encourage the development of new practices that would better support seniors living with dementia who exhibited responsive behaviors (which this group viewed as unpredictable agitation or aggression on the part of a person living with dementia). A core group of provincial leaders formed the CoP and developed the initiative that we studied, which one member saw as a discursive approach to improvement and change: “Within the context of the [CoP], because they have inroads to all of … these regions and all these local areas and these local champions, …they’ll be facilitating a more direct local discussion, multiple local discussions I should say, to help people take the information that they have got globally, or provincially, and then do something with it … in their own day-to-day practice.”
The CoP facilitated change by bringing peers and experts throughout the province into “local conversations” to consider the current situation in their communities and to devise improvements. CoP1R leadership was a shared, collaborative process, in which new participants assumed leadership roles as people worked together to plan activities, hold local conversations, and follow up on new ideas and relationships. These activities allowed them to build an ever-larger network of people who were involved in designing and implementing the desired changes.
The initiative began with four provincial co-leads and one SHRTN KB. These individuals became the main points of contact for an expanding group of regional leaders and participants. Over time program leaders from throughout the province became involved in the CoP and collaborated on the planning and implementation of local conversations. A typical local conversation would begin with introductions and then a brief presentation about responsive behaviors by an expert. This would be followed by table discussions at which local leaders and professionals discussed issues concerning responsive behaviors in the local area, and then agreed on ways to bring about improvement in their region.
When we invited participants to describe the knowledge that was the basis for CoP1R’s work, most referred to the “local conversations” whose purpose was to bring people together to discuss ideas and options for improving care. In this case study the relevant knowledge was distributed throughout the system and was predominantly tacit. One participant explained: “A lot of it is tacit knowledge. Knowledge that participants have accumulated through our own experiences. Sometimes where we think it works, sometimes where we think it doesn’t work. Our knowledge of the system as we know it, the behavioral support system, or non-system if you will, about how behavioral support services are made available, are made to work, or sometimes that we are working at cross purposes. Our knowledge of how the system itself functions. Our knowledge of how service providers work together, or not work together, is not in the same sense as knowledge like a model of clinical care.”
The CoP1R initiative was thus not about transferring a packet of knowledge (created by scientists) into frontline contexts. Rather, our interviewees told us about knowledge that could create more connectivity within the health system (i.e., knowledge about the roles, goals, interests, and activities of other individuals and groups who could be called upon to form local alliances when pursuing change).
The two main facilitative processes used in the case were the collaborative planning sessions convened by CoP leaders, and the local conversations that were used to engage local communities. Regional leaders were recruited who were embedded in regional and local health networks, and who were prepared to facilitate innovation and change by working with local participants and contexts. CoP leaders consulted with regional leaders throughout the planning process.
Knowledge users in this case included virtually all health care providers (HCPs) working with people with dementia who exhibited responsive behaviors. They were fully involved in the initiative. One of our interviewees commented, “The thing that is sort of interesting to me is that it’s a permeable barrier in that in the normal format what you get is tool kits that are given to everyone to implement but in this case what we have is information flowing back and forth from the front line people back to the project leads and then back again and it is sort of a continuous flow. So it means that the sort of ultimate learning that we all do is that much richer.”
Participants in the CoP1R case study conceived of moving knowledge into action as a process of learning and capacity building. As one CoP leader explained, “It is about … pulling ourselves together to learn how to work together and we actually, in the course of doing the work that we are doing, because we are working together, we are learning to work together which is ultimately going to strengthen the system that we create ourselves through our own experience and the upshot of that will be that clients that we serve who have responsive behaviors will get a seamless experience and will get a better quality of care.”
The work of CoP1R culminated in a meeting with an Assistant Deputy Minister of Health who was working on the Alternate Level of Care (ALC) issue, which is a term applied to a patient who occupies a hospital bed simply because the patient cannot be sent home (usually because of a health situation) but who does not need hospital care. An ALC patient is in effect wasting system resources and may be preventing another patient from receiving needed care. When CoP1R was holding its local conversations, 34% of hospitalized people with an ALC designation were people with dementia who exhibited responsive behaviors, and who could not find an LTC home willing to accept them. One CoP1R interviewee told us, “I remember the day that the ADM was told that the ALC problem is a dementia and behavioral problem. He said, ‘Really?’ And, ‘You mean that 34% of people in the ALCs in hospitals are people with dementia?’” (The percentage figure was provided by our interviewee. For a more accurate—though equally alarming—estimate of the percentages, see the 2014 study by McCloskey and colleagues.) This realization galvanized the interest of provincial policy makers around dementia and responsive behaviors. In short order, a new provincial initiative was created whose goal was to increase the capacity of health care workers and informal caregivers in the community and in LTC to work effectively with people with responsive behaviors.
CoP2T: Teams Supporting HCPs Who Work with Responsive Behaviors
The CoP2T initiative was launched because of the new funding made available by the province to support seniors in community and LTC settings who exhibited responsive behaviors (see the final paragraph in the previous section). CoP2T’s mandate was to form and deploy regional mobile teams that would support HCPs in community care and LTC in dealing with specific situations, and who would also transfer skills through mentoring and training. We worked with CoP2T while they were forming and developing tools and processes for the mobile teams.
The CoP2T Initiative was led by two core members and was supported by a KB. Membership was fluid during the period when we gathered data, and consisted mostly of regional health managers who were responsible for creating the mobile teams in their regions. Participants were located throughout the province, and they met each month via teleconference with supporting web technology to enable document sharing.
CoP2T’s purpose was to support the formation and operation of teams that would facilitate the adoption of best practices in managing responsive behaviors by frontline HCPs throughout the province. The CoP was interested in identifying common issues around responsive behaviors that were causing problems for HCPs. The CoP would then address those issues by accessing the tacit knowledge of skilled practitioners and also by locating any literature that might be helpful. Expertise and resources were shared through conversations and documents.
One participant advised us that the CoP relied primarily on tacit knowledge: “There was a … search, people with lived experience and I think about a couple of thousand people were interviewed and there were 200 practice-based champions that identified the critical issues and the go-forward strategy. So it was that foundational literature, evidence from lived experience, evidence from the practice that informed the framework and the collaborative basically I would say the emphasis has really been surfacing practice-based knowledge.”
This CoP used an ongoing planning process, consisting of monthly meetings attended by CoP leaders and the changing group of regional leaders, most of whom had administrative positions in Ontario’s Local Health Integration Networks (LHINs) (which at the time played a health system planning role within 14 regions in Ontario). At these meetings the group defined the mobile teams in terms of function, scope, depth, breadth, reach, and function. The meetings were well attended, with the fourteen LHINs represented at most meetings.
While our research team worked with this CoP, all members were either provincial leaders employed by the new provincial initiative to improve the management of responsive behaviors, or administrators with a health services planning role in the province’s LHINs. No CoP members were members of a specific mobile team. While we worked with CoP members, some began to state that it would be beneficial to involve the actual members of mobile teams in CoP discussions: “So we did talk that it’s time to look at the frontline people coming to the table because whatever I think when I was involved in other collaboratives I usually was doing some of that frontline work and that was where it was the richest because you could really tell the story.”
CoP2T was an opportunity for people involved with responsive behavior mobile teams to share learnings, case study examples, assessment tools, etc., thus allowing for an exchange of useful information among the teams. However, the people who participated in these CoP discussions were representing and speaking on behalf of the frontline providers. Before and after CoP meetings, organizational representatives from the LHINs would meet with frontline providers to share learnings from the meetings, or to gather concerns that they would bring up at subsequent meetings. Some research participants came to believe that their efforts would be more successful if the frontline members of the mobile teams were invited to join the CoP.
CoP2DD1: Promoting Cooperation Across Health Sectors
CoP2DD1’s goal was to facilitate ongoing dialogue on issues related to aging and developmental disabilities, and to promote cross-sector learning between professionals working in the senior’s health and the developmental disabilities sectors. The CoP believed that it was essential for representatives from the two sectors to build a new network of practitioners whose relationships and collaborations would yield effective responses as increasing numbers of people with developmental disabilities were moving into LTC homes (where LTC HCPs had little experience of working with this patient population).
The CoP2DD1 initiative concerned the care of people with intellectual disabilities who were living with dementia. Activities included two webinars that presented survey findings relevant for the topic, a “SHOWCASE event” that presented guidelines for caring for this patient population, and a series of face-to-face conferences to develop linkages and partnerships between the sectors. Most of our data collection concerned the SHOWCASE event.
SHOWCASE was a three-stage approach to disseminating knowledge that SHRTN CoPs had developed in the years before our research study began. A SHOWCASE process began with a webinar that presented guidelines; this was followed by an online forum that allowed for discussion and problem solving while people applied the guidelines; and the process ended with a webinar during which experts and participants shared experiences concerning their implementation successes and challenges.
Much of the work in this case was done by a working group of 15 members, and 3 key people provided leadership in distinct ways. One person acted as an administrator who handled most of the coordinating and planning. The KB took the lead on everything related to technology. A third person provided leadership in terms of subject matter expertise, research, networking with experts, and pulling together content.
This initiative relied on explicit and (especially) tacit knowledge. The SHOWCASE event began by encouraging an understanding of the guideline (which some CoP members had helped to produce). It then proceeded with activities to help participants adapt and use the knowledge in practice, with examples provided by speakers and experiential stories and questions from participants. The process concluded with activities to help participants further understand and contextualize the knowledge.
Most knowledge users in this case were managers and senior staff from various healthcare organizations and some of these knowledge users were involved in the collaborative planning process. One participant reflected on the importance of the planning discussions: “What I think is that people were able to walk away with a view of the difficulties we both face; difficulties faced by people who are doing the help, by people who are doing the developmental side, you know we all have challenges and there were some, a lot of similarities, but people didn’t realize oh yeah, we’re dealing with that, and we’re dealing with that, both sides [from the developmental disabilities and LTC sectors] are dealing with similarities but the approach is different, the language is different. So I think we need a common language across sectors…”
CoP2DD1 carried out the SHOWCASE activities as part of a longer process of transformative change. Two distinct sectors, developmental disabilities and LTC, were establishing connections and sharing knowledge to ease the transition of a specific patient population as it moved into LTC homes. The CoP was interested in establishing new relationships as well as in transferring explicit knowledge between specific audiences from the two sectors. In this case study, CoP leaders realized that it was important to create and disseminate how-to information to inform care routines, and it was also important to bring about a larger system and cultural change that would break down existing silos and support the health and wellbeing of the developmentally disabled who were now living with cognitive impairments and were transitioning into new and unfamiliar care settings.
CoP2D: Meeting the Needs of LTC Residents with Diabetes
CoP2D was formed to improve diabetes education for Ontario LTC staff. Before our case study research began, the CoP had facilitated an educational program called “Diabetes 101” for HCPs working with elderly diabetic patients. The CoP had developed a DVD containing educational modules relevant for LTC homes. When we worked with CoP2D, they were producing a webinar series consisting of ten modules based on the DVD. This webinar series was the focus of our case study.
The CoP formed a partnership with the fourteen Diabetes Regional Coordination Centres of Ontario (DRCCs) whose mandate was to provide direct support to LTC homes. The DRCCs agreed to co-host the series and distribute the DVD. This partnership allowed the CoP to expand beyond their original base in Northern Ontario to create a larger provincial network of practitioners interested in implementing improvements.
The CoP leader acted as the primary leader of this initiative. While other core team members played important roles such as finding webinar speakers, compiling reading lists, managing the email invitations and registration for webinars, and designing flyers and templates, the CoP leader was seen as the initiative’s driving force. His commitment was recognized by members during all of the interviews conducted by the research team, as shown in the following statement: “So these sessions were a support and they could not have happened without [leader’s name] and his leadership. I wouldn’t per se say it was the community of practice that made the difference. It was [leader’s name] himself.” In addition to the primary leader, the initiative was carried out by a core team with six members, along with a KB and information specialist.
The CoP2D initiative used tacit and explicit knowledge. Expert speakers were recruited who were respected physicians working with the DRCCs. The speakers used a combination of explicit knowledge derived from clinical practice guidelines and also their own practice-based tacit knowledge. One speaker explained this use of explicit and tacit knowledge: “I guess it would be a combination [of explicit and tacit knowledge], I think in general we are talking about [transmission] of clinical trials into practical use…” The importance of both tacit and explicit knowledge was emphasized during the webinars. For example, one topic of discussion was the need to understand when strict adherence to guidelines was ill-advised. One participant explained: “We have seen some variation between the specific guidelines or the specific recommendations from the different presenters when it comes to how to set those [blood glucose] targets. What is coming across as the consistent theme is the need to individualize and not to group everyone together in one lump.”
Indeed, our data shows that balancing recommendations from explicit knowledge sources with a need to use clinical expertise to individualize treatment is characteristic of this initiative. This need to individualize treatment also suggests that some participants were concerned with patient-centered approaches to the care of elderly diabetic LTC residents. One core team member commented: “… I mean guidelines are guidelines, they are not written in stone and you don’t have to follow them. They are just there to guide you. And I think that’s the message we need to get out, …that they are only there to guide you and that you don’t have to aim for those numbers, especially if someone is a certain age, depending on their mortality rate and other things going on… and that we can’t paint [with] one brush for all people.”
Participants also recognized the importance of explicit knowledge, including knowledge gleaned from the clinical guidelines on the DVD and reading lists generated by the SHRTN information specialist. One CoP member explained the role played by the information specialist in creating these lists: “… our information specialist has been working with us for each of these events to make sure they [speakers] generate a reading list that meets the needs of this particular topic that include any key or seminal resources that presenters will be referencing in their presentations and that’s happening in each of the events. …”
The CoP’s primary KTA vehicle was the webinar series. Each webinar was hosted by one of the DRCCs and covered the material contained on the DVD, and also included a participative discussion of the topic. The webinars were offered via web-based technology that allowed participants to hear the presenter and view slides and video clips.
This CoP also held regular planning meetings (attended by the CoP leader, the KB, and about six members). These meetings were structured and concluded with the assignment of action items. The planning process was seen as organized and efficient.
Despite this efficiency, an unexpected event disrupted the CoP’s initiative. Without warning, mid-way through the year the provincial health ministry announced that the DRCCs were to be integrated into the LHINs. DRCCs would no longer support activities in LTC homes and would instead focus on policy making. The DRCCs were thus forced to abandon their partnership with the CoP. This triggered a series of meetings between the CoP core team and DRCC members to consider ways of continuing the webinar series. After several weeks of uncertainty, the CoP leader secured additional funding that allowed the CoP to complete the initiative without the support of the DRCCs.
The target audience of the DVD and webinar series included HCPs working in LTC settings. When it became apparent that many participants in the webinars were senior decision makers, the initiative leaders saw this as an opportunity to strengthen the adoption of the diabetes treatments described in the webinars. As the CoP leader commented: “Many of the people who are participating are decision makers … [who] have the influence or the ability to direct back these changes and decide what’s included in education, for example, in their practice settings. We’re hoping that those who are participating will go beyond this, each one of these individual modules, and it will influence the way that they direct practice in their care settings.”
The CoP thus adapted the webinar series to the needs of decision makers and educators. They began to include presentation materials, reading lists, and contact information so decision makers and educators would be able to facilitate sessions within their own professional settings.
Although the CoP2D initiative intended to fill a specific learning and skill gap in frontline diabetes care, the CoP core team came to appreciate that they were having an impact that went beyond their original intentions. One case study participant told us, “I think what’s going to come out of it is increased awareness and knowledge. So … the information isn’t new and it already existed and it was there, however some people don’t know how to tap into information and update their facilities and then at a provincial or ministry level there are no specific requirements for diabetes care in long term care homes. So … we’re at the infancy stage, at the beginning of just a general awareness, getting people talking and then I don’t know how it’s going to evolve. …I think we definitely got the ball rolling.” The CoP thus addressed a learning gap in LTC homes, and also acted opportunistically when it discovered that there was a broader audience for the knowledge being mobilized. CoP leaders realized that improved diabetes care in LTC homes would require training in specific competencies and also required interventions targeting organizational and system leaders.
CoP3CC: Supporting HCPs Working with Elderly Patients with Complex Care Needs
The CoP3CC case involved an ongoing provincial initiative whose goal was to support health care providers working with patients living with dementia who exhibited responsive behaviors. As the province moved forward with this work, the teams providing specific support services in the LHINs realized that they needed special processes to handle situations where the persons with responsive behaviors had complex care needs that could not be resolved by any single existing group or service provider.
This CoP was made up of members of a provincial management team consisting of LHIN representatives, program chairs, and regional coordinators, whose role was to coordinate the development, implementation, and operation of services for people living with dementia who exhibited responsive behaviors. Four members of this management team became aware of the unique needs of patients with complex care needs, and they discovered that special processes were being created in some LHINs to handle these situations. These four individuals looked at these processes and identified commonalities, and then took on the mandate to develop a framework for the development of common provincial processes to support people exhibiting responsive behaviors who had complex care needs.
The knowledge used by the CoP came from a variety of tacit and explicit sources. CoP members shared experiences gathered from frontline providers. They also made use of documents created by health organizations (such as the Incident Analysis Framework that was available through the Canadian Patient Safety Institute), and some relevant scientific articles. Members relied on explicit knowledge to create the framework, and they used tacit knowledge as they discussed and considered the usefulness of the draft framework. As a draft of the framework took shape, the core team tested it by considering whether it could provide help in relation to specific case examples shared by frontline care teams in the LHINs. The core group met monthly to share and discuss the local processes for managing difficult cases. These meetings were the only activities that were evident to our research team.
This case study did not reach a point where a specific KTA process was used to move useful knowledge into practice. Instead, CoP members shared tacit and explicit knowledge with each other during monthly meetings. The intention was to develop a common framework that could be shared across the province, but we did not hear CoP members discuss what methods they would use to share the framework once it had been finalized and approved. Moreover, although the meetings allowed for information exchange among CoP members, we saw no indication that the CoP had succeeded in completing a framework to support regional processes for complex care resolution.
While our team collected data, there was no involvement of front-line providers in the work of this CoP. Some participants told us that once the framework was fully developed, they planned to ask front-line providers to test the framework in the LHINs.
In essence, this case study involved a sporadic process intended to produce and implement a knowledge product. Knowledge users were excluded from the process during the time of our observations. A few CoP members felt strongly about the initiative and seemed to genuinely want to produce a framework that would work in the province’s health regions. However, they were not supported by a KB or information specialist (we were not told specifically why these roles were not filled, though one participant implied that it was because the CoP was “undergoing some restructuring and so forth” and that it “has stagnated a bit”), and the management group that had mandated this work offered little support or guidance. Despite these barriers, the core group continued to work on the framework throughout the period when we collected data, though little progress was evident to our team.
CoP3DD2: Promoting Further Cooperation Across Health Sectors
The CoP3DD2 case study involved the same CoP that we worked with in the CoP2DD1 case, described above. This CoP was working to create an expanded network bringing together the developmental disabilities and LTC sectors, particularly in relation to elderly people with both a developmental disability and dementia. The CoP had conducted a needs assessment that revealed a “pressure point” in both sectors in terms of supporting people with dementia. In this phase 3 case study, CoP3DD2 again used a SHOWCASE approach to disseminate best practice guidelines and an early dementia detection screening tool for people with developmental disabilities.
The CoP’s SHOWCASE process began with a webinar that highlighted the guidelines and screening tool. This was followed by an online discussion forum that continued for 4 weeks. One participant described the online forum: “… during the next 3–4 weeks, we have a discussion board and we sign everybody up for the discussion board and then between the … content experts, the presenters, as well as the working group, we start posting the questions on the discussion board and try to engage the participants during this period of time, challenge them to think back to the presentation and ask specific questions about practice. …we’ll go right from pre-diagnosis all the way through asking specific questions to try to get people to kind of see how the guidelines can be practically applied. And the same thing with the early detection screening tool, we’ll do the same thing, we’ll keep saying to people you know, have you tried it, can you try it and let me know what you think, go try it, come back, tell us what you think.” The third part of the SHOWCASE process was a follow-up webinar on issues raised during the online discussion to further support the translation of knowledge into practice.
This SHOWCASE process targeted frontline staff and supervisors (rather than the senior leaders who had participated during the previous year). It included a strong focus on implementation by encouraging participants to discuss the use of the guidelines and screening tool in practice. Overall, the aim was to ensure that frontline staff received the information directly and benefited from support in using the guideline and screening tool. As one participant remarked, “…we really want to get this into the organization so not just people at the top, we want to make sure that we’re trying to get it in the middle of organizations … so I think we will talk a lot about that because we need to … find the people that are going to … probably get the most out of this and that’ll be a little challenging.” Whereas some of the other case studies saw CoP members targeting frontline caregivers and then realizing they also needed to reach senior decision makers, this CoP began by targeting senior leaders and discovered that they also needed to reach people working on the frontlines.
The case study saw ongoing interaction between explicit and tacit knowledge. The SHOWCASE process was based on explicit knowledge (i.e., especially the clinical guideline and screening tool). However, tacit knowledge was used to contextualize the research-based tools and facilitate the KTA process. For example, both webinar presenters had cross-sectoral experience working on issues of aging and intellectual and developmental disabilities. Those who helped to contextualize the research evidence and support its uptake into practice included the members of the CoP planning group, webinar presenters and facilitators, and the participants who shared experiences and asked questions.
Some participants indicated that this initiative ensured that relevant knowledge is now in circulation: “I sat at my computer and listened and watched the slides and then I took all of the links and shared them with other staff members, and then took the most recent information and put it in a PowerPoint presentation that I gave at a local community living day program and I’m taking it out to one of the rural community living day programs and was able to refer them to all of the latest material and links, check lists that they can use, all of that material on, you know, deciding about assessing people, some of the new books that are out, that sort of thing.” The data provided by participants suggests that the CoP realized that better integration of the developmental disabilities and LTC sectors would be a lengthy process requiring a variety of interventions targeting frontline workers as well as managers and senior leaders.
CoP3W: Meeting Wound-Related Needs of Elderly Patients Transitioning Between Care Contexts
This CoP was created to advance knowledge on pressure ulcer prevention and promote best practice recommendations. Initially the CoP operated under the direction of a steering committee that provided support and direction while a core working group was formed. CoP members included formal and informal caregivers from the acute care, complex care, homecare, and LTC sectors, along with researchers, policy makers, educators, and librarians.
CoP3W completed a needs assessment that included a literature review carried out by a SHRTN information specialist. This assessment revealed that the topic of pressure ulcer prevention was both highly relevant and of equal priority for all settings (home, hospital, LTC, rehabilitation, and complex continuing care). They then met with provincial and national experts in wound care (including in-person meetings with 30 participants and web-based meetings with participants from 102 sites), and ultimately concluded that knowledge gaps in pressure ulcer prevention was a critical area. Relying on information provided by CoP members and their personal work experience, the CoP leads came up with the idea of developing a wound passport tool that would contain personal wound care information that patients could take with them across the continuum of care. The tool would help to ensure that HCPs were aware of the wound care that a patient had been receiving and that was still needed. After developing the passport tool, efforts focused on preparing for a webinar to disseminate the passport. CoP leaders prepared and delivered a webinar (with 42 participants), made a presentation at a national wound care conference, and then held a follow-up webinar (55 participants).
Although the leaders of this initiative created and launched a passport tool that seemed relevant and useful to webinar participants, they experienced challenges. The CoP co-leads transitioned out of their positions with organizations that had supported their involvement with the CoP, which meant that they were no longer able to use work time for the CoP initiative. Concluding interviews with the co-leads revealed that when the initiative had formally come to an end, there was still a significant amount of work to do to implement the passport tool into health care settings. One co-lead commented, “I don’t want to see this be another thing that just…‘it was a really great idea’ and then it’s done and disappears. That would be my one fear is that that’s what’s going to happen … There’s a big difference between having people read an article and having people actually implement … The action side of it is not always as quick as you’d like. The uptake, you know, it takes… can take years…”
Nonetheless, the two co-leads and the KB viewed their initiative as a success. They created a tool that would contribute to the reduction of pressure ulcers and hosted several KTA events to start moving the tool into practice. The passport was created with information obtained from the co-leads’ clinical experience (and associated anecdotal knowledge from patients and families), evidence in the literature, and frontline workers’ professional experiences and knowledge of best practices. The knowledge underlying the development of the KTA initiative was thus a combination of tacit knowledge derived from practitioner and patient experiences, and research-based knowledge.
This initiative encountered several barriers. The co-leads noted that there was a breakdown of communication in the early phases of the initiative, which made it difficult to reach the target audience. One co-lead explained that “it’s not that other people haven’t voiced an interest. I do think that part of it was there was just a bit of a communication breakdown.” A second issue was limited awareness about the existence of the CoP. One co-lead said that the CoP “seemed like kind of a closed operation.” In her concluding interview, she noted that better communication in raising the awareness of this CoP within the wound care field may have allowed for more connections and involvement. A third communication issue related to interactions within the CoP core group, which at times was characterized by poor communication. Interviews revealed misunderstandings about the number of webinars to be held, about the CoP’s future activities, and about the status of the two co-leads. Our data indicate that tensions between the KB and co-leads may have limited the effectiveness of the leadership group.
Despite the challenges, the co-leads told us that they had attained their objective of developing and disseminating a tool that could improve wound care for seniors, that was feasible to use, and that could contribute to the reduction of pressure ulcers. Nonetheless, the CoP co-leads acknowledged that further effort would be needed to make progress on the treatment of pressure ulcers in elderly patients who transition between care facilities.
Concluding Comments on the Narrative Descriptions
These narrative descriptions were the product of our first analytical step, and here we will make a few preliminary comments about patterns that are beginning to be evident.
First, all of these CoPs rely on both explicit and tacit knowledge as they design and implement their KTA processes. Quite often the CoP aims to encourage the adoption of knowledge that takes the form of a document (such as a guideline or a set of recommendations), and in order to move this explicit knowledge source into practice the CoP calls upon the tacit knowledge of expert practitioners to show how the knowledge might be applied in specific frontline situations. The CoP initiatives also offer examples of CoP leaders accessing the tacit knowledge of frontline practitioners in order to better understand existing constraints and needs, and to invite practitioners to contribute to a collaborative problem-solving process.
Second, the narrative descriptions indicate the importance of collaborative planning and other discursive processes for many of these CoP initiatives. Most of the CoPs form a planning group that allows CoP leaders and frontline knowledge users to collaborate on understanding needs and designing solutions. In some cases, such as CoP1R and CoP2DD1, CoP leaders believed that their objectives would only be met if people from different regions and sectors were able to hold open-ended discussions to form relationships and share concerns and ideas.
Third, several of these CoP initiatives begin with a training-based intervention intended to push knowledge to the frontlines, usually through the design and delivery of webinar training. However, as CoP members worked to bring about change, and as they learned more about the frontline contexts that they were seeking to engage, many realized that their desired change required a multifaceted approach to reach different system levels and different audiences (frontline HCPs, LTC managers and leaders, and provincial policy makers). In other words, as CoP leaders encountered the complexity of the health system that surrounds and contains the frontline practices they were trying to help, they realized that more complex approaches were needed. What started as a simple, technical challenge (providing specific information to specific people) became more complex—requiring changes to the mindsets of people at different system levels, and new structural elements such as ministry sanctioned priorities.
Fourth, the fact that CoP leaders developed this more sophisticated understanding of the challenges that they needed to overcome suggests that the initial webinar-based interventions produced new information (like the data produced by a natural experiment) that allowed CoP leaders to learn. This suggests that the social learning described by many CoP scholars and researchers was almost certainly occurring in most of these CoPs.
Finally, the involvement of knowledge users and KBs in the collaborative planning process seems to be associated with CoP initiatives that enjoyed more success (for example, CoP1R, CoP2DD1, CoP3DD2). The absence of KBs and frontline knowledge users from the collaborative planning process is associated with the two case studies (CoP2T and CoP3CC) that experienced less or little success.
We will return to these subjects later in the monograph.
Findings From Our Deductive Analysis
All of the cases we studied were attempts to bring about planned change. Some involved a precise and targeted change, such as the improvement of a specific clinical practice in LTC homes. Others sought to bring together interested people to delve broadly into common concerns and challenges and to consider possible solutions.
The findings presented here—across all nine cases—are organized in terms of our research questions which concern the CoPs’ KTA processes and the role of human agents in bringing these processes to life.
What KTA Processes are Initiated Through the CoPs?
A variety of KTA processes, arising from different conceptions of KTA and serving different objectives, were at work in these case studies. Our analysis reveals five major processes that were present in these CoPs, as shown in Table 3.
KTA Processes Initiated Through the CoPs.

Some cases emphasized the importance of creating and disseminating concrete deliverables in the form of knowledge products (such as best-practice guidelines). Others placed more emphasis on deliberative processes that allowed people to assemble and problem-solve together. Seven of the nine cases included webinars that brought together participants from across Ontario to hear from experts and engage in discussion. Five webinars included follow-on activities to support knowledge users as they implemented practice changes. The other two cases focused exclusively on processes to collaboratively identify shared issues and design improvements.
The KTA processes initiated through the CoPs usually involved a combination of collaborative planning and the delivery of information through web-based educational events. Often, these educational events presented and explained a knowledge product that had either been created or endorsed by the CoP. The idea was to inform these audiences (the make-up of which differed in the cases, and could include frontline health care practitioners such as nurses, PSWs, physicians, and other allied health workers, as well as educators, decision makers such as directors of care, and others) about the importance of the knowledge contained in the knowledge product.
To help us understand the diversity of CoP strategies, we mapped them against the intervention framework devised by Chin and Benne (1984) and later modified by Daniels and Dewine (1991). This framework offers four strategies to bring about planned change. A power-coercive strategy uses power to change a system (e.g., a government imposing a regulatory regime on LTC homes). An empirical-rational strategy presents stakeholders with evidence and reasoning to justify a change (e.g., an evidence-based treatment guideline given to primary care physicians). A normative-reeducative strategy assumes that behavior arises from workplace culture, and calls for interventions to help people alter attitudes, norms, values, competencies, and relationships (e.g., awareness raising and training to create a culture of patient-centered care). Finally, an interpretive-communicative strategy assumes that the prevailing situation in a workplace is created through ongoing patterns of communication, and that change requires interventions that interrupt these patterns (e.g., town hall meetings and deliberative processes).
The KTA “collaborative planning” process shown in Table 3 involved reasoning and appeals to science and evidence, considerations of and efforts to change culture and competence, and open-ended exploratory discussions. Collaborative planning thus mapped to the Chin and Benne (1984) categories of empirical-rational and normative-reeducative, as well as to the Daniels and Dewine (1991) interpretive-communicative category. The KTA “designing and creating a knowledge product” process was generally an effort to gather and consolidate scientific evidence, and thus maps to the Chin and Benne (1984) empirical-rational category. The KTA “Designing and implementing a KTA event” process involved webinar-based training and education, and thus maps to the Chin and Benne (1984) normative-reeducative category. The KTA “capacity building” process could involve a variety of activities and interactions that promoted new ways of thinking about existing problems and the creation of new relationships and linkages that were seen to be helpful in bringing about improvement, and could be mapped to the Chin and Benne (1984) empirical-rational and normative-reeducative categories and the Daniels and Dewine (1991) interpretive-communicative category. The KTA “informal interactions” process included emergent (i.e., unexpected and unplanned) discussions that could be exploratory and opportunistic and could yield new understandings, priorities, and relationships, and can be mapped to the Daniels and Dewine (1991) interpretive-communicative category. Chin and Benne (1984) also posited a power-coercive strategy for bringing about change, in which hierarchical leaders would impose changes upon stakeholders. Although we observed no clear power-coercive processes in these case studies, we did note that two cases—CoP2T and CoP3CC—were dominated by people in leadership roles whose work was ultimately intended to alter the behavior of frontline workers (who were not participating in the CoP discussions during our period of observation), and thus arguably these two cases align with the power-coercive strategy. Table 4 summarizes the results of mapping our nine cases against this framework.
Intervention Approaches Used in the Nine Case Studies.

In most of the case studies, the KTA processes included an educational event that presented a reasoned explanation for the proposed change along with curricular components intended to help participants to develop the skills needed to implement the change. In several cases leaders also discovered that to change practice they needed to do more than educate people. This discovery took different forms in different initiatives. In CoP1P the leaders concluded that changing the physical layout of LTC homes had to be preceded by policy changes at the provincial level. CoP1O leaders found that to change oral health practice in LTC they needed to provide both skills training and descriptive information, and that they also needed to change the underlying organizational culture of LTC. In CoP2D leaders found that disruptions at various points in the health system could negatively impact their initiative, which led them to focus as much on the resilience of their own process as on educational content. Since the CoP2DD1 and CoP3DD2 cases aimed at fostering cross-sectoral cooperation, it is not surprising that their efforts focused on relationship-building. In addition, the CoP1R case was founded on the belief that changing frontline practice required numerous interventions at different system levels. This belief is also evident in the CoP2T and CoP3CC cases. The focus on policy, culture, and system levels indicates a preference for normative-reeducative approaches to change.
Finally, our findings suggest that many of the CoPs supplemented diagnostic activities with dialogical approaches to change. The CoP1R case was based on local conversations that were intended to help people understand perspectives and discover solutions to shared problems, and the fact that the main KTA activity in both CoP2T and CoP3CC was exploratory discussions suggests a similar approach to change. Five cases (CoP1P, CoP1O, CoP2DD1, CoP3DD2, and CoP2D) emphasized creating relationships, building networks, and encouraging people to engage in planning discussions, and a sixth case (CoP3W) also exhibited this tendency at the start of the initiative. This may indicate that to varying degrees the CoP leaders came to recognize the importance of the interpretive-communicative approach to change that is becoming prominent in the field of organization development (Bushe & Marshak, 2016).
To What Extent Does KTA Involve an Interaction Between Explicit Knowledge and Tacit Knowledge?
One of our major findings is that in these CoPs KTA clearly involves an interaction between explicit and tacit knowledge. Table 5 provides a summary of the interactions that were characteristic of the nine cases.
Interaction of Explicit and Tacit Knowledge in the Nine Case Studies.

The explicit knowledge generated through science was often needed to indicate “what” should be done. The tacit knowledge created through clinical experience helped to demonstrate “how” the new activity or practice is to be carried out. One might argue that even where explicit knowledge plays a primary role, this knowledge must always be mediated by clinical experience before it can be used in practice.
This balancing act appears in all of the cases we examined. The CoP2D case nicely illustrates how this works. The explicit knowledge provided through evidence-based diabetes care guidelines was seen as important and valuable. However, we observed that how these guidelines are applied in the case of complex elderly patients with comorbidities is determined on a case-by-case basis. CoP leaders and presenters therefore adopted an approach that included case-based learning where principles are placed in the context of patients with specific characteristics and symptoms, so they could demonstrate how the seemingly standardized treatment advocated by a guideline could be individualized to make it useful and relevant for a specific patient.
The behaviors evident in most cases illustrate a group of CoP leaders who identify or assemble knowledge, often in the form of evidence-based guidelines, and then attempt to disseminate this knowledge through an educational event. This dissemination frequently presented knowledge in ways to help learners understand how the knowledge might influence their own behaviors. In CoP1O, this took the form of video clips demonstrating how to perform tasks. In CoP1R, it took the form of “local conversations” in which basic principles were fleshed out through discussions of specific regional care programs and participant experiences of patient interactions.
Many of the CoPs tried to find ways to individualize or personalize the knowledge presented. However, they did not always anticipate factors that exert influence on behavior in practice (for example, the priorities in place in a LTC home, the quality indicators used to measure performance, or the policies issued by the provincial ministry).
The interactive processes used by the CoPs (for example, the collaborative planning processes and network building that most CoPs engaged in, as evident in our descriptions of the case studies) supplemented the impact of educational events. During these open-ended interactions problems were framed and analyzed, solutions discussed, and barriers identified. Relationships were formed, and networks of people who could provide advice and support were established and extended.
A simple process of social learning (that is, learning through interaction and experience) occurs when a group of people consider the explicit knowledge that is produced through science and scholarship in the light of tacit knowledge gained through the experiences of people acting in concrete situations. Although most of these CoPs were formed with the intention of transferring knowledge packages to frontline clinicians and care providers, they also created social learning environments in which participants worked together on a change initiative by assembling relevant explicit knowledge and then integrating this knowledge with their own experiential knowledge. This created two streams of activity that had the potential to bring about beneficial change. The first is the design and delivery of a KTA event, often in the form of a webinar combined with follow-up activities. The second is a less formal process consisting of the creation of relationships and networks that lead to ongoing interactions around shared interests and concerns, which may also produce behavior change in ways that cannot be anticipated.
What Roles are Evident Among Those Who Participate in These Processes?
All of the cases demonstrate some form of leadership process, which sometimes involved leadership shared amongst members of a group, and sometimes involved the leadership of one or two key individuals. Table 6 provides a brief summary of the leadership roles seen in the nine case studies.
Leadership Roles in the Nine Case Studies.

We originally wanted to see how different roles contributed to an effective CoP process. We did indeed find what we were looking for (discussed below), and also found that sometimes a key individual stood out as making a unique contribution. In eight cases, either one or two people made the most significant contributions to the work. In CoP2D, for example, several participants stated that the CoP lead during the initiative was instrumental to its success.
This finding surprised us because we conceptualized these KTA initiatives as social processes involving a changing group of actors organized in collegial, non-hierarchical ways. What we discovered was that in most CoPs leadership was provided by one or two people who were fully committed to the CoP’s goals and whose orientation to action helped to ensure success.
A specific set of roles, played by a variety of participants, emerged from the nine cases. The roles of leader, knowledge broker, champion, thought leader, information specialist, technology facilitator, and boundary spanner (network builder) were important in most of these cases.
Leadership took various forms and leaders exhibited a variety of behaviors. Four of the cases had one main leader, four cases received leadership from a two-person team, and one case had a shared leadership process with several people contributing leadership at different times. Leaders encouraged people to contribute to the initiatives: they organized and coordinated work, they drew upon existing relationships and created new relationships, they helped to create and articulate the purpose of the work, and they often demonstrated their personal commitment to the work of the CoP. Many leaders also attempted to create a process of shared leadership and decision making, encouraging participants to take responsibility for a particular task, and facilitating decision processes in which many people participated.
In seven cases the leadership process was effective and produced useful results. In one case (CoP3CC) instability and a small team resulted in slow progress, and in another case (CoP3W) acrimony developed within the leadership group. Most cases saw the leadership process begin with an effort to build consensus around a topic, and then continue with the design of a KTA process. In most cases there were opportunities for many people to contribute to the work.
The sponsoring network employed a team of KBs who provided support to the CoPs. In most cases CoP members reported that the KB made important contributions. They helped the CoPs to find an initial focus and to set concrete goals. They also helped the CoP leaders to remain organized, manage webinar technology, maintain membership lists, recruit participants, schedule meetings, prepare and distribute minutes, and access and appraise the knowledge needed to carry out the CoP’s plans. KBs also publicized the work of the CoPs, and connected CoPs to other networks and groups. Perhaps it is noteworthy that two cases struggled more than others: in one (CoP3W), the KB went on sick leave for a period of time, and there were miscommunications between the KB and CoP leads; and in the other (CoP3CC) there was no KB providing support.
Some initiatives benefited from the presence of champions or opinion leaders who were well connected and willing to publicize the benefits of participating in CoP activities. At times these champions provided a form of visionary leadership, helping the group to see outcomes that they might bring about, and encouraging people to contribute to these outcomes.
Other initiatives highlighted the role of thought leader, often an expert who shared his/her expertise by making a webinar presentation. The qualities and behaviors of these expert presenters—for example, their willingness to collaborate with others to identify the appropriate content and the best mode of delivery—had much to do with the success of the initiatives.
Several CoPs used the services of information specialists who, like the KBs, were employed by the sponsoring network. These individuals would locate information needed to achieve CoP goals, and prepared reading lists to accompany the webinars. Some CoP participants took on the role of technology facilitator. Given that the initiatives often used webinar technology with which some participants were not familiar, it was often helpful to have someone available who could coach people in how to connect to the webinars and use the technology’s features. Finally, we noticed that some CoP leaders and members acted as boundary spanners, linking the CoP to other groups and networks in ways that allowed the CoP to locate resources and publicize CoP products and events.
How Does the Active Involvement of Knowledge Users in the KTA Process Influence Knowledge Utilization?
We posed this question because we anticipated that the active involvement of knowledge users in the KTA process—which we defined as active involvement in efforts to implement and encourage the uptake of an innovation—would positively affect the uptake and use of new knowledge. We also wanted to see if the cases would illustrate how knowledge users could be integrated into a KTA initiative.
Knowledge users were involved at moderate to high levels in seven of the nine cases, as indicated in Table 7. Often this involvement included participation in planning and implementing the KTA processes. Involvement also took the form of interaction with experts and other knowledge users at webinar presentations. In two cases (CoP2T and CoP3CC) frontline knowledge users were not directly involved in activities. This may be due to the unique features of these two cases, in that both involved the preliminary efforts by a group of health leaders from across the province to problem-solve specific issues related to dementia care. In one of these cases (CoP2T), toward the end of the observation period participants were talking about inviting frontline practitioners to future meetings.
Level, Nature, and Impact of Knowledge User Involvement in the Nine Case Studies.

Most participants in the cases believed that the active involvement of knowledge users in the KTA process exerted a positive influence on knowledge utilization, but we do not have empirical data to confirm the accuracy of this belief. Nonetheless, our research participants were directly involved in concrete efforts to change and improve frontline practice, and their experiences produced the belief that involving frontline knowledge users can support KTA efforts.
Participants in the cases often suggested that active involvement of knowledge users during the preliminary phases of a CoP’s work would result in the selection of an issue that is relevant to the frontlines, thus encouraging people to participate in the KTA processes. Participants also indicated that active involvement during the dissemination of relevant knowledge should create opportunities for people to consider how the knowledge could be used in their practices. Questions and discussions could promote the tailoring of knowledge to specific workplace realities, making it more likely that knowledge would be adopted and used. We have anecdotal data indicating that this occurred in several cases. For example, leaders of the CoP1R case reported that their involvement of regional leaders and practitioners in their initiative was critical to its success, while respondents from the CoP1P case said that engagement of frontline workers was crucial to ensuring the success and practicality of the initiative, and attributed this to the practical knowledge that these people had of the care environments that were the particular concern of this initiative. Findings from the CoP2D case indicate that involving knowledge users helped to establish credibility, raise awareness, change attitudes, mobilize demand, and create a “trickle” effect as word of the initiative spread throughout the province. The CoP2DD1 case found that involving knowledge users made the knowledge under discussion more meaningful for the contexts in which the knowledge was to be used.
We considered the ways in which knowledge users were involved in the cases, and rated this involvement as low, medium or high (this is shown in the third row of Table 7). “Low involvement” included cases with no involvement of knowledge users in the initiative, or involvement only in the form of attending and participating in a webinar. “Medium involvement” included cases where some knowledge users participated on the initiative’s planning team, where a needs assessment or other form of consultation of knowledge users occurred, and where knowledge users participated in the webinar and other KTA events. “High involvement” indicates that many knowledge users participated in and influenced the planning, design, and implementation of the KTA initiative, and in some cases sponsored (by providing resources) the implementation. This analysis also involved rating the level of results produced by the case (shown in the fifth row of Table 7). An assessment of “limited” results indicates a KTA initiative in which some (but not all) objectives were met and deliverables were produced. An assessment of “reasonable but limited” results indicates that the KTA initiative produced all of its intended deliverables and held all activities, and a few outreach or follow-on activities occurred to assist with the uptake of the knowledge by frontline practices. An assessment of “good” results indicates that all objectives and deliverables were achieved, and the data provides evidence that some behavior change took place. An assessment of “excellent” results indicates that all objectives were achieved and that there is evidence that behavior change is occurring.
As shown in Table 7, knowledge users involved at a high level correspond with “excellent” and “reasonable but limited” results; knowledge users involved at a medium level correspond with “reasonable but limited” and “good” results; and knowledge users involved at a low level correspond with “limited” and “reasonable but limited” results.
What Factors Support or Hinder Effective Involvement in KTA Processes?
If the involvement of knowledge users in these initiatives facilitated the uptake and use of innovations in frontline practice, it would be helpful to know what supported and undermined this involvement. When all cases were complete, we looked at the factors that supported or hindered involvement, and identified those that were evident in at least three cases. These findings are presented in Tables 8 and 9.
Factors Present in Three or More Cases that Supported or Hindered Knowledge User Involvement.

Prevalence of Factors Supporting or Hindering of Knowledge User Involvement.

Four factors were found to support effective involvement in KTA processes: leadership and commitment (evident in seven cases); interaction and discussion (seven cases); communication technology (three cases); and SHRTN resources (three cases).
Our data showed that when effective leaders were involved in an initiative, and when those leaders and others were committed to the goals of the CoP, work went smoothly and challenges were overcome. Many participants said that meeting with others and discussing concerns and ideas was important to the success of a KTA initiative. These interactive processes allowed people to receive feedback about ideas and past efforts, provided access to new resources that helped the CoP achieve its goals, and allowed participants to learn together as they tackled problems in complex social environments. We also discovered that the use of technologies such as teleconferencing and webinar technology contributed to the success of several initiatives (though they also gave rise to challenges, as indicated below). CoPs designed and delivered province-wide initiatives without incurring enormous travel costs. Finally, several participants told us that SHRTN provided them with access to resources that were essential to the success of their initiatives. Many mentioned the important role played by their SHRTN KB.
Five factors were found to hinder effective involvement in KTA processes: heavy workloads and competing priorities (evident in five cases); absence of supporting structures (four cases); funding uncertainty (three cases); technology difficulties (three cases); and marketing challenges (three cases).
Many participants told us that the heavy workloads characteristic of frontline health care delivery, along with the competing priorities that practitioners often face (with different priorities being introduced by provincial policy makers, regional health authorities, organizational leaders, and professional licensing bodies), made it difficult for them to become involved in a health innovation that was not mandated by an employer or by a regulatory or licensing group. This concern came up repeatedly, especially in relation to the workload of PSWs and practical nurses working in LTC homes. When care routines are heavily stressed, it is difficult to find the time to participate in voluntary change initiatives. Similarly, we were told that without supporting structures such as policies and mandates, it is unlikely that the knowledge users participating in these KTA initiatives would be able to translate the knowledge into action. To change practice on the floor of an LTC home, it may be necessary to create interventions targeting individual caregivers, teams of caregivers, organizational decision makers, and health system policy makers.
These challenges were augmented by funding uncertainties encountered by the CoPs in the second and third-year case studies. CoP leaders knew that the future of the SHRTN network was being reviewed by the province, and this made it difficult to recruit people to join the CoPs or commit to a lengthy change initiative that might be cancelled before reaching completion. This challenge came close to derailing more than one of these KTA initiatives.
Some CoPs also encountered more specific difficulties that may have been due largely to missing skills or insufficient time to carry out activities. Most initiatives relied heavily on webinar technology, and it was sometimes difficult for participants to master the use of the technology. Some CoPs also encountered challenges as they attempted to market their KTA initiatives, in part because the task of creating a distribution list of interested stakeholders often took more effort than expected.
Findings From Our Inductive Analysis
As described in the methods section of this monograph, our inductive analysis involved an open-ended coding and theming exercise carried out in relation to the qualitative data gathered in each case study. This data consisted largely of interview transcripts and observational field notes, much of which concerned what people were thinking and doing as they created, designed, and implemented their initiatives to move new knowledge into action in specific health practices. Our analysis revealed patterns related to the mindsets of CoP participants, the behaviors that were enabled by these mindsets, and the structuring that participants created in order to bring stability to their efforts.
Our inductive coding analysis revealed thirty-three themes present in the nine case studies. Table 10 presents the eleven themes that are present in at least three of the nine cases. Table 11 presents this information in a summary form, allowing readers to visually take in the prevalence of themes across the cases.
Cross-Case Themes Present in Three or More Cases.

Cross-Case Themes Present in Three or More Cases.

Supplemental Additional File 1 provides a more detailed version of Table 10, relating the cross-case themes to the themes derived from the nine individual case studies. Supplemental Additional File 2 offers further detail by presenting 68 representative quotations to illustrate the cross-case themes. We also provide representative quotations in the following paragraphs that briefly explicate the major cross-case themes.
Operating within a Complex System
Our cross-case analysis indicates that the overall context for these CoPs and their initiatives is a complex system that can support or undermine the CoP. In launching their KTA initiatives within this system, these CoPs encountered both opportunities and challenges. Some CoPs realized that to effect frontline change, they had to target interventions at individuals, practices, organizations, and the overall provincial health system. At the same time, unexpected actions originating at various system levels sometimes disrupted the intentions and actions of the CoPs.
The complexity of the system was evident to an interviewee from the CoP1R initiative, who commented “…we also know that there are cultural differences across the province and how do you work with those and then how do you work with the different kind of way that people have actually developed with working their partnerships out?” A participant from CoP2DD1 also highlighted the complexity of the system: “I think there’s a great deal of interest but there isn’t as much leadership being shown at all levels, I’m talking about front line staff leadership as well as administrative and leadership, as well as policy leadership in long term care, there really isn’t as much, so that’s one of the, I think, end goals that’s probably not spoken about openly, no one wants to be patronizing towards long term care but I think one of the end goals is secretly to improve the status and gain some champions inside the long term care sector where the population under discussion also has developmental disabilities.”
Diverse and Complex KTA Events
The analysis also showed that many of these CoPs designed and implemented a wide variety of KTA events in order to achieve their own multiple purposes and to ensure that they would be providing information that was appropriate for their target audiences. CoPs often began their work by designing very specific and limited KTA events, but as CoP members worked together they began to realize that more complex approaches were needed. For example, many CoPs began by selecting a simple approach such as a webinar. However, as they gained a better understanding of the actions needed to produce the desired changes, they introduced more complexity into their plans. Over time most CoPs began to devise approaches that could influence change in multiple system contexts.
Speaking of the effects produced by their local conversations, a CoP1R participant mused, “…there’s room, I think, to still continue to build and nurture those skills in the local context, which I think we maybe just opened the door on that but haven’t really got all the way through.” Similarly, a participant from CoP2DD1 noticed the need to “…reach to new groups and networks—we have noticed that our participants in events are far more varied (different sectors, wide range of caregivers, access to researchers) than prior to being connected to SHRTN.” An interviewee in the CoP3CC case also noted the need to tailor knowledge and approaches to local contexts: “So the goal is to create a framework and actual tools that can be used by each LHIN…. So it’s really helpful to create documentation and a structure to then be able to pull out information that’s pertinent to the situation.”
The Opportunities and Challenges of Collaboration
Our findings show that most CoPs understood that achieving KTA through collaboration and interaction creates both opportunities and challenges. To collaborate was to seek common ground, create partnerships, and build networks of caregivers, policy makers, educators, and researchers who were committed to shared objectives. However, collaboration takes time and requires high levels of interpersonal skill, and stretches resources available to the CoPs.
A CoP1R participant observed that “…one of the greatest challenges and needs is to bring people together …” Speaking of the challenges inherent in having mobile teams of people with expertise in responsive behaviors work across and within different systems, a participant from CoP2T commented: “they are kind of out of very different organizations, some of them are out of long-term care homes, some of them are out of hospitals… some are attached to community support service within a longer term care home.” A participant from the CoP2DD1 case talked about strategies to encourage collaboration: “The real purpose of bringing people face-to-face is to build a relationship between sectors, so a huge chunk of the day was with the facilitator and walking through a series of questions and processes, and exercises to actually get them talking to each other.”
Multiple and Varied Strategies
We also found that most CoPs used multiple strategies to access a wide variety of knowledge sources and to incorporate a variety of dissemination techniques in their activities. Some CoPs, for example, created a knowledge product, and then searched for different ways to integrate the product into practice. Others drew on credible and relevant scientific and practice-based knowledge that could be adapted to meet local needs. In part, the diversity of knowledge sources and dissemination strategies reflects the realization that knowledge must be tailored to make it useful in local practices.
Referring to their repackaging of existing knowledge about diabetes care, a participant from CoP2D commented, “We haven’t created new knowledge … What we have done is we have taken existing information and put it into a format that allows people to make it a little more applicable to them.” A CoP3DD2 participant said, “… I’d say that some of the knowledge transferred was quite clinical in nature, there was a lot of question about medication, various treatments, so there was sort of the, some of those specific technical pieces. I think the other type of knowledge transfer was more about awareness and more kind of a process.” A CoP3W participant speculated about additional KTA activities that were needed: “Now something that we realized … is if people want to bring it into an organization, it needs to be brought to a higher level, right? To be approved and to go through the proper processes. … the other piece of work that we still need to do actually is just do a very high level, 2-min clip overview of what the tool’s about … and we’ll put it on YouTube and that way people can use it to bring to their managers …”
CoPs as Catalysts for Change
Our findings show that most of the participating CoPs acted as catalysts for action and change. In other words, the CoPs did not confine themselves to designing and implementing a project to push knowledge at target audiences. Most also saw themselves as providing a supportive social context capable of generating and facilitating a variety of actions directed toward change and improvement. Many CoP leaders recognize that KTA cannot be reduced to “a thing” such as a knowledge product. KTA involves action that promotes uptake and follow-up. Some CoPs acted as knowledge mobilization platforms, and created networks empowered to influence the delivery of care in their regions.
A CoP1R participant told us, “Within the context of the … community of practice, because they have inroads to all of these regions and all these local areas and these local champions, they will be … facilitating a more direct local discussion, multiple local discussions I should say, to help people take the information that they have got globally, or provincially, and then do something with it … uniquely in their own day-to-day practice.” A CoP2T participant added, “You know, initially we were going to have the team running around like a bunch of SWAT people saving the world and being the behavioral stamp out people. And it became clear that we needed to use in our process and through the exchange, that yes, we developed the why and the what, but the how was going to be driven by the long-term care homes. So with the front line workers and others, they identified that they—what they were more interested in was help with transitions or prevention or helping them with the observations that could help with a better way to support people with responsive behaviors. So our team has shifted totally in what they do day-to-day.”
Benefits and Challenges of Fluid Membership
We also found that several CoPs were characterized by open and fluid membership processes that promoted inclusiveness, diversity, resilience, and renewal, and also at times brought confusion and instability. Some CoPs saw leaders and members come and go, and this brought both benefits and challenges. New people, with new assets, relationships, and expertise, were available at different points in time, and this created a dynamic network of leaders and knowledge users. However, fluidity was also evident when important individuals and groups dropped out of CoP activities due to changes in mandates or jobs.
A CoP2D participant commented, “As I mentioned, leadership changed. Many of the key players and contacts changed. Several members of our …community of practice steering group, or our core group …had to step back given that they had lost those roles. So it was a big impact.” Another referred to this volatility as “quite an adventure” and as being “like a hurricane.” A participant from CoP2T referred more to the difficulties that can be produced by changing membership: “One thing that is difficult is people do change roles quite a bit right? So our core team is always evolving. So sometimes we get new people that are coming on or sometimes you know, people that are no longer in their role and so forth. So I think umm, you know, it’s always… and I think that’s with anything really, I mean… I think it’s always umm … it can be a challenge…”
Technology, Resources, and Planning
Some CoPs also found that their use of technology and other resources, and their planning processes, served to support stakeholder engagement and the movement of useful knowledge into action in frontline contexts. This cross-case theme shows that communication technology, a robust planning process, and access to sufficient resources were essential to the success of some initiatives. CoPs relied on careful planning, easy-to-use teleconferencing and webinar technology, and efficient use of time and resources. Planning processes that involved virtual meetings and a thorough discussion of issues allowed some CoPs to broaden their networks and assure that KTA events were well prepared and organized.
A CoP2D participant explained how they interacted with subject matter experts who were to make webinar presentations: “…we show them … what we will be doing, we’re going to control these functions on your behalf as the facilitator and that’s part of what we’re bringing to the table as a partner … we take care of all the technology…” A CoP2DD1 participant expressed appreciation for the resources provided by SHRTN: “The access to a knowledge broker and information specialist is a unique resource, which we highly value. Being connected with others is also key to our success.” A CoP2T participant said that technology was especially helpful: “There is real opportunity to bring people together to learn together so I think that’s really important about a collaborative, is that you open the doors for people to learn and we have such technology today that we can do that so easily.”
Aligning with Local Needs
We found many examples across the nine cases of CoPs taking pains to tailor their initiatives to align with local frontline needs. This could involve developing a KTA process that empowered participants with the motivations and skills to make changes to frontline practices, or a multi-faceted knowledge development process whose variety stemmed from the need to tailor KTA products and events to the situations faced by frontline workers.
A CoP1R participant said, “I think it will be very interesting to see this knowledge come to life at the local level and see how the work of this community of practice can influence change that’s very contextualized.” A CoP3DD2 participant said, “…we’re looking at different levels in the agencies … and targeting and making sure that the support is there for front line staff, but also now front line staff have the information directly.” A CoP1P participant also emphasized the importance of engaging with people on the frontlines: “We’ve done lots of presentations to the individual [LTC] homes, or the administrator, I mean even to Family Councils and things like that too, and to help understand it, so they can understand the changes and the benefits.”
External Leaders Facilitate and Disrupt
We also learned that people in leadership roles outside of the CoP would sometimes facilitate but could also inadvertently disrupt the work of the CoP. This cross-case theme recognizes that leaders in the external environment had their own mandates and objectives. In one case unexpected government actions created serious challenges and uncertainty. Our data also shows that while frontline staff are often willing to integrate new knowledge, their managers may be acting on different priorities that could disrupt the KTA process. This is one of the factors that led some CoP leaders to realize that KTA is often not a simple matter of pushing knowledge at a target audience, but can also require efforts to bring about change at multiple system levels.
A CoP2D participant summed up one of their main challenges: “One of the biggest challenges that we have been faced with is our primary group of partners … have gone through some very significant organizational and structural changes of late. …As a result there has been a great deal of the unknown that those teams have been dealing with and a lot of changes in the leadership teams …” A participant from the CoP2T initiative lamented the impact of leaders being reassigned to new roles: “…it breaks the momentum of the initiative in that long-term care home. And we almost—we don’t quite start at zero, but we almost start back at zero, to get them back on board…and that’s kind of…I’m not sure how you’d fix that.”
At Times Leadership is Provided by One or Two Key Individuals
Our data indicate that for at least three CoPs leadership was provided by one or two key individuals who made vital contributions without which the KTA initiative would likely have failed. These individuals could be CoP leaders acting as volunteers, or a KB employed by SHRTN. These key individuals provided motivation, organization, problem-solving, logistical support, and follow-ups on action items.
A CoP2D participant said, “what [name of CoP lead] has done, they’ve said, I mean, he is amazing me, he is amazing, he astounds me, he is so good at building cross sector, a true cross sector coalition, and that’s the kind of, that, this [KTA initiative] would not have been possible…” A CoP3W participant referred to a core group of leaders: “Primarily it’s been [name of CoP co-lead] and myself with, you know, [name of knowledge broker] support to drive this forward and then certainly also [information specialist]… So I would say that would be primarily the driving force.”
CoPs Navigate Hierarchical Tensions
Finally, we learned that some of the participating CoPs found that to move their initiatives forward they had to navigate hierarchical tensions within organizations or within the broader provincial health system. This theme indicates that hierarchical power arrangements in organizations and in the health system occasionally created tensions and barriers. One CoP created an alliance by delicately balancing different stakeholder agendas. Another’s espoused commitment to collaboration was diminished by existing hierarchical power arrangements. Others found it necessary to find ways to influence the behavior of health leaders without being able to draw on positional authority to compel compliance.
A participant from CoP1R told us about the differing uses of power and influence in their initiative: “…none of us have formal authority over each other, none of us can actually force a particular course of action on the whole group. Whereas with the other group that you don’t get to see, the LHIN is leading the charge, and really working more organizationally with the different providers, they being the fund holder, they being the planner, they being the designated government agency, has a certain amount of formal authority to drive the agenda.” A CoP2T participant said that when you lack hierarchical influence, you need to involve people in your planning: “I do think it needs to [include] some of the people who are doing the work… you can’t really plan unless you have got the people doing the work at the table.”
Discussion and Conclusions
Key Points Derived from Our Analysis
The main purpose of a multiple case study and its attendant cross-case analysis is to reveal patterns and themes that are common to the way in which a social phenomenon manifests itself in several distinct examples. In this study we considered how health care CoPs designed and implemented KTA processes to bring about beneficial changes in Ontario’s seniors’ health sector, and the roles that human agents play in those processes. Seven points deserve emphasis.
CoPs Support Learning and Problem Solving
First, this study shows that CoPs are a social structure capable of supporting a variety of learning and problem-solving processes. Our findings show that CoPs can function as flexible and resilient vehicles for moving knowledge into the frontlines of health care. All of the CoPs we studied achieved at least some of their intentions, with four CoPs achieving results that we consider reasonable but limited and three achieving either good or excellent results. These results suggest that the many CoPs operating within Canada’s health system are incrementally moving a variety of improvement initiatives forward and are sometimes helping to transform current mindsets in ways that will lead to a more comprehensive revamping of health services.
Our research was intended to reveal and describe the key characteristics of the KTA processes evident in nine Ontario CoPs. The study results show that these CoPs encompassed a variety of perspectives and approaches. This is consistent with findings from other studies showing that CoPs often act as fluid problem-solving forums that take on a wide variety of challenges and produce equally varied results (Bolisani & Scarso, 2014; Corso et al., 2009; Gabbay et al., 2014; Mabery et al., 2013; Mazer et al., 2015; Pyrko et al., 2017).
Our study also shows that CoPs can create a social milieu in which people who are coping with difficult work situations and professional challenges can “hold” each other by offering support and validation. The confluence of working with a frail, vulnerable population, confronting difficult challenges, and operating within a vast health bureaucracy can produce a situation in which efforts to bring about positive change are met with barriers and frustrations. In creating a social environment that fosters the persistence and resilience needed to implement improvements, these CoPs appear to act as a “holding environment” that offers the care and support needed by frontline workers (Kahn, 2001, 2003, 2005).
Dialogue, Perspective Sharing, and Collaboration
Second, our findings show that the KTA processes used by these CoPs rely on dialogue, perspective sharing, and collaboration to bring about beneficial change, and rarely make use of power to coerce people to adopt new attitudes, behaviors and structures. We saw CoP leaders and members acknowledge the need to use evidence to establish the rationale for change, and then endeavor to influence organizational cultures to shape and release new patterns of thought and behavior. We saw considerable use of communicative processes that allow participants to share perspectives while talking themselves into (as it were) new ways of delivering care to older persons living with frailty. This is consistent with recent work in organizational development and planned change, where increasing emphasis is placed on organizational culture, communication, and sensemaking (Bushe & Marshak, 2016; Hastings & Schwarz, 2022; Schein, 2014).
Incremental and Transformational Learning
Third, our study indicates that these CoPs enabled both first-order learning and problem solving in which relatively routine problems could be dealt with, as well as more exploratory learning processes when confronted with a need to bring about change at the level of cultures or systems.
Three KTA processes revealed in our findings—collaborative planning, capacity building, and informal interactions—are evanescent and open-ended, having to do with creating and extending relationships, mobilizing coalitions, forming shared intentions, and organizing actions whose purpose is to realize those intentions. Two other KTA processes—creating a knowledge product and hosting a KTA event—are more concrete. Together these processes align with the work of organizational and systems scholars who suggest that people acting within social forms (including CoPs) seek both stability and flexibility (Schulte, 2021; Taylor & Van Every, 2000; Trompenaars & Prud’Homme, 2004; Wenger, 1998; Yanow, 2004). Bringing about social change often requires that we venture into the unknown, form new relationships, experiment with new mindsets, and engage in new behaviors. For these changes to lead to desired results, it is also necessary for us to be clear on our intentions, to create supportive social structures (the “scaffolding” or “containers” called for by education and organization development scholars) and to design and implement actions likely to produce the desired results. Together, these five processes reflect a need to explore and search for new ideas and ways of behaving, along with a need to be pragmatic, clear, concrete, and intentional.
Integrating Explicit and Tacit Knowledge
Fourth, the CoPs that we studied, which operated in a health system that emphasizes evidence-based medicine, value both explicit and tacit knowledge. What must be done (explicit knowledge) is balanced with how it must be done (tacit knowledge). Seven of the case studies reveal two distinct streams of activity. The first stream focused on a KTA event, usually organized around a knowledge product and a webinar. The second was a more fluid and informal process of relationship building and discussions of shared concerns that allowed for ongoing problem framing and problem solving that had the potential to yield new and unanticipated insights.
These findings verify and enhance our understanding of a phenomenon that has been recognized in several other studies (Ardichvili et al., 2006; Bolisani & Scarso, 2014; Castaneda et al., 2018; Gabbay & Le May, 2011). KTA is not the simple transfer of scientific evidence into practice, but is rather a collision of epistemologies that produces dialogue, negotiation, and resolution. Science informs the frontline practitioner about “what” to do, while practical expertise provides guidance on “when and how” to do it. Explicit knowledge is mediated by the experience of clinical experts who consider the unique life experiences and health conditions of specific elderly patients, many of whom are living with a variety of health conditions that are being treated by several therapies. This helps to explain the importance of human interaction for effective KTA processes. Scientific evidence cannot simply be accepted and applied. Instead, it must be tested against numerous practical examples, to allow practitioners to better understand the circumstances that could facilitate or hinder the use of an innovative treatment. SHRTN CoPs often made use of vivid examples and exploratory discussions to ensure that promising evidence-based approaches were understood in the context of the capacities and concerns of older patients and the realities of heavy practitioner workloads. These CoPs created social learning processes that incorporate dialogue, interaction, and experience, thus contexting scientific advances against concrete experiences and living people.
This gave rise to two significant tendencies within the CoPs. One tendency was toward the stable and concrete, and usually involved the creation of knowledge products and the design and implementation of concrete learning events. The second tendency was toward the fluid and discursive, and generally involved the forming of relationships and building of networks and the use of open-ended exchanges.
Distinctive Roles of CoP Members
Fifth, several distinct social roles were evident in these CoPs, though these roles were mediated by the situations that faced each CoP. Our analysis revealed seven prominent roles that occurred in most cases: leader, knowledge broker, champion, thought leader, information specialist, technology facilitator, and boundary spanner. Each role, however, was brought to life differently in each CoP, again indicating the variability that has been found to be characteristic of many CoPs. Leaders were generally collaborative and encouraged other CoP members to take responsibility for aspects of the work, and in some CoPs leadership was shared by two or more people while in others there was one central leader. Knowledge brokering also emerges as an important role in the cases, bringing skills that allowed CoP members to become better organized, and to assist with logistical and technical tasks. We note that the more successful KTA initiatives were supported by a KB provided by the host network (only CoP3CC was not supported by a KB). This supports findings from other studies that reveal the contributions that KBs often make to KTA efforts (Conklin et al., 2013; Hoens et al., 2013). Project champions were influential people who persuaded others that the CoP was engaged in important work, while thought leaders contributed expertise to knowledge products or webinars. Information specialists helped CoP members to locate and access the knowledge needed to achieve CoP goals, and boundary spanners used their extensive social and professional networks to access resources and extend the reach of the CoP’s impact.
We suggest that these roles tend to ensure that the KTA initiative was well organized and coordinated, that expert resources related to relevant explicit and tacit knowledge were available to the CoP, and that resources that could assist with both webinars and ongoing boundary spanning and network building were also available. Table 12 summarizes these roles, and shows how these roles tended to serve specific functions that were significant for the CoPs and their KTA initiatives. Aside from the coordination and organization functions needed to create a modicum of stability and coherence, the primary roles show that these CoPs emphasized the access, integration, and use of explicit and tacit knowledge, the use of technology to enable communications and educational events, and the creation of broad, flexible networks of experts and interested practitioners.
Most Common CoP Roles and the Functions that they Serve.

Knowledge User Involvement
Sixth, our deductive analysis revealed that successful KTA initiatives have supported the involvement of knowledge users in most planning and implementation activities. Knowledge users played important roles in seven of nine cases, often participating as planners and designers of KTA initiatives as well as participating as trainees in webinars. Many research participants asserted that involving knowledge users in KTA processes is an important facilitator of change. Knowledge users helped to ensure that CoP initiatives were relevant to the concerns of practitioners, that frontline practice sites were aware of CoP activities, and that scientific knowledge was appropriately contextualized so as to be usable in the complex social environment of a specific practice. Our analysis suggests that in these nine cases, high involvement of knowledge users often corresponds to higher levels of implementation success.
Our analysis also reveals four factors that correspond to the effective involvement of knowledge users in the KTA processes we studied, along with five factors that hindered this involvement. The supportive factors are leadership and commitment, interaction and discussion, communication technology, and network resources, while the hindering factors are heavy workloads and competing priorities, absence of supporting structures, funding uncertainty, technical difficulties, and marketing challenges. Overall, our findings indicate that the presence of these supportive factors were sufficient to allow the CoPs to successfully navigate their way through barriers and achieve many of their objectives. We are struck by how a modest investment (most CoPs received no more than $20,000 CAD in support per year), when combined with human resolve, exploratory discussions and enabling technologies, can mobilize system-wide efforts to promote improvement and transformation.
A Possible Developmental Trajectory
Seventh (and lastly), our findings reveal a curious developmental trajectory for several of the CoPs that differs from developmental paths identified by other scholars. Much of the existing literature concerns CoPs that operate within large private sector organizations (Bolisani & Scarso, 2014; Borzillo, 2009), and some scholars have argued that CoPs operating in these environments begin with fluidity and uncertainty that over time gives way to a focus on more specific issues and concrete actions (Aljuwaiber, 2021; Pohjola & Puusa, 2016). Our study was concerned with CoPs that draw members from many organizations and occupational groups in the context of a province-wide knowledge network. In our large system and networked context, we found a complex, heterogeneous and loosely coupled host environment in which unanticipated changes were common. In this environment, several of the CoPs that we studied began with a concrete focus, then encountered and began to understand their multi-level systems environment with its competing priorities and overlapping cultures, after which they began to pursue multi-level and open-ended KTA processes that combined concrete objectives and deliverables with open-ended relationship building and networking. For example, CoP1O began with a concrete focus on the oral health needs of LTC residents, and over time realized that this seemingly straightforward gap in care would only be fully addressed through efforts to bring about change in the culture of LTC. Similarly, CoP2D initially sought to improve diabetes care for the elderly through the creation and dissemination of knowledge products, but over time learned that most effort needed to be put into creating new relationships and expanding their network of people interested in the topic. A third example is CoP3CC, which initially focused its efforts on planning and strategizing among a group of provincial leaders, and came to believe that success would require that they find ways of involving frontline practitioners in their work. We also note that CoP1R began its efforts with the view that it should focus entirely on creating a province-wide network of frontline practitioners interested in improving dementia care, and equip them with an understanding of continuous improvement techniques—with no focus on developing a centralized approach or a single knowledge product.
In short, these nine case studies offer stories of committed practitioners and researchers who want to bring improvement to the health care of seniors in Ontario. Initially many of them wanted to tackle what seemed like a straightforward challenge that was showing up in specific health care contexts, and they believed that by bringing together the right people and knowledge, usually in the form of an educational event, they would be able to solve the problem. However, as they worked on these problems, what at first seemed simple soon became complex. Most CoPs were tackling challenges arising in complex health care settings, involving a host of worries, values and choices, that turned out to be adaptive as well as technical (Heifetz & Laurie, 2001; Heifetz & Linsky, 2002; Schön, 1983). This meant that there was no single, linear solution available that could be simply imported and imposed upon the health practice. Instead, engaged and committed practitioners needed to consider the affordances and constraints characteristic of these practices and the larger systems in which they were embedded, and the relevance of knowledge available through scientific research and expert practice. Before long, the CoPs and their leaders were concluding that the changes they were promoting called for action at several levels within the health system.
This helps to explain the importance of human interaction for KTA processes. We encountered numerous instances of collaborative planning, relationship and network building, and efforts to bring the perspectives of multiple stakeholders into deliberative processes. Bringing improvement to these health practices was not a simple matter of imposing scientific findings upon the practice, or of persuading practitioners to integrate new evidence into their work—though in some cases this was clearly part of the implementation process that we observed.
The KTA processes initiated through the CoPs that we studied first emerged on the frontlines of health care where skilled practitioners encounter the challenges of providing health services to older persons. Perhaps it is time to supplement the notion of moving knowledge into action (represented by the abbreviation KTA) with a notion of using action to mobilize knowledge. These cases afforded us a view of the commitment and concerns of practitioners who represent many disciplines (doctors, nurses, PSWs, social workers, and others). Given our vantage point, we saw that these KTA processes began with action: the actions of practitioners while delivering care and reflecting together on their work, as they discover challenges and concerns that require changes to the way that work is carried out. This moment of insight arising while action is underway then catalyzes the mobilization of people and resources, held together by the CoP, as they seek a better understanding of the challenge and begin a search for solutions.
Early studies of knowledge translation emphasized the importance and fidelity of knowledge created through science, and wanted to discover a bridge—a conduit or method of transfer—that would allow this precious resource to reach the hands of practitioners where it could be put to use (Fixsen et al., 2005; Fixsen & Blasé, 1993). Over time, this view has changed. Our study helps us to understand that for scientific knowledge to be useful in practice, it must be integrated with practitioner knowledge—with the expertise, values, and preferences alive in a specific social context. In saying this, we are harkening back to the work of Fisher who invited us to consider two epistemological paradigms: the rational and narrative paradigms (Fisher, 1978, 1984, 1985). The rational paradigm reminds us that people are rational, that understanding can be reached and decisions made on the basis of data, deductions, inferences, and logical arguments, that there is such a thing as scientific and technical expertise, and that the human world gives rise to many problems that can be solved through rational analysis and dispute. The narrative paradigm, on the other hand, tells us that people are storytellers and world builders, that some decisions are made on the basis of “good reasons” or values derived from experiences unfolding within individual biographies, social histories, and cultures, and that the human world consists of manifold competing narratives that we sift through and select from based on their coherence and probability. We suggest that most of the CoPs that we studied served as a meeting place for these two paradigms.
The nine CoPs we studied provided a temporary and occasional home for dedicated practitioners who were intent on addressing shortcomings in the health system, and the improvement processes that they implemented relied extensively on relationships, connections, and interactions. They assembled within the CoP to think and work together, to bring the evidence produced by science into the busy context of day-to-day practice. These CoPs provided a sense of validation and belonging, a venue for targeted action, and a crucible for forging a bond between scientific breakthroughs and practical expertise.
CoPs as Exploratory Social Forms
Our findings illustrate three pervasive characteristics of the KTA processes that fell within the scope of our inquiry. First, these CoPs are attempting to design and implement changes within a complex system. This is evident in the first six cross-case themes presented in Table 10. The efforts of these CoPs to bring improvement and change in Ontario’s seniors’ health system must contend with the uncertainty inherent in a complex social and task system comprising well over a thousand health practices and programs serving the needs of more than 10 million users (approximately 2.5 million of whom are over the age of 65) spread across 1 million square kilometers (a geographic area larger than France and Spain combined). The CoPs designed and implemented KTA initiatives in the context of a complex provincial system made up of a bewildering array of organizations, occupational groups, big and small initiatives, strategic and tactical priorities, research projects, and distinct patient populations that in some instances supported the work of the CoPs and in others undermined that work. Moreover, this provincial system was open to influence from other health systems across Canada and other parts of the world, and was subject to political decisions of which CoP leaders might not have been aware. As they sought to bring improvements to health organizations and programs in the midst of this complexity, many CoPs discovered that their interventions needed to be targeted at multiple levels within the provincial health system. At the same time, unexpected actions originating at various system levels sometimes disrupted the intentions and actions of the CoPs. For example, CoP2D designed an intervention that required the active support of a special administrative team whose members were located throughout the province, but midway through the intervention this team’s mandate was fundamentally and unexpectedly changed by the government, making it impossible for them to play the role that they had agreed to. Navigating around this unexpected barrier became a vital priority that consumed the attention and energy of CoP leaders for several weeks.
The cross-case themes also show that the complexity of the system gave rise to increasingly complex interventions. The CoPs formed multiple purposes, designed and implemented diverse action plans, and attempted to recruit new members and connect with varied audiences. Though some CoPs began by designing very specific KTA events (such as webinars) for specific audiences (such as frontline workers in LTC homes), they came to realize that more varied approaches were needed. For example, an effort to improve oral health care was initially seen as just a skill-building exercise but soon grew to encompass efforts to shift the culture in LTC homes (Kothari et al., 2015).
The complexity of the system in which the CoPs function also produces a need for collaboration and interaction. Numerous perspectives are needed to reveal the scope of the issues that CoP members wish to influence, and action is required in many system contexts in order to shift existing patterns of thought, behavior, and structuring. The CoPs began by bringing people together around shared objectives and strategies. Members worked together to seek common ground, create partnerships, and build networks of caregivers, policy makers, educators and researchers who were committed to shared objectives. Intensive collaboration, however, is often time consuming and requires deft interpersonal skills. These constraints sometimes limited the effects that CoPs were able to achieve.
Complexity also gives rise to a need for multiple strategies to access diverse knowledge sources and to disseminate relevant knowledge to stakeholder groups. Most CoPs used a variety of techniques to achieve their objectives. All of the CoPs we studied used collaborative planning processes, and most also employed deliberative dialogue, adult learning, web-based learning, information design, coaching, online discussion forums, and other methods to reach their audiences, and frequently endeavored to tailor the knowledge to make it useful in local practices.
The fact that CoP members and potential stakeholders were spread across numerous organizational contexts within a vast geographic area made it necessary for the CoPs to draw on communication technology, inclusive planning processes, and logistical supports available through SHRTN. Without ongoing coordination efforts, CoP initiatives would have become fragmented and anemic. Without web-based and teleconference technology, it would have been impossible to invite participation from practitioners throughout the province. Complexity encouraged CoP leaders to plan carefully and deliberately, to rely on the supportive efforts of KBs and librarians, and to use technology to build and maintain their coalitions.
Second, to bring about change within this complex system, the CoPs acted as a temporary social context that enabled relationality, reflexivity, experimentation, and learning. Scholars and practitioners of social change often state that complex change requires the creation of a special social context—a container—that can help change leaders to cope with the discomfort of uncertainty and risk, and to access support from like-minded colleagues and experts (Bushe, 2010; Conklin et al., 2012a, 2012b; Corrigan, 2016; Kahn, 2012; Smith, 2003).
SHRTN CoPs were formed to take action on specific challenges related to seniors’ health, and received funding to carry out a 12-month initiative. The relationality of the CoPs (through which they brought together people, ideas, and expertise) is evident in our narrative descriptions of the cases, and from the third, fourth, and sixth cross-case themes. The reflexivity of these CoPs is evident in their collaborative planning processes, and their propensity to learning is evident in ways in which CoPs arrived at a better understanding of the challenges they faced (outlined in the narrative descriptions) that often resulted in altered plans and approaches. CoP3D, for example, significantly revised their approach midway through their year when the DRCC role was suddenly changed, while CoP1OH concluded that the realities of LTC meant that improved oral health care required not just skill training but also culture change. Similarly, the CoP1R initiative allowed for a collaborative process that would lead to unique solutions in local health contexts (thus requiring a process of learning).
Our inductive analysis shows that these CoPs functioned as contexts that supported action directed toward change and improvement. Many of the CoP leaders recognized that KTA cannot be reduced to a single deliverable such as a knowledge product. KTA involves action that promotes adoption, experimentation, and prolonged use. Some CoPs functioned as platforms on which groups and networks could form around shared concerns and goals, and from which relevant knowledge could be gathered, appraised, and mobilized. Moving outward from the security of these supportive platforms, stakeholders became willing to try to influence the delivery of care in their regions and organizations.
The flexibility that was characteristic of these CoPs gave rise to a temporary and somewhat evanescent character that was evident in part through the ongoing turnover of leaders and members. This informal and fluid membership produced two notable effects. On the one hand it promoted inclusiveness, diversity, resilience, and renewal, while on the other hand it could also introduce moments of confusion and instability. New people, with access to new resources, relationships, and expertise, became available at different points in time, and many CoPs used this ongoing turnover in membership to extend their reach through the personal networks of new members. However, fluidity was also evident when influential individuals and groups dropped out of CoP activities due to changes in mandates or jobs. When this happened, CoP activities were sometimes temporarily suspended so more planning could occur to identify new ways of moving forward.
Third, our cross-case themes indicate that the problems addressed by these CoPs are best understood as adaptive challenges rather than as technical problems. Many scholars have pointed out that it is useful to distinguish between problems that are essentially technical in nature and those that are adaptive (some prefer the terms wicked or systemic problems, or aleatory uncertainty) (Heifetz & Laurie, 2001; Holman, 2015; Kahane, 2004; Porteous, 2013; Rittel & Webber, 1973; Schön, 1983; Senge et al., 2015; Tetlock & Gardner, 2015).
A technical problem is a type of problem that falls into one or another domain of technical expertise, and can be solved by calling upon the relevant technical expert to identify and apply the known solution. An adaptive problem is a type of problem that falls into the realm of incommensurate human values, culture, ideologies, preferences, and life experiences. To make headway on an adaptive problem, we must bring people together to share perspectives, reasoning, and experiences, to see if we can find a common framing of the challenge that we are considering, and to discuss what actions are acceptable to most stakeholders that might serve to mitigate or resolve the problem.
The SHRTN CoPs that we studied often began their initiatives with an aim of introducing new knowledge through training. As they developed or refined their knowledge products and designed and delivered their webinars, they often realized that more complex cultural or systems change would be needed to fully achieve their aims. This is evident, for example, in the work of CoP1O to improve oral health care, CoP1P to improve the physical layout of LTC homes, and is also present in the CoP2DD1 and CoP3DD2 initiatives to foster collaboration and connection between the developmental disabilities and LTC sectors. Our first, second, fourth, and fifth cross-case themes in Table 10 also highlight the complexity of the challenges that these CoPs seek to address.
Some CoPs in our study recognized the need to navigate through the hierarchical power arrangements that are evident in the provincial health system. These CoPs discovered that the distribution and use of hierarchy and power in the health system could create tensions and barriers. One CoP made it a priority to discover and then balance different stakeholder agendas, while another discovered that existing power arrangements created barriers to forming a collaborative to bring about change. CoPs often found it necessary to influence the behavior of health leaders without being able to draw on positional authority to compel compliance. Most CoPs came to invest heavily in networking, interaction, and relationships.
It also became evident to most CoPs that change in health care organizations would not result from the imposition of a uniform (or one-size-fits-all) intervention carried out by a central group of change agents. Instead, CoP leaders came to realize that change would only occur if interventions were tailored to and aligned with the needs and situations of specific caregiving contexts. This sometimes took the form of a KTA process that sought to empower participants with the motivations and skills to make changes to frontline practices, without dictating precisely what these implementation efforts would look like. Other CoPs used a multi-faceted knowledge development process whose variety stemmed from the need to tailor KTA products and events to the different situations faced by participating frontline workers.
Adaptive challenges are characterized by numerous perspectives and behaviors that can sometimes disrupt a carefully planned sequence of actions. Some CoPs found that health leaders in organizations outside of the CoP made decisions and implemented strategies that inadvertently impacted the work of the CoP in helpful or disruptive ways. Virtually all of these CoPs formulated objectives that would likely have received broad support from health leaders across the system—objectives having to do with making life better for people living with dementia and for health care personnel providing care to these patients, with improving diabetes and oral health care for LTC residents, with assisting the transition of people living with developmental disabilities from their home in the community to a care facility, and so on. The CoPs represented a temporary social context in which members could “think together” about recalcitrant adaptive challenges, sharing tacit knowledge while also accessing research evidence that could support efforts to bring about new learning and positive change (Pyrko et al., 2017). However, the health system is made up of numerous overlapping and nested organizations and subsystems, all interacting together in a province-wide system, and work is carried out in the midst of a changing set of program, organizational, and system priorities. It is not surprising that on occasion one health leader’s priority might impact negatively (and inadvertently) upon the work of a CoP. Our data show that while frontline staff are often willing to integrate new knowledge, the actions taken by leaders could sometimes interfere with and disrupt the KTA process.
This meant that determined, committed, and resilient leadership was often necessary for the CoPs to see their initiatives through to completion, and we found that this leadership was present in most of the CoPs. Leadership might be provided by one person or a small team, and often included the work of the KBs who were employed by SHRTN. Many of our interview participants told us that without this core group of determined leaders, the CoPs would have struggled to achieve their objectives. These key individuals provided motivation, organization, problem-solving, logistical support, and follow-ups on action items.
Considered together, our eleven cross-case themes speak to the complexity of Ontario’s health care system, and to the challenges that arise from this complexity when members of a CoP take action to bring about beneficial change in frontline caregiving contexts. Many CoPs found it necessary to access knowledge from a variety of sources, and to devise a variety of interventions or a multi-part intervention. Given the complexity of the system—which many interview participants characterized as fragmented by silos and competing priorities—the use of networks, community-based approaches, and interactive methods allowed CoP leaders to approach change as a general capacity-building exercise rather than as an effort to change a specific behavior in a specific caregiving site. Though webinars were the most common KTA vehicle, CoPs often seemed to be engaged more in an effort to influence people rather than to educate them.
The themes also illustrate that these CoPs found themselves confronted with opportunities and challenges that often arose from the same source. The health care system is the site of numerous policy imperatives and change initiatives that are intended to produce beneficial improvement, and that also constitute a turbulent and unpredictable social environment. The SHRTN CoPs offered an opportunity to receive support and to pursue connections with like-minded professionals interested in solving problems in health care workplaces. SHRTN was also a source of uncertainty as the government considered the future of the network and delayed making a decision on ongoing funding. Moreover, the provincial government launched other initiatives that inadvertently redeployed existing resources that were a vital part of the change initiatives that some CoPs were pursuing. The CoPs themselves reflected the fluidity and uncertainty of the broader environment, with membership and leadership roles constantly changing. This allowed the CoPs to constantly discover new resources and ideas, and it also made it more difficult to sustain the continuity of interventions.
These themes suggest that CoPs represent a strategy to allow for learning, cross-fertilization, and innovation in a complex and fragmented health system. A CoP opportunistically brings people together from different groups and organizations, and leverages existing networks of relationships to create channels through which knowledge might travel. Ontario’s health system comprises a complex network of relationships among individuals, licensing bodies, institutions, programs, government organizations, health charities, patients, and others, interconnected by numerous communication and interaction channels. Overtop this is positioned a CoP whose members are located at various places within this complex environment, thus providing the CoP with multiple gateways into the system.
A Theory of Action for Communities of Practice
Our cross-case analysis produced Figure 1, which we offer as a broad theory of action to explain the behavior observed in these CoPs.
We are using the term theory of action in the sense of program evaluators (who also use the term program theory) and action scientists, who suggest that people who design programs or interventions to bring about change do so on the basis of a theory of action (implicit or explicit) that posits that a certain action or set of actions will produce certain effects (Argyris et al., 1985; Rogers et al., 2000). Evaluators use the concept to understand the intentions underlying the program that they are to evaluate. Action scientists use it to create an activity map of the task and social environment that is experiencing dysfunction and is seeking improvement.
The theory of action evident in the work of these CoPs includes seven important components. First, responding to the invitation from SHRTN, a group of people come together to form the CoP around a particular concern or topic in seniors’ health. Together they investigate shared issues and concerns, often by conducting a needs assessment among relevant health care programs, facilities, and practitioners, and agree on a problematic situation or challenge that requires a solution.
Second, CoP members delve further into the nature of the problem and arrive at a shared understanding of the problem and how it might be ameliorated. They do this by assembling explicit knowledge (usually evidence-based knowledge created through science) that sheds light on the problematic situation that the CoP intends to address. Third, the CoPs also recognize that this explicit knowledge that has been created and assembled far from frontline caregiving sites must be integrated with tacit knowledge to make it relevant for and acceptable to the knowledge users who are immersed in their busy worlds of practice. Often knowledge users were invited to enter into the CoP’s planning process and directly influence the interpretation and tailoring of the explicit knowledge, and sometimes expert practitioners were invited to play that role on behalf of a broader audience of knowledge users. Some CoP leaders refer to this step in their process as individualizing the recommended treatment approaches to make them appropriate for the patient, or tailoring the knowledge to make it meaningful for specific groups of frontline practitioners.
Fourth, the contextualized knowledge is conveyed to the intended audience through an educational activity enabled by web technology, though on occasion it also included face-to-face interaction. The most common example of this was the webinar, with CoP leaders facilitating the event, and expert speakers explaining how the new evidence-based knowledge could best be used in common practice situations. Sometimes the webinar would lead into a follow-up activity, which might include an online message board that allowed participants to discuss their experiences in applying the knowledge in practice, or a follow-on webinar discussion that allowed participants to problem solve their implementation challenges in a supportive environment. Though the nature and strength of these follow-on activities varied, all of the webinars were expected to be followed by the fifth component of the CoP theory of action, which consisted of knowledge users attempting to apply the knowledge in practice. This effort to implement the knowledge was generally beyond the direct reach of the CoP leaders, and although they often received anecdotal accounts of successes and frustrations, they were unable to assess the extent to which the educational activities brought about concrete and sustainable change.
However, by creating a community of interested experts and knowledge users, and by using a collaborative process that often brought numerous people into a planning process that invited contributions from practitioners across the province, the CoP’s theory of action included a second trajectory that begins with the sixth component: the creation and maintenance of a network of relationships of interested practitioners (as well as researchers, policy makers, and educators) who worked in institutional and geographic contexts across the province. While they focused specifically on the creation and delivery of the educational webinars, they also allowed their discussions to range widely over the issues that concerned them, and the challenges and opportunities for effecting change. Many of them noticed and discussed the possibility that frontline practice change was unlikely if the broader system was not supportive of the change. They talked about the need for policies and mandates emanating from the provincial health ministry and from the LHINs that provide regional oversight, and the need for a supportive culture in the organizations where change was to occur. In some cases, these discussions gave rise to advocacy efforts that extended beyond the target audience for the webinar. In other cases, they expanded their target audience to include decision makers who might be encouraged to create new policies and procedures consistent with the knowledge being conveyed through the webinar. Out of these fluid relationships and discussions emerged the seventh component of the CoP theory of action, which consisted of ongoing relationships and discussions about changing practice.
This stream of activity was deliberative and open-ended, and tended to resemble a process of second-order change or double-loop learning whereby CoP members might reconsider their own assumptions and mindsets as they sought sustainable solutions to intractable challenges (Argyris, 2004; Bartunek & Moch, 1987). We highlight the way in which the theory of action characteristic of the CoPs we studied aligns with social learning theory in Figure 2.
The initial problem-framing phase yields a diagnosis along with an effort to move useful knowledge into practice through a knowledge product, educational event, and follow-on activities. This effort culminates in individual attempts to apply the new ideas and approaches in specific practices. The implementation challenges encountered in these practices would often be reported back to CoP members (and in some cases the CoP leaders and members were themselves involved in implementation efforts on the frontlines), leading to a consideration of whether the webinars, knowledge products, and other translational techniques might be improved in some fashion.
However, at the same time the challenges encountered would become the subject of open discussion and deliberation among CoP members, fueling a process of second-order learning that encompassed the original attitudes, goals, and assumptions that had sparked the initiative. Some CoPs reconsidered their original didactic and technical approach to the problematic situation, and realized that success would require that they mobilize efforts to intervene at more than one level of the provincial health system. In some cases, this resulted in the creation of new approaches and initiatives that would build upon what had already been accomplished, or that would attempt to influence the policy and cultural environment that was perceived as creating barriers to beneficial change.
These CoPs, then, could be seen to engage in a process of learning and adaptation that could encompass an expanding awareness of the complex interdependencies at work within the health system. The CoPs showed a distinct orientation to action that is evident in the creation of knowledge products and the development and delivery of webinars. They also displayed a growing awareness of the need for network expansion and perspective sharing to promote new conceptualizations and ideas, along with the creation of the relationships needed to mobilize action at multiple system levels. In effect, CoP members needed to be focused and intentional about seeking to improve a problematic situation, and also aware that the health system is characterized by numerous complementary, overlapping, and competing interests. To create improvement, it was often necessary to search for opportunities in the baffling web of perspectives, interactions, and structures that make up the system.
Earlier in this monograph we shared an example from CoP1R, which aspired to better meet the needs of people living with dementia who exhibited responsive behaviors. This example illustrates how second-order change took shape through expanding networks and exploratory discussions (all information in this example is derived from CoP1R interview data), and is worth restating here. While CoP leaders and members were militating for improvements in the care of people with dementia, provincial policy makers were more concerned with unsustainable pressures that were being placed on Ontario hospitals. At that time much attention focused on Alternate Level of Care (ALC) patients who occupied beds in acute care institutions that provided resources and services of a greater intensity than that needed by the patient. The ALC patient was viewed as “wasting” system resources, and as preventing another patient from receiving needed care. At the time when the CoP1R initiative was underway, researchers and policy makers were beginning to recognize that a significant number of hospitalized patients with an ALC designation were people with dementia (McCloskey et al., 2014). Data were indicating that those patients with dementia and responsive behaviors were unable to reintegrate into LTC homes or the community, and thus were “stuck” as ALC patients in acute care facilities.
One of our CoP1R participants told us during a closing interview, “I remember the day that the ADM [Assistant Deputy Minister] was told that the ALC problem is a dementia and behavioral problem. He said, ‘Really?’ And, ‘You mean that 34% of people in the ALCs in hospitals are people with dementia?’” These patients were categorized in terms of problems related to the heart, kidneys, lungs, and so on, instead of in terms of their cognitive impairments, but it was the cognitive impairment that was keeping them in ALC. That realization was the trigger for a sudden growth in interest on the part of policy makers around dementia and responsive behaviors. If the capacity of health care workers and informal caregivers in the community and in LTC could be increased so they were able to work effectively with people with responsive behaviors, considerable progress would be made on the ALC problem.
In other words, the CoP1R leaders and their network of partners had created a platform of practitioners who were advocating for change. People living with dementia and their family members were indicating that this problem was having a significant and negative impact on quality of life. A growing number of researchers were focusing on people with complex cognitive disorders and were bringing to light the difficulties being experienced by both patients and health care providers. And finally, senior policy makers, who set provincial priorities and ultimately controlled health system funding, realized that if they could solve the challenge of responsive behaviors, they would simultaneously alleviate the ALC problem. As our participant told us during this interview, these factors converged into a “perfect storm” of motivation and activity that propelled the CoP initiative toward success. The breakthrough had little to do (at least directly) with the “local conversations” that were the main activity undertaken by the CoP, and much more to do with the discussions, deliberations, and networking carried out by CoP leaders around their shared concerns.
Conclusions and Implications
The research reported here has added to our understanding of the way that CoPs can contribute to the movement of evidence-based and experiential knowledge into frontline health care practices. We close by highlighting six points that indicate the importance of this research.
First, this research shows that a CoP can function as a temporary social context that enables reflexivity, relationality, experimentation, and learning, and that initiating improvements within the health system often takes the form of a wide-ranging response to a vexing adaptive challenge.
Second, our research confirms the importance of CoPs as a vehicle for understanding and taking action to resolve adaptive challenges. Like Iaquinto et al. (2011), we found that SHRTN CoPs encountered seemingly intractable problems that involved numerous factors, requiring a multidisciplinary response. The mindsets, actions, and structuring evident through these CoPs demonstrates a way of responding to an adaptive challenge. When encountering a situation that appeared problematic and intractable, CoP leaders found it necessary to think about systemic issues and system levels, and to think about creating the conditions needed to bring about helpful change. Our case studies reveal an attitude toward change and a process for bringing about change when faced with a wicked problem. The attitude has to do with curiosity and an orientation to learning and experimentation through action, and the process is incremental and reflective. Our findings support those of Iaquinto et al. (2011), suggesting that a CoP operating within a systems context—that is, within an emergent and complex problem area involving many people and groups—can help to highlight the systemic nature of the problem, create a context for bringing people together and sharing diverse perspectives on the problem area, and develop the capacity of CoP members to take action. Like Iaquinto et al. (2011), we also found that CoPs operating within a complex system can be vulnerable to shifting priorities and new initiatives launched from the top of the hierarchy. Given the dominant approaches to leadership and decision making in our health system, senior policy makers were oriented toward their system in a top-down manner and were for the most part unaware of the SHRTN CoPs and their efforts. In some cases this meant that well-intended reforms interfered with CoP plans and thus impeded useful change and innovation.
Third, our findings suggest that a CoP operating within the context of a complex system may experience a developmental trajectory different from one operating within a simpler organizational context. Others have found that a CoP focused on creating a tangible product to satisfy an organization’s objectives will face many concrete and technical concerns and will experience a trajectory that begins with uncertainty, evident in goals and plans, and then moves toward a reduction in uncertainty as CoP members focus on one or more concrete problems (Pohjola & Puusa, 2016). Our study, however, suggests a different trajectory for CoPs dealing with adaptive challenges in the midst of an uncertain system context. Although some SHRTN CoPs began with a clear goal focused on a concrete problem, many came to realize that this problem arose in the context of a complex social system that was influenced by forces originating at different system levels—with individuals, specific practice groups, an organization, a region, or the overall provincial health system. Before useful solutions could be identified, CoP members needed to understand that they were working in a complex and overdetermined environment, and devise a process to allow them to access new perspectives and test and monitor various solutions. In effect, these CoPs began by identifying a problem and devising a single-loop approach to its solution, and over time developed a new and more nuanced understanding of the problem and a double-loop approach.
Fourth, our research suggests that even when a CoP is intentionally created by system leaders, and is to some extent supported and managed by those leaders, the nature of the CoP phenomenon is to be exploratory and relatively unconstrained. To add something new to efforts to improve and transform a health system, a CoP offers an exploratory and adaptive response to the shared problem that CoP members have assembled around. CoPs can function as a context in which participants from different backgrounds and with different expertise and levels of experience can share different concerns and perspectives, can in effect think together (Isaacs, 1999; Pyrko et al., 2017) and arrive at innovative solutions capable of functioning at more than one system level. Our findings indicate that when some CoPs grapple with a compelling problem of practice they soon discover the systemic complexity that surrounds this problem, and then begin to consider new approaches and solutions.
Fifth, we are reminded of the call to action issued by Bowen and Graham: “We must collectively find ways to provide incentives to both researchers and knowledge users to work together in identifying pressing research questions and conducting solutions-focused research to address these questions in a timely manner” (Bowen & Graham, 2013, p. S7). Our findings suggest that CoPs represent one of the ways in which this important collaboration can be achieved. These case studies reveal that KTA is often the integration of explicit and tacit knowledge in a specific organizational context. The CoPs emerge as a social framework that hosts the process of inquiry as practitioners search for solutions to difficult problems. CoPs offered support and encouragement while new ideas were discovered, debated and tested, and allowed for the creation of relationships and networks that could heighten the system’s capacity to learn and innovate. They act as a venue for the reflective practice mandated by many licensing bodies, which Donald Schön described as the “…dialogue of thinking and doing through which I become more skillful” (1987, p. 31).
Innovation has been shown to be a messy and emergent process that yields errors and failures before producing success (Van de Ven et al., 2008). Understandably, health care organizations and the people they serve have a low tolerance for errors. At their best, CoPs allow health care practitioners to step outside the boundaries of their workplaces and enter a supportive social environment where the urgent needs of practice and the findings of scientific research can be integrated, tested, and put into action.
Sixth, we suggest that our findings and conclusions indicate that the CoP as a specific type of social arrangement is more relevant than ever. The global coronavirus pandemic that struck in early 2020 is a near-perfect example of a wicked problem (Moon, 2020; Pourdehnad et al., 2020; Radin, 2020), and a problem moreover that local, national, and international leaders struggled to mitigate. In Ontario, where our research took place, and also in other jurisdictions in Canada and around the world, the pandemic has had devastating, lethal effects among the frail elderly living in LTC homes (Estabrooks et al., 2020). It is reasonable to ask how health practitioners and leaders might organize themselves to better understand and respond to the unexpected trajectory of a virus such as COVID-19. Our research suggests that a CoP, where hierarchy is diminished and relationships are expanded to maximize access to useful perspectives and experiences, where a process of social learning is created that allows new ideas to be proposed, tested and monitored, all in an incubator of inescapable real-life situations demanding immediate and urgent attention, is worthy of serious consideration.
Further research is needed to verify and extend our conclusions. Have other researchers found that CoPs are able to enact a double-loop learning process when faced with intractable problems? Is this phenomenon mediated by the nature of the context that houses the CoPs, or by the form and extent of control or direction exercised over the CoPs? Is it possible to identify and describe specific development trajectories for CoPs based on the contexts in which they operate and the problem types that they deal with; and, if this is possible, might this offer guidance for CoP sponsors who intend to nurture and develop effective problem-solving CoPs?
Strengths and Limitations
Our methods allowed us to gather a large quantity of data concerning the phenomenon that interested us, and to provide a comprehensive description of that phenomenon. We assembled comprehensive qualitative databases on the basis of multiple data-collection methods and data sources, and we used rigorous deductive and inductive analytical procedures to produce our findings and conclusions. We are confident that these findings and conclusions are an accurate reflection of the experiences of the nine instances of KTA processes in these CoPs.
These methods also involve certain limitations. Our findings do not allow us to draw generalizations about all KTA efforts undertaken by CoPs, nor can we make predictions about the future.
Our data collection efforts were necessarily influenced by the questions that we asked and by the inclinations and preferences of the CoP members who participated in our study. Although we made an effort to gather all of the relevant data, we acknowledge that these data can be only a partial representation of the phenomenon that was the focus of our study. Our findings and discussion reveal important aspects of KTA processes undertaken by the participating CoPs, and it is likely that additional interesting discoveries have yet to be made.
The CoPs whose KTA initiatives formed the basis for our nine cases operated within a particular social and political context—that of the province of Ontario, Canada, from 2009 to 2014. There is no doubt that the economic, social, technical, and medical environments of that period were characterized by features that were unique to that time and place, and these features may have changed in the intervening years. This suggests that readers should be cautious in drawing conclusions from our research about CoPs operating in very different contexts.
Most previous work has focused on CoPs that formed and operated within a single organization. Our study looked at CoPs operating in a sector or system, with members drawn from many organizational contexts. Our findings thus contribute to ongoing work that is identifying the characteristics of CoPs operating in network or system contexts. For example, we found that CoPs operating within a health system tend over time to broaden their focus and interest to take in systemic barriers and devise multifaceted approaches to change. It is also possible that the type of leadership support needed for this sort of work differs from the support offered to organizational CoPs. Whereas some work has shown that organizational CoPs are more successful when organizational leaders help them to focus on specific problem areas deemed important by leaders (Borzillo, 2009), our study indicates that health system CoPs can succeed without system leaders influencing goals and providing direction.
Several of the CoPs that participated in our study tried to mitigate or solve specific problems that occurred in specific practice contexts, and over time came to see a need to reframe these problems and take a more system-level view of their work. Are CoPs equally adept at learning and problem solving related to well-understood technical challenges as well as more puzzling adaptive challenges? To what extend do CoPs operating in a context such as a health system prioritize targeted and precise change efforts as opposed to efforts to share perspectives, create new understandings, and nurture the capacity to pursue improvements at different system levels? Are there specific ways in which CoPs bring about the integration of explicit and tacit knowledge, and how does this correlate with success in change efforts? We believe that further work is needed to confirm and possibly extend these findings.
Supplemental Material
sj-doc-1-sgo-10.1177_21582440241281644 – Supplemental material for Moving Knowledge into Action Through Communities of Practice: Multiple Case Studies of Successful System Change to Improve the Health of Older Adults
Supplemental material, sj-doc-1-sgo-10.1177_21582440241281644 for Moving Knowledge into Action Through Communities of Practice: Multiple Case Studies of Successful System Change to Improve the Health of Older Adults by James Conklin, Anita Kothari, Paul Stolee, Larry Chambers and Ken LeClair in SAGE Open
Supplemental Material
sj-doc-2-sgo-10.1177_21582440241281644 – Supplemental material for Moving Knowledge into Action Through Communities of Practice: Multiple Case Studies of Successful System Change to Improve the Health of Older Adults
Supplemental material, sj-doc-2-sgo-10.1177_21582440241281644 for Moving Knowledge into Action Through Communities of Practice: Multiple Case Studies of Successful System Change to Improve the Health of Older Adults by James Conklin, Anita Kothari, Paul Stolee, Larry Chambers and Ken LeClair in SAGE Open
Footnotes
Abbreviations
AKE – Alzheimer Knowledge Exchange
ALC – Alternate Level of Care
CoP – Community of Practice
DRCC – Diabetes Regional Coordination Centre
HCP – Health Care Provider
KB – Knowledge Broker
KTA – Knowledge-to-Action
LHIN – Local Health Integration Network
LTC – Long-Term Care
PARIHS – Promoting Action on Research Implementation in Health Services
PI – Principal Investigator
PSW – Personal Support Worker
RN – Registered Nurse
SHKN – Seniors Health Knowledge Network
SHRTN – Seniors Health Research Transfer Network
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research described in this monograph was funded by a grant from the Canadian Institutes for Health Research (CIHR), Funding Reference Number 106696.
Data Availability Statement
The raw data on which this study is based cannot be shared due to the terms of the ethics clearances for the project. However, the nine narrative case study reports that were produced through the deductive and inductive analysis, and the three cross-case analysis reports that were produced through the cross-case analysis, can be obtained through a request to the first author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.