
Abstract
Integrated early childhood development (ECD) programs boost child health and developmental outcomes. However, the factors contributing to the successful implementation of such programs in informal urban settlements are not well researched. We conducted 14 focus group discussions and 13 key informant interviews with 125 caregivers of children under the age of 5 years and stakeholders, exploring their views on enablers and barriers to implementing an integrated ECD program in an informal settlement in Kenya. Strategic engagement, capacity building, transparency, fair compensation of ECD workforce, communication skills, and the need to tailor ECD programs to local realities were discussed. An equity-focused implementation approach for integrated ECD programs is timely.
Introduction
Children under the age of 5 years in low-and-middle-income countries (LMICs) face the greatest risk for not reaching their development potential (Black et al., 2017; Tran et al., 2017). A myriad of factors, mostly relating to early life exposure to deprivation and threats like malnutrition, household poverty, violence, poor health of caregivers, and insufficient cognitive stimulation are some of the underlying factors (Tran et al., 2017; Walker et al., 2011). Therefore, interventions are urgently needed to reduce child and familial exposure to risk and promote optimal development in affected children. The Nurturing Care Framework for Early Childhood Development (NCF), launched in 2018 provides a road map built on the best available evidence of how children develop and which policies and interventions improve development and thriving in the early years of life (WHO-UNICEF-WorldBank, 2018). The NCF emphasizes the need for an integrated approach to early childhood development (ECD), whereby efforts should wholesomely address young children’s needs for good health, optimal nutrition, security and safety, opportunities for early learning, and responsive caregiving (WHO-UNICEF-WorldBank, 2018). The evidence from LMICs supports the effectiveness of integrated ECD interventions in boosting developmental outcomes (i.e., cognition, language, and motor development) for young children (Zhang et al., 2021) and improving caregivers’ outcomes (like mental wellbeing, maternal knowledge of ECD, mother-child interactions, and parenting skills; Jeong et al., 2018; Shi et al., 2018). Integrated ECD broadly refers to ECD programs which combine multiple services or supports across different agencies in health, social welfare, employment services, and education (Britto et al., 2014). Also, integrated ECD is more effective than standalone interventions because it involves the use of similar resources such as facilities, client contacts, transportation, for different components, and thereby can help to harmonize the goals and strategies of various departments to improve cost-effectiveness and sustainability (DiGirolamo et al., 2014).
Successful implementation of integrated ECD programs is fundamental for the sustainability of these programs, and it is a growing concern for researchers, funders, evaluators, and community partners (Cavallera et al., 2019; Milner et al., 2019; Pérez-Escamilla et al., 2018). Program sustainability refers to the existence of structures and processes which enable a program to leverage resources to implement and maintain evidence-based policies effectively and activities (Schell et al., 2013). Conversely, inefficient implementation leads to resource wastage and loss of community trust and thus the lack of sustainability of ECD programs in the long run. Research on integrated ECD programs in LMICs acknowledges the complexities resulting from the multi-sectoral nature of ECD (Pérez-Escamilla et al., 2018) and that a variety of challenges must be addressed for ECD interventions to be successful and sustainable (DiGirolamo et al., 2014). For example, research on ECD from Chile, South Africa, Bangladesh, and India has shown a common tendency to implement a “one-shoe-fits-all” design, making it difficult to achieve responsiveness to local needs (Pérez-Escamilla et al., 2018). Other researchers have noted a disconnect between what is designed at the protocol level and what is feasible in reality. Therefore, they have emphasized the need for improved cohesion between the stakeholders involved in protocol design and those with contextual knowledge and expertise of the local setting that the ECD program is intended to be implemented and scaled (Cavallera et al., 2019). Other considerations for the successful implementation and sustainability of integrated ECD programs in LMICs include the need for transparency and accountability; strategic approach to the components of planning, supervision, human resource capacity, monitoring, evaluation, and learning; equity in the identification of beneficiaries; strong leadership; funding stability; strategic and open communication; and the ability for the program to impact positive change (Cavallera et al., 2019; DiGirolamo et al., 2014; Luoto et al., 2021; Pérez-Escamilla et al., 2018).
Noteworthy, the underlying factors which influence the sustainability of integrated ECD interventions in informal urban settlements are complex and currently not well researched within LMICs in sub-Saharan Africa—where almost 60% of urban dwellers reside (UN-HABITAT, 2014). In Kenya, for example, informal urban settlements are usually located in environmentally non-conducive settings lacking adequate access to formal services, which leads to high competition for meagre resources, thus increasing adversity among families (Mutisya & Yarime, 2011; Ren et al., 2020). In addition, there are pockets of vulnerable dwellers who are immigrants in such settings, some of whom may lack legal documentation of their residential or nationality status (UNHCR, 2020). Besides, multiple layers of leadership and representation often exist in informal urban settlements in Kenya owing to the diverse sub-communities (Dafe, 2009; Wanjiru & Matsubara, 2017). Collectively, these realities suggest that some of the factors affecting ECD program success and sustainability are universal, and some are potentially unique to informal urban settlements. Therefore, it is of significant value to meaningfully engage and consult with local stakeholders plus community members across all stages of the design and implementation of integrated ECD programs to examine their opinions on potential barriers, enablers, and opportunities for improving ECD program implementation. This step also aligns with the NCF’s emphasis on parents, families, and other primary caregivers as the main providers of nurturing care, and whose specific needs and capacity should be supported in meeting all the needs of young children (Britto et al., 2017; WHO-UNICEF-WorldBank, 2018).
The present qualitative study was conducted to understand factors underlying the sustainability of integrated ECD programs within an informal urban settlement of Dagoretti sub-county in Nairobi city in Kenya from the perspective of caregivers and key stakeholders. This work has contributed toward guiding the design of an ongoing intervention that operationalizes the nurturing care framework within this informal settlement.
Theoretical Framework
We utilize a framework for conceptualizing program sustainability by Shediac-Rizkallah and Bone (1998). According to the authors, “sustainability appears to be a multi-dimensional concept of the continuation process and the term encompasses a diversity of forms that this process may take.” Their framework identifies three major factors that influence program sustainability: project design and implementation, organizational setting, and broader community environmental factors. The project design and implementation factors refer to resources available to the project, for example, staff, financial resources, and time for project implementation to reach fruition. They suggest that implementers should ensure a sufficient project negotiation process, pay attention to the project type and ensure that the project is effective, pay attention to the adequacy of the program duration, paying attention to project financing, and the need for professional development. The organizational setting factors refer to organizational and managerial structures and processes, which can include aspects to do with: institutional strength, level of integration with existing services and programs, program champion or leadership, also including administrative structure, and the political process within the organization, which can either support or inhibit its continuation. The broader community environment-related factors refer to the socio-economic and political environment and the involvement/participation of community members in the program. The authors of this framework acknowledge that some of these factors are well accepted, while others have received less empirical support. Some of the factors are more amenable to control by program staff than others (Shediac-Rizkallah & Bone, 1998).
Methods
Study Criteria and Recruitment
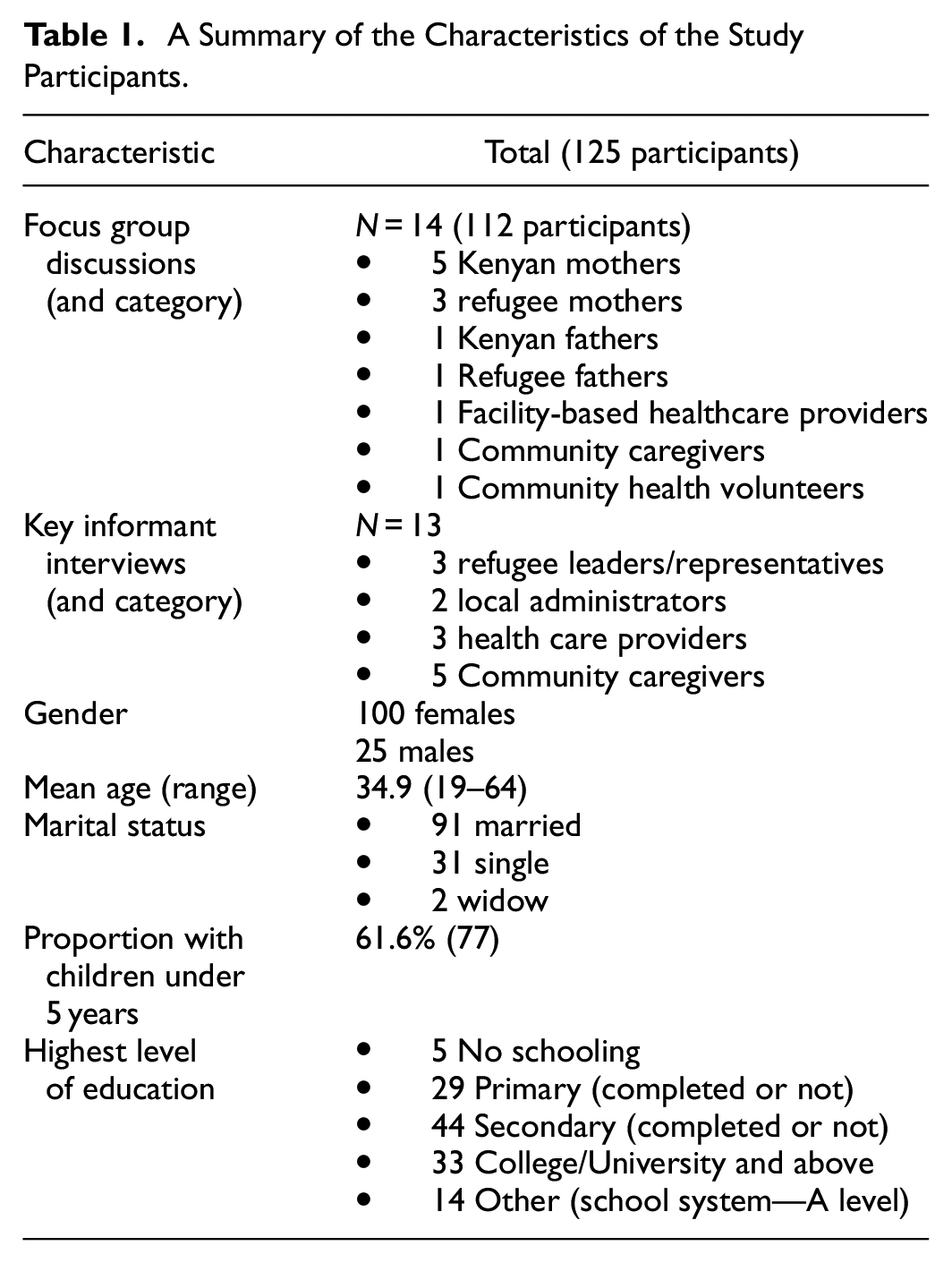
One hundred and twenty-five study participants took part in this qualitative study between August and October 2018 in the informal settlements of the Dagoretti sub-county in Nairobi, Kenya. Participants were purposively recruited through snow-balling sampling. Participants were recruited through purposive sampling approaches, to ensure diversity in respondents by gender, by Kenyan and refugee nationalities, as well as to include a range of caregivers of children below 3 years, local leadership and community representatives, and health professionals. The research team worked closely with the community structures, such as Community Health Volunteers (CHVs) and refugee leaders to provide support with the mobilization of caregivers who met the eligibility criteria. We conducted 14 focus group discussions (FGDs) comprising a total of 112 participants. Five of these FGDs were made up of Kenyan mothers, and three were made up of refugee mothers. An FGD was also conducted for each group of Kenyan fathers, Refugee fathers, facility-based healthcare providers, community caregivers, and community health volunteers. We also conducted 13 key informant interviews (KII) with refugee leaders/representatives, local administrators, and healthcare providers. The diversity of the participants in this study was important for the triangulation of the views shared about ECD program implementation in the community. The majority (80%) of the respondents were females with ages ranging from 19 to 64 years, and about 62% of them had children under 5 years (see Table 1 for details)
A Summary of the Characteristics of the Study Participants.
Qualitative Interviews
A semi-structured FGD and KII guide was developed, and it captured a variety of topics on attitudes, beliefs, and practices in parenting and caregiving for young children. Regarding the focus of this paper, participants were asked about the potential facilitators and barriers to implementing an integrated ECD intervention within their community. In the context of this study, the integrated ECD intervention referred to a community-based ECD program concurrently addressing multiple needs of families and children of native Kenyans and embedded refugees living in urban informal settlements. This integrated ECD intervention would be delivered by community health volunteers supported by the project team in homes and within project centers in the community. Some of the key components of the integrated ECD intervention would include responsive caregiving, paternal involvement, economic empowerment, social cohesion, and mental health. Using a vignette (see Supplemental Material for interview vignette) to make the discussions more interactive and vivid, participants were described to a potential intervention project which could be implemented in their community and would involve organizations and service providers working together with caregivers to help them take better care of their young children. The description involved examples of various aspects of an ideal integrated ECD program, for example, forming caregiver groups, finding a central venue to meet regularly, home visitations by delivery agents, discussion of a set of curricula on a variety of topics like healthy feeding, how to stimulate child development, opportunities for teaching and training a child while young, and how to deal with challenges and parenting stress among many other potential topics. Using a vignette was a useful approach to help standardize the interviewing approach, and counter information bias, which could arise from varying knowledge levels or contextual understanding of what an integrated ECD intervention meant. Both FGDs and KIIs were conducted by trained research assistants in a quiet venue with privacy and were moderated in Kiswahili or English. We utilized open-ended questions followed by further probing to explain their responses. The views documented in this manuscript were spontaneous. To ensure that participants openly shared their views without fear of judgment and without external influences arising from power asymmetries, we ensured that the caregiver groups were gender and immigration status disaggregated. For example Kenyan fathers, Refugee fathers, Kenyan mothers, Refugee fathers. We also ensured that healthcare providers and community health volunteers had their separate FGDs so that views were communicated from a shared level of experience and expectations. To ensure that the research assistants conducted high quality interviews characterized by attentive listening, probing responses, and ascertaining that interviews/discussions had reached a point of data saturation, a senior qualitative researcher randomly attended some FGDs and KII from start to the end. The research team also held a debrief meeting at the end of each day when FGDs or KIIs were conducted so as to discuss what worked well and potential areas of improvement in the data collection procedures. All participants provided written informed consent to participate in this study. We asked for permission from all participants to take notes and audio record the discussions and interviews conducted.
Qualitative Analysis
The audio-recorded interviews and discussions were transcribed verbatim and translated to English. The translated scripts were scrutinized by four authors (AA, CN, VA, and EN). AA and CN developed initial codes from a priori and emergent issues followed by a series of discussions by the research team and consensus reached on developing them into themes and final refinement of thematic descriptions and relationships with guidance from the framework for conceptualizing program sustainability by Shediac-Rizkallah and Bone (1998). VA and EN used the theme-based approach to chart the data, and the developed framework was used as a basis for the interpretation of the results. This approach helped to counter potential bias, which could arise from the individual researcher’s own interpretation of the study findings in ways that may not correctly represent the views of the study participants. Besides, this approach also helped the team to review the credibility, validity, and potential transferability of the findings of this study. NVIVO software was used for coding. A descriptive analysis summarized participants’ demographic characteristics and the perceptions identified during FGDs or key informant interviews.
Results
What Could Lead to the Successful Implementation of an Integrated ECD Intervention?
As summarized below, we categorized participants’ views according to the three broad categories of project design and implementation factors, organizational setting factors, and broader community environment factors (Shediac-Rizkallah & Bone, 1998).
Project Design and Implementation Enabling Factors
Having a Good Community Engagement Strategy
Participants identified various attributes of a good engagement strategy linked to improved implementation of integrated ECD interventions. First, carefully planned mobilization and sensitization activities were discussed as crucial for improving buy-in, especially when caregivers clearly understand what is required of their participation and how they would benefit from the integrated ECD program. Secondly, participants recognized the need for implementers of integrated ECD to establish strong partnerships and ensure that they build on existing structures and resources within the community, for example, the Sub-County Health Management Team, local leadership structures, and community health volunteers (CHVs) workforce. Working closely with the community-level structures was perceived as involving constant dialog (e.g., through meetings) and identifying the roles or support that stakeholders would contribute to the ECD project. Besides, some participants expressed that working with existing community-level structures can reduce the duplication of efforts and resources. Below are some participants’ quotes on good community engagement: …you have to start with a certain group (referring to caregivers). You call them together, and you can even use the local leaders within that area. They know them, and they are able to help with this. The CHVs know them and can also help mobilize the mothers (caregivers). So when they (caregivers) are brought together and explained about the intended program, I think many of them will be willing to join. (KII, community caregiver). ..the most important thing is working with the sub-county team because if you do not, nothing will happen.. so it’s important if you are starting up to identify the role of each stakeholder, maybe during stakeholders’ meetings, then engage them in different aspects (KII, community caregiver). … we already have an organized existing structure according to the Kenya Essential Package for Health, so we have mapped a large percentage of the households, and we know them, and they are attached to a community health volunteer… and you don't need to reinvent the wheel, you just go right ahead and implement it, because that's what we use under the existing structure (KII, Doctor).
Having a Strategic Participant Recruitment Approach
Some participants explained that successful implementation requires proper participant recruitment and sampling processes, such as an initial mapping and piloting exercise to identify the right target group. In addition, some suggested that it is important to have a well-defined project scope which, for instance, initially focuses on one sub-county where a few caregiver groups can be recruited, and then later, this can be scaled up. Still, in connection with participant recruitment, there was some emphasis on the importance of data usage, for example, household social demographic data, with the view that such data can help inform the priority needs, the right beneficiaries to target and how to prioritize resource allocation.
Doing really good groundwork on the target mothers you want to work with. I would personally say narrowing it down. Maybe if it’s Dagoretti, and we have two sub-counties in the north and south… we start with the south and then scale it up if it really works. So you just try it with a few groups of women first and see how it works out (KII, community caregiver). …if we get to know the social demographics of the…households; children under five, households of those with disabilities, households with orphaned and vulnerable children, that would be very helpful because the resources are always limited so we can know how to prioritize as we allocate the resources (KII, Doctor)
Proper Scheduling and Adequate Length for Program Implementation
Some participants suggested that a longer project timeframe can avail opportunities for proper feedback and strengthen the capacity of implementing partners. Others believed that project activities such as training and group sessions need to be scheduled to consider caregivers’ busy schedules so that they are well attended. Their views were that unfavorable scheduling of project activities results in de-motivation and poor attendance of program activities by the beneficiaries.
…also the amount of time. If training takes a lot of days, some (referring to beneficiaries/caregivers) will drop out because of other issues and then what I’m thinking is, training should be from morning to lunchtime then people go home because if you put people there for a whole day, it affects other things because people have other engagements (KII, community caregiver). It will depend on the schedule.., because some do menial jobs of washing to cater to her children’s food or one who will cook mandazi in the morning and will not opt to leave them for the program. But, mostly, it will depend on the time and the place (FGD, Refugee Fathers). …even after five years, they (referring to a certain ECD implementing organization) didn't look like they had done proper household economic strengthening to know who (referring to beneficiary households of the ECD program) should graduate, or who should replace these when they finished. (KII, Kenyan CHV)
Financial Stability
Some participants explained that to ensure the successful implementation of an integrated ECD program, there needs to be sufficient funding, which can also be enhanced by exploring alternative funding possibilities, training caregivers on entrepreneurship, coupled with proper financial management mechanisms. Setting up a community savings scheme to meet the financial and other needs of the caregivers was identified as one of the ways to enhance the sustainability of an integrated ECD program.
Maybe you form a group of mothers. Then you support them financially as they make savings within the group so that the money they can save doesn't all get lost because sustainability is the problem. So helping these mothers to save money is what will help that program. (KII, Community nurse).
Organization Setting Enabling Factors
The Involvement of a Transparent Workforce and ECD Champions/Program Advocates
There was an emphasis by the participants on the importance of involving transparent and accountable individuals in project implementation. Notably, participants’ views on the need for transparency were limited to the ECD workforce, and the transparency of an implementing institution as a whole was considered important. It was discussed that an ECD implementing institution/organization should demonstrate that the ECD program is committed to providing the needed parenting skills and supporting beneficiaries in most need. Also, beyond the need to engage various relevant local stakeholders for buy-in purposes, participants pointed out the important role of having individuals who can champion and advocate for ECD, motivate the ECD workforce, and interest the community members about the value of ECD. Motivational trainers and facilitators, influential leaders (e.g., local administrators such as the Chief), and some renowned in the community were identified as potential ECD champions who can boost the acceptability and smooth implementation of an integrated ECD intervention.
And those with that project should have an aim, meaning they should do as they had planned and should not have greedy people. that's why when you start something you should put measures so that when someone goes against them, the law follows them and there should be transparency (KII, Refuge community assistant). …through our offices and those CHVs I told you, they will move around and sensitize them (the caregivers) through barazas [community meetings]. So, you know, Kenyans know that whatever the Chief says is right, and they also feel safe (KII, Chief).
Capacity Building and Training
These aspects were described as important factors for the success of integrated ECD project implementation. Some participants discussed that it is important to embed learning activities that involve practical lessons and incorporate useful skills. Entrepreneurship, nutrition, family planning, stress management, hygiene, life skills, parenting, and caregiving skills were the topics that participants considered suitable for an integrated ECD project implemented within their setting. Such knowledge and skills were viewed as important components for empowering caregivers to improve their incomes and livelihoods. There was also discussion about the value of building the capacity of program staff, especially in communication and ECD project implementation skills. Furthermore, as part of capacity building and training, some participants emphasized the vital role of follow-up and review meetings to reinforce the key messages learned during the ECD training.
The program will be useful if people are educated on nutrition and stress management (KII, Refuge community assistant). The program will bring parents together, where they will be educated on parenting skills and economic empowerment (KII, Refugee leader). It will be important since it will be a group session where life skills will be taught (FGD, Refugee mothers). … if an organization like yours doesn't follow up on what you have taught us, I will go and relax, and the others too will relax. So everyone will forget what we have been taught. There must be monthly follow up and review meetings during which we come and sit, and we ask each other where the challenge was and what we can do to succeed (FGD, Kenyan mothers)
Broader Community Environment Enabling Factors
The Extent to Which the Proposed Intervention Is Tailored to the Realities and Socio-Cultural Conditions Within the Community
Some participants emphasized that the ECD intervention or program should meaningfully reach and benefit the vulnerable groups, such as the young mothers, single mothers, and the extremely impoverished caregivers within the community. It was also discussed that an ECD program should be responsive to caregivers’ complaints and concerns. Poverty was one of the cited realities. Some participants proposed that the integrated ECD program should incorporate entrepreneurship training or provide start-up capital to caregivers. Other participants believed that a positive image of the program results from how responsive it is to the community needs and issues and that it is the program’s positive image that attracts more support and commitment from primary beneficiaries and stakeholders.
The perception the program is committed to supporting vulnerable groups and providing parenting skills… will be important because it will help to support the vulnerable groups within the community (FGD, Kenyan mothers). …there are times when the participants fail to participate, so they should be motivated to become serious with it. Motivation like money or food (KII, Refugee)
What Could Hinder the Successful Implementation of an Integrated ECD Intervention?
We asked participants about the perceived barriers to successfully implementing an integrated ECD intervention in their community. Their views comprised mostly organizational setting and project design/implementation factors, and to a lesser extent, the broader community factors. Participants’ quotes on these issues are also included in the section below.
Project Design and Implementation Related Barriers and Their Solutions
Inadequate Mobilization and Engagement of Target Beneficiaries and Local Stakeholders
Some participants explained that the failure to involve and consult with stakeholders during program inception could negatively affect their support and commitment to the program. Besides, there were views that without adequate mobilization and engagement, community members may develop some misconception about the aims of the integrated ECD program, and some could end up with a feeling of being exploited.
Sometimes the people from the community think that they are being used for the gain of the organization, so the aim of the program should be explained well (FGD, health workers). The potential challenges may be there if the stakeholders are not appropriately involved from the very beginning (of the program), but if we involve all stakeholders, I see it succeeding (KII, Doctor)
The Lack of a Clear Program Exit Plan
Some of the participants expressed the concern that community members may be left unprepared and vulnerable after completing an ECD intervention, majorly because there wasn’t a clear exit strategy in place.
…so there has to be a clear sustainability plan so that after the exit of this program, the communities are not just left hanging. All that can be done through preparedness, prior preparation, involvement of all the stakeholders. I believe this should motivate them and alleviate the challenges (KII, Doctor)
Organization Setting Related Barriers and Their Solutions
Lack of Transparency and Unethical Practice by ECD Workforce
Participants cited various forms of injustices and unethical actions that ECD program staff may practice. These included favoritism and tribalism, leading to the lack of fairness in enrolling people into programs. In addition, some cited the practices of misappropriation of resources and corruption, especially during the distribution of project incentives and supplies to beneficiaries.
…because you can plan a project, but amongst you, some have bad motives, …there are people in the project that will take the money and make it theirs so that the program will collapse… (KII, Refuge community assistant). .. challenges include corruption, for example, in the case of good nutrition (referring to nutrition supplements). You’ll find some will avail themselves and find that it’s over. Like what the other participant has said, the facilitators of that program should deal one-on-one with the people they want to help. Otherwise, if they engage a middle person, it will be a problem (FGD, Kenyan mothers)
Poor Communication Skills
Some participants believed that sometimes, project facilitators or trainers have a poor attitude and express rudeness toward program beneficiaries which can discourage full participation and compliance to the ECD intervention program. Some other participants explained that using poor communication skills by ECD program staff could result in misconceptions and evoke unrealistic expectations such as the expectation of sitting allowances or financial assistance by program beneficiaries.
The attitude of those teaching us also varies. You can find someone who has a (bad) attitude… an attitude like that can make the project fails …next time, you won't go to those people (refers to participants not attending sessions by trainers with a bad attitude) because they're not good (FGD, Kenyan mothers)
Poor Compensation/Remuneration of the ECD Workforce
There were views expressed by some of the participants, suggesting that ECD workforce, mostly the CHVs who often serve as delivery agents, are usually poorly facilitated and compensated for their service. Indeed, some pointed out that these delivery agents sometimes work voluntarily. They explained that poor compensation could lead to the delivery agents’ loss of motivation and interest in program implementation.
The community health volunteers are volunteers, so if they’re not facilitated, that may be the challenge because currently, the government is not facilitating them. So, they need to be facilitated because if they are not, you will find that they cannot sustain voluntarism. So, they will seek other income-generating activities (KII, Doctor).
Broader Community-Related Barriers and Their Solutions
Behavioral Change Reluctance and Resistance
Some participants shared that sometimes certain program beneficiaries can resist practicing what they are taught during the intervention program, while others can refuse to disseminate the key messages/skills on ECD to the other caregivers or peers in their communities. Besides, some pointed out that program beneficiaries can use the materials provided by the intervention (e.g., nutritional supplements, equipment for income-generating activities) for other purposes or sell them instead of using them to benefit ECD within their households. Others generally expressed the concern that it is difficult to secure community members’ dedicated interest and participation in program activities in their community. The participants explained that if beneficiaries fail to take the messages seriously or refuse to adhere to the behavioral change messages of the ECD program, the delivery agents (e.g., CHVs) can lose motivation to conduct follow-up visits to their homes.
Some will tend to take the project supplies (materials) and sell them outside, and for some, instead of giving them to the children, they will resort to eating them themselves. Some will even …sell it at their pleasure, and yet it has been written ‘not for sal’, (FGD, Kenyan mothers) so the challenge is maybe the CHV goes to the caregiver’s home and misses him at times, the caregiver does not take the information seriously (FGD, Kenyan mothers)
Unrealistic Expectations by Beneficiaries
Some of the participants explained that the unrealistic expectation by beneficiaries about receiving hand-outs and financial allowances or assistance could negatively impact their motivation and long-term commitment to the program. In addition, some participants felt that unrealistic expectations could result from unclear communication from the program staff.
So if you tell them there is a training and you don’t give them money, they feel like they better go and look for food for their children. So when they hear of an NGO (i.e., non-governmental organization), they always see money (KII, Chief). ..another problem I have seen with many (community members) is tokenism. Some (community members) will attempt to get the allowance and will not care the moment you stop giving them the token. They will run away (KII, Ward representative).
Socio-Economic Hardships
Some participants identified socio-economic hardships among some of the important barriers which can impact participation in an integrated ECD intervention. Among the socio-economic hardships discussed were the incurrence of transport expenses partly due to long distances involved in accessing venues for project activities and household poverty which can result in the prioritization of other activities which cater for basic needs than taking part in the ECD program activities. It was also recognized that security concerns, especially thefts, can be a major threat for ECD program-related income-generating activities (e.g., poultry and tailoring machinery). The language barrier was also identified as a potential hindrance to the full participation of some beneficiaries.
To set up the income-generating activities……. If it's a place where there's theft, and you start keeping poultry, they get stolen, so they will need a good place, secure obviously. If it's sewing machines you've bought for them, they should keep them at a good secure place (KII, community caregiver) Like me, I've come from far, not from around these areas, and yet I want to participate and attend those teachings (FGD, Refugee mothers) Not attending and delays in session where mothers prioritize searching for food or do domestic chores, and at times a child may be sick - so will have to go the hospital first (KII, Refugee leader).
Gender and Power Asymmetries
Some participants discussed a variety of gender and power asymmetries, characterized by restriction of female caregivers’ participation in ECD project activities by their male spouses, favoritism, and tribalism were discussed.
Everything that is new is resisted before it takes off, you may have problems with the men allowing their women to go to such group meetings, but I think the women are willing to learn (KII, community caregiver)
Discussion
Our study highlights that the perceived enablers and barriers for integrated ECD program implementation in an urban informal settlement aligned with factors conceptualized in Shediac-Rizkallah and Bone’s (1998) framework. Participants mostly discussed: strategic engagement, participant recruitment, scheduling of activities, and adequacy of the program duration and program exit strategy (as project design and implementation factors); involvement of transparent ECD workforce and champions, capacity building, accountability and transparency, compensation of ECD workforce, communication skills (as organization setting factors); and the need to tailor ECD program to local contextual realities, behavioral change reluctance/resistance, unrealistic expectations among beneficiaries, socio-economic hardships, gender, and power asymmetries (as broader community factors).
The findings of this study demonstrate that local stakeholders and community members are knowledgeable and resourceful, thus capable of supporting or working with implementers to identify and recommend feasible solutions to the challenges which may impact the effectiveness of integrated ECD interventions. This finding further emphasizes the importance of increasing community engagement, for example, through careful mobilization, consultation with, increased involvement, collaborating, and sharing leadership with local stakeholders and community members throughout the entire cycle of ECD programs. This helps to align the goals of the ECD program to the needs and priorities of the community, which lessens unrealistic expectations, boosts buy-in, and community ownership (Kabue et al., 2022; Wallerstein et al., 2015). Indeed community engagement is critical for health programs, and research from LMICs shows its positive impact on behavior change and cost-effective sustained transformation in health outcomes and wellbeing (Farnsworth et al., 2014). The process of community engagement for ECD programs in urban informal settlements, however, remains insufficiently documented within the literature and is an important area for future research.
In our study, the quality and attributes of the ECD workforce were extensively discussed as important determinants of the success of integrated ECD program implementation. First, careful selection, adequate capacity building in the areas of communication, interpersonal skills and program implementation, good reputation, and transparency (e.g., ECD champions) were recognized as important attributes for a good quality workforce. These factors, coupled with good compensation, were perceived as important drivers for staff motivation and commitment to championing integrated ECD program goals. Our findings are in line with the research on scaling ECD programs in four countries, which also identified the issues of capacity development, motivation, and fair compensation of the ECD workforce as being essential for achieving quality and sustainability of ECD programs (Pérez-Escamilla et al., 2018). In many discussions with participants in this study, CHVs were identified as suitable ECD champions and program delivery agents. Indeed, the role of CHVs in addressing the critical shortage of health workforce, in building trust and bridging the gap between healthcare professionals and the local community has been well recognized within the Kenyan context (Muia et al., 2019; Rachlis et al., 2016). However, as discussed by participants in our study, more efforts in fairly compensating CHVs and adequately building their capacity has been further emphasized in various research findings within the Kenyan setting (Aseyo et al., 2018; Muia et al., 2019).
The need to tailor ECD interventions to the contextual realities of dwellers in urban informal settlements in ways that tackle social determinants of health and improve resilience is an important lesson from our participants’ views. First, integrated ECD programs need to be targeted equitably so that groups in most need, including those at risk of exclusion, are well reached with resources and fully involved in all program aspects. Moreover, these views also indicate that it is important to have deliberate measures in place to combat injustices like tribalism, favoritism, corruption. These measures, for example, include having accountability structures within an ECD program, having a set of organizational values in place, vetting of program delivery agents, using clear communication in understandable language coupled with open feedback loops. The importance for ECD programs to integrate skills’ building and activities aimed at improving income generation among beneficiaries to lessen poverty and over-reliance on the ECD program were highlighted by participants in our present study. Some views also indicated that resilience among beneficiaries could be improved through timely collaborative planning for the ECD program exit strategy so as to improvise strategies for beneficiaries to sustain positive change following program closure. In general, these findings highlight the need for equity-focused-implementation in ECD programing. On a positive note, there is a growing body of research on actions and frameworks to guide decision-makers and researchers on how to ensure that program planning, design, implementation, and evaluation processes are more equitable (Eslava-Schmalbach et al., 2019; McNulty et al., 2019).
Our study highlights the importance of applying a gender-lens in ECD program implementation to identify opportunities for improving women’s autonomy and full participation in ECD programs. Furthermore, there is a need for these programs to involve the broader family besides only primary female caregivers. The participants’ views may also indicate that existing differences in gender roles and norms, coupled with a scarcity of resources, are linked to the dilemma of competing responsibilities and pressing priorities (domestic chores, taking care of sick children, and extensive hours at menial work) among caregivers in urban informal settlements. This, in some ways, impacts the choice of targeted beneficiaries (e.g., female caregivers and siblings), their availability as well level of participation in ECD programs. Therefore, ECD program activities (this includes their venues, number of sessions, a dose of delivery, and duration of the activities) should be planned reasonably and in full consultation with the community members to understand pathways for strengthening rights-based and gender-responsive ECD programing. The need to apply gender-lens in research, intervention and policies on child health and ECD is growingly underscored (Muraya et al., 2021; Staab, 2019).
Strengths and Limitations
Overall, this study’s strengths include the use of a diverse mix of participants from an urban informal settlement, in Kenya’s capital city, including caregivers, healthcare providers, refugee leaders, and local administrators. We believe that this diversity of study participants enriched the dialog by capturing views from people in positions of power and decision-making, as well as residents with varied socio-cultural, gender, and lived experiences. However, some of the views from this study may not be generalizable to other urban informal settlements with different living conditions and dynamics. In our study setting, refugees were embedded and lived in the same community with Kenyans. Research however indicates that refugees who dwell in Kenya’s urban settings often experience significant hardships including language barrier, lack of legal documentation, and disproportionately poorer access to employment, social, and healthcare services (Abubakar et al., 2019; Fotso et al., 2008). Plausibly, some of the identified factors that influenced implementation of ECD programs in our setting may arise from unique structural inequalities experienced by embedded refugees, and yet some of these factors may not fully represent the realities of other urban informal settlements without or with very small refugee sub-populations. Besides, our study was conducted during the COVID-19 pre-pandemic era and it is likely that current experiences may differ due to additional challenges arising due to COVID-19. The potential weakness from this is that our participants’ views may not have readily captured various issues relating to workforce, financial and physical resources availability/access, and caregiver factors which were uniquely exacerbated by the pandemic and yet such factors could presently influence successful implementation of integrated ECD interventions within their communities. At the backdrop of our analysis and results interpretation, we recognize that much as sustainability is often included as a sub-concept under the broader concept of implementation, the factors that influence successful implementation are not necessarily always the same factors that would enable continued implementation into longer-term sustainability (Scheirer, 2013). Also, data collection, analysis, and interpretation in qualitative research are subject to individual influence. However, we countered this by maintaining reflexivity and having contributions from a diverse research team throughout this research. Besides, we used the framework for conceptualizing program sustainability by Shediac-Rizkallah and Bone (1998) so as to guide in the in our interpretation of the views shared by our diverse study participants, and this may have helped minimize potential biases in the analysis process.
Future Directions
The views of participants from the present study on enablers and barriers to implementation of an integrated ECD intervention in an informal urban settlement highlight the invaluable role of meaningful mobilization and community engagement, workforce capacity development and fair compensation, the need for equity-focused implementation approach in addressing contextual realities in these settings, and the need to apply a gender-lens in ECD programing. Based on participants’ views, we propose the following suggestions for improving integrated ECD programs. Right from outset throughout the entire project cycle of integrated ECD programs, there must be thorough stakeholder and community engagement. This is likely to improve co-design, resource mobilization, and local ownership of integrated ECD programs. Secondly, motivation and commitment of ECD workforce is valuable for successful implementation of integrated ECD programs. Therefore, governments and institutions implementing ECD need to devise deliberate measures toward improving compensation and remuneration, accountability and transparency, wellbeing of the workforce, and open communication across all levels within integrated ECD workforce. Thirdly, during the design, monitoring, and evaluation of integrated ECD interventions there is need to carefully conduct thorough needs assessments and to integrate co-design approaches so as to ensure that contextually relevant needs which span beyond child-rearing, as well as potential barriers to program success are equitably addressed within the integrated ECD programs in a culturally appropriate manner. Lastly, empowerment of the local community to proactively take control of their own and their families’ wellbeing is a paramount end goal of integrated ECD interventions. This points to a need for continued capacity and leadership building, as well as gender-sensitive approaches to empowerment local communities in order to sustain the long-term impacts of integrated ECD programs.
The validity and reliability of our study are impacted by various study limitations noted in the earlier sections, including its being conducted in the pre-pandemic period, the unique characteristics of our study setting (e.g., an embedded refugee population) and potential researcher bias or influence in the interpretation of the findings. Future research is needed to explore how the variation in project design, organizational, and broader community factors influence the efficacy of ECD interventions in an urban informal setting, as this is currently among the existing gaps in ECD research (Zhang et al., 2021). Future studies, preferably involving a mixed-methods approach, larger samples, and conducted in varied geographic settings during the COVID-19 pandemic, as well as the post-pandemic era is needed to explore in more depth the factors which influence the success of integrated ECD interventions in urban informal settlements. So as to improve the reliability and validity of the qualitative findings, future studies should integrate research methods, by applying both qualitative and quantitative approaches to allow for triangulation of findings bit also maximize on the methodological strengths of these approaches. It may also be important to integrate research methods which can rate consensus and priority of the study findings among the study participants, for example through applying nominal group techniques (McMillan et al., 2014). Furthermore, future researchers should aim toward translating their findings on factors influencing the implementation of ECD programs into a set of robust process and outcome indicators, which can enhance smoother monitoring, evaluation, and learning processes in integrated ECD program implementation.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440231208986 – Supplemental material for Stakeholders’ Perspectives of Enablers and Barriers to Successfully Implementing an Integrated Early Childhood Development Program in an Informal Urban Settlement in Kenya
Supplemental material, sj-docx-1-sgo-10.1177_21582440231208986 for Stakeholders’ Perspectives of Enablers and Barriers to Successfully Implementing an Integrated Early Childhood Development Program in an Informal Urban Settlement in Kenya by Derrick Ssewanyana, Marie-Claude Martin, Vibian Angwenyi, Margaret Kabue, Kerrie Proulx, Linlin Zhang, Tina Malti, Eunice Njoroge, Carophine Nasambu, Joyce Marangu, Rachel Odhiambo, Eunice Ombech, Mercy Moraa Mokaya, Emmanuel Kepha Obulemire, Greg Moran, Stephen Lye, Kofi Marfo and Amina Abubakar in SAGE Open
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the International Development Research Centre (IDRC) and Aga Khan Foundation Canada (AKFC) through the project on Improving Early Childhood Development and Well-Being in Refugee and Other Marginalized Communities (Center File: 108506-002). The funding bodies did not play any role in the in the design of the study and collection, analysis, and interpretation of data and in writing this manuscript.
Ethical Approval and Consent to Participate
This study was granted ethics approval by the Aga Khan University Institutional Review Board—Ref: 2017/REC-93(v1) and a research permit was granted by National Commission for Science, Technology & Innovation (NACOSTI), and Ref: NACISTI/P/19/50782/31710.
Data Availability
Data from this qualitative study may be shared upon request to the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.