
Abstract
A descriptive qualitative study among 12 religious leaders and 10 members from seven different religions using in-depth interviews was conducted to explore the factors that influence HIV testing among religious people in the area of Traditional Authority Chitukula, Lilongwe district. Participants and sites were purposively selected and all interviews were recorded using a digital recorder, then transcribed and translated into English. Data were analyzed using a thematic approach. The study showed that prayer has a prominent role in the management of HIV and AIDS. The barriers to HIV testing include a belief in faith healing, the rules of a specific church, and a perception of a low risk of HIV infection among religious people. Interventions that could promote HIV testing include the implementation of HIV self-testing, mobile and or door-to-door HIV services, church-based HIV testing services, and facility-based services that are integrated with other services to preserve privacy. Religious platforms can be leveraged in the delivery of HIV testing services. The promotion of religious-based prevention interventions needs to consider the foundations and beliefs of each religion and be able to contextualize the methods which can be achieved by continuous dialogue and support from religious leaders.
Introduction
Globally 37.7 million people were living with HIV and AIDS in 2020 and 66% of these resided in sub-Saharan Africa (UNAIDS, 2021). Of the people that were HIV infected 84% knew their status which was below the global target of 90% at the time (UNAIDS, 2021). The prevalence of HIV in Malawi was at 10.6% while in Lilongwe where the study was conducted, the prevalence was 11.5% (Ministry of Health, Malawi, 2018). Malawi has registered progress in the number of people that know their HIV status which is at 90.9% among those that are HIV infected (Ministry of Health, Malawi, 2022). Although there has been an increase in the HIV testing rates, they fall short of the current target of having 95% of people that are HIV infected knowing their status. Malawi adopted differentiated ways of implementing HIV testing to close the gaps in the targets (Ministry of Health, Malawi, 2014). These strategies include active index testing and assisted HIV self-testing using community-based cadres (Ministry of Health, Malawi, 2014). In the 2020 to 2025 HIV testing policy, Malawi aims at rolling out differentiated HIV services among men, children, female sex workers, and their clients, men who have sex with men, refugees, migrant laborers, prisoners, students of higher education institutions, and colleges, and people in uniform (Ministry of Health, Malawi, 2020). Faith-based organizations (FBOs) are recognized as partners in the provision of HIV services (Berkley-Patton, Moore, et al., 2013; Berkley-Patton et al., 2019; Derose et al., 2011; Jobson et al., 2019; Nunn et al., 2013; Pichon & Powell, 2015). FBOs are highly accessible, cover a wider population, and can support fragile public health systems (Ochillo et al., 2017; Rakotoniana et al., 2014). FBOs conduct HIV-related activities (Derose et al., 2011; Rakotoniana et al., 2014; Stewart et al., 2016) and also care for HIV-infected people, promote HIV awareness, and encourage HIV testing (Derose et al., 2011). FBOs embed HIV activities within their health activities or run parallel programs that overlap with other services (Palar et al., 2013). Furthermore, FBOs have jurisdiction over issues of personal behavior, morality, family life, and beliefs through their direct contact with people at various milestones in life (Lesolang, 2014) which remain critical to HIV services. Moreover, FBOs are advantageously positioned to tackle the HIV and AIDS pandemic because they have permanent structures present at the grassroots level in most communities. Agate et al. (2005) argued that the provision of HIV screening services within a church would be effective since most congregants attend church weekly (Agate et al., 2005). This was later confirmed in studies conducted in South Africa and the USA where older men and people were reached with HIV testing respectively through a church platform (Jobson et al., 2019; Kuofie et al., 2019).
The breadth and scope of HIV services offered by FBOs vary with other organizations offering HIV testing on their premises while others find it more feasible to work with testing agencies as opposed to being a certified testing site (Pichon & Powell, 2015). The support from faith leaders optimizes the uptake of HIV services (Lindgren et al., 2013; Mendel et al., 2015; Rankin et al., 2016; Ransome et al., 2018). After all, they are trusted and remain culturally appropriate venues because they have health services as part of their goals in society (Stewart et al., 2018). In Malawi, 77% of the population are Christians while 15% are Muslims, and the remaining 8% practice traditional African religions one of which is the Aaron group. The other African religions practiced include Bimbi, Napusenapuse, Chipangano Church, Church Cha Makolo, and African Abraham. However, there are no statistics that indicate the proportion of people that belong to the Aaron religion because of its discrete nature (Kuofie et al., 2019; National Statistical Office, 2015; Trinitapoli, 2011). The dominance of religious affiliation in Malawi makes FBOs key stakeholders in the HIV and AIDS response. (Kuofie et al., 2019; National Statistical Office, 2015; Trinitapoli, 2011). Thus, religious groupings are key partners in the fight against HIV and AIDS because they provide HIV services amongst other health programs. The Malawi Government is keen to work with various faith-based organizations to accelerate the uptake of HIV prevention strategies by using faith-based platforms as a delivery point, handling issues on faith-based healing, support of adherence to ART among congregants, and training Faith Leaders in HIV and AIDS emerging issues (Ministry of Health, Malawi, 2014). The religious fraternity has been key in the response to HIV and AIDS in Malawi and they operate under the umbrella of the Malawi Interfaith AIDS Association (Ministry of Health, Malawi, 2014). Although FBOs are involved in HIV testing activities their major constraint is financing to manage and run the programs since they are heavily Government or donor-dependent (Ministry of Health, Malawi, 2014). Additionally, religious leaders in Malawi are regarded as community leaders or opinion shapers who influence the uptake of services (Rankin et al., 2016). Arguably, a religious leader’s knowledge of HIV services influences church members’ behavior (Lindgren et al., 2013). Notably, FBOs remain key in the provision of HIV testing services and could be leveraged to provide more support.
With the adoption of the UNAIDS 95-95-95 goals, there is a need to expand the avenues for HIV testing by exploring religious institutions’ roles (UNAIDS, 2014). The suboptimal HIV testing rate impedes the attainment of the UNAIDS goal of 95:95:95 because the last two 95s are dependent on the first 95 which focuses on knowing one’s HIV serostatus which can only be achieved through HIV testing (UNAIDS, 2014). Countries are encouraged to scale up testing programs to achieve the target of at least 95% of the diagnosis of people living with HIV by 2030 (Phillips et al., 2019). Although Malawi had made substantial progress in reaching the UNAIDS 90-90-90 goals, only 76.8% of the population were aware of their HIV status which was below the target set at the time we conceptualized Malawi the study (Ministry of Health, Malawi, 2018). During this time, it was noted that 39.6% of men and 25.7% of women were not aware of their HIV status. All this was happening at the time when the National HIV and AIDS prevention strategy for Malawi advocated for voluntary HTC and the creation of demand for HTC (NAC 2015–2020). Realizing the gap that was there in reaching the target of HIV testing, this study explored the factors that influence HIV testing among religious people in the area of Traditional Authority (T/A) Chitukula, Lilongwe district. Specifically, this study asked the following question: What are the factors that influence HIV testing among religious people in T/A Chitukula, Lilongwe district? This information will reinforce FBOs’ support for HIV and AIDS services. The information from this study will inform the local authorities in Lilongwe and beyond on the roles and ways of strengthening religious institutions as platforms for offering HIV services.
Methods
Study Design
A descriptive qualitative cross-sectional study was conducted to gather information on the factors that influence HIV testing among religious people in the central region of Malawi. The design enhanced the understanding of experiences of religious people toward HIV testing, the unique manners by which they encounter HIV testing services, and the variation in their HIV testing experience and perceptions (Jobin & Turale, 2019; Kim et al., 2017). This method was deemed appropriate because it allowed the gathering of information through the immersion of the researcher in the world in which these phenomena are taking place (Kelly et al., 2019; Kim et al., 2017).
Study Setting
The study site was in Lilongwe district in the area of T/A Chitukula. The city of Lilongwe is in the Central Region and is the capital of Malawi. The Lilongwe district has 18 T/As and T/A Chitukula is located in the northeast of Lilongwe with both urban and rural sections. The study was conducted in TA Chitukula because it offers a variety of urban and rural perspectives including multiple religious’ groupings. There are three prominent religious groups in TA Chitukula: Christian, Islam, and traditional religion. Among Christian denominations, there are Catholics and Protestants. There are 68 Christian denominations and 2 Islamic groups Quadria and Sukuti. Lilongwe district also has a traditional African religious grouping known as Aaron. The study was conducted among the following religious groups Roman Catholic Church, Church of Central African Presbyterian (CCAP), Assemblies of God, Apostolic, Jehovah’s Witness, Islam, and Aaron (Gule wamkulu). Roman Catholic and Church of Central African Presbyterian (CCAP) are among the denominations that offer 43% of health services in Malawi including HIV and AIDS services.
Sample Size
Participants were drawn purposively (Palinkas et.al., 2015) from six prominent religions of Roman Catholic, CCAP, Assemblies of God, Jehovah’s Witness, Apostolic faith church, Islam, and the traditional Aaron religion. A total of 22 religious people were recruited comprising 12 leaders (two from each of the six religions) and 10 members. Twenty-five participants were deemed enough to have rich data and at the same time solicit views from both leaders as well as members (Guest et al., 2006). In the end, only 22 interviews were conducted because the remaining three were not available at the agreed times. Roman Catholic, CCAP, Assemblies of God, and Islam were chosen because of their large followings. The Apostolic Faith and Jehovah’s Witness were chosen due to the perceived health beliefs of the two religions as they restrict their members from accessing health services. The Aaron group was chosen because of its widespread practice in T/A Chitukula and its stand on HIV testing was not known. However, there are no statistics that indicate the proportion of people that belong to this religion.
Sampling
Participants were sampled following a purposive approach and they were selected from the six denominations to reflect variations in terms of views from men and women (Palinkas et al., 2015). The two leaders from Aaron were selected using snowball sampling because it is a closed religion (Browne, 2005). In this study, a closed religion was defined as one that is practiced in secret, with services being conducted at the graveyard. The clerk to the T/A helped to identify the first Aaron leader known as “Wakunjira” (a name given to Aaron religious leaders) because this religion is closely linked to Chewa culture. The places of worship were the entry point to recruit participants. Religious leaders were first consulted and briefed about the study during worship days. Permission was then given and thereafter, participants were selected. Also, a purposive sample of 10 congregates, 2 from Roman Catholic, 2 from CCAP, 2 from Islam, 2 from Assemblies, 1 from Jehovah’s Witness, and 1 from Apostolic were recruited for IDIs. This was done to ensure that the views of congregates are taken on board.
Data Collection
All current leaders, whether male or female, and followers of the above-mentioned religions were eligible for the study. These leaders were interviewed as representatives of their religions to explore their views, beliefs, and experiences about factors that may enhance or hinder HIV testing. The data collection tool was piloted with two people, one from Living Waters and the other one from Anglican churches, and corrections were made before the commencement of the actual data collection. Findings from the pilot study were not used in the research, but only guided the perfection of the data collection tool. The data collection tool was also reviewed and verified for its content by the research supervisor ALNM who is a qualitative research expert. Data were collected from June to August 2017 using a pretested semi-structured in-depth interview guide which was developed based on the study objectives. The semi-structured in-depth interview guide was translated into Chichewa by a bilingual individual fluent in both Chichewa and English and back-translated by another person into English. The Principal Investigator checked if the documents gave the intended information.
All the interviews were face-to-face and conducted by the Principal Investigator and two well-trained research assistants. The research assistants were trained on the informed consent form, research ethics, logistics, the in-depth interview guide (probing techniques and taking field notes), and verbatim transcription of data. They assisted in the identification of participants, arranging interview time, and place for the interviews. The interview guide contained open-ended questions and probes which were used to facilitate the IDI.
The principal investigator is a Public Health Specialist and she is well trained in research methods which included qualitative and quantitative approaches, and data analysis as part of her Master of Public Health training courses. She introduced herself to the religious leaders and congregates as a researcher studying toward a Master of Public Health degree d and covered the purpose of the study as well. She assured the participants that their refusal to participate in the study will not have any negative consequences on their standing in their church in any way such as being prohibited from practicing their religion or ex-communication from their respective religions. One of the research assistants holds a Bachelor of Public Health degree and the other one holds a Bachelor’s degree in Education Sciences. The researchers had similar religious backgrounds with some of the study participants and completely different religious beliefs from others in the study area, so they remained neutral by avoiding asking biased questions during data collection and only reflected on what emerged from the data without adding their views during data processing and analysis. Broadly, some of the questions which guided the interviews were as follows:
Explain to me in detail the role of prayer in the management of HIV and AIDS.
What do you think are the opportunities and challenges of addressing HIV and AIDS in a faith-based context?
What do you think are the religious factors that encourage people to go for HIV testing?
What do you think are the religious factors that discourage people to go for HIV testing?
Information on personal factors that stimulate the faith community to seek HIV testing, religious beliefs that are associated with HIV testing, knowledge of HIV and AIDS, and how faith leaders deliver HIV and AIDS services to the congregates was collected. All data were digitally recorded and researchers compiled field notes as well. The initial contact with the potential study participants was at their place of worship during designated service days. However, participants were allowed to choose a place and time convenient to them where they could be interviewed. Most of the participants chose their homes as a place for the interviews. The interviews were conducted in a private room where only a participant and an interviewer were present. Data were kept in a secure computer with a password known to the research team only and the field notes were kept in a lockable cabinet.
To maximize the integrity of our findings the researchers reflected on their perspectives regarding religion and HIV And AIDS to avoid influencing both the data collection and interpretation (Jennings, 2012). All key findings were summarized at the end of each interview as a form of member checking to enhance the credibility of the findings and dependability was achieved through multiple discussions amongst the researchers while the description of the context where the study was done maximized the transferability of the findings to similar settings (Leung, 2015). Interviews ranged from 30 to 40 minutes.
Data Analysis
All data were transcribed verbatim by the research team. The transcripts were then translated into English by two transcribers. Each transcript was audited by the PI against the original audiotape. There was a systematic quality check of the transcripts whereby every 7th minute and 20th minute of the transcripts were checked against the audio. The auditing served as a quality control measure of the transcription and translation. Data were inductively and deductively coded from the data and objectives and literature respectively and analyzed using thematic analysis (Braun & Clarke, 2006). The data were analyzed manually; transcripts were read and reread numerous times by the researchers. The use of multi-disciplinary team members improved the reliability of the codes as they were discussed before being used and any areas of discrepancies were discussed for resolution (Burla et al., 2008). A thematic analysis approach was applied as follows: We familiarized ourselves with the data by repeatedly reading the transcripts and listening to the recordings and this was followed by the generation of initial codes. The analysis team members compared their understandings of contents in terms of major themes, points of agreement, and areas where there was disagreement. Codes were then sorted into potential themes by considering how different codes may combine to form a theme or how they fit under an overarching theme. We reviewed and refined the themes and that resulted in other themes being collapsed into each other because there was not enough data to support them, others broken down into separate themes, and others created as they were some codes that did not belong to any theme. The themes were defined and refined and were examined for differences and similarities. The refined themes were verified against the audio data. We achieved inter-coder reliability by comparing codes iteratively amongst researchers and discussing areas of discrepancies to consensus (Burla et al., 2008).
Results
Demographic Characteristics of Religious Leaders
Of the 12 leaders that were interviewed, only 1 was female. Their age ranged from 23 to 84 years and two had no education. Only one was catholic and was not married (Table 1)
Demographic Characteristics of Leaders.

Demographic Characteristics of Followers
Of the 10 followers that were interviewed, 4 were not married, 3 were males and their ages ranged from 18 to 67 years, and only 2 were not educated (Table 2).
Demographic Characteristics of Followers.

The results from the interviews are presented in three main themes and these include (a) Role of religion in HIV Testing and Counseling, (b) Religious related barriers to HIV testing and counseling, and (c) Interventions for promotion of HIV testing among religious people
Role of Religion in HIV Testing and Counseling
Most participants stated that the role of religion in HIV counseling and testing is to encourage their followers on taking the test and to teach people the benefits of it. The knowledge of HIV testing helps the followers to make informed decisions about having a test. Religious leaders in the study viewed their institutions as platforms where information may be passed to congregants.
The role of religion is to encourage believers to go for HIV testing. They should not deceive themselves because they are believers, church elders, or pastors, they cannot contact HIV. It is everyone’s responsibility to get tested and know their status and live by the advice given at the hospital.
(Religion Group 5, male leader, age 43)
Religious leaders admitted that they are putting minimal effort into encouraging their members to take an HIV test during their service unlike in the past when the epidemic was new. The assumption that the congregants are now used to the messaging on HIV testing influenced the level of emphasis placed by religious leaders.
As a church, I should say that we don’t talk much about HIV and AIDS the way we used to do in the past. What I noted is that when a problem becomes chronic we tend to get used to it and it no longer becomes an issue. (Religion Group 4, Male leader, age 23)
In the past, the government would prompt religious institutions to share messages on HIV testing which is not the case at the moment. This has resulted in religious institutions exerting minimal effort on HIV testing matters within their institutions.
…to say the truth we have been quiet for a long time without telling people about HIV and AIDS and this is because there has not been any new information on the diseases To say the truth if one is reminded of an issue it becomes easier to take steps. (Religion Group 2, Male leader, age 50)
Notably, other sectors regard HIV and AIDS issues as personal matters while others believe in prayer for everything and in both instances, HIV testing would not be promoted. It was apparent in the discussion that the most acceptable means of HIV prevention for religious people is abstinence for unmarried people and faithfulness for married people. This is because sex outside of a marriage is considered a significant sin regardless of condom use according to most participants.
HIV can be prevented in several ways but we, as religious people, teach our followers that they can prevent HIV by being faithful to their partners and abstinence from those not married. Let me emphasize here that the church will not allow in any way the use of condoms! (Religion Group 4, Male leader, age 23)
In contrast, some religions allow the use of condoms among married couples as a form of family planning or in cases where there are infidelity issues. The following extracts indicate this finding.
My religion allows the use of condoms because it’s one of the family planning methods. In Islam, family planning is there and is allowed even in the Holy Quran the law is saying that a baby is supposed to be breastfed for two years after birth. Is this not family planning? (Religion Group 2, Male leader number 2, age 26)
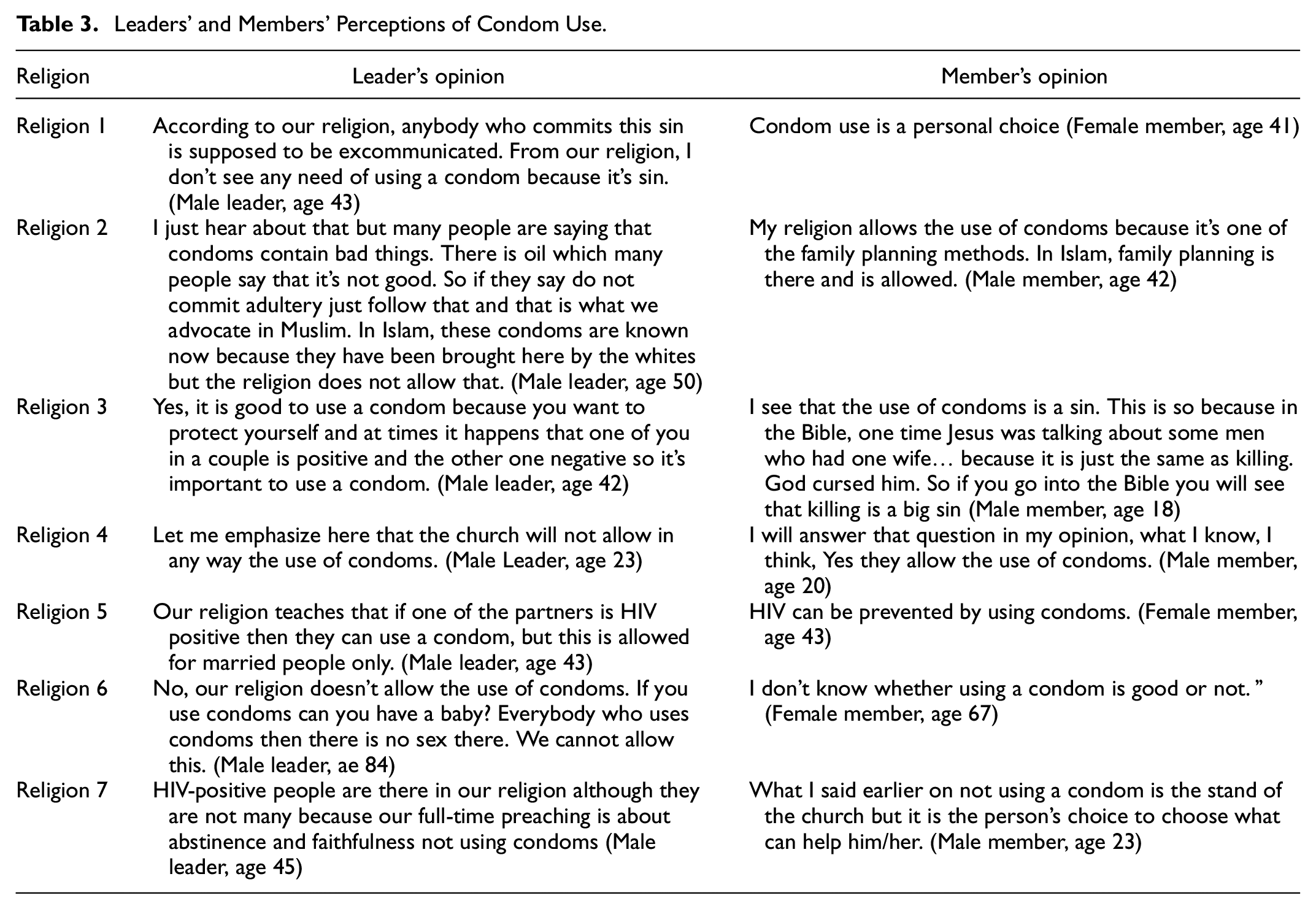
Although most respondents expressed that the use of condoms as a prevention strategy is not allowed by their religion, there were variations between religions and even within the same religion between religious leaders and followers. Leaders adhere to their religion’s stance that condoms are not allowed, while some members viewed it as a personal responsibility (Table 3).
Leaders’ and Members’ Perceptions of Condom Use.
Role of Prayer in HIV and AIDS Management
Religious people believe that prayer can cure any other disease including AIDS and would prioritize prayer over everything. In such cases, the congregants will be encouraged to pray over every ailment and may be barred from seeking health services.
We (the religious group) don’t advocate for HIV testing, as such, we don’t broadcast anything about that. We believe in Jesus Christ as a healer. Read Mathews 6 verse 8 which says: Jesus met Peter’s father-in-law who was suffering from malaria and he just 1touched his head he was healed. (Religion Group 5, Male leader number 2, age 42)
Curative benefits of prayer were also expressed in the ability to reduce the effects of the virus and boost immunity in return as expressed below:
On HIV and AIDS, prayer plays a very unique role because a person is advised to repent every sin which he has committed against God, and after that, we pray for him/her till the virus becomes weak and we continue with prayer till the virus is eliminated. (Religion Group 7, Male leader, age 45)
… Prayer just boosts the immune system but does not cure the virus, it does not give adverse effects. (Religion Group 4, Male follower, Age 20)
Participants reiterated that prayer yields emotional healing because it brings hope to the hopeless and facilitates the act of caring for one who is sick.
Another role of prayer is that it gives hope to someone who has HIV so that he stops being worried about his status. (Religion Group 3, Female Leader, age 48)
Alternatively, some religious people did not believe in faith-healing and insisted that God created drugs for every illness.
In our religion, we don’t believe in faith healing. Because our teaching says that our God cannot create a disease without its drug because the people that develop drugs do so with the gift of wisdom that comes from God. (Religion Group 2, Male leader number 1, age 26)
Religious-Related Barriers to HIV Testing and Counseling
Belief in Faith Healing
Faith-healing deters religious people from seeking HIV testing because they believe that God heals them hence rendering a test irrelevant. Furthermore, the belief in faith-healing delays health-seeking when one is ill because religious people will first consult a faith healer and only approach a health facility if the initial consult fails.
You know what? Just near that building (pointing at a building nearby) my sister and her husband stayed there. The two were strong Pentecostal believers of faith-healing such that when my brother-in-law fell sick, their pastor was just praying for him, but when the situation got worse we forced my sister to take her husband to the hospital. (Religion Group 1, Female member, age 41)
Some churches prohibit their followers from seeking medical assistance from a hospital including HIV testing services. Members of such religious groups risk being ex-communicated if they attend health services because that would entail a lack of faith in their beliefs.
When a person is sick, first of all, we pray for him, and if still sick we request permission from our leaders to go to the hospital. They do allow us… My priests may ex-communicate me from church if I am found taking a test at the hospital without their permission… (Religion Group 7, male follower, age 23)
Perceptions of Risk
Other religious people have a low HIV-risk perception of themselves and attribute it to the availability of spiritual men or prophets in their religion to reveal what someone did in secret. Therefore, they fear adultery and premarital sex because people will know about it.
… in our church, some people are gifted with supernatural powers and can know what one does in private, such that when a member commits adultery, they can know what was done. Their supernatural powers prevent the youths from committing adultery because they will know about it and will report it to the church. (Religion Group 7, Male follower, age 23)
Interventions for Promotion of HIV Testing Among Religious People
There is no specific HIV testing strategy preferred by all religious people. Participants highlighted the need of having multiple ways of reaching members with HIV testing services. These methods include self-testing, mobile or door-to-door, having HIV testing centers within the facility, and limiting testing to hospital facilities only. The leaders stated that they reach people using varying methods and could not state one method but encouraged the promotion of several interventions or strategies.
We reach people through different means, as religious people we cannot force people to follow a specific way. There are many HIV testing platforms and we should let our members use any one of them while respecting people’s privacy. (Religion Group 4, Male Leader, age 23)
However, the main concern was privacy during the testing process. To safeguard privacy, some religious people stated that self-testing would promote HIV testing and was preferred because a hospital-based test does not offer privacy such that when one has tested HIV positive, other people know because of the facial expressions displayed after testing HIV positive.
So a good way of testing is an oral test whereby they explain to you how to do it at the hospital and you are given a choice whether to do it at the hospital or carry it home and do it yourself. It takes about 20 minutes for you to see the results. (Religion Group 5, Female Member number1, Age 43)
Others prefer mobile or door-to-door HIV testing because it is convenient, especially in rural settings where people reside far from health facilities and cannot afford transport.
There are remote areas where transportation costs are expensive, mobile clinics will be beneficial in these areas for people to take tests. (Religion Group 2, Male leader number 2, age 50)
Also, other religious people suggested having HIV testing sites within the places of worship. They argued that if HIV testing is conducted at places of worship, their leaders will act as role models; as a result, many people will be tested.
The best way to get more people tested is to engage our leaders and conduct the testing within the religious premises. I remember this worked very well in Mangochi where a certain organization came into the company of our religious leader to run HIV testing services and it resulted in more people taking HIV testing. (Religion Group 2, Male leader number 1, age 26)
Participants recommended that the optimal days to reach most people would be during a designated day when services are conducted. It was also stated that worship day gatherings were an opportunity to reach most people who are in attendance. Furthermore, religious leaders are influential to their followers thereby optimizing uptake of HIV testing when they are engaged in the services thus they are an important entry to testing messages and services. Some religions also have structures for the management of HIV and AIDS services.
In our religion, we have structures at many levels. We use these structures to teach people about HIV and AIDS and other health issues in general. (Religion Group 4, Male leader, age 23)
Others preferred hospital-based HIV testing but argued that such services should be integrated with other services other than running them vertically to enhance privacy.
It is important to do multiple tests at once. For instance, when they are conducting, let’s say malaria test, they should also test for HIV and give results at the same time and in the same room. HIV testing services should not be separated from other services. People die because they don’t want to get ARVs from the Lighthouse (publicly) and at times they hire someone to get the drugs for them. (Religion 5, Female member number 1, age 43)
Discussion
Our study shows that the religious sector has a role in the implementation of HIV and AIDS services including creating awareness and promoting prevention. Prayer has a central place among religious people and they believe that it can cure, boost immunity, and offers emotional healing among HIV-infected people. The barriers to HIV testing that are related to religion include the belief in faith-healing which is embedded within the rules of a specific institution and a perception of low risk of HIV infection among religious people. Interventions for promoting HIV testing in the religious sector include; As well, one of the implementations of HIV self-testing, mobile and or door-to-door HIV services, church-based testing services, and facility-based services that are integrated with other services to preserve privacy.
As well, one of the findings is that the role of the church is to create awareness and cement what was asserted earlier that religious platforms can reach more people with HIV testing messages and services (MacCarthy et al., 2015; Nunn et al., 2013). Religious settings are popular and if actively involved will reach the masses with HIV and AIDS services (Ochillo et al., 2017). Additionally, religious leaders have positional power to influence their congregants on the uptake of interventions (Lindgren et al., 2013). Similarly, as reiterated in our study, religious leaders were comfortable with raising awareness and encouraging congregants on HIV testing because such activities are congruent with their mission statements (Derose et al., 2011). It has been argued that involvement and dissemination of HIV-related activities requires a leader who is passionate about support from lay workers as necessary (Derose et al., 2011). Thus, religious leaders can influence the uptake of HIV testing among their congregants.
The role of religious leaders in HIV and AIDSs could be strengthened by continued training (Rakotoniana et al., 2014; Stewart et al., 2018) which is tailored according to their needs (Stewart et al., 2018). Continuous and sustained capacity building will translate into continued involvement of the religious leaders in HIV and AIDS matters (Anugwom & Anugwom, 2018) which was also alluded to in our study. Contrariwise, in other settings, sharing HIV services is challenging among religious leaders hence needing support and strengthening of skills (Stewart et al., 2016). Religious leaders ought to be trained in the specific roles and responsibilities of HIV testing services.
Religious institutions are platforms where love is advocated for and expressed to HIV-infected people thus offering emotional healing as was reiterated in our study (Bluthenthal et al., 2012; Derose et al., 2011; Stewart et al., 2018). It has been argued that the incorporation of health issues in spiritual care enhances coping with the condition among those infected (Stewart et al., 2018), and improves spiritual wellbeing which is associated with attendance to HIV services (Yates et al., 2018). Contrary to our findings, in other areas, HIV and AIDS are often viewed through a moral lens which inevitably leads to stigma and discrimination (Anugwom & Anugwom, 2018). This is because stigma or fear of it limits the congregants’ and church leaders’ involvement in HIV and AIDS services within a congregation (Mendel et al., 2015). In other cases, stigma arises because of the belief that HIV infection is a result of punishment from God (Zou et al., 2009). Religious institutions promote love as part of their services which is an attribute that can be extended to HIV-infected congregants.
Teaching congregants about abstinence as expressed in our study is consistent with other studies that assert that such teaching remains congruent with religious missions (Derose et al., 2011) and it has been argued that religious groups use aspects like abstinence as synonymous with good habits and morals (Lindgren et al., 2013). Although churches use external support for HIV testing services, they have retained control in teaching congregants about abstinence and condom use which illustrates their motive to ensure that such messages remain aligned to their doctrines. (Derose et al., 2011). In an earlier study, despite Pentecostal youths being exposed to both faith and secular orientation toward HIV prevention strategies, they upheld the faith-based one which underscores the importance of their belief system in interacting with HIV services (Mpofu et al., 2014) which emphasizes the importance of leveraging on religious platforms for the provision of HIV services.
Our study advocates for the establishment of HIV testing centers within church platforms. Implementation of HIV services within a church is feasible and effective (Berkley-Patton et al., 2010; Berkley-Patton et al., 2012; Berkley-Patton, Moore, et al., 2013; Derose et al., 2011) and reaches more men (Jobson et al., 2019) and could use existing platforms within the church to optimise the delivery of HIV services (Berkley-Patton, Thompson, et al., 2013) by church leaders ( Berkley-Patton et al., 2016). We argue that closing the remaining gap in HIV testing will require using religious platforms to accelerate the closure. It has been asserted that church-based HIV testing could avert stigma and discrimination and remains acceptable since it upholds some cultural context as well because of the trust that exists (Stewart et al., 2016). Implementation of church-based HIV testing will require training and strengthening skills of the providers of the services if they are laypeople (Stewart et al., 2016). The services could latch on to the already existing health ministries within religious groups (Stewart et al., 2018). The church is an available platform that can ably implement HIV-testing services.
The silence on the use of condoms in our study is common among religious sectors because it is against most of their beliefs as they fear that unmarried congregants would be partaking in premarital sex (Anugwom & Anugwom, 2018; Barmania & Aljunid, 2016; Derose et al., 2011; Trinitapoli, 2011). The silence could also stem from the uneasiness that comes with talking about sexual issues (Lindgren et al., 2013) and again the dilemma that is faced by religious leaders in wanting to uphold their religious values against the use of condoms while being cognisant of the secular demands and the divergent views held by followers (Ochillo et al., 2017). Our findings on the limited promotion of condom use concur with what was raised in earlier studies in Malawi where seemingly most religious groups discourage premarital sex (Muula, 2010) with religious leaders strongly stressing the importance of abstinence and fidelity in marriage for both men and women (Rankin et al., 2016). Religious leaders fear that an acceptance of condoms would promote infidelity and undermine the message of abstinence which is core to religious beliefs (Muula, 2010; Ochillo et al., 2017). An earlier study stated that other religious leaders would encourage condom use to their members when privately consulted (Ochillo et al., 2017) while others recommended them when one is at risk of contracting HIV (Rakotoniana et al., 2014). Despite youths being aware of the non-promotion of condom use in churches, some still use them in the vein of practicing safer sex (Ochillo et al., 2017). Youths that are more aligned to a religious group are also less likely to use condoms in a sexual encounter which heightens their level of risk (Skovdal et al., 2011). We contend that there is a need of refining the messaging around condom use among the religious sector to achieve an understanding that highlights the risk element with each decision youths make. Furthermore, as much as religious leaders teach their followers the religious doctrines, the followers seem to make independent decisions that create a level of risk that is not targeted with interventions. The study reveals that members supported the use of condoms, contrary to the stand of their religions which is consistent with an earlier study conducted in Malawi among FBOs (National Statistical Office, 2019; Rankin et al., 2008). These similar findings underscore the importance of continuous engagement with faith and religious leaders for an effective plan for the prevention of HIV. The use of condoms may be challenging for FBOs to implement because they contradict their beliefs and virtues.
Previous studies have shown that faith-healing plays a role in HIV care in Malawi and offers a life free from worry about HIV issues which was reiterated in our study (Manglos & Trinitapoli, 2011). The difference in our study is that in some religions, the belief in faith-healing bars them from seeking any medical services including an HIV test. The belief that prayer will cure HIV as stated in our study extends what was reported earlier in Malawi where congregants were encouraged that the closer they are to God the less likely they will contract the virus (Lindgren et al., 2013). In some instances, the belief in faith-healing is a critical barrier to compliance with HIV-prevention strategies and the uptake of antiretrovirals.
The low perception of risk reported in our study among religious people is congruent with earlier studies (Stewart et al., 2019; Williams et al, 2011). Furthermore, our study reported that HIV testing is influenced by low-risk perception, faith healing, and religious doctrines as factors that influence HIV testing remains congruent with findings from a previous study that found that HIV testing is affected by risk perception, illness, level of stigma, and discrimination and anonymity of testing services (Kaai et al., 2012). The low-risk perception among religious people needs to change with messages that are tailored and emphasize that HIV affects anyone including religious people. Contrary to our findings on low-risk perception, other pastors are inclined that their youth congregants are engaged in risky sexual behaviors and could not be at a lower risk of contracting HIV (Stewart et al., 2019).
Door-to-door (Croxford et al., 2020; Mulubwa et al., 2019), HIV self-testing (Hatzold et al., 2020; Hlongwa et al., 2020) approaches as reiterated in our study have been advocated for in earlier studies and notably religious people could benefit from them as well. Although door-to-door HIV testing was cost-effective (Mangenah et al., 2020), the costs associated with it could be further reduced by using the platforms and volunteers within a church that offs-set the costs of running a door-to-door HIV testing approach.
Limitations of the Study
The nature of our study does not allow for generalization therefore the views may apply to those selected however the results provide insights on perceptions of religious leaders and their congregants on HIV testing. The views collected were perceptions and may not be honest responses as a way of stating what is socially acceptable, however, participants were encouraged to talk openly and assured that their identity will remain anonymous even in the reports. Future studies should consider using mixed methods approaches to maximize the results that will be gathered from various religious institutions among larger samples. Additionally, there is a need to expand to other districts or Traditional Authorities to maximize the scope of the results.
Strengths of the Study
The strength of this study lies in the sampled participants as they were drawn from various religions that are common in the area thus providing a broad scope of responses. The variety in responses as per religious beliefs provides policymakers with a variation for them to consider as they interact with religious circles.
Conclusion
Efforts in closing the gaps in HIV testing and reaching the vital few people remaining will require embracing all variations and operating and implementing strategies that remain congruent with other beliefs that influence uptake. Religious platforms are an avenue for HIV testing implementation and education on HIV and AIDS that need to be used more to attain the first 90 in the UNAIDS goals. The promotion of religious-based prevention interventions needs to consider the foundations and beliefs of each religion and be able to contextualize the methods which can be achieved by continuous dialogue and support from religious leaders. There is a need for more research on the implementation strategies that may be used to promote the uptake of HIV testing within religious settings.
Footnotes
Acknowledgements
We are thankful to the study participants that took part in the management of the various religious groups that allowed us to conduct the study in their institutions.
Dr. Nyondo-Mipando is supported by the Malawi HIV Implementation Research Scientist Training program (Fogarty: D43 TW010060) and these funders had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance and approval were granted by the College of Medicine Research and Ethics Committee (COMREC—Number P.01/17/2105) before commencing the study. The various religious groups provided support for the study. Each participant provided written informed consent before any study procedures and participants who could not read nor write thumb printed on the form after it was read to them in the presence of an impartial witness. We assured all participants that their participation in the study will not affect their membership to their religious grouping. We used codes instead of their actual names to preserve their confidentiality, anonymity, and privacy.