
Abstract
Background. Positive mental health can be defined as the presence of emotional, psychological, and social well-being. The original version of the Positive Mental Health (PMHs) scale appears to have good psychometric properties. This study aims to validate the Spanish version for the general population. Methods. A sample of 845 participants (425%–50.30% women) aged between 14 and 70 years (M = 32.1; SD = 4.2) was used. Descriptive analyses were performed on the items, as well as confirmatory factor analysis, convergent validity with protective factors and with risk factors. Results. Factor analysis confirmed a unidimensional structure with excellent model fit indices, high positive convergent validity especially with resilience to suicide attempts and optimism, and high negative convergent validity mainly with anxiety. Conclusions. The PMH is a scale with the necessary reliability and validity to be used in different psychosocial contexts, especially in the health care of the Spanish population.
Keywords
The term Positive Mental Health (PMH) was coined in 1958 when Marie Jahoda proposed that, within an appropriate social context, individuals should be able to manage their time, have meaningful social relationships, work effectively with others, have high self-esteem and be active. She summarized it as the ability of the individual to stand on their own two feet without making demands or impositions on others (Jahoda, 1958).
Two theories have traditionally dominated the field on the components of PMH. The first is the hedonic perspective, which focuses on the subjective experience of happiness and life satisfaction (Keyes et al., 2002). The other is the eudaimonic perspective, which focuses on psychological functioning and self-actualization (Ryan & Deci, 2001). Taking both approaches into account, PMH can be defined as the presence of a state of general emotional, psychological, and social well-being (Keyes et al., 2002). PMH thus refers to individuals who have a positive sense of well-being, resources such as self-esteem, optimism, a sense of mastery and coherence, satisfying personal relationships, and resilience or the ability to cope with adversity (Huppert, 2009; Word Health Organization [WHO], 2005).
However, despite the growing recognition of the importance of positive factors, there has been some criticism of this definition, arguing that it was constructed by considering only a portion of the world’s population and lifestyles, particularly in developed countries. The global generalizability of the findings of these studies is limited, which means that further research is needed on the positive protective constructs by studying different cultures (Bieda et al., 2017).
Currently, mental health can be described in two dimensions: one corresponding to mental disorders, symptoms, and psychological problems, and the other corresponding to PMH (WHO, 2005). PMH is not the same as the absence of psychopathology, they are part of two different but related constructs and both can be present in an individual at the same time. It is therefore important that there are assessments that not only determine the absence of psychopathology, but also the presence or absence of PMH and the levels at which it is present, in order to find relationships between the two dimensions. This in turn would allow for a more comprehensive view of mental health (Lukat et al., 2016).
Recently, a unidimensional scale called the Positive Mental Health Scale (PMHs) has been proposed, based on the combination of hedonic and eudaimonic perspectives for the definition of PMH, understood as the presence of a state of general emotional, psychological, and social well-being (Keyes et al., 2002). This 9-item Likert-type scale was tested in Germany in a series of samples of university students, psychiatric patients and the general population (Lukat et al., 2016). It was also adapted for Turkish university students, where positive correlations were found with optimism, happiness, and general self-efficacy, and negative correlations with depression, anxiety, and stress (Çeçen & Vatandaşlar, 2021). The scale showed good correlations with life satisfaction variables (Lukat et al., 2016). In addition, higher levels of PMH have been shown to be associated with healthier lifestyles (Lukat et al., 2016) and better suicide-related outcomes (Velten et al., 2022).
It was adapted during the COVID-19 pandemic for Iranian university students and showed excellent convergent validity with post-traumatic growth and social support and divergent validity with depression and post-traumatic stress disorder. It was able to discriminate between students at higher and lower risk of suicide (Naghavi et al., 2021). However, no studies have been found that have adapted this scale to the Spanish context (general population).
The present study aims to investigate the psychometric properties of the Positive Mental Health Scale, specifically to assess its structure and internal consistency in the general Spanish population. Protective psychological variables such as suicide resilience, self-efficacy, optimism, and perceived social support are expected to be positively related to the construct of positive mental health, in contrast to other (psychopathological) variables.
Method
Participants and Procedure
From an initial sample of 1293 participants, 448 were excluded because they did not meet one or more of the inclusion criteria. The inclusion criteria were: (a) being 14 years of age or older, (b) completing all questionnaires, (c) being of Spanish nationality or living in Spain, (d) reading the research information sheet and accepting and signing the informed consent form, and (e) in addition, participants between 14 and 18 years of age also had to accept and sign their participation with their parents’ or guardians’ first name and surname. Data from participants aged 14 to 18 years were included because it was considered of great interest to assess positive mental health in adolescents and young people. The final sample consisted of 845 participants, 425 (50.30%) females and 420 (49.70%) males, aged 14 to 70 years (M = 32.1, SD = 4.2). The contrast statistics used (Chi-square and Student’s t-test) showed that there were no significant differences in the sample in terms of age, but there were significant differences in terms of work or academic activity, as there was a significant proportion who were only studying or studying and working at the same time (Table 1).
Description of Sociodemographic Data.
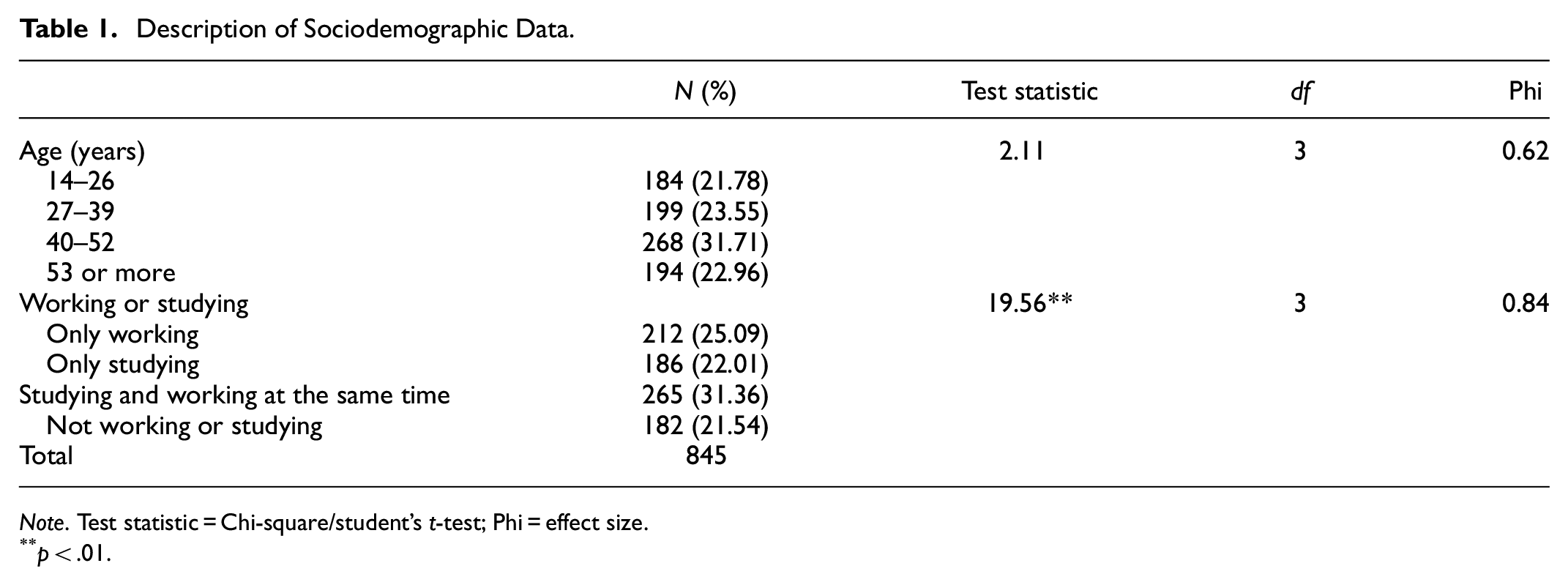
Note. Test statistic = Chi-square/student’s t-test; Phi = effect size.
p < .01.
First, the research ethics committee of the University of Jaén (Spain) was asked to approve the study (reference number: DIC.20/9.TFM). Permission to use the scale was obtained from the original author (Lukat et al., 2016). The original version of the PMH was then translated into Spanish (from Spain) using a standardized translation process consisting of a back-and-forth translation process in which the original version was translated by two native Spanish translators (one a psychologist and the other a Ph.D. in English Philology), both with a high level of English proficiency (Gjersing et al., 2010). A third psychologist reviewed the two translated versions and synthesized them into a single version. The original translators agreed with the synthesized version. The synthesized version was then back-translated into English by two different people (one a psychiatrist and the other a doctor of psychology). One of the back-translators was a native English speaker, while the other had studied in the UK. The same person who synthesized the initial translated versions reviewed the two back-translations and they were synthesized into one. Words that had been translated differently were discussed and agreed upon. Finally, the original instrument, the translated version, and the back-translated version were compared by a committee of Spanish doctoral students in psychology with a high level of English. Finally, the final version followed all the necessary steps for the cultural adaptation of psychological instruments (Muñiz & Fonseca-Pedrero, 2019; Appendix).
A snowball sampling method was used to send participants a link to a Google form containing the questionnaire. The link was distributed through social networks such as Facebook and Instagram, and email contacts were also used. The data was collected between April and December 2021. Participants received no compensation for taking part in the study. Participants completed the questionnaires in Spanish through an online survey platform (Google Forms, licensed by the University of Jaen in Spain). Informed consent was obtained from all participants, and the study followed the ethical guidelines of the Spanish Society of Psychology and the tenets of the Declaration of Helsinki.
Instruments
Sociodemographic data sheet. This measures gender, age, and employment or education status.
Positive Mental Health (PMH) by Lukat et al. (2016). This measures positive emotional psychosocial well-being, where the higher the score, the more positive the mental health. This unidimensional scale has 9 items with a 4-point Likert-type response (e.g., 3 = agree; 0 = disagree; e.g., “I enjoy my life”). It showed high reliability in the original version among university students and the general population in Germany (α = .92 and .93).
Hospital, Anxiety, and Depression (HAD-14) by Snaith and Zigmond (1986), adapted by Herrero et al. (2003). This has a 7-item subscale for anxiety (A; e.g., “My head is full of worries”) and a 7-item subscale for depression (D; e.g., “I’m still enjoying things as usual”) using a 4-point Likert-type format. This scale has good internal consistency for the overall scale (.90), .84 for the depression subscale, and .85 for the anxiety subscale. In this study the α for the whole inventory was .89 and it was also adequate for the subdimensions (αA = .86; αD = .83).
Life Orientation Test-LOT-R by Scheier et al. (1994) adapted by Ferrando et al. (2002). This instrument has 10 items with a 5-point response scale, where 0 is strongly disagree and 4 is strongly agree. Of the 10 items, only 6 measure aspects related to dispositional optimism, the rest are distractors (optimism, e.g., “usually expect to have a good day”). The internal consistency of the Spanish version was α = .70. In the present study, α = .77 was found for optimism.
General Self-Efficacy Scale-GSE (Schwarzer & Jerusalem, 1995), translated into Spanish by Sanjuán et al. (2000). This measures general self-efficacy and has 10 items with a response scale from 1 (completely wrong) to 4 (completely right; e.g., “I can solve difficult problems if I try hard enough”). The internal consistency of the Spanish version was .84 and in the present study α = .90.
The Multidimensional Scale of Perceived Social Support (MSPSS) by Zimet et al. (1988) was adapted into Spanish by Landeta and Calvete (2002). This 12-item instrument with 7 response alternatives (where 1 is “strongly disagree” and 7 is “strongly agree”) measures the subject’s perception of their level of social support (e.g., “There is a person who is there when I am in a difficult situation”). The reliability of the original study in samples of university students was α = .85 and in the present study α = .97.
Scale of Resilience to Suicide Attempts (SRSA-18) by Sánchez-Teruel et al. (2021). This assesses resilience to suicide attempts and predicts future suicide reattempts 6 months after the first attempt (e.g., item 3: “When I have a problem, I ask my family or friends for help”). The 18-item scale has adequate internal consistency (α = .88; ω = .89) and concurrent validity with general resilience and resilience in suicidal ideation. In the present study, α = .88.
Data Analysis
Incomplete data represented less than 2% of the responses and a multiple imputation method (SPSS) was used for the missing values (Graham, 2012). A descriptive analysis of the items was carried out first. A confirmatory factor analysis (CFA) was then carried out using SPSS 23 AMOS. The method used in the confirmatory analysis was generalized least squares (GLS). The fit indices and criteria were: χ2, root mean square error of approximation (RMSEA; less than 0.05; Steiger & Lind, 1980), goodness of fit index (GFI; greater than 0.90; Jöreskog & Sörbom, 1986), comparative fit index (CFI), and Tucker-Lewis index (TLI; TLI and CFI ≥ 0.95; Tucker & Lewis, 1973). Finally, tests of scale reliability and convergent validity were carried out.
Results
Descriptive Analysis and Internal Consistency of the Items
The results of the Spanish PMHs gave a mean (and standard deviation) of 19.16 (6.42), with a minimum score of 0 points and a maximum score of 27 points, and univariate normality (Table 2). All items correlated well with the total score, and there was no improvement in the overall reliability of the scale when any of the items were removed.
Descriptive Statistics, Skewness and Kurtosis Indices, and Item Analysis.

Note. SE = standard error of skewness and kurtosis; K-S = Kolmogorov-Smirnov test.
p < .05. **p < .01.
Confirmatory Factor Analysis
The results showed multivariate normality of the item scores (Mardia = 126.28; Mardia, 1970) and that the χ2 was adequate and significant (χ2 = 139.36; df = 93; p < .01). All parameter estimates were excellent for a factorial model with nine items, and a single common factor was estimated: RMSEA (95% CI) was less than 0.05 (0.02[0.01, 0.04]), there were adequate values for CFI (0.97), TLI (0.96), and GFI (0.98), with high agreement between the model fit indices. This demonstrates the unidimensionality of the PMH items for this sample of the general Spanish population.
Reliability and Convergent Validity
In terms of internal consistency of the PMHs, we found α = .96 and ω = .97, confirming the previous descriptive results (Table 2), which showed that eliminating some of the items would not improve the reliability of the scale in this sample.
In terms of convergent validity, as Table 3 shows, there was a significant and positive relationship between positive mental health as measured by the PMHs and optimism (LOT-R = 0.79; p < .05), and in particular with resilience to suicide attempts (SRSA-18 = 0.92; p < .05). There also appeared to be high negative convergent validity between the PMHs and anxiety (HAD-A = −0.80; p < .05).
Convergent Validity Between PMHs and Different Protective and Risk Variables.

Note. PMHs = Positive Mental Health Scale; GSE = general self-efficacy; LOT-R = optimism; SRSA-18 = resilience to suicide attempts and reattempts; MSPSS = perceived social support; HAD-A = anxiety; HAD-D = depression.
Significant correlation at the .05 level.
Significant correlation at the .01 level.
Discussion
This study examined the psychometric properties of the nine-item PMH scale in a Spanish population. In general, the PMH-Scale showed good psychometric properties. The results found in this study are similar to those of the original German version (Lukat et al., 2016) and very similar to the subsequent adaptations in other countries and cultures (Brailovskaia & Margraf, 2020; Çeçen & Vatandaşlar, 2021; Naghavi et al., 2021). In fact, a unidimensional structure of the scale was found with excellent model fit indices and high reliability, as well as convergent validity with optimism and resilience to suicide attempts and reattempts, and high negative convergent validity with anxiety.
All this helps us to understand that positive mental health is an essential part of mental health in general, as it allows us to shed light on the presence of protective factors of well-being - instead of only focusing on risk factors—as suggested by previous studies (Bibi et al., 2020; Brailovskaia et al., 2020; Hu et al., 2022; Teismann et al., 2019). This tool provides a more ecological approach to understanding mental health in the population. Negative associations between the PMH scale and depressive symptoms were consistent with the hypothesis.
One of the limitations of this study may be the particular global context at the time due to the COVID-19 pandemic, which significantly affected the lifestyles of people in different areas (Brailovskaia & Margraf, 2020). This makes it difficult to generalize the results. This global situation of great adversity may have influenced participants’ responses, focusing more on psychopathological outcomes rather than resilience outcomes, suggesting the need for future studies in a “post-pandemic” context to determine whether there are significant changes and whether this is reflected in the results. Finally, the information in this study could be improved if measurement invariance had been applied, which would be useful if there were two (or more) groups being compared together. This could be done in a future study.
Conclusions
The PMHs is a unidimensional instrument that shows high levels of reliability and validity in the general Spanish population. The fact that this is the first translation of this scale into Spanish represents a great opportunity for further adaptations with respect to gender and age in the Spanish population, as well as cultural and linguistic validations in other geographical contexts, such as Latin America.
Its brevity and ease of administration should help it to become part of psychosocial intervention projects and programs in the general and clinical population. This would allow us to offer a more transdiagnostic view of mental disorders, increasing the need to measure and incorporate protective factors within mental health.
Footnotes
Appendix
Positive Mental Health (PMH-scale) in Spanish.

| 0 = disagree/no estoy deacuerdo | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| 1 = I tend to disagree/Tiendo a estar en desacuerdo | ||||
| 2 = tend to agree/Tiendo a estar de acuerdo | ||||
| 3= agree/de acuerdo | ||||
| 1. I am often carefree and in good spirits/Suelo estar despreocupado y de buen humor | ||||
| 2. I enjoy my life/Disfruto de mi vida | ||||
| 3. All in all, I am satisfied with my life/En general, estoy satisfecho con mi vida | ||||
| 4. In general, I am confident/En general, tengo confianza en mí mismo | ||||
| 5. I manage well to fulfill my needs/Me las arreglo bien para satisfacer mis necesidades | ||||
| 6. I am in good physical and emotional condition/Me encuentro en buen estado físico y emocional | ||||
| 7. I feel that I am actually well equipped to deal with life and its difficulties/Siento que estoy realmente bien equipado para afrontar la vida y sus dificultades | ||||
| 8. Much of what I do brings me joy/Gran parte de lo que hago me produce alegría | ||||
| 9. I am a calm, balanced human being/Soy un ser humano tranquilo y equilibrado |
Source. Adapted from Lukat et al. (2016). Creative Commons Attribution 4.0 International License. Adapted with permission.
Author Contributions
David Sánchez-Teruel: Conceptualization, writing—original draft preparation, experimentation, modeling validation, investigation, methodology, modeling reviewing, and reviewing and editing. María Auxiliadora Robles-Bello: Conceptualization, writing-original draft preparation, experimentation, modeling validation, investigation, methodology, modeling reviewing, and reviewing and editing. Souhib Lorabi, Selma Boufellous and Irhomis Mendoza-Bernal: experimentation, modeling validation, investigation, modeling reviewing, methodology, and reviewing and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.