
Abstract
The current study investigated the psychometric proprieties of the Romanian form of the Preschool Anxiety Scale—Parent version (PAS). The sample consisted of 514 Romanian children (266 boys and 249 girls) aged 3 to 6 years. The mothers of these children completed the PAS and the Parenting Styles and Dimensions Questionnaire—Mother Form (PSDQ), and the children’s teachers completed the Behavior Assessment System for Children, Second Edition, Teacher Rating Scale (BASC-2 TRS). Results reveal that the PAS has satisfactory psychometric proprieties on the Romanian sample: it shows a good reliability and a good fit of the data with the underlying correlated five-factor structural model. The construct validity of the Romanian form of the PAS was supported by a significant relationship between the PAS total anxiety score and various BASC-2 (anxiety, withdrawal behavior, atypical behavior, learning problems, adaptability, social skills, learning skills, and leadership), and PSDQ (authoritarian, permissive, and authoritative parenting style) scales. Age had a significant effect on the generalized anxiety, physical injury fears and separation anxiety scales, and girls scored significantly higher than boys on the total anxiety score and the physical injury fears scale.
Introduction
This paper addresses the adaptation of the Preschool Anxiety Scale—Parent version (PAS; Spence et al., 2001) to the Romanian culture. The PAS is an assessment instrument for the measurement of anxiety in kindergarten children, and robust measurement of this issue is important in the context of increasing number of reported anxiety cases in small children (Salvati Copiii Romania, 2010). A transparent report of the adaptation process for this measure is important for clinical professionals, for educators and parents in Romania. Internationally, our report is important because it compares the invariance of the Romanian form of the test with other cultural adaptations, thus shedding light on the cross-cultural validity of this widely used instrument, and because our approach to the adaptation may inspire other researchers who embark on similar projects.
Anxiety disorders are one of the most prevalent forms of psychopathology among children and adolescents, with studies reporting a prevalence increasing from 5.5% in 2007 to 6.4% in 2011 to 2012 (Bitsko et al., 2018). More recent, in the USA, data from the 2016 National Survey of Children’s Health (NSCH) shows that, among children aged 3 to 17 years, 7.1% currently have anxiety problems, but only 59.3% of these children receive treatment (Ghandour et al., 2019). In Romania, a national analysis published in 2010 reported that 20% of the child population suffers from mental health problems affecting their functionality, and 13% of those (i.e., 572.741 children) have been diagnosed with anxiety disorders (generalized anxiety, social anxiety, phobia, separation anxiety, or panic disorder) (Salvati Copiii Romania, 2010).
Romanian children are more vulnerable to mental health psychopathology than children in other European countries, due to several reasons: the public mental health system is oriented primarily toward treatment and less toward prevention, there is a lack of collaboration between educational institutions and mental health services, parents are reticent to approach mental health assessment, a limited number (only about 5%–10%) of school counselors (who could contribute to prevention and to the early diagnosis of school-aged children) have competences in clinical assessment, and there no screening projects are conducted in public schools (Salvati Copiii Romania, 2010).
Anxiety in early childhood is becoming a serious problem because of its increasing incidence and its complex clinical pattern. Many factors (e.g., family context, the child’s medical history) are common risk factors for the early onset of anxiety disorders, but among these parenting style has a special place (Lau et al., 2017).
Diagnosing anxiety at an early age is important, because its detection and proper treatment may prevent the later development of more severe mental health issues in children. This is in fact one of the reasons childhood anxiety disorders have such a high: they are chronic and persist over the years, into adult life (Majdandžić et al., 2018), tending to evolve in time in association with comorbid disorders, mainly depression and conduct/behavioral problems. For example, in the USA, 1 out of 3 children with anxiety also exhibit conduct/ behavior problems, and childhood anxiety is a risk factor for developing depression (Axelson & Birmaher, 2001). Clinical research emphasizes the idea that anxiety disorders developed at an early age can be effectively addressed in primary or educational settings, by focusing on parenting strategies rather than on direct treatment of the child (Cheung et al., 2013), making the intervention far less expensive and more likely to be accessed also by lower income families (Ghandour et al., 2019).
While a larger number of measures have been proposed for the screening of anxiety disorders in preschool children (e.g., the Anxiety Disorders Interview Schedule for DSM-IV Parent Version, ADIS-P-IV, Silverman & Albano, 1996; the Child Behavior Checklist, CBCL, Achenbach, 1991; or the Strengths and Difficulties Questionnaire, SDQ, Goodman, 1997), instruments for comprehensive assessment are far fewer. The most widely used of these (Leung et al., 2019) is the Spence Children’s Anxiety Scale (SCAS) (Spence et al., 2001). In her studies, Spence (1997) identified six diagnostic subtypes of anxiety in children: generalized anxiety, social anxiety, obsessive-compulsive disorder, physical injury fears, panic attack and agoraphobia and separation anxiety. Among these, five were diagnostic-subtype categories applicable to preschool children, defined by 28 anxiety symptoms, and resulting the five subscales of the Preschool Anxiety Scale—Parent version (PAS; Spence, 1997). The scale is a valuable instrument for practitioners to identify young children who are at risk for developing anxiety disorders and to tailor proper family-based interventions in order to prevent escalation of the symptoms and severe clinical cases in later life. Our current study focuses on the cultural adaptation of the PAS for Romanian preschool children.
The present study reports on the adaptation of the Preschool Anxiety Scale—Parent version (PAS; Spence et al., 2001) for Romania. The test is an important measure of anxiety in the preschool population and is the first standardized comprehensive test for the assessment of anxiety in 2 to 6 years old children in Romania. Our study also contributes to the wider literature by providing findings about the cross-cultural replicability of the PAS, and reporting on the anxiety of preschool children in an understudied East-European culture.
The PAS is a parent-report instrument, containing 28 items that evaluate anxiety symptoms or related affects. The items are statements of varying symptom severity and are distributed across five basic scales: generalized anxiety (5 items), social anxiety (6 items), obsessive-compulsive behavior (5 items), physical injury fears (7 items), and separation anxiety (5 items). Items are rated by respondents using a 5-point Likert-type scale (not true at all, seldom true, sometimes true, quite often true, very often true). Internal consistencies ranging from .64 to .94 have been reported in the standardization sample (Spence et al., 2001). Examples of items are: “Has difficulty stopping him/herself from worrying” (generalized anxiety), “Worries that he/she will do something to look stupid in front of other people” (social anxiety), “Keeps checking that he/she has done things right (e.g., that he/she closed a door, turned off a tap)” (obsessive-compulsive behavior), “Is scared of heights (high places)” (physical injury fears), and “Is reluctant to go to sleep without you or to sleep away from home” (separation anxiety).
The PAS already has a history of adaptation to other cultures. It was adapted in Western Europe to the Dutch language and culture (Broeren & Muris, 2008), and in South-East Asia to the Chinese language and culture (Leung et al., 2019; Wang & Zhao, 2015). The Dutch adaptation was conducted on 275 preschool children aged 2 to 6 years. The five scales had moderate to high reliability coefficients (α between .59 and .86). On the exploratory factor analysis, the five-factor model fitted reasonably with the original model (Broeren & Muris, 2008). The PAS was adapted in mainland China in 2015 on a sample of 1,854 mothers of 3 to 6 years old children and all 28 items had loadings in excess of .31 on their hypothesized factors. Also, the five factors were found to be strongly intercorrelated, with rs ranging from .52 to .87. Cronbach’s α coefficients were .87 for the total scale, .55 for separation anxiety disorder, .72 for physical injury fears, .75 for social phobia, .68 for obsessive–compulsive disorder, and .70 for generalized anxiety disorder (Wang & Zhao, 2015). The Hong Kong version of PAS was adapted on a sample of 1,317 parents of 3 to 6 years old children. The confirmatory factor analysis showed a good fitting model and a good factorial validity of the correlated five-factor model. The version also demonstrated acceptable reliability and satisfactory validity, with Cronbach’s α coefficients ranging from .90 to .64 (Leung et al., 2019).
Our work on the cultural adaptation of the PAS to the Romanian language and culture brings with it two main benefits. From a research perspective, our data (as well as data further collected with the adapted form of the test) is valuable as it will permit the cross-cultural comparison of the structure and evolution of anxiety disorders in children; this is important as Eastern Europe in general and Romania especially are severely understudied cultures in this regard. We will also provide several analyses on the validity of the PAS (both related to its structure and to its correlation with other tests), that may generalize to other language forms of the test. From a practical perspective, it will empower Romanian clinical psychologists with a valid measure with which to diagnose anxiety disorders at an early age, enabling them to develop interventions informed by robust assessment.
The Cultural Adaptation Process of the PAS
The cultural adaptation process of the PAS in Romania followed the guidelines for test translation and adaptation issued by the International Testing Commission (International Test Commission, 2008). The translation procedure followed a number of four steps. First, two independent translators (one psychologist and one linguist) produced each a Romanian (translated) version of the test. Second, first author of the present paper, acting as adjudicator, discussed the two translations with both initial translators and produced a consolidated Romanian form. Third, two blind backtranslations were produced by two Romanian-English teachers working independently. Fourth, an expert committee with two bilingual doctoral level clinical psychologists lead by the first author of this paper discussed discrepancies between the original and back translated English forms of the test and made the appropriate changes to the Romanian form. The resulted Romanian form of the test is the pilot-version that was used in the current paper.
This study reports on data and analyses that focus on the psychometric properties of the Romanian form of the PAS, which will be the only dedicated standardized test assessing anxiety in preschool children in Romania (excepting the anxiety scale of the BASC-2, which is part of a broadband measure). We examine the convergent correlational patterns of the PAS with the Behavior Assessment System for Children, Second Edition, Teacher Rating Scale (BASC-2 TRS; Reynolds & Kamphaus, 2004); this analysis is especially interesting because the two tests used assessments provided by different sources, that is, parents and teachers respectively, avoiding issues related to common method variance.
Methods
Sample
Our data reflects a community sample of 514 children (266 boys and 249 girls) aged 3 to 6 years. This total sample was split into two different age groups. The first group contained 293 children aged 3 to 5 years, attending kindergarten (138 boys and 155 girls). The second group contained 221 children 6 years of age attending preparatory class (127 boys and 94 girls). The sample contains an almost equal amount of rural (249 children; 132 in the first and 117 in the second age group) and urban (265 children; 161 in the first and 104 in the second age group).
All these children were assessed with the focal test (the PAS) by their mothers (ages from 20 to 50 years for the mothers of children 3–5 years, M = 32.59, SD = 5.16: ages from 24 to 58 years for the mothers of 6 years old children, M = 33.84, SD = 5.48), and were also assessed with the BASC-2 TRS by their teachers: 52 female teachers from 34 educational units.
Procedure
This study is part of a larger research about the relationship between parenting styles, anxiety and atypical behavior in preschool children (Cucu-Ciuhan, 2021). When we started the study, the first author had meetings with kindergarten teachers from schools in South Romania, and teachers who accepted to voluntary participate were instructed on how to collect data. Every participant teacher selected 10 children (with high, medium and low degrees of anxiety) from their class for the study. Written informed consent was taken from the children’s’ parents. The study followed common ethical practices in research with human subjects.
Measures
Child anxiety
Child anxiety was measured with the Preschool Anxiety Scale—Parent Version (PAS; Spence & Rapee, 1999), on five dimensions: generalized anxiety, social anxiety, obsessive-compulsive disorder, physical injury fears, panic attack and agoraphobia and separation anxiety. The instrument is described above. Reliabilities in our sample are reported in Table 1.
Reliabilities and Scale Intercorrelations for the PAS Scales.
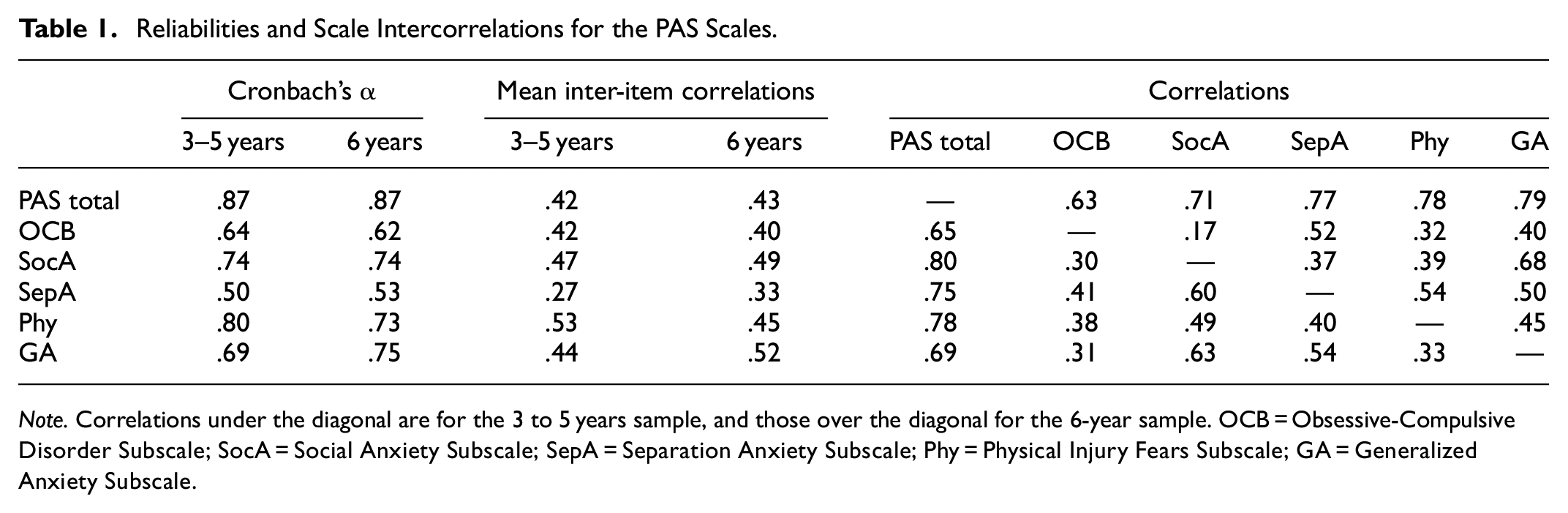
Note. Correlations under the diagonal are for the 3 to 5 years sample, and those over the diagonal for the 6-year sample. OCB = Obsessive-Compulsive Disorder Subscale; SocA = Social Anxiety Subscale; SepA = Separation Anxiety Subscale; Phy = Physical Injury Fears Subscale; GA = Generalized Anxiety Subscale.
Variables convergent and divergent with anxiety
Data about variables related in a convergent or divergent manner to anxiety were collected with the Romanian version of the Behavior Assessment System for Children, Second Edition, Teacher Rating Scale (BASC-2; Reynolds & Kamphaus, 2004). The BASC-2 is a comprehensive multidimensional screening test for mental health problems in children, that was adapted for the Romanian population (Ion et al., 2011) and is commonly used in clinical practice. We used the Teacher Rating Scales (TRS) in two different forms: the BASC-2 TRS 2 to 5 years, for all the kindergarten children in our sample, and the BASC-2 TRS 6 to 11 years for all the preparatory school year children. The BASC-2 TRS 2 to 5 years has 100 items, and the BASC-2 TRS 6 to 11 years has 139 behavioral items (e.g., “Tries new things,” “Adapts easy with new teachers”); all of which are rated using a 4-point frequency scale (never, sometimes, often, always). Both forms score on 11 main scales (Hyperactivity, Aggression, Anxiety, Depression, Somatization, Atypicality, Withdrawal, Attention Problems, Adaptability, Social Skills, and Functional Communication) and the 6 to 11 years form has four supplementary scales (Conduct problems, Learning Problems, Leadership, and Learning Skills). Reliabilities for all the scales and forms are reported in Table 2.
Means and Standard Deviations for the PAS Scales: Romania Compared to Other Cultures.
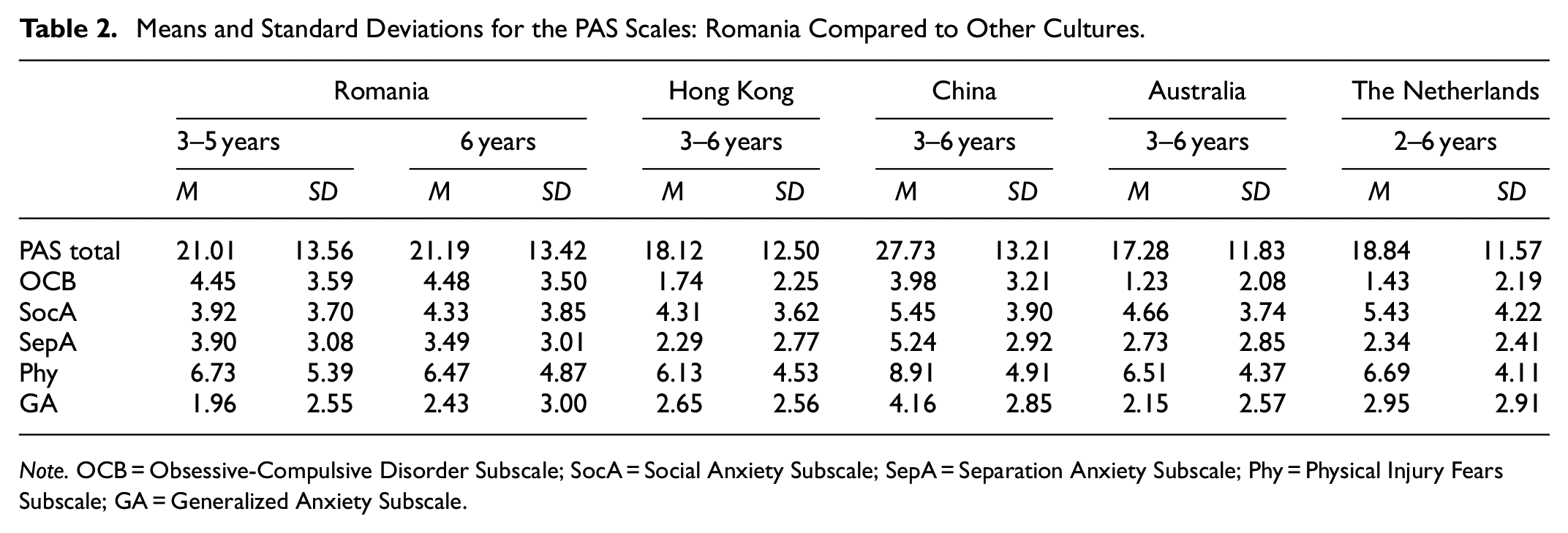
Note. OCB = Obsessive-Compulsive Disorder Subscale; SocA = Social Anxiety Subscale; SepA = Separation Anxiety Subscale; Phy = Physical Injury Fears Subscale; GA = Generalized Anxiety Subscale.
Parenting styles
The Parenting Styles and Dimensions Questionnaire—Mother Form (PSDQ, Robinson et al., 1995) was used to assess the parenting style. The PDSQ is a parent report test measuring the three parenting styles of authoritative, authoritarian, and permissive parenting (Baumrind, 1971). In our study, the PDSQ was filled by the child’s mother, who also assessed the father’s parenting style (i.e., “[He guides] [I guide] …”). The test has 62 items (e.g., “[He guides] [I guide] our child by punishment more than by reason.”) that are rated using a five-point frequency scale (never, once in a while, about half of the time, very often, always). Internal consistencies in our sample are reported in Table 3.
CFA Estimates for PAS for Romania.

Note. OCB = Obsessive-Compulsive Disorder Subscale; SocA = Social Anxiety Subscale; SepA = Separation Anxiety Subscale; Phy = Physical Injury Fears Subscale; GA = Generalized Anxiety Subscale.
Demographic variables
The Questionnaire for Family Context and Child Development was designed by the first author of this paper in order to collect demographics (age, gender, parent’s age, marital status, living conditions, siblings, urban/rural area, parent’s education, economic status, family medical history) and the life history of the mother and child (pregnancy, birth, child’s medical history, psychiatric diagnosis, life events, school attending, principal caretaker), as well as qualitative data about the family context and the evolution of the child. It has 18 items with 2 to 6 response choices and was filled in by the child’s mother.
Analytical Strategy
First, we computed means and standard deviations, reliabilities (Cronbach’s α and mean inter-item correlations), and scale intercorrelations for the focal test (PAS). Second, analyzed the factor structure of the PAS through of a confirmatory factor analysis. Third, we investigated age and gender effects on the PAS. Fourth, we investigated the convergent and divergent correlations of the PAS with the scales of two other measures: the BASC-2 and the PSDQ. All analyses were computed separately for the 3 to 5 years and the 6-year sample, with the exception of the confirmatory factor analysis, which was computed based on the consolidated sample, due to the advantage of a larger sample in this analysis (Bollen, 1989).
Results
Reliabilities and Scale Intercorrelations
Table 1 presents reliabilities (Cronbach’s α and mean inter-item correlations) for the PAS total scores and scales, separately for the 3 to 5 years and the 6 years sample. The reliabilities for the Romanian form of the test are between .50 and .80 (3 and 5 years) and between .53 and .75 (6 years) for the PAS scales, and .87 for both samples for the PAS total score. The lowest scale reliability is for the Separation Anxiety scale (.50 for the 3–5 years and .53 for the 6 years sample). The highest scale reliability in the 3 to 5 years sample is for the Physical Injury Fears scale (.80), and in the 6-year sample for the Generalized Anxiety scale. Mean inter-item reliabilities are between .27 and .53 (for the 3 and 5 years sample) and between .33 and .52 (for the 6 years sample).
Scale intercorrelations (also in Table 1) are between .30 and .63 for the 3 and 5 years sample, and between .17 and .68 for the 6 years sample.
Means and Standard Deviations
Table 2 presents the means and standard deviations for the PAS total score and scale scores (for both samples), together with the similar results obtained in the various countries where data on the PAS were previously reported. Direct comparison of mean scores in cross-cultural data is inappropriate unless a specific level of equivalence (usually metric equivalence) was previously established (Byrne & van de Vijver, 2010). Only the paper reporting on the Hong Kong data (Leung et al., 2019) presented a confirmatory factor analysis on the PAS, showing adequate fit to the expected model, but even in this case, a multigroup CFA, the recommended procedure in such cases (Byrne, 2008) could not be performed.
Confirmatory Factor Analysis
Table 3 presents the standardized regression weights (i.e., factor loadings) of the 28 PAS items onto the corresponding factorial dimensions, in a correlated five-factor model. The model fit for this confirmatory factor analysis, loading each of the items on the scales prescribed by the scoring keys, was acceptable: CFI = 0.927, TLI = 0.902, RMSEA = 0.046 (95% CI 0.041–0.052), SRMR = 0.049. The factor loadings of the items on corresponding dimensions ranged from .35 to .66. The factor determinacies (i.e., the correlations between the latent and observed factors) were of .86, .92, .88, .90, and .90 for the five respective scales.
Age and Gender Effects
For the correlation between age and the PAS scales (using the combined sample, 3–6 years), significant effects were shown for the Generalized Anxiety scale (r = .11 p < .01), Physical Injury Fears scale (r = .10 p < .05), Separation Anxiety scale (r = .13 p < .01). Table 4 shows the gender effects for the PAS scales. For the 6-year sample no significant differences between boys and girls were found. For the 3 to 5 years sample, significant differences were found for the PAS total score (t[290] = −1.92, p< .01, d = .22) and for the Physical Injury Fears scale (t[290] = −2.94, p < .05, d = .33). The MANOVA analysis showed that there were no statistically significant differences in the PAS scores based on the interaction effects of gender and age.
Gender Effects for the PAS Scales.
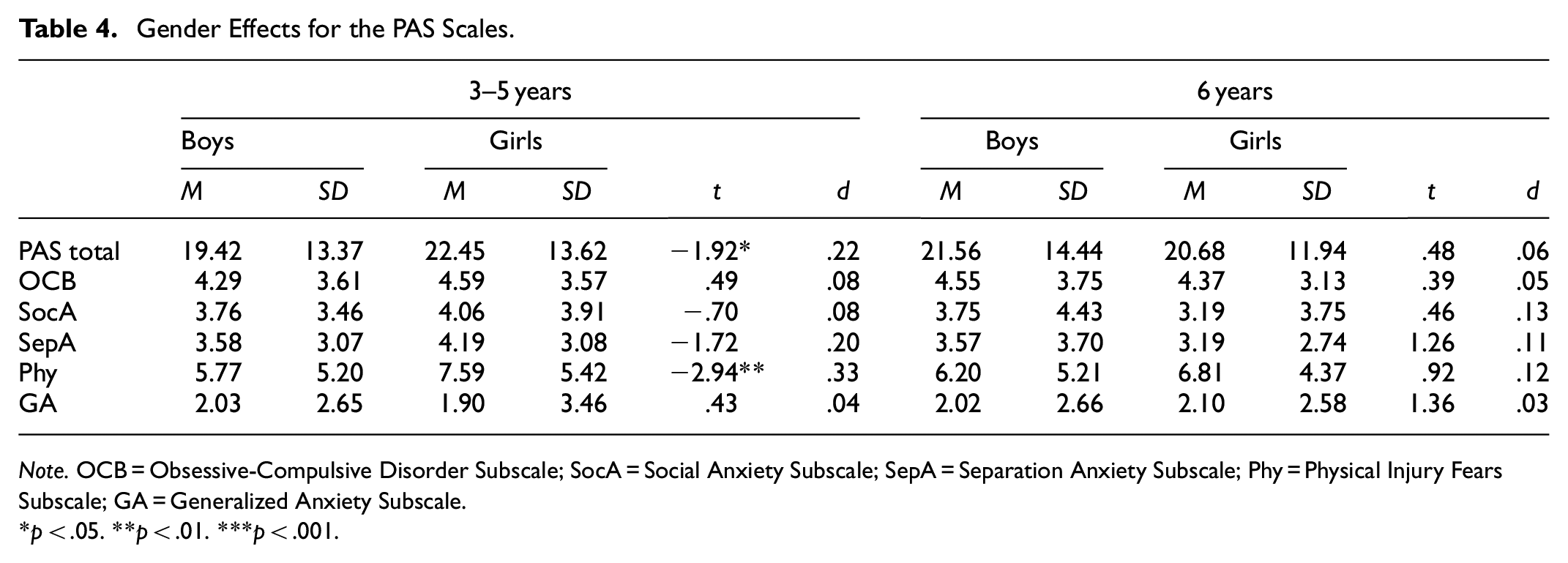
Note. OCB = Obsessive-Compulsive Disorder Subscale; SocA = Social Anxiety Subscale; SepA = Separation Anxiety Subscale; Phy = Physical Injury Fears Subscale; GA = Generalized Anxiety Subscale.
p < .05. **p < .01. ***p < .001.
Convergent Validity
Table 5 presents the means, standard deviations and reliabilities for the BASC-2 and PSDQ scales that were used for an analysis of the convergent and divergent validity of the PAS, and Table 6 presents the respective correlations, all separately on the 3 to 5 years and 6-year sample.
Means, Standard Deviations, and Reliabilities for BASC-2 and PSDQ Scales.

Correlations Between PAS Scales, and BASC-2 and PSDQ Scales.

Note. OCB = Obsessive-Compulsive Disorder Subscale; SocA = Social Anxiety Subscale; SepA = Separation Anxiety Subscale; Phy = Physical Injury Fears Subscale; GA = Generalized Anxiety Subscale.
p < .05. **p < .01. ***p < .001.
The PAS Total Anxiety scale showed reasonable convergent validity with the BASC-2 Anxiety scale for both 3 to 5 years and 6 years children (rs of .19 and .30, p < .001), as it did for the Withdrawal Behavior scale (rs of .20, p < .001 and .27, p < .01). For the 6 years group, the Total Anxiety scale also showed positive correlations with Learning Problems (r = .23, p < .001), Atypical Behavior (r = .23, p < .001), and significant negative correlations with Adaptability (r = −.26, p < .001), Social Skills (r = −.17, p < .05), Leadership (r = −.21, p< .01), and Learning Skills (r = −.15, p < .05).
Correlations between the PAS Total Anxiety scale and the various PSDQ scales are also in the expected direction. For the 3 to 5 years sample, the PAS Total Anxiety scale showed significant correlations (positive) with Authoritarian Parenting Style, both for Mother (r = .17, p < .001) and Father (r = .19, p < .01), and with Permissive Parenting Style, also both for Mother (r = .24, p < .01) and Father (r = .19, p < .05). For the 6 years sample, the PAS Total Anxiety scale showed significant correlations (positive) only Authoritarian Parenting Style Mother (r = .43, p < .001) and Father (r = .40, p < .001), and with Permissive Parenting Style Father (r = .23, p < .01), and (negative) with Authoritative Parenting Style, both Mother (r = −.16, p< .01) and Father (r = −.20, p < .01).
The PAS subscales also show important convergent correlations in the expected direction with various BASC-2 and PSDQ scales, as shown in Table 5.
Discussion
Summary of Findings
The present study showed the Romanian form of the PAS to have satisfactory psychometric properties, with a very good reliability for the total anxiety score and average to high reliabilities for each of the five scales. The correlated five-factor model, including generalized anxiety, obsessive-compulsive behavior, separation anxiety, social anxiety, and physical injury fears revealed a good fit for the data, and the result is in line with the findings from other cultures (e.g., Australia, mainland China, Hong-Kong, and Netherlands) (Leung et al., 2019). The Romanian form of the PAS also showed the expected relationships with corresponding scales of the BASC-2 (e.g., positive correlations with anxiety, withdrawal behavior, atypical behavior and learning problems, and negative correlations with adaptability, social skills, learning skills, and leadership). The PAS also showed high convergent validity with authoritarian and permissive parenting styles as measured by the PSDQ. Age was found to have a significant effect on three subscales: generalized anxiety, physical injury fears, and separation anxiety. Significant gender differences were found in the total anxiety score and in the physical injury fears subscale (but only for the 3–5 years sample), with girls scoring higher than boys. No significant differences in PAS scores were found based on the age × gender interaction.
Comparison With Previous Studies
In general, mean scores on the Romanian PAS were lower than those reported in mainland China (Wang & Zhao, 2015), but higher than for Hong Kong (Leung et al., 2019), Australia (Spence et al., 2001), and the Netherlands (Broeren & Muris, 2008).
Romanian children scored significantly higher on obsessive-compulsive behavior compared with all other countries. Saad et al. (2017) show that the severity of obsessive-compulsive symptoms in the pediatric population does not differ between genders, does not correlate with socio-economic status, is slightly associated with increasing age, but correlates with child functional impairment, behavioral problems, and comorbid conditions (Saad et al., 2017). In our sample, an investigation of the BASC-2 scales scores shows that we register high means in attentional problems and withdrawal behavior, which are usually associated with functional impairment and behavioral problems. This could explain the higher obsessive-compulsive scores in our sample compared to other countries. We also observed that two of the five items on the obsessive-compulsive behavior scale have significant higher scores than the other three: “Washes his/her hands over and over many times each day” (M = 2.19, SD = 1.60) and “Keeps checking that he/she has done things right (e.g., that he/she closed a door, turned off a tap)” (M = 1.38, SD = 1.41). This could lead to another explanation for the higher obsessive-compulsive behavior scores in our sample: since the mothers completed the PAS test in the presence of the child’s teacher, they may have given more desirable answers to the two items that they considered to refer to the child’s good behavior.
Also, Romanian children scored significantly lower on generalized anxiety than all the other countries, but we note that Hong Kong, the Netherlands and Australia also show a low score on this scale (Leung et al., 2019; Spence et al., 2001; Wang & Zhao, 2015). Lower scores in our sample are registered on two particular items: “Has trouble sleeping due to worrying” and “Spends a large part of each day worrying about various things.”
Parenting practices have an important role on the insertion and development of anxiety symptoms in children, and our findings are consistent with results obtained in other cultures. Anxiety in children is correlated with an authoritarian parenting style, that is, intrusive, controlling and overprotective parents lead to a tendency in children to avoid threat instead of controlling it, and to develop anxiety (Hudson et al., 2011). This is also consistent with the findings from China, where parents are more restrictive and punishment oriented and where PAS scores are higher compared to other countries (Leung et al., 2019; Wang & Zhao, 2015).
Implications and Limitations
The current study showed that the Romanian PAS is a valid and reliable instrument for the measurement of anxiety in preschool children and that it can be used with confidence in clinical and research contexts. Anxiety in Romanian preschool children show the expected five-factor structure, therefore suggesting that clinicians should use this structure when assessing a child’s specific individual profile and designing psychological interventions. Romanian children showed higher scores than any other country on the obsessive-compulsive behavior scale. This may suggest a need for extensive research to specifically identify the cultural-sensitive factors that lead to this symptomatology.
The practical implications of the current study are also important, both for Romanian and international specialists. In Romania, the validation of an assessment instrument for measuring preschool children anxiety will enhance the clarity and effectiveness of the diagnosis of these issues in children. International researchers may use our findings in their own efforts to adapt this important measure or other similar instruments to other cultures, or in creating and/or adapting evidence-based instruments designed to measure emotional difficulties in preschool children.
We also note several limitations of the current study. First, we were not able to compare the ratings of mothers and fathers, since all the parents who completed the tests were mothers. Second, we could not approach cross-cultural comparison of mean scores in a robust framework, as we lacked data on which to establish equivalence between the structure of data reported in the different other cultural adaptations of the PAS.
Despite these limitations, we consider the results of this study important both in providing results that contribute to the establishment of the PAS as a landmark psychometric instrument, and in reporting data on child anxiety in an understudied culture.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The article contained in the submission has not been published elsewhere and is not currently being considered for publication. The assessment described in this paper are made in a psychology individual practice office approved by the Ethics Committee of the University of Pitesti, Romania (No. 608/23.06.2021). Written informed consent forms were signed by the parents of all children included in the study.