
Abstract
To assess the knowledge, attitude, practice, and determinants of intimate partner violence (IPV) among nursing female student in a tertiary hospital in Abakaliki. A cross-sectional descriptive study was done in a tertiary hospital in Abakaliki between 1st March 2018 and 31st August 2018 among 450 nursing female student. They were interviewed using a Composite Abuse Scale (CAS) version 2013. Analysis was done using IBM SPSS Statistic version 20. The prevalence of any type of IPV among respondents was 47.8%. The majority (70.9%) were aware of IPV and the commonest mode of information was mass media (60.0%). Majority of the respondent would resort to prayer following IPV and only 15.5% would report to police. The most common form of abuse reported was emotional &or harassment abuse (26.6%). Student’s age (OR = 0.42; 95% CI [0.41, 0.92]), social class (OR = 0.60; 95% CI [0.40, 0.90]), level of study (OR = 0.45; 95% CI [0.29, 0.68]), and partner’s level of education (OR = 0.60; 95% CI [0.42, 0.88]) were determinant of respondent experiencing IPV. Less than 50% of the respondent were aware of legislation against IPV. The study shows a high level of IPV among the studied group. Screening for IPV is advocated among the students’ population especially among the young adolescent. Efforts should also be made by the government to increase awareness about Nigerian law against IPV.
Introduction
Intimate partner violence is a global health problem. It includes physical violence, sexual violence, stalking, and psychological aggression by a current/former romantic and/or sexual partner (Breiding et al., 2015). The true burden of IPV is not known. While men can be recipients of IPV, women experience IPV at higher rates. IPV is estimated to affect 35% of women worldwide (World Health Organization [WHO], 2013). There is a regional variation on the lifetime prevalence of IPV, the highest rate is seen in developing world of which African (36.6 95% CI [32.7, 40.5]) region is second to South-East Asia (37.7 95% CI [32.8, 42.6]) region on cases of physical and/or sexual intimate partner violence (WHO, 2013). Various studies in Africa including Nigeria have shown the level of “domestic terrorism” that women under go from their partners. In Nigeria a high prevalence rate of IPV has been reported (Anzaku et al., 2017; Benebo et al., 2018; O. I. Fawole et al., 2005; Onanubi et al., 2017; Umana et al., 2014) among Nigerian women. These disturbing findings in Nigeria are also seen in other studies in African countries (Burgos-Soto et al., 2014; Delamou et al., 2015; Malan et al., 2018; Ogum Alangea et al., 2018).
The patriarchal nature of African societies which encourages male dominance with the subjugation of women as a “tool to a means” is an important factor to IPV (Bowman, 2003). In Nigeria, for example, the gender equality index is low, Nigeria is estimated to rank 128th in Global Gender Gap Index with score of 0.635 (World Economic Forum, 2019) and this might probably be contributing to IPV. Some women justify IPV against other women which might ultimately encourage further acts of IPV (Ajah et al., 2014; Esere et al., 2009). The victims’ apparent non-reporting of an assault to appropriate channels for redress and lack of enabling laws in some African countries encourages the perpetration of this bastard act (IPV) to thrive. It is, however, gladding that with the passage of Nigerian law against IPV, succor would be given to victims of domestic violence (Violence Against Persons (Prohibition) Act, 2015).
The male partner is the common perpetrator of female IPV. Some of the risk factors for this behavior among men include drug dependence, jealousy, alcoholism, low educational attainment, having multiple sexual partners, inability to meet financial needs, childhood abuse, and family history of domestic violence (Adebayo, 2014; Esere et al., 2009; Matseke et al., 2012; Ntaganira et al., 2008; Onoh et al., 2013; Shamu et al., 2011). IPV is associated with several negative health problems on the victims which some of them are: physical injuries, disabilities, substance use problems, suicidal ideation, difficulty in establishing a further relationship with men, sleep disturbances, fear, poor academic performance, anxiety, and substance abuse (Breiding et al., 2014; Onanubi et al., 2017; Spencer et al., 2016; Wood et al., 2018) huge man-hour lost in production, and health-related cost (National Center for Injury Prevention and Control, 2003). It could also lead to femicide and Africa has been reported to have the highest rate of intimate femicide (UNODC, 2019). IPV has been argued to occur in three phases which are the tension building phase, crisis phase, and the honeymoon phase (Shelter For Help in Emergency, 2022). The cycle of abuse tends to increase without intervention and could result in femicide. Femicide could occur either in tension or crisis phase. The mechanism of femicide vary and could result from physical injury, neglect of the victim, the victim being under tension and unlikely to seek and receive prompt medical care when sick as this is likely to be prevented by the perpetrator.
Unintended pregnancy, adverse pregnancy outcome, nonuse of condoms, sexually transmitted diseases including HIV/AIDS are some of the sexual and reproductive health problems of IPV (Maman et al., 2000; Bernstein et al., 2016; Hampanda et al., 2017; Onanubi et al., 2017). Exposure to IPV can increase women’s risk for human immunodeficiency virus (HIV) infection (Hampanda et al., 2017). It also affects partner disclosure of HIV status and a woman’s adherence to therapy with resultant poor performance on antiretroviral medication (Maman et al., 2000). Ignoring the increasing global burden of IPV, therefore, can be a hindrance to the international community effort in ending the AIDS epidemic by 2030 (WHO, 2017). This becomes particularly important in sub Saharan countries like Nigeria where the prevalence of HIV/AIDS disease is assuming an epidemic proportion. Apart from the above findings, IPV negatively affects the academics performance of the victim.
The majority of women undergo trauma in silence which makes it difficult to intervene and eradicate IPV (Ibekwe, 2007; WHO, 2012). This “silence syndrome” in Nigeria constitute an impediment to eradicating the cankerworm called IPV (Ibekwe, 2007). According to a study by Linos et al. less than 40 % of Nigerian women that are victims of intimate partner abuse reported ever seeking help to stop the chain of abuse from the perpetrator. Help-seeking among the victims were found to be dependent on the level of Human Development Index of the states (Linos et al., 2014) which calls for a deliberate effort to empower women and develop the girl child in Nigeria as a long term measure in addressing IPV. Various reasons adduced for women’s tolerance of an abused partner include “fear of retaliation, lack of alternative means of economic support, concern for their children, lack of support from family and friends, stigma or fear of losing custody of children associated with divorce and love with the hope that the partner will change” (WHO, 2012).
In Nigeria, reduction or possible elimination of partner based violence would involve the education of women on their reproductive and sexual rights. There is a need also to address the cultural belief systems that are not supportive of women’s rights in Nigeria (Ibekwe, 2007). It has been advocated that women should have zero tolerance of domestic violence and every case should be reported to appropriate authorities (Ibekwe, 2007; Titilayo et al., 2014). This will enable punishment of perpetrators and deter perpetrators from further incidents, compensate survivors, and provide them with the necessary interventions for their rehabilitation. It has been argued by Ibekwe (2007) that violence against women should be made a state affair and with the recent promulgation of law against IPV in Nigeria (Violence Against Persons (Prohibition) Act, 2015), it is hoped that affected women in Nigeria will seek redress when their right is infringed by their partner.
This work is embarked upon to assess the knowledge, attitude, and practice of IPV among nursing students in a tertiary hospital in Abakaliki. It will also help to assess their rate of IPV victimization and its determinants. Findings from our study will assist the authority in the hospital to proactively put measures in place to assist and prevent IPV among the students. It will also help to improve their curriculum toward prevention and management of IPV after their nursing education.
Materials and Methods
Study Design
To assess the knowledge, attitude, practice, and determinants of IPV among nursing female student in a tertiary hospital in Abakaliki.
Methods
Study Setting
The study was carried out in nursing and midwifery schools of Alex Ekwueme Federal University Teaching Hospital, Abakaliki.
Study Population
The study population was female nursing students that met the inclusion criteria. They were consenting females who were not pregnant and are currently in an intimate partner relationship for the past 12 months. Study population was limited to those who are currently in an intimate partner relationship to help reduce recall bias and to help us assess the current risk that the students are undergoing. Those who were excluded were those who refused to consent, sick, or are not in an intimate partner relationship for the past 12 months. A simple random sampling method (ballot method) was used for respondent’s selection. Consented students were asked to pick a piece of blue paper marked “Yes” and “No” with replacement from a black polythene bag into which an equal number of paper “Yes” and “No” paper were added. Students that picked a paper marked “Yes” were recruited as the study population. They were interviewed between January 2018 and May 2018 in a dedicated office using a pre-tested structured questionnaire (Cronbach’s alpha = .72) and a Composite Abuse Scale (CAS) version 2013 (Hegarty et al., 2005). The questionnaire was filled by the participant after thorough explanation and understanding of the study instrument. The social class of the study population was determined based on the work of Olusanya et al. (1985) which used the educational level of the women and the occupation of the husband for determination of a woman’s social class. The social class of the study participants that were not married were based on that of their parents. They were graded into social classes 1 to 5. Social class 1 and 2 were classified as upper social class while social class 3, 4, and 5 were classified as lower social class. “Intimate partner violence (IPV) is defined as actual or threatened physical, sexual, psychological, emotional, or stalking abuse by an intimate partner while an intimate partner is defined as a current or former spouse or non-marital partners, such as a boyfriend or dating partner” (Basile et al., 2007). Knowledge of IPV was assessed using 22 items, correct answer was scored as 1 and incorrect answer as 0. Overall knowledge scores were calculated by adding the individual scores (answers); the highest scores was 22. A score of 10 and above was assessed as adequate overall knowledge of IPV while a score less than 10 was assessed as inadequate overall knowledge of IPV. The 22 items instrument was pretested among 30 nursing students on ward posting in AEFUTHA. The internal consistency was found to be good (Cronbach’s alpha of 0.70).
Sample Size
The sample size was gotten using the formula N = Z2 PQ/D2. Where N = required sample size. Z = 1.96 at confidence level at 95%; P = estimated population of 44.6% (Esere et al., 2009) D; margin of error at 5% and Q = 1 − P. The sample size for the study is 460 after the addition of a 20% attrition rate.
Ethical Consideration
Ethical approval for this study was obtained from the ethical committee of the hospital. The ethical approval number is REC APPROVAL NUMBER 14/11/2017-19/12/2017. Approval for the use of CAS was obtained from Kelsey Hegarty of the University of Melbourne. Informed and written consent was obtained from the participant before inclusion into the study.
Composite Abuse Scale (CAS)
“CAS is an easily administered self-report measure that provides standardized subscale scores on four dimensions of intimate partner abuse consisting of 30 items presented in a six-point format requiring respondents to answer “never,”“only once,”“several times,”“monthly, weekly,” or “daily” in twelve months. It assess the following: Severe Combined Abuse Factor, Emotional Abuse factor, Physical Abuse factor, and the Harassment factor. The CAS is made up of four subscales: Severe Combined Abuse (SCA; 8 items; possible score 0–40), Physical Abuse (7 items; possible score 0–35), Emotional Abuse (11 items; possible score 0–55), and Harassment (4 items; possible score 0–20)” (Anikwe et al., 2021; Hegarty et al., 2005).
The Severe Combined Abuse Factor Represent Severe Physical Abuse Items, All Sexual Abuse Items, and Physical Isolation Aspects of Emotional Abuse
“Raped me; Used a knife or gun or other weapons; Took my wallet and left me stranded; Tried to rape me; Kept me from medical care; Locked me in the bedroom; Refused to let me work outside the home; Put foreign objects in my vagina” (Anikwe et al., 2021; Hegarty et al., 2005)
The Emotional Abuse Factor Include Verbal, Psychological, Dominance, and Social Isolation Abuse Items
“Told me that I was not good enough; Told me that I was stupid; Did not want me to socialize with my female friends; Told me that I was crazy; Became upset if dinner/housework was not done when they thought it should be; Blamed me for causing their violent behavior; Tried to turn my family, friends and children against me; Told me that no one else would ever want me; Told me that I was ugly; Tried to keep me from seeing or talking to my family; Tried to convince my family, friends and children that I was crazy” (Anikwe et al., 2021; Hegarty et al., 2005).
The Physical Abuse Factor Has 7 of the Less Severe Physical Abuse Items
“Pushed, grabbed or shoved me; Hit or tried to hit me with something; Shook me; Slapped me; Threw me; Kicked me, bit me or hit with a fist; Beat me up” (Anikwe et al., 2021; Hegarty et al., 2005).
The Harassment Factor Represents Actual Harassment
“Harassed me over the telephone; followed me; Hung around outside my house; Harassed me at work” (Anikwe et al., 2021; Hegarty et al., 2005).
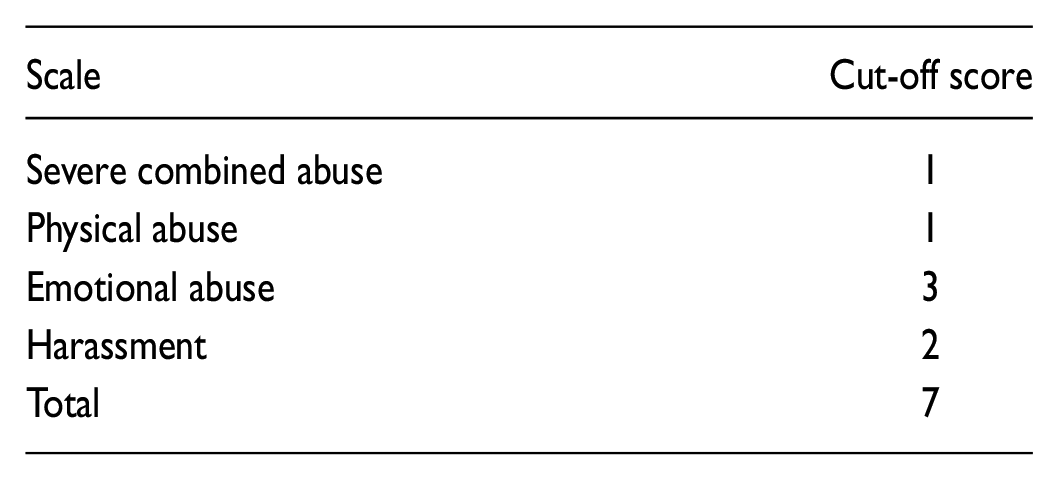
“The subscale score was calculated and was compared with a predetermined cut-off score for each subscale (Hegarty et al., 2005) as shown below to determine whether they have suffered that abuse” (Anikwe et al., 2021). A subscale score greater than the set score would determine that the respondent had such abuse. Example if a woman has a SCA score of 10, Emotional abuse score of 15, Physical abuse score of 30, and Harassment abuse score of 20 the total score is 75; each score above is greater than the predetermined cut-off score and the woman will be adjudged to have suffered each of the above abuses. Categorization will determine the category of composite abuse. An overall score of 7 and above determines an individual that has suffered an abuse.
CAS Cut-Off Score
Abuse Categorizations
“The type of abuse experienced by each respondent was categorized as shown below. SCA took precedence over the other forms of abuse so that any participant who had experienced SCA fell into the SCA category (Category 1). The second category includes all participants who had experienced Physical Abuse in combination with Emotional Abuse and/or Harassment. Participants who have experienced at least one episode of Physical Abuse, but no other forms of abuse, fell into the third category, Physical Abuse Alone. The final category contains all participants who had experienced Emotional Abuse and/or Harassment, but not any other form of abuse” (Anikwe et al., 2021; Hegarty et al., 2005).
Abuse Categorizations Sequence

Validation of CAS
“To test the reliability and internal consistency of the CAS, we surveyed 36 female nurses in the Department of Obstetrics and Gynaecology of Alex Ekwueme Federal University Teaching Hospital, Abakaliki. Respondents completed the questionnaires twice in 2 weeks and responses were matched and compared for test-retest reliability. The internal consistency for the scale was good (Cronbach’s alpha = 0.72)” (Anikwe et al., 2021).
Data Analysis
Data analysis was done using IBM SPSS statistic 20 software. Chi-square (χ2) and logistic regression analysis were used for categorical variables where applicable. The student’s age (≤23 or >23 years), marital status (married or single), year of education (≤3 or >3 years), and social class 1 and 2 (upper social class); social class 3, 4, and 5 (lower social class) were reclassified for easy analysis. The partner’s characteristics were also reclassified into ≤30 years and >30 years. The odds ratios with their 95% CI were calculated to determine the strength and presence of an association. p-Value of <.05 is adjudged significant. Odds ratio <1 implies decreased likelihood of being a victim of IPV, while OR > 1 represented increased probability of suffering from IPV.
Results
A total of 460 questionnaires were shared, out of which 450 (97.8%) students were in intimate partner relationships and were analyzed. From Table 1, the mean age of the women was 23.0 (95% CI [22.4, 22.6]) years (not in the Table). The majority of the study population were between 20 and 24 years. More than 40 % of the respondent belong to lower socioeconomic class. More than three-quarters are single. The mean partner’s age was 30.0 (95% CI [29.0, 31.1]) years (not in the Table) with the majority being employed. The highest level of education attended by the male partner was tertiary education.
Socio - Demographic Characteristics of the Women (n = 450).

From Table 2, the majority had adequate knowledge of IPV which they got majorly from friends and watching television. Only 12% of women were aware that stalking is a form of IPV. When asked whether they have a friend with a history of IPV, 46% (207) was affirmative in their answers.
Respondent Knowledge About Intimate Partner Violence.

Multiple answer allowed.
Among our study population, only 47% were aware of such legislation against IPV. The commonest source of information was reading the newspaper and watching television (Figure 1).

Sources of information about Nigerian Law against IPV.
Table 3 below shows the profile of IPV observed in the women. The point prevalence of IPV was 47.8%; 37.8% including those with and without experience have a history of being afraid of their partner. The commonest type of IPV experienced was Emotional &/or Harassment abuse.
Profile of Intimate Partner Violence Among the Study Respondent.

As shown in Table 4, more than 50% of the student would report a case of IPV. A majority (167, 37.1%) of those that will report said they would report to their parent while 24% will report to the partner’s parent. Less than one-fifth of the respondent would report to the criminal justice system for redress on experiencing IPV. Those that would not report attributed their major reason for not reporting on fear of further attack (26.0%) and shame (24.0%). The Table also shows that majority of the respondent would resort to prayer (243, 54.0%) while 35.1% (158) would keep quiet on being assaulted.
Respondent Reaction and Attitude Toward Intimate Partner Violence.
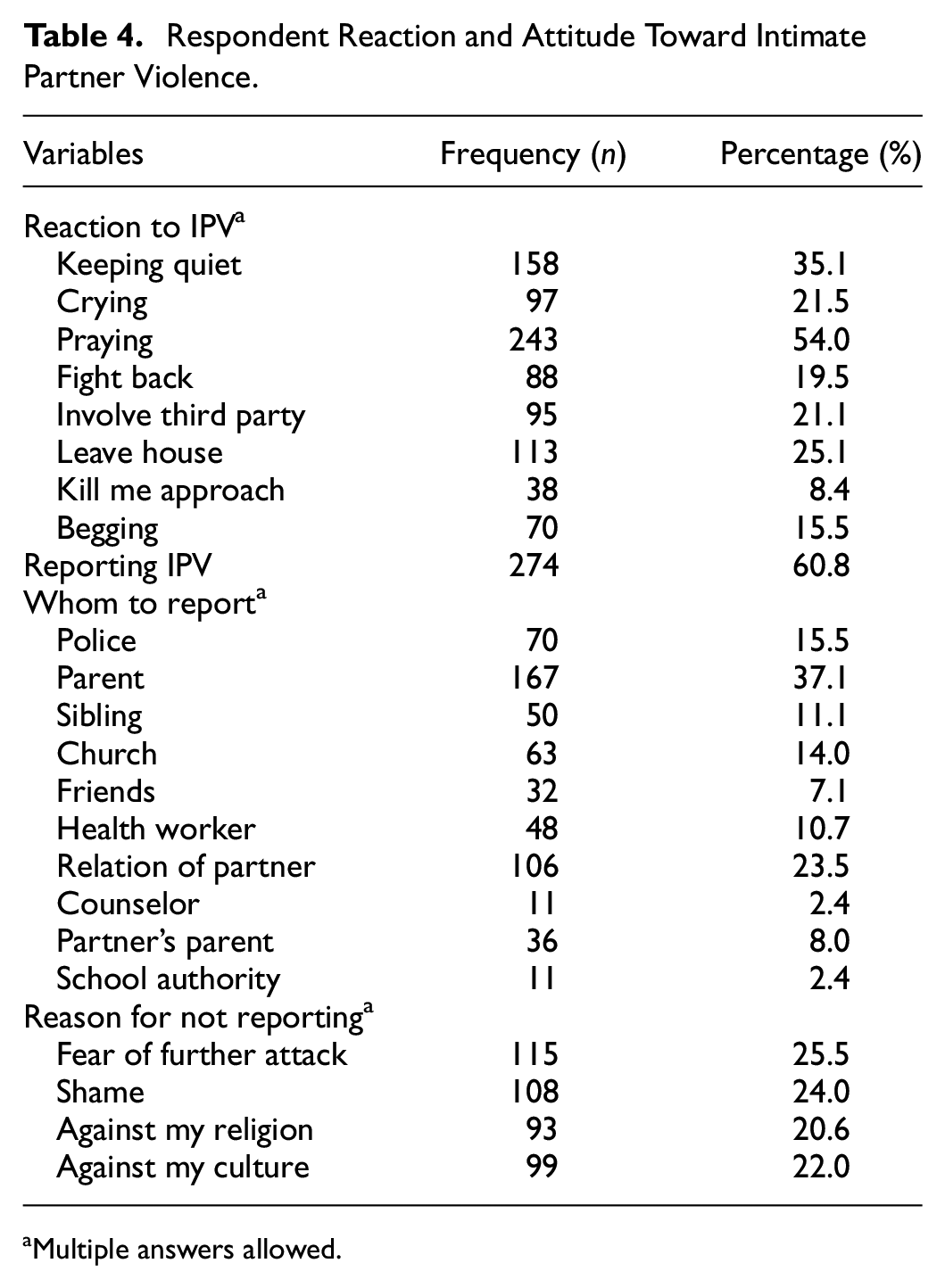
aMultiple answers allowed.
From Table 5, the age of the respondent and history of IPV had a significant association. There is a 58% chance of a student who is more than 23 years being assaulted than those that are ≤ 23 years with true effect size of 35% to 73%. Being in lower socio-economic class is associated with increased odds of being a victim. Cohort of women who are married were at reduced risk of IPV than being single (OR = 0.61 95% CI [0.24, 0.48]).
The Determinant of Intimate Partner Violence Among the Respondent.

Significant.
Discussion
IPV is an epidemic which needs to be prevented. This study is embarked upon to assess the knowledge, attitude, practice, and determinants of intimate partner violence among nursing students in, Abakaliki. Our study shows that the majority of the female nursing students have adequate knowledge of IPV and the common sources of information are mass media (60%), friends (26%), and reading books (18%). The most common type of IPV known by the study group was sexual violence which was followed by emotional and psychological violence. This might be a reflection of the type of assault that has been experienced by themselves, their friend and relation. It is quite discomforting that about 53% of the students are not aware of a Nigerian law that was recently promulgated against intimate partner violence. Apart from its recent promulgation into law by Nigerian government (Violence Against Persons (Prohibition) Act, 2015) being a factor for lack of knowledge among the study population, the fact that only 15.5% (70) of the students are willing to report to the Police might not be unconnected to the socio-cultural and religious factors affecting the fight against elimination of violence against women (Ibekwe, 2007). It, therefore, calls for dissemination of information about this law to the general populace by the Nigerian government. This will help the victim seek redress, punish perpetrator, deter perpetrators from further incidents, compensate survivors and provide them with the necessary interventions for their rehabilitation.
In our study, the rate of IPV among the study population was unacceptably high as almost 50% of the student reported being a victim of IPV within 12 months before the study. This is in keeping with the high rate of IPV in the study area (Anzaku et al., 2017; Benebo et al., 2018; Onanubi et al., 2017; Owoaje & OlaOlorun, 2012; Oyediran & Feyisetan, 2017; Tanko et al., 2016; Umana et al., 2014) and other African nations (Burgos-Soto et al., 2014; Ogum Alangea et al., 2018; Spencer et al., 2016). The two most common forms of IPV observed in the women were Emotional &/or Harassment abuse (26.6%) and SCA (14%). Physical, Emotional &/or Harassment abuse and physical violence were reported in 5.6% and 1.6% of respondents respectively. The rates of different forms of IPV seen in our study, however, differs from a similar study in Kano, Nigeria (Tanko et al., 2016); difference in the study population might account for this observation. (National Population Commission Nigeria, 2014). The occurrence of SCA among the female nursing students is highly disturbing as SCA represents the most severe form of abuse a woman can suffer (Hegarty et al., 2005) which can lead to the death of the victim. IPV increases the odds of negative physical and mental health conditions of the victim (Breiding et al., 2014; Spencer et al., 2016) and a significant contributor to poor academic performances of the victim (Wood et al., 2018). It can therefore adversely affect the academic performance of our study population thereby impinging on their future development. This finding from our study calls for urgent interventions by the Government and Non-Governmental Organization (NGO) in Nigeria to help address this “domestic terrorism” which these unfortunate women are experiencing.
IPV “cripples” and isolates a woman (Follingstad et al., 1990; Sassetti, 1993) and it not surprising from our study that a sizable number of the female nursing students are afraid of their male partner which might not be unconnected to the level of violence that they have undergone from their partners. It is however encouraging from our study that most of the women studied would report a case of IPV although it is disappointing that most would report to their relatives as shown in Table 4. This finding from our study negates the thinking that for the eradication of violence against women, women should have zero tolerance of it and every case of violence should be reported to appropriate authorities for redress (Ibekwe, 2007; Onanubi et al., 2017). It highlighted the need for a clarion call on the need to educate the women folk on their right and to the “evil” nature of domestic violence to themselves and her children (O. A. Fawole et al., 2016; National Population Commission Nigeria, 2014; Spencer et al., 2016; Titilayo et al., 2017).
More than two-fifth of the women interviewed attributed their reasons of not wanting to report a case of IPV to culture and religion while fear and shame accounted for the majority of their reasons which agrees with earlier reports (WHO, 2012). Cultural and Feminist theories of IPV in Africa offer a more plausible reason for these responses among our study population (Bowman, 2003). The patriarchal nature of traditional African societies with subordinate positioning of women with its pervasive gender inequality and interacting with traditional mores and norms supporting wife battering in Africa are plausible reasons for this attitudinal rationalization seen among our study population (Bowman, 2003). Benebo et al. (2018) in a study showed that community belief system that justify IPV negates the positive influence of women’s status on IPV reduction (OR = 1.89; 95% CI [1.26, 2.83]). Programs should, therefore, be put in place to re-orientate community members to embrace gender equity, mutual respect, and amicable resolution of family issues as a panacea to partner violence (Oyediran & Feyisetan, 2017).
The mean age of the women was 23.0 (95% CI [22.4, 22.6]) years with the majority belonging to 20 to 24 age brackets. This age bracket is the late adolescent stage when young girls might be trying to start an intimate partner relationship, for possible marriage, with the opposite sex. This agree with an earlier report of women at risk of intimate partner violence (Breiding et al., 2014; Onanubi et al., 2017; Stöckl et al., 2014). Our study population are mostly single and in low socioeconomic strata which leaves them prone to monetary manipulations by the opposite sex for their selfish gains. The mean age of female partner’s in our study was 30.0 (95% CI [29.0, 31.1]) years and it is the age bracket when most men have established a source of livelihood in the study area and are looking for a life partner.
The female nursing student’s age, social class, year of study, and partner’s level of education are a significant determinant of IPV among the women studied (p < .05). In our study, students who are 23 years and below and in low socioeconomic class have an increased odd of been assaulted by their partner and vice versa. This finding from our study could be explained from the perspective of Right and Feminist theories of IPV in Africa (Bowman, 2003). The Feminist theory of IPV in Africa attributes women’s subordinate position, passivity, gender inequality, and economic dependence as fundamental to the development of domestic violence (Bowman, 2003). Our study population being young and in lower class as an extension of feminist thinking, therefore, leaves them unacceptably prone to abuse by their male partner who are much older and economically less dependent. Apart from this, an explanation of the abuse could arise from the influence of cultural dictates of domestic violence in Africa and individual psychology and psychopathology of the batterer (Bowman, 2003). The latter argues that the batterer engages in violence against their partner as a result of personal insecurity and deep psychological dependence on their victim. In our study, the male partner being unemployed increases the risks by 73% of his partner being assaulted by him (95% CI [0.51, 1.06]); p > .05) and this odd is increased among male partners with below tertiary education (OR = 0.60; 95% CI [0.42, 0.88]). Above observations is in tandem with other works on this subject (Onanubi et al., 2017). According to the ecological model of violence, relationship level factors predisposing female youth to IPV seen in our study include unemployment and lower levels of education. Other factors include female partners having multiple partners, partner’s exhibiting controlling behavior, use of substance abuse and those who experienced violence when growing up (Krug, 2002; Uthman et al., 2010).
Limitations of the Study
Our study is a cross-sectional study involving only the nursing student in our center and the findings of this study could not be a representative of the population of the students in Abakaliki. It, however, opens a window to the possible prevalence of IPV in the state and Nigeria in general. It is also limited by the fact that a causal relationship could not be ascertained and there might be recall and social desirability bias. An effort was however made to reduce recall bias and social desirability bias by encouraging recall of IPV in the past 1 year and informing the study population not to write their names, phone numbers, and that the findings and report would not have anything to do with them. Privacy was also provided for them when answering the questionnaire. The study instrument (CAS) was validated in the study area before applying it to our respondents to ensure its validity in assessing partner violence in the study area. The questionnaire was pretested before being applied. Our study was also limited by non-inclusion of women that were not currently in relationships and people who were sick as these women might have suffered from IPV.
Conclusion
Our study shows a high level of IPV in the studied group is high. The two most common form of IPV is Emotional &/OR Harassment abuse and SCA. It is however encouraging that the majority of the students believed that IPV should be reported. We recommend appropriate management of such cases and effort made to inform the women and the general populace at large of Nigerian legislation against gender-based violence because of poor awareness seen in our study. Enablement should also be provided by the Government and NGOs to assist the victim to seek redress.
Footnotes
Author Contributions
CCA and IHA: study design, data collection/analysis, and interpretation of findings and drafting of the manuscript. BCO and ACI: interpretation of findings and drafting of the manuscript. RLE and JNE, CCI: data analysis and the interpretation of findings and drafting of the manuscript. All participated in the review of the final manuscript. All the authors approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for the study was obtained from the Health Research and Ethics Committee of the hospital.
Informed Consent
Informed written consent was obtained from the study population.
Availability of Data and Material
All data generated or analyzed during this study are included in this published article.