
Abstract
Gender disparities when delivering healthcare are attributed to gender bias and gender-related pathophysiology. We examined the interaction of gender with the provision of postoperative intensive and intermediate care. Specifically whether for major surgeries, co-morbidities and lengths-of-surgery, women receive intensive and intermediate care as often as men. A two-phase prospective study performed in an Israeli university medical center explored utilization of postoperative intensive/intermediate care. Phase 1 examined gender differences in a broad range of postoperative intensive and intermediate patients. Phase 2 examined consecutive patients undergoing major abdominal and vascular surgeries to ascertain whether for similar surgeries and co-morbidities, women were as likely as men to receive intensive/intermediate care. Phase 1 (n = 1883)—Proportionately more males were admitted to intensive/intermediate areas because they more often were trauma victims or had pre-existing ischemic heart disease. Female admissions were notable for obstetrical emergencies and post-meningioma excisions. Phase 2 (n = 796)—The proportion of males and females receiving intensive/intermediate care did not differ after specific surgeries, for example, hepatectomy, carotid endarterectomy. However, among patients with underlying ischemic heart disease men, more often than women (15% vs. 21%, p < 0.05), received intensive care after elective surgery. Although pathophysiologic differences resulted in more men than women, receiving postoperative intensive/intermediate care, gender bias might also be operative. These observations highlight the importance of considering the influence of gender when choosing a postoperative care location to insure that gender differences in the levels of care are due to pathophysiology and not gender bias.
Much recent research has focused on gender disparities in the delivery of healthcare (Theobald et al., 2017). The reasons for these disparities are multi-factorial and include differences in how men and women perceive and report illness and symptoms; misjudgment of women’s health risks; unconscious healthcare worker prejudice; and discrimination against women influenced by cultural biases (Łyszczarz, 2017). These factors can result in gender bias leading to inequalities in the access to and utilization of health services (Łyszczarz, 2017). Such gender-related differences have also been observed in Israel. Nationwide elderly-specific quality indicators showed that elderly Israeli women received lower quality primary care than men (Podell et al., 2018). Likewise, elderly Israeli Bedouin women had poorer 1-year prognosis following acute myocardial infarctions than their male counterparts (Plakht et al., 2011). Furthermore, older Israeli women had lower rates of pneumococcal and influenza immunization than men (Schwartz et al., 2013). Similar observations, were made in other countries, not only among the elderly, but among all age groups (Łyszczarz, 2017). However, it is also important to note that gender disparities in the provision of health care can also be due to the differences between the types of illnesses that occur in men and women, as well as differences in the severity and incidence of symptomatology. Furthermore, medical providers sometimes overlook or misinterpret women’s symptoms (Lawesson et al., 2018). Therefore, when investigating gender differences in the extent and outcomes of medical care it is important to consider both biases and pathophysiology.
Several, but not all, studies report that women are less likely to be admitted to ICUs (Larsson et al., 2015, 2019; Valentin et al., 2003) and have higher ICU mortality (Lipes et al., 2013; Mahmood et al., 2012). This study uniquely expands on these previous observations of gender disparities by exploring whether and how gender relates to the provision of both postoperative intensive and intermediate care services using data collected from an Israeli university medical center. This is a timely topic given modern surgery’s ability to routinely and successfully perform increasingly complex operations on elderly patients of both genders and on patients with serious underlying pathologies/injuries (Klopfenstein et al., 1998; Neuman & Bosk, 2013). The data used in this study was collected as part of a health services project aimed at identifying and developing methods to evaluate in-patient surgical care systems and then using these methods to gain administrative and clinical insights into system operations (Klein & Weissman 2002; Weissman, 2005; Weissman & Klein, 2011).
The initial phase of the study examined the differences between male and female postoperative admissions to intermediate and intensive care units. Among the objectives was exploring the hypothesis that more males than females receive such enhanced postoperative care not because of gender bias but because of the male propensity to develop severe underlying medical problems at younger ages and also have more postoperative complications, such as hemorrhages (Churnin et al., 2015; Grewal et al., 2012). Moreover, men and women display different hormonal and cytokine patterns following trauma, surgery and sepsis that may influence morbidity and survival (Guidry et al., 2014; Mörs et al., 2016).
The second phase of the study explored the hypothesis that women are less likely than men to receive intensive and intermediate care after undergoing the same types of major abdominal and vascular surgeries (such as colectomies and hepatectomies), despite the surgeries being of similar durations and the women and men having similar degrees of pre-existing co-morbidities. This hypothesis was partially based on reports that women are less likely to receive aggressive care after presenting with cardiac symptomology (Agarwala et al., 2020).
Materials and Methods
Two prospectively collected data-sets comprised of patients (>14 years old) undergoing surgery at an Israeli 745-bed tertiary care hospital and Level I trauma center were used in this study. Both data-sets included information on the patient’s preoperative medical history (surgical and underlying illnesses and American Society of Anesthesiologists (ASA) Physical Status Classification [American Society of Anesthesiologists, 1963]); on the type and extent of intraoperative care (i.e., the variables needed to calculate the Surgical Complexity Classification [Copeland et al., 1991] and Intraoperative Therapeutic Intervention Score [Klein & Weissman, 2002]); and on the postoperative course (care location immediately after surgery).
Phase 1 used a prospectively assembled data-set, previously employed to explore other aspects of postoperative intensive and intermediate care, such as the demographic and clinical differences betweem elective and emergency surgery patients (Weissman & Klein, 2008a, 2008b). This data-set contains information from three cohorts of consecutive adult surgical patients receiving postoperative intermediate and intensive care (Weissman & Klein, 2008a, 2008b). The cohorts included patients admitted over 9 months to the cardiothoracic ICU, over 10 months to the neurosurgical ICU, and over 18 months to either the General ICU (mainly surgical patients [GICU]) or for intermediate (INT) care stays. The data collection periods for the cohorts entering the cardiothoracic ICU and neurosurgical ICU were shorter because the patients were relatively homogenous and provided sufficent data to characterize these two patient groups. The GICU and intermediate care cohorts were more heterogeneous and thus were studied for longer periods to facilitate a better understanding of such diverse groups and facilitating examining subgroups. Cohorts and not larger populations were studied because of the large quantity of information per patient. The location of care immediately after surgery was decided by the treating anesthesiologists and surgeons. There are written admission criteria for extended intermediate and GICU admissions based on the American College of Critical Care Medicine (1998) Practice Parameters which are the framework, but not the absolute guidelines, for physician decisions (Nasraway et al., 1998). Analysis of this dataset focused on testing the hypothesis that men do not receive enhanced postoperative care more frequently than women because of gender bias, because males are predisposed to develop severe underlying medical problems at younger ages than females and also develop more postoperative complications.
Phase 2 was performed after Part 1 showed few gender-related differences among intermediate and GICU patients who had undergone elective and non-trauma emergency surgery. Data were prospectively collected over 4 months on a broader (not just those receivng intermediate and intensive care) consecutive group of patients undergoing major abdominal and vascular surgery, that is, no trauma victims were included. Data collection began 18 months after completion of Phase 1’s data collection. To allow for more detailed data analysis additional perioperative evaluation measures were used to better describe each patients’s underlying medical problems. The additional preoperative information included the Revised Cardiac Risk Index (Lee et al., 1999) and Charlson Co-Morbidity Index (Charlson et al., 1987) while the additional post-operative information included the post-operative day 1 Acute Physiologic and Chronic Health Evaluation II (APACHE II) and Therapeutic Intensity Scoring System (TISS) (Cullen et al., 1974; Knaus et al., 1985). Sources were patient charts and the surgeons, anesthesiologists, and nurses caring for the patient. ICU and hospital lengths of stay were obtained from hospital discharge summaries, as was mortality data. Analysis of this more detailed data-set examined the hypothesis that for specific types of major surgeries, co-morbidities, and lengths-of-surgery, women are less likely than men to receive intensive and intermediate care.
The Surgical Complexity Classification was adapted from the POSSUM audit score (Copeland et al., 1991): Minor surgery (1 point)—for example, dilation & curettage, tooth extraction, cataract extraction, incision and drainage of rectal abscess; Moderate surgery (2 points) —for example, appendectomy, cholecystectomy, mastectomy, transuretheral resection of prostate, open reduction, and internal fixation of hip or long bone fracture; Major surgery (4 points) —for example, laparotomy, bowel resection, cholecystectomy with choledochotomy, peripheral vascular procedure, major amputation posterior spine fusion, abdominal hysterectomy; Major surgery plus (8 points) —for example aortic procedure, abdominal-perineal resection, pancreatic or liver resection, esophagogastrectomy, craniotomy, cardiac surgery, anterior-posterior spine fusion/instrumentation.
Statistical Analysis
The nature of the data distributions was examined with the Kolmogorov-Smirnov test. Normally distributed data are presented as mean ± SD. For continuous variables, intergroup (males vs. females) differences were examined with two-tailed Students t-tests. The central tendency of continuous, non-normally distributed data are reported as medians and analyzed using non-parametric statistics, such as the Wilcoxon rank sum test. Categorical data were presented as relative percentages and compared using Chi-square tests. P values < 0.05 were considered to indicate statistical significance.
We used multivariate regression analysis to determine whether gender was an independent determinant of postoperative care intensity (TISS) during any of the two Phases of the study. Logistic regression was used to ascertain whether gender was a factor in receipt of intensive, intermediate or floor care immediately after surgery. Two models were tested, GICU/INT versus floor and GICU versus INT/floor care. Only variables with p < 0.1 upon univariate analyses were included in the multivariate logistic analysis. Data were analyzed with Systat version 12 (Systat Softwae Inc. San Jose, CA).
The Institutional Review Board of the Hadassah Medical Organization approved this research. Because of its observational nature informed consent was waived.
Results
Phase 1
Demographic data
Phase 1 included 1,883 postoperative patients and supported the hypothesis that more males than females received enhanced postoperative care because of the male propensity to develop severe underlying medical problems at younger ages and not because of gender bias. Specifically, more males underwent cardiothoracic surgery (elective—71% males, emergency—68% males) so that the cardiothoracic ICU population was predominantly male. Eighty percent of the males underwent coronary artery bypasses while a great proportion of the females had valve replacements (Table 1). Among the emergency intensive/intermediate care patients 47% of the males, but only 22% of the females, were trauma victims (Tables 2 and 3). Men were more often the victims of gunshot and stab wounds and were more severely injured as evidenced by a higher admission rate to the GICU, higher incidence of postoperative mechanical ventilation and a higher mortality rate (Table 3).
Elective Cardiac and Neurosurgery: Male Versus Female Patients (Phase 1).
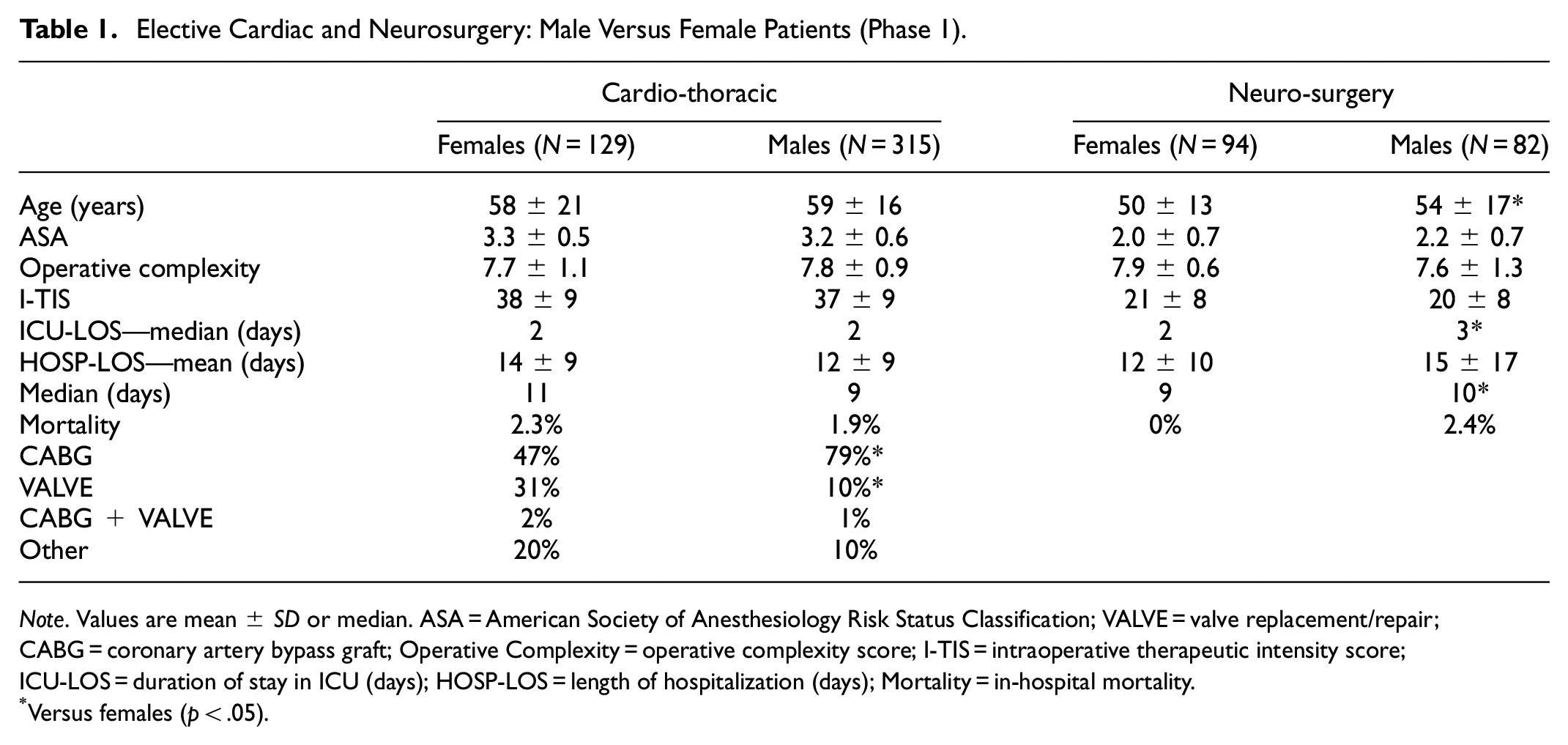
Note. Values are mean ± SD or median. ASA = American Society of Anesthesiology Risk Status Classification; VALVE = valve replacement/repair; CABG = coronary artery bypass graft; Operative Complexity = operative complexity score; I-TIS = intraoperative therapeutic intensity score; ICU-LOS = duration of stay in ICU (days); HOSP-LOS = length of hospitalization (days); Mortality = in-hospital mortality.
Versus females (p < .05).
INT/GICU Patients: Males Versus Females (Phase 1).

Note. Values are mean ± SD or median. ASA = American Society of Anesthesiology Risk Status Classification; IHD = history of ischemic heart disease; PCI = percutaneous coronary intervention; Operative Complexity = operative complexity score; I-TIS = intraoperative therapeutic intensity score; ICU = percent of patients admitted to an ICU. The remainder received INT care; HOSP-LOS = length of hospitalization (days).
Versus females (p < .05).
Trauma Victims: Males Versus Females (Phase 1).

Note. Values are Mean ± SD. I-TIS = intraoperative therapeutic intensity score; ICU = percent of patients admitted to the GICU. The remainder received intermediate care.
Versus females (p < .05).
Comparison of Specific Surgeries (Phase 2).

Note. Values are mean ± SD or median. CEA = carotid endarterectomy; ASA = American Society of Anesthesiology Risk Status Classification; RCRI = revised cardiac risk index; Charlson = Charlson co-morbidity score; INT = intermediate care—Stay of >12 hours in PACU; IHD = history of ischemic heart disease; PCI = percutaneous coronary intervention; I-TIS = intraoperative therapeutic intensity score; HOSP-LOS = length of hospitalization; TISS = therapeutic intervention scoring system.
Versus females (p < .05).
Descriptive analysis
Gender differences due to different pathological processes were found among patients undergoing elective neurosurgery. Females were younger and had shorter ICU stays because more women (n = 42) than men (n = 21) underwent craniotomies for meningiomas, an extra-parenchymal tumor (Table 1). Males generally underwent surgery for intraparenchymal tumors resulting in longer ICU stays. Additionally, 31 women received intensive/ intermediate care because of complications (e.g., pre-eclampsia and hemorrhage) following ceaserean section
Among the non-trauma emergency surgery patients a greater proportion of male than female patients received ICU rather than intermediate care (Table 2). This higher percentage of male patients was associated with a greater incidence of ischemic heart disease and prior cardiac surgery/percutaneous coronary interventions among the men.
Logistic regression analysis
Logistic regression analysis of the elective surgery patients showed that gender was not among the determinants of receiving GICU, as opposed to intermediate care, while age, Intraoperative Therapeutic Intensity Score, ASA Classification, and Surgical Complexity were determinants. In the analysis of emergency surgery patients, both an elevated Intraoperative Therapeutic Intensity Score and male gender were determinants of GICU care.
Phase 2
Phase 2 included 796 patients (on retrospective calculation this sample size was sufficient, to a power of 0.80, to differentiate a 6% difference between male and female ICU admissions). and tested the hypothesis that for specific types of major abdominal and vascular surgeries, co-morbidities and lengths-of-surgery, women are less likely than men to receive intensive and intermediate care (Table 4). As a group, the women who underwent elective surgery received proportionately more intermediate/intensive care because more of them received such care after undergoing colectomies. This greater female proportion was despite the males being older than the females (63 ± 14 (SD) vs. 60 ± 16 years, p < 0.05) and having more pre-existing medical problems as evidenced by significantly higher Charlson Co-Morbdity Indices (3.8 ± 2.2 vs. 4.5 ± 2.3, p < 0.05) and Revised Cardiac Risk Indices (median 0 vs. 1, p < 0.05).
Multivariate linear and logistic regression analyses
Multivariate linear regression analysis (overall r = 0.62) of these elective surgery patients, with the extent of postoperative care measured using TISS as the dependent variable, found that gender was not a significantly associated factor (p < 0.07) while ASA Classification, length of surgery, Revised Cardiac Risk Index, and Charlson Index were significant determinants (p < 0.01). Among emergency surgery patients, age, ASA Classification, and length-of-surgery were significant associated factors (p < 0.001), while gender again was not significant (p < 0.07). Furthermore, logistic regression analysis showed gender was not associated with the location of postoperative care (Supplemental Table 1). Therefore, overall we did not detect evidence of gender-related differences in the receipt of intensive/intermediate care.
Descriptive analysis
Overall, 40% of men, but only 19% of women undergoing elective surgery had histories of ischemic heart disease, while among the emergency surgery patients there were only minimal differences (females—27%, males—32% [Table 5]). With advancing age, males, as opposed to females, had significantly higher Revised Cardiac Risk, but not Charlson Co-Morbidity Indices, reflecting the greater incidence of ischemic heart disease among males (Table 6). However, female elective surgery patients with ischemic heart disease were less likely to receive intensive care than their male counterparts despite having similar I-TIS scores (Table 5).
Comparison of Male and Females: Ischemic Heart Disease and Vascular Surgery (Phase 2).

Note. Values are mean ± SD or median. ASA = American Society of Anesthesiology Risk Status Classification; RCRI = revised cardiac risk index; PCI = percutaneous coronary intervention; Charlson = Charlson co-morbidity score; I-TIS = intraoperative therapeutic intensity score; HOSP-LOS = length of hospitalization; TISS = therapeutic intervention scoring system.
Versus females (p < .05).
Versus vascular surgery (p < .05).
Versus female vascular surgery (p < .05).
Versus female other surgery (p < .05).
Gender Comparison by Age: Elective Surgery (Phase 2).

Note. Values are Mean ± SD [Median]. ASA = American Society of Anesthesiology Risk Status Classification; Charlson = Charlson co-morbidity score; IHD = history of ischemic heart disease; RCRI = revised cardiac risk index; Op Comp = operative complexity score; I-TIS = intraoperative therapeutic intensity score; HOSP-LOS = length of hospitalization; TISS = therapeutic intervention scoring system; HTN = history of hypertension; DM = diabetes mellitus.
Versus females (p < .05).
Discussion
This study had much patient population breadth since it encompassed many types of surgeries and examined gender differences from a variety of perspectives. Although, there were demographic and clinical differences and similarities between men and women undergoing major surgery, the study showed that many of the disparities in the provision of intensive/intermediate care were due to pathophysiological differences although there was a possibility of gender bias among women with ischemic heart disease.
Phase 1
After surgery proportionately more males (58%) than females (42%) received postoperative intensive/intermediate care, as also noted by others (Wichman et al., 2000). This male preponderance was due to the greater severity of both the primary surgical problem and pre-existing diseases. Young males were the predominant victims of major trauma, which is attributed in part to their risk-taking behavior (Mitchell et al., 2012; Olajumoke et al., 2014; Turner et al., 2003). Although, over the past few decades more females have become trauma victims sustaining injuries of similar magnitude to those of men as reflected in the present study where about a third of trauma victims were women (Wohltmann et al., 2001). However, the men received more intensive intraoperative therapy, more frequently were admitted to the ICU (60%–40%), stayed there longer and had twice the mortality rate. The latter may be due to more severe injuries but may also be due to physiologic gender differences that reportedly resulted in lower mortality rates among female trauma victims younger than 50 years (Wohltmann et al., 2001). Additionally, male gender was associated with higher case fatality rates when stratified by age, but not by injury type or severity (Sethuraman et al., 2014). The longer ICU stay in males may reflect their increased propensity to develop post-injury pneumonia, although females had a higher mortality risk if they contracted post-trauma pneumonia (Gannon et al., 2004; Napolitano et al., 2001; Sharpe et al., 2014).
Besides more often being trauma victims, men received proportionately more postoperative intensive and intermediate care than women due to their undergoing more vascular surgery, especially open aortic surgery, and a higher incidence of ischemic heart disease (41% vs. 32%). The latter was also demonstrated by the greater proportion of cardiac surgery patients being male and that men by and large underwent CABG rather than pure valve replacement/repair surgery (Manjunath et al., 2014; Swaminathan et al., 2016). The higher incidence of ischemic heart disease among males was among the factors associated with their receiving more intensive, rather than intermediate, care after major elective and emergency non-cardiac surgery. The consequences of these observations is that in medical centers with few or no trauma admissions a significant proportion (53%) of the population receiving intensive or intermediate care following surgery would be males over 50 years old. This is consistent with other observations which noted that, compared to females, male postoperative ICU patients had greater mortality (especially those ≥75 years), longer ICU stays, and utilized more ICU resources (Reinikainen et al., 2005; Riccardi et al., 2011; Shahan et al., 2015). Such differences were not observed among medical ICU patients (Harten et al., 2005). In another study of patients undergoing emergency surgery, 30-day mortality was higher in males and was associated in both genders with increasing complexity of surgery and in men, also with increasing age and seniority of the anesthesiologist (Harten et al., 2005). The results of Phase 1 thus strengthen the hypothesis that more males than females received enhanced postoperative care because of the male propensity to develop severe underlying medical problems at younger ages and not because of gender bias.
Conversely, there were instances of female predominance due to pathophysiologic differences between men and women. A prime example was that meningiomas were more common among elective female neurosurgery patients. The preponderance of meningiomas in women is a well-recognized, but poorly understood, phenomenon (Baldi et al., 2018; Kuratsu & Ushio 1996; McCann, 2000; Wanis et al., 2021). Furthermore, some of the women who had undergone cesarean sections due to severe pre-eclampsia or uterine hemorrhage received intensive/intermediate care (Chantry et al., 2015; Guntupalli et al., 2015; Padilla et al., 2021; Yi et al., 2018). This observation is consistent with those of Hazalgrove et al. (2001) who noted that 1.8% (210 of 11,385) of admissions to 14 British ICUs were from obstetric services and that 0.17% to 0.73% of all deliveries were admitted to an ICU mainly for treatment of pre-eclampsia and hemorrhage. Therefore, active high-risk perinatology services can impact the demand for critical care beds (Hazalgrove et al., 2001; Quah et al., 2001).
Phase 2
Phase 2, like Phase 1 did not reveal overt gender bias. The latter was demonstrated by both multivariate and logistic regression analyses that did not find gender as an independent variable associated with the intensity of postoperative care (TISS) nor its location (intensive care unit, intermediate unit or floor). However, Phase 2, which focused only on major abdominal and vascular surgery, did show evidence that gender might have influenced the provision of intensive, as opposed to intermediate care, among patients with a history of ischemic heart disease. A higher proportion of male elective surgery patients (21% vs. 15%) with ischemic heart disease received intensive care despite similar Intraoperative Therapeutic Intensity Scores and TISS. Among, the reasons might have been the longer surgeries and higher incidence of COPD among the males, but might also be due to subjective factors, including gender bias (de Marvao et al., 2021). These observations support part of our hypothesis, that for certain co-morbidities, women are less likely than men to receive intensive and intermediate care. The observations also appear consistent with our thesis that women receive less aggressive care after presenting with cardiac symptomatology or history. Women are said to suffer from “under-recognition, under-diagnosis, and under-treatment” of coronary artery disease (Trutter et al., 2020). Further evidence for this thesis was demonstrated by a greater percentage of men having previously undergone coronary artery bypass surgery (30% vs. 6%) while more women had had previous percutaneous coronary interventions (50 vs. 36%). The greater use of percutaneous coronary interventions in females is consistent with other studies and might be attributed to the greater mortality after CABG reported among females by some, but not all, investigators (Basaran et al., 2007; Blankstein et al., 2005; Robinson et al., 2021; Ouzounian et al., 2013). Women and men have comparable benefits from percutaneous interventions while post-coronary artery bypass surgery morbidity is more common in females than males, especially if they are diabetic (Kardys et al., 2007; Mikhail et al., 2010; Ritchison et al., 2007).
Male elective surgery patients had more underlying cardiac disease (40% vs. 19%) and COPD (19% vs. 12%) as illustrated by a significantly higher Charlson Co-Morbidity Index, Revised Cardiac Risk Index, and mortality. Furthermore, when stratified by age, there were no age-associated gender differences in the incidence of hypertension, but ischemic heart disease was more common among men and occurred at an earlier age. These findings are expected given that the greater severity of atherosclerosis in males is especially prominent in coronary arteries, less so in carotid arteries and not as apparent in the aorta and peripheral vessels (Matyal, 2008). The higher incidence and earlier age of onset explains the greater use by males of postoperative intensive and intermediate care. Females tend to develop ischemic heart disease later in life and have a worse prognoses than men, attributed to narrower coronary arteries and more frequent diastolic dysfunction (Blankstein et al., 2005; de Marvao et al., 2021; Matyal, 2008; Porter et al., 2020). It is important to note that in the current study, ischemic heart disease was recorded as present on the basis of prior medical history. However, much ischemic heart disease in women goes undetected because coronary artery disease often has an atypical or silent clinical presentation. As a result, they are less likely to undergo diagnostic tests and therapy for coronary artery disease (Fox, 2008; Hessian et al., 2018).
When specific operations were examined, for example, hepatectomy and open carotid endarterectomy, there were no gender differences in the proportion of males and females receiving intensive and intermediate care nor were there differences in the intensity of postoperative care as measured by TISS. These observations are especially important since there are reports that under certain circumstances the extent of care afforded women was less than that provided men (Agarwala et al., 2020; Kent et al., 2012). Among elective hepatectomy patients the only gender-related differences were that the men had more underlying cardiac disease, hypertension, and COPD. However, the females had a slightly higher mortality rate which is in contradistinction to studies showing that the female liver is more tolerant to stress and not consistent with the observation that males are at greater risk for post-hepatectomy mortality (Virani et al., 2007; Yokoyama et al., 2007). However, compared to colectomy and carotid endarterectomy patients, hepatectomy patients were younger because they underwent a strict selection process that eliminated those with significant preexisting medical conditions. Therefore, the male hepatectomy patients had less cardiac disease and lower ASA Classifications than males undergoing colectomy and vascular surgery. Carotid endarterectomy patients differed from the colectomy and hepatectomy patients in that a greater proportion of both male and female patients had ischemic heart disease, COPD, diabetes, and hypertension that translated into higher ASA Classifications and Revised Cardiac Risk Index. This is not surprising given the close association of carotid with coronary and peripheral vascular atherosclerosis (Hertzer et al., 1985). Previous studies reported that women undergo endarterectomies less often than men. However, in some, but not all, studies women have higher rates of post-endarterectomy TIA, strokes, and mortality (Akbari et al., 2000; James et al., 2001; Sarac et al., 2002; Stelągowski et al. 2017).
Limitations
This study was performed in a single tertiary care institution and thus reflects that institution’s clinical practices and operational realities. An institution’s perioperative care is greatly influenced by its facilities, staffing, clinical and administrative practices, and the types and volume of surgery performed. The level of nursing and physician care provided on hospital floors also determines the acuity of postoperative patients that are referred for postoperative intensive and intermediate care (Coggins, 2000). Furthermore, Israel has universal healthcare for all its citizens so that hospital and physician reimbursement were not issues.
A further limitation was the study’s observational and non-critical nature. It recorded and analyzed existing hospital staff practices and was not designed to examine whether their decisions were justified. Yet, despite these limitations the study provides much information about the differences and similarities between men and women undergoing surgery. Such information is useful in and of itself and importantly can serve as the basis for designing future investigations.
Conclusions
Previous studies performed in Israel showed evidence of gender disparities within the healthcare system, as well as in other segments of society (Bental et al., 2017; Plakht et al. 2020; Podell et al., 2018). The present study demonstrated that although pathophysiologic differences resulted in men, more often than women, receiving postoperative intensive/intermediate care in some, but not all, situations gender bias was also operative. These observations thus highlight the importance of considering the influence of gender when examinng the provision of healthcare and if disparities are observed, discerning whether they are due to pathophysiological differences or gender bias.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440231153044 – Supplemental material for The Impact of Gender on the Postoperative Consumption of Intensive and Intermediate Care Resources
Supplemental material, sj-docx-1-sgo-10.1177_21582440231153044 for The Impact of Gender on the Postoperative Consumption of Intensive and Intermediate Care Resources by Charles Weissman in SAGE Open
Footnotes
Acknowledgements
The author would like to thank Nava Klein RN for her efforts in the collection of the data.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Israel National Institute for Health Policy and Health Services Research [1998/6/a].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.