
Abstract
The obesity pandemic is increasingly threatening Asian populations. This is especially so for children from higher-income countries, such as Singapore. Among the various driving factors of obesity, parents’ health knowledge, attitudes, and practices are underexplored. The present study uses a nationally representative sample of 1,491 responses from Singapore to investigate parental knowledge, attitudes, and practices (KAP) about childhood obesity. Latent class analysis (LCA) on parents’ responses to the KAP survey reveals four unique parenting patterns: the limited knowledge group, the group with negative attitudes, the best practice group, and the limited practice group. Children of families in the best practice group are shown to have the lowest obesity risk. Furthermore, statistically significant variations in parental subgroups are found across several socio-economic factors. For example, parents with positive responses to all KAP variables tend to be younger, have a higher household income, do not work full-time, and live in a separate household from the children’s grandparents. The findings may provide important policy implications for targeted preventative interventions for parents whose children may face higher obesity risks.
Keywords
Introduction
Childhood obesity has been established as a major health crisis, threatening the health and well-being of children worldwide (Karnik & Kanekar, 2012). From 1975 to 2016, the global rate of childhood obesity increased from 4% to 18% (WHO, 2018). While studies have found that the rising trend of children’s and adolescents’ BMI in high-income countries has been plateauing since 2000, the BMI of children and adolescents has accelerated in Asia (Abarca-Gómez et al., 2017). For example, China and India are expected to be the top two countries with the highest number of obese children by 2030, with projections of about 62 million and 27.5 million obese children, respectively (World Obesity Federation, 2019). In Singapore, where the Chinese, Malays, and Indians account for the majority of the population, the prevalence of childhood obesity has been one of the core issues on the agenda of policy-makers (Singapore Ministry of Health, 2020; Tan & Sinaram, 2014). A recent survey showed that 13% of Singaporean children aged between 6 and 18 in mainstream schools are overweight (Lee, 2018), which is alarming when compared with Singapore’s neighboring countries such as Cambodia (2%), Indonesia (12%), Malaysia (7%), Myanmar (3%), Thailand (11%), and Laos (2%) (Lindsay et al., 2017). Comparing the situation to 1976, when the childhood obesity rate of primary school students was below 3%, 17.39% of male and 13.07% of female Primary-5 students are overweight (BMI ≥90th percentile) in 2019 (Karuppiah et al., 2021). Such trends are particularly concerning as existing literature has established a strong association between childhood obesity and obesity in adulthood, wherein 36.2% of Singapore adults aged 18 to 69 are overweight nowadays (Guo & Chumlea, 1999; Lee, 2018; Reilly & Kelly, 2011).
Parents’ health-related knowledge, attitudes, and practices play a crucial role in children’s body weight management (Birch & Davidson, 2001; Mabiala Babela et al., 2016; Rausch et al., 2015; Straughan & Xu, 2022). With obesity being notoriously resistant to treatment (Spear et al., 2007), researchers recommend that obesity prevention start early from childhood (Baidal & Taveras, 2012). Additionally, greater attention needs to be placed on parents as they are most commonly the primary caregivers of young children. As caregivers, parents create a contextual environment that influences the child’s dietary and physical activity habits (Birch & Davidson, 2001; Faith et al., 2001). Parenting practices significantly affect their child’s nutritional patterns through nutrition knowledge and feeding practices (Benton, 2004; Lim et al., 2020; Patrick & Nicklas, 2005; Savage et al., 2007). These dietary patterns formed in childhood have been studied to remain consistent and to continue into adulthood (Mikkilä et al., 2005). Furthermore, parental factors significantly influence children’s physical activities (Gustafson & Rhodes, 2006; Jacobi et al., 2011). Children tend to participate in more physical activities when parents are supportive and encourage such behaviors (Pugliese & Tinsley, 2007). Moore et al. (1991) found that a child is 5.8 times more likely to do physical exercise if both parents actively participate in physical activity. Similarly, parents’ and children’s sedentary behaviors are positively correlated (Cillero & Jago, 2010; Wagner et al., 2004). Therefore, examining parental knowledge, attitudes, and practices about childhood obesity would be instrumental in the efforts to curb obesity (Tinsley, 2003).
In the past few decades, the Knowledge, Attitude, and Practice (KAP) survey has been widely used to understand individuals’ health-seeking behaviors and evaluate the effectiveness of public health programs (Hausmann-Muela et al., 2003; Launiala, 2009; Manderson & Aaby 1992). For example, Mabiala Babela et al. (2016) use the KAP framework to assess parents’ obesity-related KAP in Congo; Rausch et al. (2015) examine the government-led health intervention programs’ impact on American parents’ knowledge, attitudes, and behaviors of nutrition and physical activity. Nevertheless, few studies focus on parental knowledge, attitudes, and practices (KAP) about childhood obesity within an Asian context. Besides, existing studies failed to demonstrate the relationships between Asian parents’ KAP and childhood obesity within a socio-cultural context (Launiala, 2009; Ratcliffe, 1976). There is an urgent need to investigate Asian parents’ KAP about childhood obesity and how obesity-related KAP relates to socio-economic factors.
This study has two objectives. The first is to examine parents’ obesity-related KAP profiles using latent class analysis (LCA). The second is to identify whether the different parenting groups are affected by various socio-economic factors. This paper begins with a review of the KAP framework. In the following section, we describe the data collection, variables, analysis, and results. The discussion section concludes with the theoretical and practical implications of the findings.
A Brief Review of the KAP Framework
The Conceptual Framework of KAP
The Knowledge, Attitudes, and Practices (KAP) survey, also referred to as the Knowledge, Attitudes, Belief, and Practices (KABP) survey, is a methodological instrument that was first developed as a means to understand family planning practices around the world (Cleland, 1973; Ratcliffe, 1976). The methodological model has, however, been widely used to understand health behavior and health-seeking practices (Hausmann-Muela et al., 2003; Manderson & Aaby, 1992).
The KAP survey framework primarily measures, as the name suggests, three aspects of health behavior (Hausman-Muela et al., 2003; Launiala, 2009): (1) The knowledge that individuals have regarding health information, mainly referring to knowledge of biomedical concepts regarding health (Pelto & Pelto, 1997); (2) The attitudes that individuals hold toward an issue defined as “a learned predisposition to think, feel and act in a particular way towards a given object or class of objects” (Ribeaux & Poppleton, 1978); and (3) The practices that individuals partake in, with regards to addressing an issue, typically referring to the “preventive measures or different health care options” that individuals utilize (Hausman-Muela et al., 2003). Some studies using the four-dimension framework also include individuals’ beliefs about an issue, primarily defined in contrast to knowledge and attitudes as “traditional ideas, which are erroneous from the biomedical perspective, and which form obstacles to appropriate behavior and treatment-seeking practices” (Launiala, 2009).
Within the framework, the former two or three components can either be coherent with each other or conflicting. For example, knowledge, attitudes, and beliefs can be seen to work together to share the practices (Friedman & Shepeard, 2007; Launiala, 2009), while knowledge and beliefs/attitudes can also contrast each other as seen in the biomedical perspective versus traditional ideas dyad (Good, 1994; Pelto & Pelto, 1997).
The Application of the KAP Survey Framework
Scholars have utilized the KAP survey framework to understand a diverse range of health behaviors worldwide (Hausmann-Muela et al., 2003; Manderson & Aaby, 1992). Within its application in health studies, KAP surveys are predominantly used to “collect data on what is known, believed and done about a particular topic.” They help to “plan, implement and evaluate programs and can identify knowledge gaps, cultural beliefs, or behavioral patterns that may facilitate or impede the success of a program” (Zahedi et al., 2014). One study by Haji-Mahmoodi et al. (2002) utilized the model to understand the factors that shaped breast self-examination behavior amongst female health care workers in Tehran, Iran. Jette et al. (2003) utilized the model to understand the relationship between the knowledge, attitudes, and beliefs surrounding the use of evidence in practices and its actual use amongst physical therapist members of the American Physical Therapy Association (APTA). Such studies have also had policy implications and have identified particular areas for intervention for potential policies to affect behavioral change.
Determinants of KAP
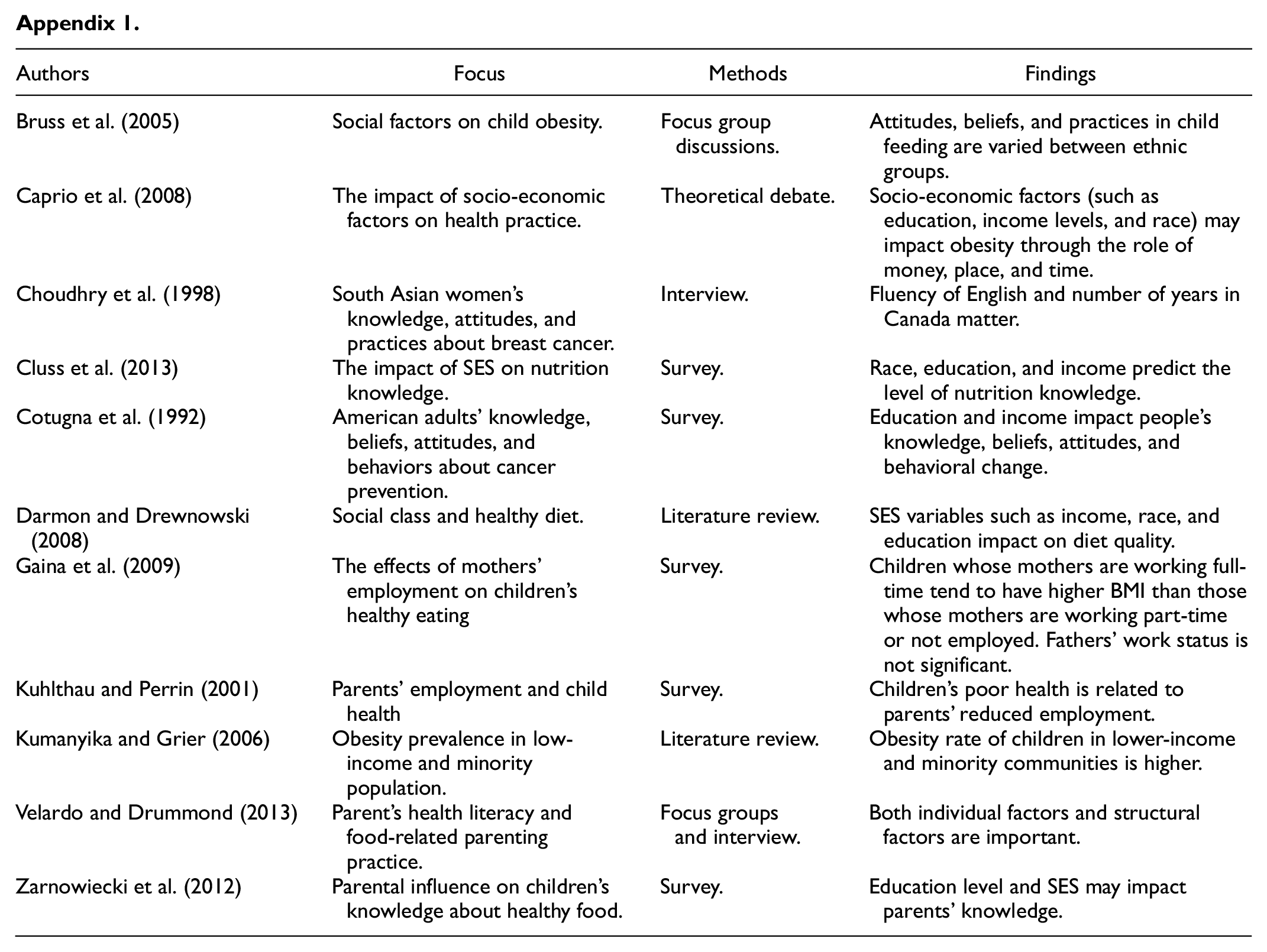
Previous literature has explored the various determinants of individuals’ knowledge, attitudes, and practices (Studies reviewed in this part are listed in Appendix 1). In terms of health knowledge, an individual’s income, race, and education level have been shown to affect the level of health knowledge an individual might have (Cotugna et al., 1992; Darmon & Drewnowski, 2008; Kumanyika & Grier, 2006). A study by Cluss et al. (2013) conducted in the U. S. with 135 low-income parents of obese children found that parents with a lower income (p = .03), lower education level (p = .02), and who were black (p = .02) have poorer nutrition knowledge than parents who possess a higher income, higher education level, and are non-black. Additionally, a study by Zarnowiecki et al. (2012), based in Australia involving 192 five to six years old children and their parents, illustrated how socio-economic status (SES) and educational levels associate with the different ways parents think of a child’s health. While parents of a low SES are more likely to think of the behavioral aspects of health, parents of a high SES are more likely to think of health in scientific measures.
Regarding the determinants of beliefs and attitudes, an individual’s cultural background has been identified as a key factor that shapes the former. Caprio et al. (2008) argues that ethnic groups in the U. S. hold distinct cultural values and health beliefs. In particular, African American women and white women have different perceptions regarding the ideal body size. Notably, the coordinated management of meaning (CMM) model conceptualizes how culture shapes particular health beliefs of individuals, ranging from family traditions to cultural values at the societal level (see Bruss et al., 2005).
Health practices can be conditioned by many socio-economic factors, such as parents’ age, employment, income, race, and education (Bruss et al., 2005; Caprio et al., 2008; Cotugna et al., 1992; Darmon & Drewnowski, 2008; Gaina et al., 2009; Kuhlthau & Perrin, 2001; Straughan & Xu, 2022). For example, Gaina et al. (2009) indicate that mothers’ working status significantly impacts children’s eating patterns while fathers’ employment does not, which implies that mothers and fathers may play a different role in children’s obesity. While KAP is understood as translating knowledge and attitudes (KA) to specific behavioral or practice outcomes, scholars have argued that other structural factors need to be taken into account when examining the relationship between KA and actual practices (Baum & Fisher, 2014). For instance, Velardo and Drummond (2013) argue that it is crucial to consider “individualistic behavioral approaches” to health intervention and take into consideration structural influences to avoid an exclusive focus on individual agency. Other studies illustrate this as well; a study with 22,043 adults on cancer prevention KAP found that only 35% of respondents reported dietary change, though 90% agreed that diet and disease were related (Cotugna et al., 1992). Another study on Asian Canadians showed that South Asian women generally had limited breast cancer knowledge and did not engage in breast cancer detection practices (e.g., Only 21% of the women knew that detecting breast cancer was essential, and 47% had never done a breast examination; Choudhry et al., 1998). Scholars should thus be aware that while strong, the relationships between knowledge, attitudes, and practices may be influenced by various socio-economic factors. Therefore, the present study will include age, gender, education, income, occupational status, household structure, and ethnicity to better understand parents’ KAP.
The Present Study: Applying KAP to Understand Childhood Obesity
The above literature provides a basic understanding of the KAP framework and what factors impact an individual’s KAP. The present study employs the KAP framework to understand the parental influence on childhood obesity. We first collected data from a questionnaire survey on Singaporean parents to assess parents’ KAP. Latent class analysis (LCA) is then used to identify different parenting groups based on parents’ KAP profiles. Lastly, we examined how parents’ socio-economic factors impact parents’ obesity-related KAP via regression analysis.
Methods
Participants
A questionnaire survey was conducted in Singapore between June and November 2018. A random list of 2,500 household addresses were provided by the Department of Statistics in Singapore. About 2,116 households with at least one child under 14 years old were selected for our study. For each selected household, we invited either the father or mother of the child to answer the questionnaire. Written informed consent was obtained from all participants before the survey. It took about 10 to 15 minutes to complete each survey. Our research team visited 2,108 households and received 1,488 valid responses. Of the sample, 66.1% of the respondents are female, 60.8% are below 41 years old, 61.2% are Chinese, 20.2% are Malay, 18.6% are Indian, and 72% are staying in a four-room or five-room HDB apartment. Regarding education, 40.4% of the respondents have a bachelor’s degree, 33.3% have a post-secondary diploma, and 26.3% have a secondary education and below.
Variables
Knowledge, Attitudes, and Practices
We first searched for available scales from the existing empirical studies. Then the research team created a new KAP scale since there are no suitable measures for parental obesity-related KAP for the present study. Although one study by Mabiala Babela et al. (2016) provides a KAP scale, the scale was not validated and designed for parents’ obesity-related KAP. Besides, their scale contains 30 items that are too complicated to be used for latent class analysis for this study. Thus, the research team generated a shortened list of items to capture parents’ KAP of childhood obesity (see Table 1). After careful discussion by the research team, we chose three items for each KAP subscale. The knowledge subscale was adapted from questions about knowledge of healthy eating in Etelson et al. (2003) which explores parents’ knowledge of the nutritional value of foods and what constitutes a healthy diet (Etelson et al., 2003; Parmenter & Wardle, 1999). The attitude subscale was modified from the measures of concern about child weight in Birch et al. (2001) which captured parents’ concern about the impact of childhood obesity. Following the recommendations by Singapore Health Promotion Board (2016), obesity interventions should include healthy eating and physical activities. Thus, we measured practice using three items that capture parents’ management of children’s healthy eating and physical activities (Lim et al., 2020). In the questionnaire, all KAP items were rated by a four-point Likert scale (1 = “Strongly disagree,” 2 = “Disagree,” 3 = “Agree,” and 4 = “Strongly agree”). Tests of construct validity and reliability of the KAP scale were introduced in the following sections before we proceeded into further analysis. We recoded all KAP items into dichotomous variables when they were used for latent class analysis (e.g., “1” and “2” were coded as “0”; “3” and “4” were coded as “1”). However, the three items measuring attitudes (e.g., a1, a2, and a3) and one item of knowledge (e.g., k2) were coded reversely (e.g., “Disagree” and “Strongly Disagree” are coded as “1”). Table 1 shows that (1) the percentage of the participants whose knowledge is satisfactory ranges from 73.59% to 85.47% in the three knowledge items, (2) the percentage of the cases whose attitudes are positive ranges from 83.12% to 84.31%, and (3) the percentage of the cases with good practices ranges from 64.15% to 79.79%.
The KAP Scale Items.

Note. Item k2 and a1 to a3 are reverse-coded questions. The values in the last column are the percentage of “Yes = 1” answers.
Socio-Economic Factors
Based on the literature review above, we selected a list of explanatory variables including age, gender, ethnicity, marriage status (1 = married; 0 = never married, divorced, or widowed), education (1 = Below secondary, 2 = Secondary, 3 = Post-secondary, and 4 = Bachelor and above), household income, residence type (1 = 1-room to 3-room public housing, 2 = 4-room to 5-room public housing, and 3 = private house such as a condo or landed house), work status (1 = not working, 2 = working part-time, and 3 = working full-time), number of household members, whether living with parents (1 = Yes, and 0 = No), and whether domestic helpers were hired (1 = Yes, and 0 = No). These variables served as important predictors of class memberships in the four regression models.
Analysis
Confirmatory Factor Analysis (CFA)
Since the KAP scale in the present study is newly generated within a Singaporean context, it is necessary to examine its construct validity before we proceed to additional analysis. We employ CFA rather than exploratory factor analysis (EFA) since KAP is a relatively established framework (Hurley et al., 1997). According to KAP, our hypothesized CFA model includes three dimensions and each dimension contains three items (see Figure 1). We use the asymptotic distribution-free (ADF) method to estimate the CFA model (Xu & Chen, 2021). Multiple goodness-of-fit indices are used to assess the model fit: chi-square to the degree of freedom ratio (χ2/df), root means squared error of approximation (RMSEA), standardized root means squared residual (SRMR), and comparative fit index (CFI). It is commonly agreed that values below .08 for RMSEA, values less than .08 for SRMR, and values of CFI greater than .90 indicate a good model fit (Chen et al., 2018; Gagné et al., 2010; Kenny, 2015; MacCallum et al., 1996). Scholars also suggest that a value of SBχ2/df lower than 3 indicates a good fit (Kline, 2015).

Results of confirmatory factor analysis.
Latent Class Analysis (LCA)
The purpose of LCA is to identify the underlying subgroups of parents with different KAP profiles. Through a set of categorical variables (e.g., parents’ KAP in the present study), LCA can estimate various measurement models with different number of latent classes within the target population (e.g., from one class model to six-class model; Lanza et al., 2007, 2010). Researchers can identify the optimal number of latent classes by comparing parameter estimates, information criteria, and fit indices (e.g., AIC and BIC). Compared to factor analysis, a variable-centered approach dealing with subgroups of variables, LCA is also known as a person-centered approach as it deals with unknown groups of people. The results of LCA are useful for designing a targeted intervention in public health or public policy domains.
We use the KAP variables to identify the latent classes of parents, with each class representing a particular group of parents whose children may have similar levels of obesity risks. Mplus 8.3 is employed to estimate different latent class models (two classes to five classes). Furthermore, three indices are used to compare the model fit between different models: Akaike information criterion (AIC), Bayesian information criterion (BIC), and adjusted BIC. The model with a lower AIC, BIC, and ABIC fits the data better. Additional tests are employed to examine whether the current model (k classes) fits the data better than k-1 classes: Vuong-Lo-Mendell-Rubin likelihood ratio test (VLRT), Lo-Mendell-Rubin adjusted LRT (ALRT), and bootstrapped parametric LRT (BLRT; see Table 2). The hypothesized model fits the data better if VLRT, ALRT, and BLRT are significant (p < .01).
Comparison of Model Fit Between Different LCA Models.

Note. AIC = Akaike information criterion; BIC = Bayesian information criterion; ABIC = sample-size adjusted BIC; VLRT = Vuong-Lo-Mendell-Rubin likelihood ratio test (LRT); ALRT = Lo-Mendell-Rubin adjusted LRT; BLRT = bootstrapped parametric LRT.
Regression: Linking KAP to Various Socio-Economic Variables
Following the LCA, one additional research inquiry of interest is which socio-economic factors influence a particular parent’s class membership. More specifically, we aim to test how a parent’s socio-economic background influences his/her children’s obesity risk levels. Logistic regression examines the associations between SES variables and class membership. The dependent variable is whether an individual belongs to a particular latent class (e.g., LC1; 1 = Yes, and 0 = No). Independent variables contain all socio-economic factors discussed above.
Results
CFA
The hypothesized model shown in Figure 1 renders a good model fit: χ2/df = 55.92/21 < 3, RMSEA = .039, CFI = .980, and SRMR = .038. Factor loading for each item ranges from 0.34 to 0.78 except the item k2 (factor loading = 0.29). The factor covariance ranges from 0.078 to 0.91 (see Figure 1). Health practice shows a positive covariance with knowledge and attitudes. Nevertheless, its covariance with attitudes is not significant. We use ordinal alpha to check the internal consistency of the scale items in each dimension. Alpha values for the three dimensions of knowledge, attitudes, and practices are .55, .77, and .58 respectively. Although an alpha coefficient higher than .70 is recommended, values between .50 and .60 are still acceptable for preliminary social science studies especially when the scale contains a limited number of items (Chen & Xu, 2021; Hamedani et al., 2019; Nunnally et al., 1967; Peterson, 1994; Streiner, 2003; Xu, 2022; Xu & Chen, 2021). Consequently, the three-dimension KAP scale with nine items is deemed adequate.
LCA
Results of LCA show that the four-latent-class model is preferred with consideration to balancing between model fit and parsimony (see Table 2). Therefore, we selected the four-class model for reference. The reasons include (1) all the indices strongly favor the four-class model (e.g., BIC); (2) it is more interpretable for the risk profiles across groups; and, (3) each latent class consists of a considerable number of respondents. Table 3 presents the results of latent class distribution and membership probabilities.
Item-Response Probability, Class Counts, and Proportions (4-Class Model)

As shown in the top panel of Table 3, each column displays the probabilities of individuals from a particular class reporting “1 = Yes” in each KAP variable. Higher probabilities hint at certain characteristics of risk profile membership. Each latent class is given a descriptive label based on the KAP variables with high item-response probabilities for this particular class. Latent class LC1 is named “Limited knowledge group” which consists of respondents who are characterized with limited knowledge, positive feedback on attitudes, and moderately low level of health practices. Latent class LC2 is labeled with “Negative attitude group” as respondents in this class are characterized by a moderately high propensity to report positive feedback on knowledge and health practices, but highly likely to report negative attitudes. Latent class LC3 is named “Best practice group” the comprises responses with positive feedback in all KAP dimensions. Lastly, latent class LC4 is labeled “Limited practice group.” Respondents in this group tend to have positive attitudes and a moderately high level of knowledge but report negative feedback in physical activities.
LCA also estimates the group membership for each respondent. Class count and class proportions are shown in Table 3: 59.91% of the respondents belong to LC3 (Best practice group), 12.47% belong to LC1 (Limited knowledge group), 10.18% of respondents from LC2 (Negative attitude group), and 17.45% of respondents belong to LC4 (Limited practice group). Compared with LC3 members with the least risk of childhood obesity, children of parents in LC1 and LC4 may have higher risks. Children of respondents from LC3 may have the least risks of obesity, while LC1 and LC4 may have a higher risk. Interestingly, LCA does not extract any classes with respondents who report negative feedback to all KAP dimensions.
Regression
Correlation analysis in Table 4 provides the preliminary findings of which SES factors are associated with the membership of each latent class. For example, younger age, higher education level, higher household income, Indian ethnicity, and married respondents are correlated with the membership of LC3. While respondents with older age, lower education, and higher household income may tend to belong to LC4.
Correlation.

p < .05.
Results from logistic regression analysis are shown in Table 5. The membership of the latent class LC1 (limited knowledge) is associated with working full-time and Chinese ethnicity. Other independent variables are significant. Regarding the LC2 (negative attitude), results demonstrate that smaller public housing types, lower household income, non-Chinese, and more family members in the same household are associated with the membership of LC2. The membership of LC3 (the best practice group) is associated with younger age, high household income, non-full-time work status, and not living with grandparents. For group LC4 (limited practice), older age and lower education show significant associations with individuals’ membership in this group.
Examining the Impact of Socio-Economic Factors on Class Membership.

Note. Standard errors in parentheses.
p < .1. **p < .05. ***p < .01.
As we are more interested in the latent class LC3 in which group members report positive feedback in all KABP dimensions, we selected LC3 for further discussion. As mentioned above, 59.91% of the total respondents in our study belong to LC3. LCA results demonstrate that parents in LC3 have good nutrition knowledge, positive attitudes toward weight control, and consciously encourage children to participate in physical exercises and to eat healthily. Therefore, compared to other latent classes, children of respondents in LC3 may have the lowest risk for obesity. Regression results indicate that younger parents who have a high household income and do not reside with their parents are more likely to belong to this lower-risk group. Interestingly, work status shows a negative sign, meaning that respondents with fewer working hours tend to belong to LC3. One explanation is that, with other conditions being equal, parents who work fewer hours would be able to spend more time on child-rearing activities such as collecting health information, preparing healthy food, and participating in physical exercises.
Discussion
Main Findings
Parents’ obesity-related knowledge, attitudes, and practices play a crucial role in shaping children’s healthy lifestyles and maintaining healthy body weight (Birch & Davison, 2001; Love et al., 2020). The present study drew on the KAP survey to understand how parents’ KAP impacts childhood obesity. First, by surveying Singaporean parents, the present study employed latent class analysis to group parents by assessing their KAP indicators. Four latent groups of parents with different levels of KAP were identified: 12.47% of respondents belong to latent class LC1 (Limited knowledge group), 10.18% belong to latent class LC2 (Negative attitudes group), 17.45% fall into latent class LC4 (Limited practice group), and 59.91% of respondents fall into the latent class LC3 (Best practice group). Children of the respondents from each group may have varying obesity risks (e.g., children of parents in LC3 have lower risks than those in LC4).
Second, the results of LCA demonstrate that individuals’ health knowledge, attitudes, and practices can be non-aligned, which reaffirms findings in existing literature (Good, 1994; Mabiala Babela et al., 2016; Pelto & Pelto, 1997; Rausch et al., 2015). In many cases, changes in knowledge and attitudes do not necessarily lead to changes in practices. In the present study, participants in LC4 reported good health knowledge and satisfactory levels of attitudes but still indicated limited participation in physical activities and sports. Similarly, although participants in LC2 seemed not to perceive obesity as an issue for their children, they still showed a moderately high propensity to report positive feedback on knowledge and health practices.
Lastly, we associated the class membership with various socio-economic factors to understand what determines a respondent’s KAP profile. We found that (1) respondents in the limited knowledge group (LC1) are more likely to be those of Chinese ethnicity and working full-time; (2) participants in the negative attitude group (LC2) are likely the lower-income and non-Chinese parents who are living in smaller HDB apartments with more household members; (3) the older and lower educated parents are more likely to fall into the limited practice group (LC4); and (4) the membership in the best practice group (LC3) relates to a younger age, higher household income, non-full-time work status, and families not co-residing with children’s grandparents.
Theoretical Implications
The three most critical contributions of the present study merit mentioning. First, the present study is a pioneer attempt to address parents’ KAP about childhood obesity within an Asian context. The KAP survey provides a valuable instrument to assess the effects of family environmental factors on child obesity. With increasing evidence supporting the significant impact of family environment on childhood obesity (Birch & Davison, 2001; Birch et al., 2001; Golding et al., 2019; Persky et al., 2019; Straughan & Xu, 2022), the multi-dimensional KAP framework proves promising in future childhood obesity research in other Asian societies.
Second, a person-centered approach via LCA maps the different types of parents with varied obesity-related KAP profiles. The four groups of parents reflect four parenting styles with varying levels of obesity risk. Children whose parents report positive responses to all dimensions of KAP would have the most negligible obesity risks. While those whose parents with poor knowledge and limited practices may face higher risks. LCA results also provide an insightful picture of the interplay between various KAP factors. In 59.91% of the cases, respondents with sufficient health knowledge and awareness about the negative impacts of obesity are more likely to pay attention to nutrition management and their children’s physical activities, which is consistent with the extant literature (e.g., Friedman & Shepeard, 2007). However, an individual’s responses to the three KAP dimensions may be inconsistent as this study exhibited how 17.45% of the parents with good knowledge and positive attitudes still reported limited practices.
Lastly, the present study confirms that best practices in child-rearing are a function of multiple socio-economic factors. A large body of literature argues that children’s development and well-being are primarily determined by parental practices (Amato & Fowler, 2002; Gesell et al., 2021; Herle et al., 2020; Lim et al., 2020). Children tend to do well when parents are supportive, spend time with their children, and monitor children’s health and behavior (Bronfenbrenner, 1979; Haidar et al., 2019; Kohn, 1977; Vittrup & McClure, 2018). However, adequate health knowledge and parenting practices are conditioned by parents’ socio-economic background (Case & Paxson, 2002; Flores et al., 1999; Gibbs & Forste, 2014; Rafferty & Griffin, 2010). The present study supplements the literature with evidence from a multi-ethnic country in Asia. Our findings confirm that different parenting styles are associated with age, income, education, ethnicity, occupation status, and household structure. More interestingly, the findings highlight the cultural characteristics in child-rearing. Unlike in western countries, traditional familism persists in most Asian societies (Feng & Straughan, 2017). It is common to see three generations co-residing together in Singapore and many other Asian countries as many elderly Asian grandparents expect care from their children and at the same time help to take care of the grandchildren. This intergenerational household structure may shape parenting practices and children’s health status, as demonstrated by this study that grandparents acting as primary caregivers may put children at a higher risk of obesity.
Policy Implications
The increasing prevalence of childhood overweight and obesity has enormous health and economic consequences for individuals, families, and public health systems in Asian societies (Fan et al., 2017; Lindsay et al., 2017; Quah et al., 2019). The present study informs that health intervention programs can utilize the KAP survey to identify the most vulnerable families. Subsequently, targeted interventions should be designed for each particular group of families. For example, education programs should primarily target those with poor obesity-related knowledge, negative attitudes, and limited health practices (e.g., parents from LC1 and LC4 in the present study). The targeted health intervention programs could substantially reduce the cost of obesity prevention in Singapore.
Moreover, policymakers of health promotion agencies should be cognizant of how the socio-economic status of parents conditions parenting styles. The present study’s findings imply that children with parents who are older and less educated may face higher obesity risks. Therefore, policymakers should allocate more public health resources to these families. Since grandparents as caregivers are commonly linked with childhood obesity through misconstrued knowledge (e.g., the higher the fat content, the more nutritious the food), beliefs (e.g., fat children are healthy), and behaviors (e.g., overfeeding) (Jiang et al., 2007; Li et al., 2015), health promotion programs should also target grandparents who are the primary caregivers.
The third recommendation is to build a family-friendly working culture. The evidence from our study shows that parents from the best parenting practice group are more likely to be those with a higher household income and fewer working hours. In Singapore, it is common to see both parents working full-time and childcare responsibilities largely delegated to domestic helpers, childcare services, or grandparents. Many parents may not have the time to manage their children’s diet and physical activities. Thus, we recommend that policy-makers and employers should support working parents by enabling them to balance work and child rearing responsibilities.
Limitations and Future Research Directions
The present study has several limitations. Firstly, the KAP scale item pool may not be fully comprehensive. We constructed the item pool mainly based on the existing literature. Therefore, bias may exist and some critical information about parents’ knowledge, attitudes, and practices about childhood obesity may be missing. Secondly, due to limited resources, the data used for analysis are cross-sectional, which may limit any casual interpretations. The self-reported data may also suffer from common method bias and spurious relationships between parents’ socio-economic variables and parenting profiles. Third, self-reported survey data may also risk social desirability. For example, respondents may over-report the positive responses to questions like health knowledge and good parenting practices but under-report some negative perceptions (e.g., unhealthy practices). Lastly, the current study’s findings are based on a single context and may not be transferrable to other countries. For example, Singapore’s economic conditions, human capital, working culture, and social demographics may be different from many other nations. Besides, Singapore is a multi-racial and English-speaking country. Both traditional lay perceptions of children’s body weight and western understandings may influence Singaporean’s obesity-related KAP. Nevertheless, these limitations do not undermine the value of the present research. The findings add value to both future obesity research and health promotion practices.
Using LCA to examine parents’ KAP in other contexts is recommended for future research directions. Researchers can conduct more robust studies using a more comprehensive KAP scale to identify parenting styles and their impact. Future studies can also use a longitudinal research design that allows data collection in different life stages of children or consider collecting data based on a parent-child dyad approach to address the social desirability issue. Given the distinct risk profiles of parents and various explanatory factors (e.g., age, education, income, occupational status, residence type, ethnicity, and household structure), future research may also want to investigate the mechanisms of how these factors influence parents’ obesity-related KAP and children’s body-weight.
Conclusion
The present study draws on the KAP framework to understand Singaporean parents’ obesity-related knowledge, attitudes, and practices. We identified four groups of parenting styles with different levels of KAP and childhood obesity risks using LCA on a nationally representative sample. This study adds value to the literature by (1) mapping the different types of parents with varied obesity-related KAP profiles, (2) demonstrating that knowledge and attitude changes do not necessarily lead to behavior changes, and (3) linking different parenting styles to various socio-economic factors. This study is one of the early attempts to apply KAP to investigate the parental influence on childhood obesity in a multi-racial country in Asia. As such, the findings have important implications for childhood obesity prevention interventions, especially for societies that share a similar cultural and demographic makeup as Singapore. Future studies can use a more comprehensive KAP questionnaire and a more sophisticated research design to investigate parental factors of childhood obesity in Singapore or in other Asian contexts.
Footnotes
Appendix
| Authors | Focus | Methods | Findings |
|---|---|---|---|
| Bruss et al. (2005) | Social factors on child obesity. | Focus group discussions. | Attitudes, beliefs, and practices in child feeding are varied between ethnic groups. |
| Caprio et al. (2008) | The impact of socio-economic factors on health practice. | Theoretical debate. | Socio-economic factors (such as education, income levels, and race) may impact obesity through the role of money, place, and time. |
| Choudhry et al. (1998) | South Asian women’s knowledge, attitudes, and practices about breast cancer. | Interview. | Fluency of English and number of years in Canada matter. |
| Cluss et al. (2013) | The impact of SES on nutrition knowledge. | Survey. | Race, education, and income predict the level of nutrition knowledge. |
| Cotugna et al. (1992) | American adults’ knowledge, beliefs, attitudes, and behaviors about cancer prevention. | Survey. | Education and income impact people’s knowledge, beliefs, attitudes, and behavioral change. |
| Darmon and Drewnowski (2008) | Social class and healthy diet. | Literature review. | SES variables such as income, race, and education impact on diet quality. |
| Gaina et al. (2009) | The effects of mothers’ employment on children’s healthy eating | Survey. | Children whose mothers are working full-time tend to have higher BMI than those whose mothers are working part-time or not employed. Fathers’ work status is not significant. |
| Kuhlthau and Perrin (2001) | Parents’ employment and child health | Survey. | Children’s poor health is related to parents’ reduced employment. |
| Kumanyika and Grier (2006) | Obesity prevalence in low-income and minority population. | Literature review. | Obesity rate of children in lower-income and minority communities is higher. |
| Velardo and Drummond (2013) | Parent’s health literacy and food-related parenting practice. | Focus groups and interview. | Both individual factors and structural factors are important. |
| Zarnowiecki et al. (2012) | Parental influence on children’s knowledge about healthy food. | Survey. | Education level and SES may impact parents’ knowledge. |
Acknowledgements
The authors thank the four anonymous reviewers for their insightful comments. We are also grateful to colleagues Professors Qiushi Feng and William Tov, Ms Grace Cheong, and Mr Micah Tan for their contributions in framing the arguements.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the Ministry of Education, Singapore, under its Academic Research Fund Tier 2 grant (MOE2016-T2-2-085). Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors and do not reflect the views of the Ministry of Education, Singapore.
Ethical Declaration
The present research was conducted in accordance with the general ethical guidelines and the ethical approval was obtained from the Institutional Review Board (IRB) of Singapore Management University. Written informed consent was obtained from all participants prior to the survey.