
Abstract
There is increasing evidence shows that fear of childbirth (FOC) may have short- and long-term adverse effects on mothers and babies if left untreated. The childbirth process is an experience with many dimensions, multifaceted, and unique for each woman, still strongly influenced by the social-cultural context in which women belongs. To identify and explore the factors contributing to the fear of childbirth among recently delivered women of Pune city, India. The study used a qualitative study approach. A total of 15 in-depth interviews were conducted with women who have recently given birth in maternity hospitals. Interviews were conducted using an interview guide (open ended-questionnaire). Interviews were audio-recorded. The participants were called into a separate room for the interview; full privacy was given to the interviewees, thus making a safe and reliable environment. All collected interviews were transcribed and analyzed. Axial coding was used to develop codes into major themes contributing to FOC were derived. Seven major themes emerged from the analysis of the transcribed interviews. The seven major themes are fear related to the child, fear of parenthood, fear due to mode of delivery, negative pregnancy/delivery experience, psychological aspects attributed to fear of pregnancy, fear of pain, and social background. FOC occurs in most of pregnant women irrespective of parity. The determinants of FOC are influenced by women context; thus, variation in factors of FOC is observed. The FOC related factors show the complex interconnection between them, and it may vary from woman to woman and settings to settings concerning women context.
Keywords
Introduction
Every women experience the feeling of giving childbirth based on her particular context (Nilsson et al., 2018) differently. For most women childbirth is a highly awaited, joyful, and satisfying experience. However, it is also accompanied by the most severe pain a woman will ever experience in her whole life (Prakash et al., 2017). For every woman, pregnancy involves physiological and psychological changes that prepare the woman for motherhood (Beydag et al., 2007). The childbirth process is an experience with multifaceted and unique dimensions for each woman, still strongly influenced by her social and economic context (Larkin et al., 2009). Thus, understanding the childbirth process requires careful consideration of social, cultural, and economic factors that may influence the experience of childbirth for that woman (Latifnejad Roudsari et al., 2015).
The global pooled prevalence of Fear of Childbirth (FOC) is 14% (O’Connell et al., 2017). Approximately 5% to 16% of pregnant women suffer from severe FOC (Adams et al., 2012; Laursen et al., 2008; Melender, 2002; Nieminen et al., 2009; Nilsson et al., 2018; Waldenström et al., 2006). Another study shows that 18% of the women report fears about pregnancy and delivery (Gowri et al., 2015). Prevalence of FOC in India is 17.7% (Jaju et al., 2015; O’Connell et al., 2017). The measurement of FOC with scale Wijma Delivery Expectancy/Experience Questionnaire (W-DEQ) >85 criteria, the prevalence of high FOC vary between countries (Adams et al., 2012; Nordeng et al., 2012; Storksen et al., 2012). These variations are attributed to the timing of assessment, study setting, measurements used to report the fear of childbirth, and cultural contexts (Ryding et al., 2007; Waldenström et al., 2006). Many studies reported that 6% to 10% of pregnant women suffer from FOC that affects everyday life (Adams et al., 2012; Kjaergaard et al., 2008; Laursen et al., 2008; Pazzagli et al., 2015)
Fear of childbirth is a common problem affecting women’s health and well-being during pregnancy, delivery, and postpartum (Nilsson et al., 2018). FOC may contribute to the increased complications during labor, birth, and postpartum period. The diversity of aspects like can elucidate women’s fears; pain, obstetric injury, emergency cesarean section, and behavior of Health Care Staff (HCS). But for some women, the greatest fear that has been distinguished is of delivering a physically damaged or congenitally malformed child.
Literature reveals that factors such as anxious personality, previous sexual abuse, past traumatic birth or any traumatic experience in health care, previous miscarriages, long duration of infertility, smoking, low social supports, and poor partner relationships have been associated with fear of childbirth (Aksoy et al., 2014, 2015; Raisanen et al., 2014). A common manifestation of severe FOC is the appeal or demand for cesarean section (CD) by the women (Fuglenes et al., 2011; Storksen et al., 2015; Stützer et al., 2017). It has been found that women with fear of childbirth (FOC) are more vulnerable, short-tempered, with lower self-esteem, and anxiety-prone compared to women in general (Alipour et al., 2012; Jokic-Begić et al., 2014; Ryding et al., 2007). Further, women with former FOC are at a greater risk of post-traumatic stress symptoms or disorder after childbirth (Söderquist et al., 2009). It has found in many studies that greater intensity of FOC has been shown to be associated with mental health problems such as depression, anxiety, and panic disorder before, during, and after childbirth, even in women without a history of depression (Raisanen et al., 2014; Rouhe et al., 2015; Storksen et al., 2012). Perinatal psychological health problems have been studied very well in high-income countries. In contrast, studies on the psychological health of problems of pregnant and postpartum women are rarely studied in low- and middle-income countries (Alipour et al., 2012). Two decades of well-conducted longitudinal studies demonstrate that mild to moderate perinatal distress can have serious adverse effects on mothers and children, including preterm birth and low birth weight, child developmental delay, and poor child mental health (Kingston et al., 2014).
Rapidly increasing literature shows that the FOC is reported worldwide, and researchers are paying much more attention to this issue than earlier. However, in the Indian setting only few studied are conducted certain population. Substantial evidence shows that Indian poor women often face financial hardship during pregnancy and childbirth. However, no studies is examining the poor women or urban poor women fear of childbirth in India. Therefore, this study aims at understanding the factors contributing to FOC and its relation (interconnection) with the other factors during pregnancy period (pre, during, and post pregnancy).
Methods
Study Design and Setting
This qualitative study conducted to describe the meaning and significance of individual experiences and also help in exploration of fear of childbirth. The study was conducted at non-governmental organization lead maternal and child health welfare hospital situated in Pune city of Maharashtra, India.
Relationship with participants
The female interviewer and the interviewees met each other for the first time on the day of the interview. Thus, there was no established relationship between the interviewer and the interviewees prior to study commencement. The participants were informed about the interview, its purpose, and the interviewer by the interviewer herself.
Participants selection
The purposive sampling method was used to select the sample. The main inclusion criteria for selecting the sample were the women who have recently delivered in the institution. Both nulliparous and primiparous included. The participants were selected irrespective of their age groups, occupation, education, economic strata, and area of residence. Women who had given birth in the last 45 days of the institution and were willing to participate in the study were selected. In total, we approached 26 eligible women; among them, 15 eligible women were consented to participate in the study. The study completed 15 in-depth interviews.
Ethical considerations
The written consent was taken from the participants before the interview. The written consent from was provided to the participants to read by themselves and after the approval and confirmation, their signature was taken. In case of no education or physically challenged the thumbprint of the interviewee and sign of the witness was taken in consideration after which the actual interview was conducted. All the personal information concerning their consent is guaranteed to be confidential as per ethical consideration. The student institutional ethical clearance was obtained from the university.
Data Collection
A semi-structured open-ended questions interview guide prepared based on the literature review; was used for data collection. The interview guide consisted of questions on demographics, women experience in the place of birth, pregnancy experience, fear of childbirth, factors related to fear of delivery, and any other information related to women’s birth experience. The female interviewer had undergone intensive training in conducting in-depth interviews with women who had recently given birth. Interviews were conducted in the institution where women given birth. The participants were called into a separate room for the interview where only the interviewer and the interviewee were present. Full privacy was given to the interviewees thus making a safe and reliable environment for the interview. Also, the confidentiality was maintained. Interviews were conducted in the Hindi language and lasted around for 30 to 45 minutes. All interviews were audio recorded and notes were taken wherever required. Interviewer has made all efforts to bring out the women’s fear of childbirth. Probing questions were asked for bringing clarity in the information. The participants were recruited until no new relevant knowledge was being obtained from new participants (data saturation).
Data Management
The collected data (audio recordings) were used for transcription. A single person did the transcription in MS Word 2016 for each participant. The process of repeated reading and listening to recording performed to ensure data cleaning and accuracy. After the completion of transcription and data cleaning for every participant, the final transcripts were used for analysis.
Data analysis
The transcript for every participant was read for three times to identify the relevant codes. Since the interview was conducted in Hindi language initially the codes were identified in Hindi. The Codes were then translated in English with the participant reference number. The data was coded by the single data coder using axial coding. Step 1, the codes under the same headings were categorized into groups and recorded as primary sub-themes. Total 113 codes were identified, out of which 50 primary sub-themes were formed. In step 2, 50 primary sub-themes were further analyzed and categorized into more complex categories; 22 secondary sub-themes. In final step 3, the secondary sub-themes were again further analyzed into seven complex domains, resulting in the finding of main themes (factors) responsible for FOC in women of Pune city.
Furthermore, as is intrinsic to the method, the whole data set was given equal attention to fully consider repeated patterns within the data. All initial codes relevant to the research question were incorporated into the main themes. At any point, if any of the themes that did not have enough data to support them or were too diverse were discarded. This refinement of the themes took place on two levels, first and foremost with the coded data ensuring they formed a coherent pattern, and secondly once a coherent pattern has formed the themes were considered in relation to the data set as a whole. This step ensured that the themes accurately reflect the evident that were found in the data set as a whole. Supplementary coding was also done at this stage to ensure no codes had been missed in the earlier stages. Once the clear idea of the various themes and how they fit together was emerged, the next step of analysis was performed. Different Microsoft files were made for each; codes, sub codes, sub-themes, and themes.
Results
Demographic Characteristic of the Participants
The participants were mostly of age falling between 18 and 35 years. Almost all of the respondents were housewife and the few who were working had left the jobs because of pregnancy. The participants completed education ranged from class fifth to graduation level. All the participants belonged to middle-income families. Most of the participants lived in the urban areas; very few came from the peri-urban area of Pune city.
Determinants of Fear of Childbirth
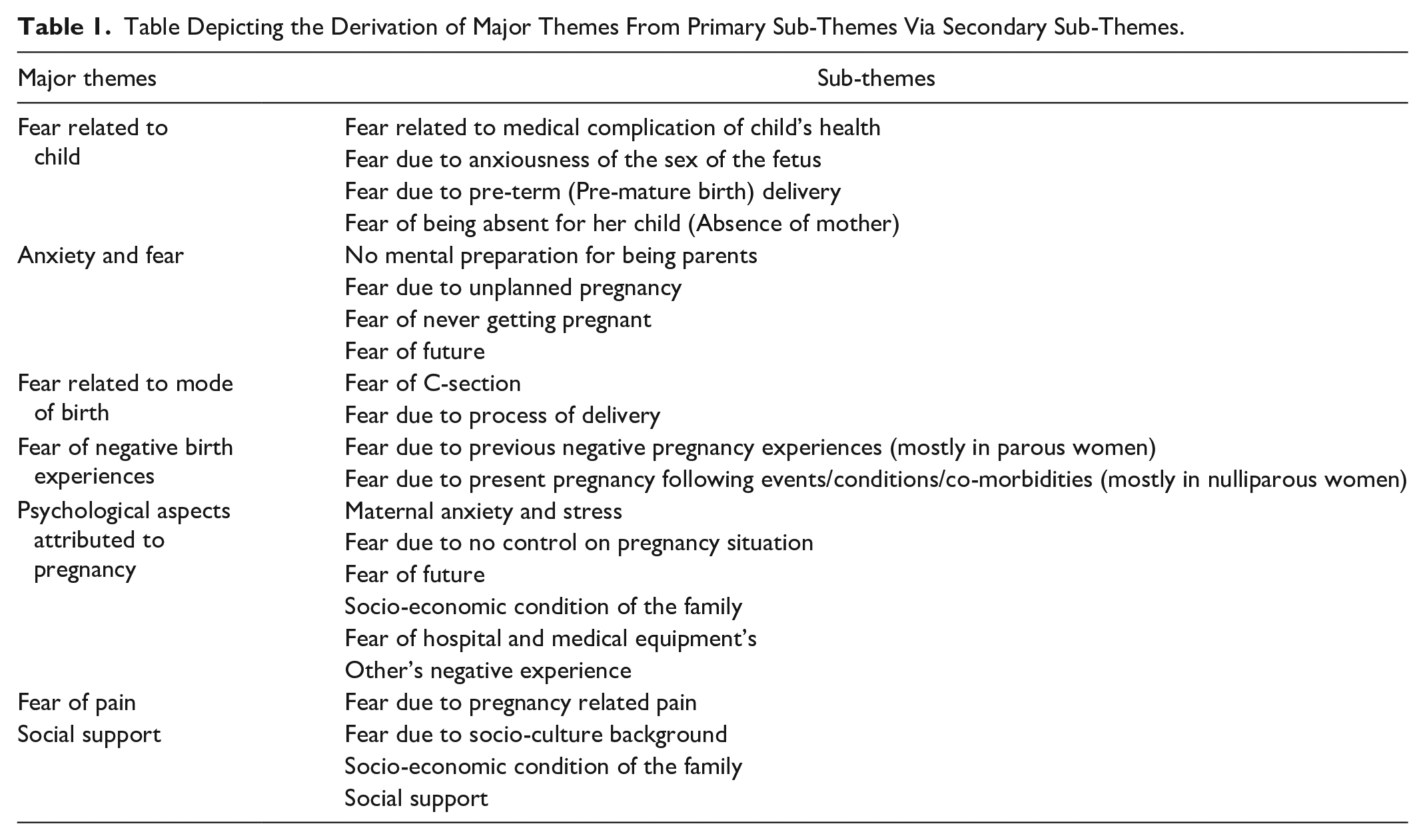
The thematic analysis used to the transcripts to elicit the key concepts evident for FOC. Total seven significant major themes emerged, which as crucial in determining the concept of FOC in Indian pregnant women. Themes and sub-themes are presented in Table 1. The descriptive theme-wise results are present, which explores FOC underlying factors.
Table Depicting the Derivation of Major Themes From Primary Sub-Themes Via Secondary Sub-Themes.
Fear related to child
The theme “Fear related to child” is defined as arousing any dreadful emotion or thought in women during pregnancy, childbirth, and postpartum, leading to maternal stress or anxiety. The fear related to a child is found to be fear pertaining to a medical complication of child health, fear due to anxiousness of the sex of the fetus, fear due to pre-term (Pre-mature birth) delivery, fear of being absent for her child (Absence of mother). Most of the participants were scared of possible medical complications in the child. Some multiparous women had already experienced sudden abortion, which still had an impact on their present pregnancy. Further, women with complications during pregnancy had higher levels of fear related to the child; expecting her difficulties may lead to the child’s poor health. Women who had a girl and were now pregnant had fear related to the sex of the child. The following narratives will explicitly give the idea of women suffering.
Till the time I got into the delivery room, I was completely blank and blackout due to fear of having a baby girl. Even after delivery, I didn’t ask anybody what happened (is it a baby boy or baby girl) to me (4.9).
The bleeding was ongoing for a long period, which was not natural and good, during the second month of pregnancy. What if the bleeding didn’t stop? What if I lose my child? (8.2).
Since I had so many complications in my pregnancy and also had many medical health problems. What if my baby is born handicapped? What if my baby is born abnormally? (8.5).
In some multiparous women, the sex of the child was the biggest concern of stressed conditions. Because either they already bear a girl child in their family, or the family demand was for a baby boy.
In my second pregnancy, I was very much scared and concerned about the gender of my child. My first child was a baby girl, so everyone in the family wished for a baby boy. I even expected the same so that I could complete my family with the ratio of 1:1. But still, I am a mother. I just want a baby to be healthy and good. However, the atmosphere of my family used to be heated and many fights happened between my man and other family members over the gender of the baby. After seeing all, I was very much terrified and concerned for my baby (4.3).
Many women were filled with dread for a child’s health during pregnancy and childbirth. This is either because the child born to them was a pre-term baby or had some medical complications. Not informed or unnecessary separation of the baby from the mother can also disturb mothers psychology from being normal to stress. The women with intense fear due to self-concern took the negative.
They took my baby from me immediately after delivery; I got terrified for what reason. Later, my husband told me that the heart of my baby was beating very slowly. It has been three days since I am still here in the hospital, and have not seen my baby since for three days. Though I get the updates of my baby from my husband, I am scared for my baby (1.6).
Anxiety and fear
Anxiety and fear emerged as a central theme. The theme is defined as evoking any negative thoughts or emotions from becoming parents, guardians, or caring for a baby as a burden or unwanted. It has emerged from the theme that women could not cope with unwanted pregnancies and lack of preparedness for the childbirth process, which has resulted in higher levels of stress and depression even after childbirth. Underlying are some narrations of participants evidencing the theme.
I didn’t wish for this child. This baby was out of blues. I didn’t know when I conceived. I got to know I was pregnant after one and a half or two months after conceiving. Now, what to do? How will I take care? How will I fulfil the needs of this baby? These thoughts scare me (4.12).
This is my first baby, first caesarean delivery, and that to15 day before due delivery date. The baby is so small to handle; how I will hold the baby? How will I take care of the baby? How should I care for the baby? Will I be able to handle my baby? I’m so scared(6.3).
On the contrary, fear of being incapable of giving birth is common in women with a long duration of infertility or infertile women. Women with a long period of infertility or inability to conceive; report mild to severe FOC as they felt incapable of giving birth.
We both wanted to have a baby, but I could not conceive even after many tries and medical help. I got terrified; what if we never have a baby? What if I never am able to conceive? Is there any fault in me? (2.1).
I was not able to conceive a baby even after trying for 3-4 years. I was very much afraid. What if I never get pregnant? What if I never be able to become a mother? (9.1).
Fear related to mode of birth
Fear due to mode of delivery is defined as fear elicited due to having a negative or fearful thought and emotions of thinking of the process of delivery or procedure of delivery. It has emerged from this theme that most women were concerned and had FOC due to the C-section births and pain related to it. Many participants’ horrified by the procedure performed during childbirth irrespective of the mode of delivery. Further, women with a lack of knowledge about pregnancy management and delivery procedures in the hospitals have been reported as the primary reason for their fear of childbirth. In emergency delivery, health care providers have communicated with the family members and women were not known anything has led to the higher levels of fear and anxiety. Some of the narratives have been expressed.
I was in a lot of pain, and it was increasing intensively with time. The doctor told me that my baby head is above and my legs are below, so we have to do caesarean delivery. I’m terrified of all this; after hearing about my caesarean delivery I was more terrified (2.3).
I wanted to have normal delivery because I’m afraid of caesarean delivery, but the doctor told me normal is not possible in my case, I got terrified. Still, in the delivery room, I was only praying to God that it’s okay if anything happens to me, but please keep my child safe (2.6).
I didn’t know anything about caesarean delivery. The doctor told me I would have some issues and complications at the time of delivery and said I need to have caesarean delivery, which frightened me (5.1).
I had zero knowledge about caesarean delivery. I was scared of hospitals and the injections. It was my first baby. When they took me to delivery room for caesarean delivery, I got so horrified that I even cried. I was very much scared for myself (6.2).
Fear of negative birthing experiences
Fear induced due to previous negative birth experiences is one of the major them emerged from the study. This theme is defined as dreadful emotion or destructive thought persuades in pregnant women due to fear of previous negative pregnancy experiences. The majority of participants have had this kind of fear. This fear also may subsidise once women give birth. The following narratives of participants give a deeper understanding of this kind of fear. Also, first-time pregnant women are prone to anxiety and stress. The first-time mothers not have any experience; hence, they reported more FOC. The events following pregnancy like pain, vomiting, nausea, tiredness, prolongation, or pre-term deliveries bother much to first-time mothers.
Before the current pregnancy, I was pregnant for some time, but then the baby was not growing. I checked and took treatment, but it was not functional, so doctor told me that I needed to take out this child as it’s not growing. It’s dead (sad and dull). I lost my child. What if the same happens with this baby? This thought only terrifies me (11.1).
During my first baby, I was so scared and weak that even doctors were not taking the guarantee of my baby because the heartbeat of my baby was shallow. . . I used to take stress in this pregnancy because of what happened in first (3.5).
I got ulcers in my mouth during the sixth and seventh months of my pregnancy. I could not eat or drink anything for at least two months, which affected my body and my baby’s health. I was very stressed and fearful (2.5).
Psychological aspects attributed to pregnancy
This theme is the most complex because of overlapping factors. The psychological aspects attributed to pregnancy itself are self-explanatory. This theme majorly covers negative psychological state of mind that is stress, anxiety, fear, or depression due to elements related to pregnancy. The women with their first pregnancy often sense more pressure of pregnancy than the experienced women.
I have full support from my husband and his family, but I, myself, have a negative impact on this pregnancy, and it’s because they long to have this child, but I’m still not in the phase of becoming a mother (15.4).
I’m bearing so much now. Will, I’ll be able to handle this? What will happen next? How my baby will be? I was so scared of everything. This baby is for so long inside me (3.2).
Some of the women expressed fear for hospitals and medical equipment’s; this could be either due to fear of the medical system, medical staff, or person characteristics of being scared of hospitals since childhood. Harmful or disrespectful experiences in the hospital or medical care system by the medical team can also induce fear in pregnant women (Jungari et al., 2021). Women’s abuse and violence in health care facilities is an emerging public health concern topic as “Respectful maternity care.”
When they were taking me to the delivery room, my heart was filling with fear and I was very stressed and nervous. Since childhood, I’m scared of hospitals and injections. Then that delivery room had so much in it. . . Oh god! (9.3).
I got very much scared seeing the delivery room and its equipment’s. I did not know anything (11.2).
Some women are scared of the whole pregnancy situation as nothing is in their control; while talking about control on the situation, they probably relate to gender of the baby, normality of the pregnancy outcome (normal or abnormal child), and thoughts on future conditions. Also, overthinking over the future could turn into fear for the future for both, for herself or for child.
I was not able to conceive. At last, I’m pregnant & this is my 1st baby after many prayers and trying for the last three years. Finally! But what’s next? What if something happens to my baby or me? What if again my body doesn’t hold my baby for long? (2.2).
In recent years, women also have enormous psychological fear of changes in body posture due to pregnancy, and worry about body image. Many participants have reported this. This increasing self-image trend leads to fear of damaging own self-image. Thus this increase in fear and depression leads to stressful pregnancy and childbirth.
Stomach will get bigger and will look loose with starch marks because of delivery, which I don’t like at all so I have tied this cloth around my stomach tightly. It pains though I’ll still tie because I’m scared that I will not look good after childbirth (1.5).
FOC and depression go hand in hand; FOC could be a sign of hidden depression or depression could be a sign of unveiled FOC in women. Some women or a new couple are so ambitious that they won’t give up their independent life and end up being childless or complicated pregnancy followed due to anxiousness of losing career.
Fear of pain
Fear of pain can be related to any dreadful feelings, thoughts, or emotions during pregnancy due to any pregnancy-related pain. Some of the participants had a fear of successful completion of pregnancy and giving birth to a child. Some of the women were worried that something may happen during pregnancy or childbirth, which raised the level of fear. Fear of pain and a self-suspected low pain tolerant are amongst the most common causes of FOC.
In the first 4th months, I had loads of pain because of vomiting and body pain. And sometimes, it used to be so severe that I used to think something would happen to me. I was very much worried for myself and for my baby. What if something happened to me? Who will take care of my baby? (2.4).
The pain had increased so much, and the intensity of pain was still rising, my BP was high, and the baby was not coming out. I was horrified and getting negative thoughts in my head (5.4).
Fear of pain often combined with fear of losing control. Fear of labor pain or fear during delivery is powerfully associated with fear of pain in general (and it is one of the most common reasons underlying the request for cesarean delivery in nulliparous women.
The pain was getting unbearable for me. I got scared for myself and for my baby. I was very much afraid for both of us and this pain. . . (11.3).
I was in extreme pain, and its intensity was increasing second by seconds. I asked a nurse to look, but she refused to say, “it happens you stay at your place”. The pain was getting unbearable for me; for a second, I thought today is my last day. . . (10.3).
The pain could be so enormous that pregnant women with low self-belief often think that they will die after delivering the baby. This dread to death, thus, increases the pessimistic nature in women, also complicates their pregnancy and child-maternal relationship.
Social support
Social support emerged as one of the important themes of study. This theme covers all types of help needed/expected from society, social networks, and relatives by pregnant women. This could be positive for some women if they receive expected to support and to some could be harmful if they are left alone in their hard time.
Many people use to say that I’m the very heavyweight I won’t be able to conceive and even if I did. . . it won’t last. Others tell me their painful stories, which made me enormously scared for my pregnancy (9.4).
Social support is the means of exchanging human resources between individuals, which always requires stable associations. The women who get pregnant before marriages are more prone to severe FOC—being pregnant before the wedding creates not only societal problems for women but also for her family. Thus, in that scenario, it is observed that the women are isolated from society and are abandoned by family members.
My family wanted me to abort the child because I was still not married. What will others say? Will society not accept this? But I was very much afraid of abortion, and I didn’t even wish for one (7.4).
Every woman expects emotional support from her social group, partner, family, relatives, and friends during pregnancy. Lack of social and familial support may lead to suffering from conditions like stress and primarily depression. According to studies concerning primary FOC, there is evidence showing that previous psychological morbidity can put women particularly at increased risk if she also lacks support from her social network.
Study on the one hand, have found a robust association between FOC and pregnancy-related anxieties and on the other, specific personality characteristics and socio-economic factors. Additionally, low education or low socio-economic level were also considered as the predisposing factors of anxiety during pregnancy or initiation of FOC
In the middle of pregnancy, when I realized my child movement within me, I was very happy but at the same time worried about the future. I was scared because of my home conditions (15.3).
I had financial problem back home which got increased and I was very sick which affected my baby’s health. I got scared of my health and family financial condition (4.10).
I was already in bad financial condition. I was having hard time paying the rent for my house, educating my two-girl child and then this baby . . . How will I take care for this baby now? What about her future? (4.11).
Discussion
The objective of the study was to explore the underlying factors of fear of childbirth among the women recently given birth to a child. The study used a qualitative approach to collect the data on reporting FOC factors in the urban charity hospital in Pune, India. There have been few studies conducted in India on the fear of childbirth; therefore, this study contributes immensely to the literature. Overwhelmingly, seven themes emerged from the qualitative data depicting the range of factors responsible for fear of childbirth among pregnant women.
Current study results found that women with first-time pregnancy and second-time mothers were affected by the fear of childbirth. From emerged themes, it is observed that fear related to child, psychological aspects attributed to fear of pregnancy and negative pregnancy/delivery experiences are the most prominent theme attributed to fear of child birth in both nulliparous and multiparous women. Whereas, from the existing literature for developed countries trace for fear of becoming parent, social background, fear of pain, personal characteristics and psychological background, fear of being incapable of giving birth, previous negative childbirth experience, history of abuse and violence, and mental health problem related to fear of childbirth was obtained.
One of the important and fascinating aspects that emerged from the result was that the Indian women suffering from intense FOC are afraid of cesarean delivery and they seek for regular deliveries. Especially the women tormented with the fear of mode of delivery are often afraid of cesarean delivery and tend to demand normal deliveries instead of cesarean delivery. At the same time, past literature shows that the count of women bearing with FOC, requesting for cesarean delivery or elective cesarean delivery has increased (Fuglenes et al., 2011; Hatamleh et al., 2019; Rouhe et al., 2011).
The study found that one of the critical risk factors of fear of childbirth is familial pressure to give birth to a son. Families’ demands women to deliver son and innocent women have a constant fear of having girl child. India and South Asian countries have strong son preferences embedded in their culture (Mitra, 2014; Pande & Astone, 2007). Many studies have documented evidence of women being pressured to have a son and having baby girls, which often leads to even violence (Jain et al., 2017; Mahapatro et al., 2011). These deeply rooted gender inequalities and son preference could put women at risk of fear of childbirth and postpartum depression. The government of India has undertaken several measures and initiated a number of programs to create awareness among the people about son preference. In India, sex determination in pregnancy is an offence under the law. However, the poor implementation of laws is a concern.
The social and economic background of pregnant women plays crucial role in successful completion of pregnancy. The study found that women lacking social or family support during pregnancy had experienced higher levels of fear of childbirth. Women belonging to the poor households and not having economic empowerment had more worrisome pregnancy which ultimately contributed to fear of pregnancy and childbirth. Substantial literature shows that poor women in India have less utilization of maternal health services and have more pregnancy complications (Pathak et al., 2010; Singh et al., 2014). Women with lack of family or husband support during pregnancy and childbirth also leads to the poor maternal health care utilization (Jungari & Paswan, 2019). Furthermore, the current study also found that women who were pregnant before marriage, lacked support from the family and partner and high social stigma leads to traumatic pregnancy and childbirth. Community-level interventions targeting adolescent girls to educate about reproductive issues will benefit from preventing unwanted pregnancies.
Lack of knowledge about pregnancy complications among women reported as the reasons for the fear of childbirth. Also expecting complications in infant escalate the fear of childbirth among the pregnant women. Similar results have been reported in some other countries. Educating women during antenatal visits about the possible pregnancy complications and its signs before all the processes occur/done is a possible and no cost strategy to boost the confidence of pregnant women.
The study shows that most respondents were worried about parenthood, which triggered fear of childbirth among them. In India, most of the births are unplanned hence, became a psychological and economic burden for unprepared parents, and mothers being more burdened with pregnancy issues. Effective pre-conception counseling services to newly married women about the pregnancy and childbirth could contribute in the reducing the unwanted pregnancies.
The results draw attention to the need for early detection and treatment of fear of childbirth among the pregnant and recently delivered mothers. The effective pain management during childbirth can reduce the fear of childbirth among pregnant women. The health care providers should be trained and equipped with the skills to understand the screen for the possible fear of childbirth among pregnant women. The role of health care providers became very much crucial finding FOC in early pregnancy may provide an opportunity to support maternal mental health (Ayers, 2014; Haines et al., 2011, 2015). The study reported that women were afraid cesarean delivery and one of the factor for fear of childbirth. Previous contrary studies reported that women who opted for the cesarean delivery due to the fear of childbirth (Diema Konlan et al., 2019; Wigert et al., 2020).
The interventions to treat high FOC in women should intend to reduce their childbirth-related anxiety and stress and simplify the acceptance of uncertainties associated with the future delivery (Bewley et al., 2002; Wijma et al., 2016). The consequences of treating maternal anxiety and FOC can be assessed in many different ways, such as in terms of alleviation of apparent stress and better adjustment and acceptance during pregnancy, drawing out the request for cesarean delivery, having better mother-infant bonding during pregnancy and postpartum, have fewer childbirth complications, and having less postpartum problems (Hofberg & Ward, 2003). There is no need for pharmacological treatment of women with FOC, unless co-morbidity like clinical anxiety, depression, or panic disorder are involved (Saisto & Halmesmäki, 2003). Some interventions are present which are given to reduce FOC focus especially on the recovery of PTSD symptoms following childbirth. The major interventions that are prevalent in developed countries are antenatal preparation classes, relaxation training with psycho-education, psychotherapy and psychological support, psycho-education. These are the treatment or interventions which are supported based on results of randomized trails. These other interventions are: briefing, counseling, treatment in aurora clinics, haptotherapy, and treatment based on the PLISSIT model, auriculotherapy, and cognitive therapy. These therapies are either done in a single resource setting or with small sample size, not enough to generalize to all populations. All these interventions are available in a country where a maternity special care centre is present. These special care centres deals with the women requiring special treatment during their pregnancy and are referred by their respective clinicians. Treating FOC requires several visits in special maternity care (Nerum et al., 2006; Raisanen et al., 2014). These special maternity care centres are yet not available in developing countries like India.
Limitations
The study has some limitations to mention. The study conducted is an institution-based study hence; the factors of FOC reported in the study may be limited and may be missed out many other factors. Study participants were belonged to middle income class families, therefore, the background factors reported in this study may not be generalized in other settings. Study was conducted in the hospital were women given birth the possibility of reporting different kind of factors of FOC may not be ruled out completely for the home deliveries.
Conclusion
Most of pregnant women have faced and reported FOC. As the pregnancy is a multifaceted condition, the intrinsic factors leading to FOC shows strong complex interconnection between them which may vary from women to women and settings to settings. From the emerged themes in the study, it was observed that fear related to the child, psychological aspects attributed to fear of pregnancy, and negative pregnancy/delivery experiences are the most prominent theme attributed to fear of childbirth in women. An important finding of this study states that women are afraid of cesarean delivery and they seek normal deliveries.
There is need for early detection and treatment of fear of childbirth, which otherwise, will affect the women and child’s health especially women’s mental health, mother-child relationship, and could also hinder women’s daily life activities. The data on these factors may help to identify women at risk that require prenatal psychological intervention. Also, it is observed that the higher levels of the FOC could be predicted by screening anxiety sensitivity, trait anxiety, expected labor pain, and sources of knowledge about childbirth in the pregnant women during antenatal check-ups. Further research is recommended.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.