
Abstract
Mental distress is highly prevalent in university students, and autistic traits can hinder academic education. The substantial lifestyle changes experienced by new university students can induce mood and anxiety dysfunctions and subsequent suicide-related behaviors. The aims of this study were to evaluate the detectability of suicidal ideation using the Kessler Psychological Distress (K6) questionnaire, a short and easily administered measure, and to elucidate the relationship between K6 scores and developmental disorders following university admission in medical students. The mental states of 341 new students at University School of Medicine were prospectively evaluated using the short questionnaire including the K6 at admission and 6 months later. Participants were simultaneously assessed on the five core features of autism spectrum disorder (ASD), four features of attention-deficit hyperactivity disorder (ADHD), and presence of suicidal ideation on this short questionnaire. K6 scores were significantly higher 6 months after admission than at admission (p = .028). Students with suicidal ideation had significantly higher K6 scores than those without (p < .001), and K6 scores at admission differentiated students with suicidal ideation both at admission (area under the curve [AUC] = 0.947) and 6 months after admission (AUC = 0.913). K6 scores were positively correlated with scores of ASD- and ADHD-related items (ρ = .451 and .440, respectively) and with autism-spectrum quotient scores (p = .041, ρ = .501). In conclusion, the K6 questionnaire may be useful in efficiently detecting university students with suicidal ideation or autistic traits.
Keywords
Introduction
Mental disorders are highly prevalent in university/college students and are found in 20.3% to 41.1% of all students (Auerbach et al., 2016; Poorolajal et al., 2017). In particular, anxiety is very prevalent in medical students owing to study burden and busy schedules (Kulsoom & Afsar, 2015). Research shows that 83.1% of these students with mental disorders had pre-matriculation onset of those disorders (Auerbach et al., 2016). Furthermore, suicidal ideation was found in 3.4% of first-year university students using online surveys (Blasco et al., 2019). Therefore, screening for mental disorders in new university/college students is extremely important to prevent the progression of mental health problems and to prevent associated suicide (Zhang et al., 2015). The frequency of developmental disorders such as autism spectrum disorder (ASD) is increasing (Weintraub, 2011). Both ASD and attention-deficit hyperactivity disorder (ADHD) are frequently found in college students (Takahashi et al., 2016). Students experiencing such problems, particularly those with ASD, frequently feel isolated and many have a lifetime history of suicidal behaviors (Jackson et al., 2018). Therefore, an appropriate questionnaire is needed to identify such students and to facilitate proper diagnosis and treatment.
Previous studies screening mental disorder in university/college students have used the University Personality Inventory (UPI; Kitazoe et al., 2015; Yoshida et al., 1998; Zhang et al., 2015), the General Health Questionnaire–28 (GHQ-28; Poorolajal et al., 2017), and the Depression/Anxiety/Stress Scales–21 (DASS-21; Kulsoom & Afsar, 2015). Although these studies have reported useful data on student health problems, these three questionnaires contain many items (50, 28, and 21 items, respectively) and are not easy to use. In contrast, the Kessler Psychological Distress (K6/K10) questionnaires comprise six and 10 items, respectively, and have an excellent record of detecting mood and anxiety disorders (Furukawa et al., 2008; Kessler et al., 2002; Sakurai et al., 2011). The K6 was included in the U.S. National Health Interview Survey in 1997 (n = 36,116) and 1998 (n = 32,440), and the scale strongly discriminated between cases of Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994)/Structured Clinical Interview disorders (area under the curve [AUC] = 0.879; Kessler et al., 2002). Therefore, although the K6 is quite a simple questionnaire, its capacity to detect mood and anxiety disorders is reliable. Furthermore, both scales (particularly the K6) show good usability as they are very short (Sakurai et al., 2011). However, the K6/K10 has been used mainly with adults (Furukawa et al., 2008; Kessler et al., 2002; Sakurai et al., 2011), and their suitability for university students has not been fully established. In addition, the relationship between K6/K10 scores and suicidal ideation or developmental disorders remains to be elucidated.
In the present study, to evaluate the detectability of suicidal ideation using simple K6 questionnaire, new medical university students were prospectively and consecutively enrolled. Furthermore, the relationships between K6 scores and suicidal ideation and the core features of ASD and ADHD were thoroughly evaluated by using a short and general questionnaire for the first simple screening for anxiety and developmental disorders. To the best of our knowledge, this is the first report to show relationships between K6 scores and specific mental health disorders, including suicide-related behaviors and autistic traits, in medical university students.
Method
Study Design and Participants
A total of 350 of all new medical students at a university in Japan between 2017 and 2018 were prospectively studied. The study protocol was approved by the Ethical Committee of the Hamamatsu University School of Medicine (Approval Number: R16-293), and written informed consent was obtained from all subjects. This study was registered with the University Hospital Medical Information Network (UMIN) Clinical Trials Registry (UMIN-CTR, UMIN ID: UMIN000026513).
Questionnaires and Data Collection
Questionnaire surveys were consecutively conducted at university admission and at 6 months after admission. Subjects were asked to complete self-administered short questionnaire (items are shown in Supplementary Table 1). The Japanese version of the K6 questionnaire (Furukawa et al., 2008) was used, which comprises the following six items: (1) During the last 30 days, about how often did you feel nervous? (2) During the last 30 days, about how often did you feel hopeless? (3) During the last 30 days, about how often did you feel restless or fidgety? (4) During the last 30 days, about how often did you feel depressed? (5) During the last 30 days, about how often did you feel that everything was an effort? (6) During the last 30 days, about how often did you feel worthless? The K6 did not include the question about suicidal ideation. The K6 is scored using a 5-level response scale, ranging from 0 to 4 (0 = none of the time, 1 = a little of the time, 2 = some of the time, 3 = most of the time, 4 = all of the time); this generates a scoring scale with a range of 0 to 24.
On this short questionnaire (Supplementary Table 1), simultaneously, ASD-related five features, ADHD-related four features, and presence of suicidal ideation and insomnia were also assessed using the same 5-level response scale. The representative ASD-related five items were extracted from Autism-Spectrum Quotient (AQ) questionnaire (Baron-Cohen et al., 2001), and the representative ADHD-related four items were prepared in reference to Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013). Representative ASD-related features are as follows: (a) Other people frequently tell me that what I have said is impolite even though I intended to say it politely, (b) I find it difficult to understand what someone is thinking or feeling even when I can see someone’s face, (c) Other people frequently tell me that I keep doing the same thing over and over, (d) I have such a strong interest in one thing I get confused if I cannot do it, and (e) I tend to notice details that others do not, such as smells and sounds. As for internal consistency, Cronbach’s alpha coefficient of ASD-related five items was .744. If a student scored 3 or more on any ASD-related item, their AQ scores (Baron-Cohen et al., 2001) were obtained. AQ questionnaire asked how strongly they endorse these statements (items). However, on the contrary, Social Responsiveness Scale (SRS) questionnaire for autistic traits asked how frequently they endorse these statements (items; Constantino et al., 2003). Therefore, it seems that to ask its frequency for the screening of autistic traits is also reasonable. Representative ADHD-related features are as follows: (a) I frequently make mistakes in performing many activities, (b) I find it difficult to keep concentrating during many activities, (c) I cannot keep still and keep moving as if something rushes me, and (d) I find it difficult to wait my turn in conversations or games. As for internal consistency, Cronbach’s alpha coefficient of ADHD-related four items was .753. These items were also scored using a 5-level response scale, ranging from 0 to 4. If a student scored 2 or more on the item of suicidal ideation, we judged the student was positive for suicidal ideation. Subjects completed the UPI questionnaire (items are shown in Supplementary Table 2) only at admission. The UPI comprises 60 items divided into four categories (Nozomi et al., 2016): (a) physical complaints, (b) depressive tendency, (c) anxious tendency, and (d) compulsive, paranoid, and referential ideas. Regardless of these four categories, total score of UPI was counted as sum of the number of positive items other than Numbers 5, 20, 35, and 50 (Supplementary Table 2). While the reliability of the Japanese version of K6 (Furukawa et al., 2008), AQ, and UPI (Kitazoe et al., 2015) have been shown in previous studies, the reliability of exploratory questions for core features of ASD and ADHD have not yet been tested. Data on age, sex, university faculty, body mass index, smoking history, alcohol drinking history, and amount of exercise were collected from the university student health administration database.
Statistical Analysis
Statistical analyses were performed using JMP-13.1.0 (SAS Institute, Inc., Cary, NC, USA). Categorical data were compared using the chi-square test or Fisher’s exact probability test for independence, and continuous data were compared using the Wilcoxon rank-sum test. The ability of K6 scores at admission to discriminate students with suicidal ideation from those without was evaluated using receiver operating characteristic (ROC) curve analysis. Continuous data for the same student at different time points were compared using the paired t test. The relationships between questionnaire scores (discrete variable data) were analyzed using Spearman’s rank correlation coefficient. All tests were two-sided, and statistical significance was set at p < .05.
Results
Characteristics of All New Students at Admission
A total of 341 of the 350 new students (97.4%) participated in the survey; nine did not give their consent for participation. Table 1 shows the characteristics and lifestyle habits of participants. The median age was 18 (range = 18–22) years, and there were more females than males (males 138, females 203). The median body mass index was 20.6 (range = 15.2–31.8), and many students exercised for 30 min or more per day (66.3%). No participants were current or ex-smokers, and none drank alcohol daily.
Characteristics and Lifestyle Habits of Participants.

Note. K6 = Kessler Psychological Distress questionnaire.
K6 and UPI Scores, and Relationships Between K6 Scores and UPI Total/UPI Item Scores
The median K6 score was 1 (range = 0–18). There were 31 (9.1%) students with K6 scores ≥5 and nine (2.6%) with K6 scores 10 (Table 1). There were no significant differences in K6 scores between males and females, or between students in the faculties of medicine and nursing. The median UPI score was 8 (range = 0–51). The relationship between K6 and UPI scores is shown in Figure 1. There was a weak but positive correlation between K6 and UPI scores (ρ = .360, p < .001). On 26 of the 60 UPI items including suicidal ideation, positive rates tended to be higher in students with K6 scores ≥5 than in those with K6 scores <5 (p ≥ .05 in all items; Figure 2). Students with K6 scores ≥5 tended to have higher positive rates than those with K6 scores <5 not only on items related to depressive and anxious tendencies but also on items related to physical complaints and compulsive/paranoid/referential ideas. All of other 34 items of UPI were not different between groups (p ≥ .05).

The relationship between K6 and UPI scores at university admission.
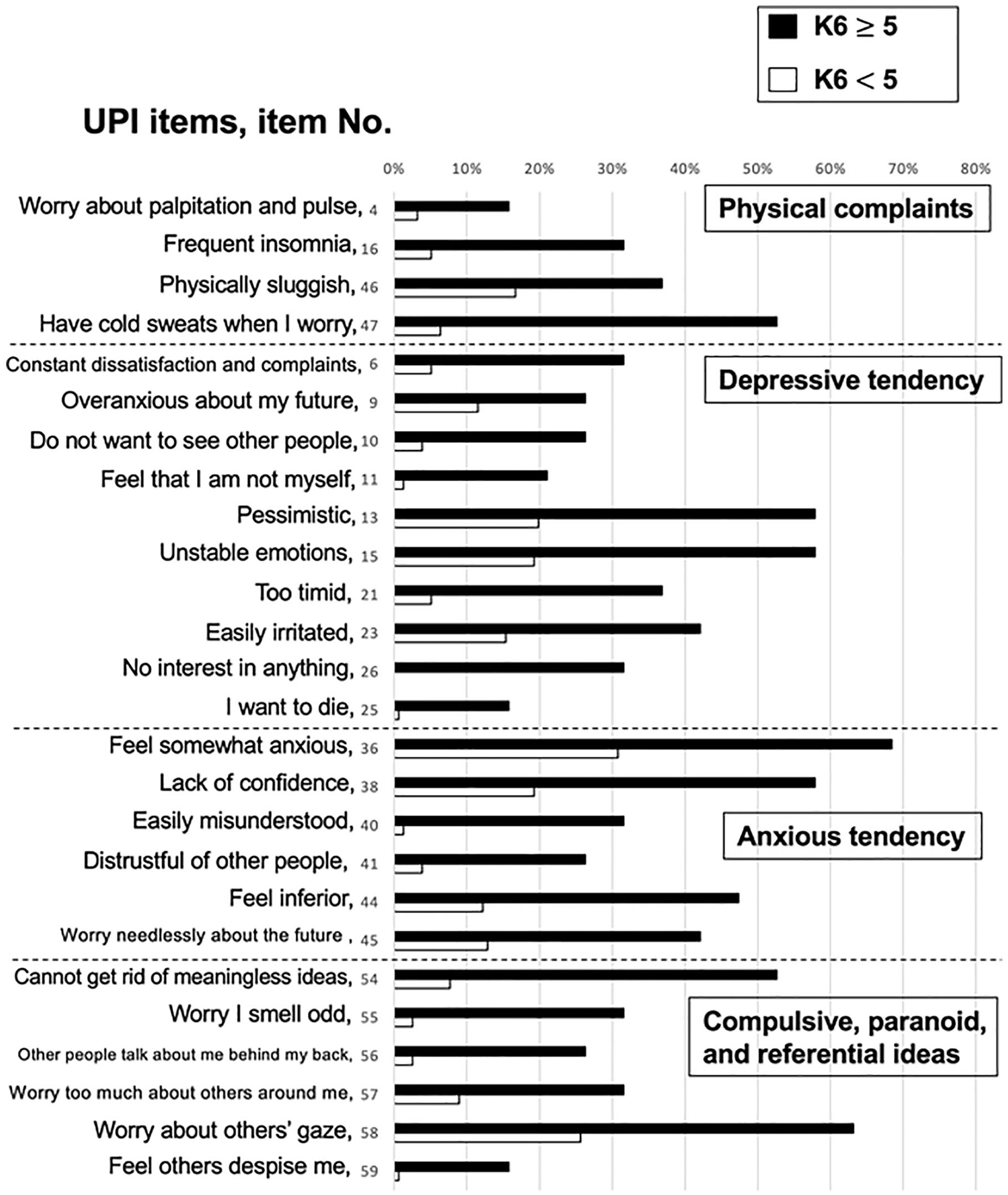
Difference in positive rate on each UPI item between students with K6 scores ≥5 and those with K6 scores <5.
The Detectability of Suicidal Ideation Using K6 Questionnaire Score at Admission
Suicidal ideation is one of the most severe symptoms in students with mental distress. At admission, nine of 341 (2.6%) students had suicidal ideation, and these students with suicidal ideation had significantly higher K6 scores than in those without (p < .0001; Figure 3A). To confirm the utility of K6 scores for discriminating between students with suicidal ideation and those without, an ROC analysis was performed. A K6 cutoff score of 3 differentiated students with suicidal ideation from those without (AUC = 0.947, sensitivity = 88.9%, specificity = 81.9%; Figure 3E). The AUC was highest for K6 scores; however, UPI scores (Figure 3B and F; AUC = 0.776, sensitivity = 66.7%, specificity = 89.5%, cutoff score = 19), ASD-related scores (Figure 3C and G; AUC = 0.915, sensitivity = 88.9%, specificity = 79.8%, cutoff score = 4), and ADHD-related scores (Figure 3D and H; AUC = 0.918, sensitivity = 66.7%, specificity = 98.5%, cutoff score = 7) also differentiated students with suicidal ideation from those without.

K6 scores at admission differentiated students with suicidal ideation from those without.
The Detectability of Suicidal Ideation at 6 Months After Admission Using K6 Questionnaire Score at Admission
In a consecutive evaluation, 317 students (attrition rate 7%) were also evaluated 6 months after admission. K6 scores at 6 months after admission were significantly higher than those at admission (median = 1.82 vs. 1.56, p = .028; Supplementary Figure 1). In addition, 10 of 341 (2.9%) students had suicidal ideation. To confirm the utility of K6 scores at admission in predicting suicidal ideation at 6 months after admission, the K6 scores of these students were compared and an ROC analysis was also performed. Students with suicidal ideation at 6 months after admission had significantly higher K6 scores than in those without (p < .001; Figure 4A). In the ROC analysis, a K6 cutoff score of 2 differentiated students with suicidal ideation from those without (AUC = 0.913, sensitivity = 100%, specificity = 68.9%; Figure 4E). The AUC was highest for K6 scores; however, UPI scores (Figure 4B and F; AUC = 0.888, sensitivity = 100%, specificity = 68.3%, cutoff score = 12), ASD-related scores (Figure 4C and G; AUC = 0.862, sensitivity = 80.0%, specificity = 79.8%, cutoff score = 4), and ADHD-related scores (Figure 4D and H; AUC = 0.826, sensitivity = 70.0%, specificity = 84.6%, cutoff score = 4) also differentiated students with suicidal ideation from those without. However, increase in K6 scores from baseline was not significantly related with suicidal ideation.
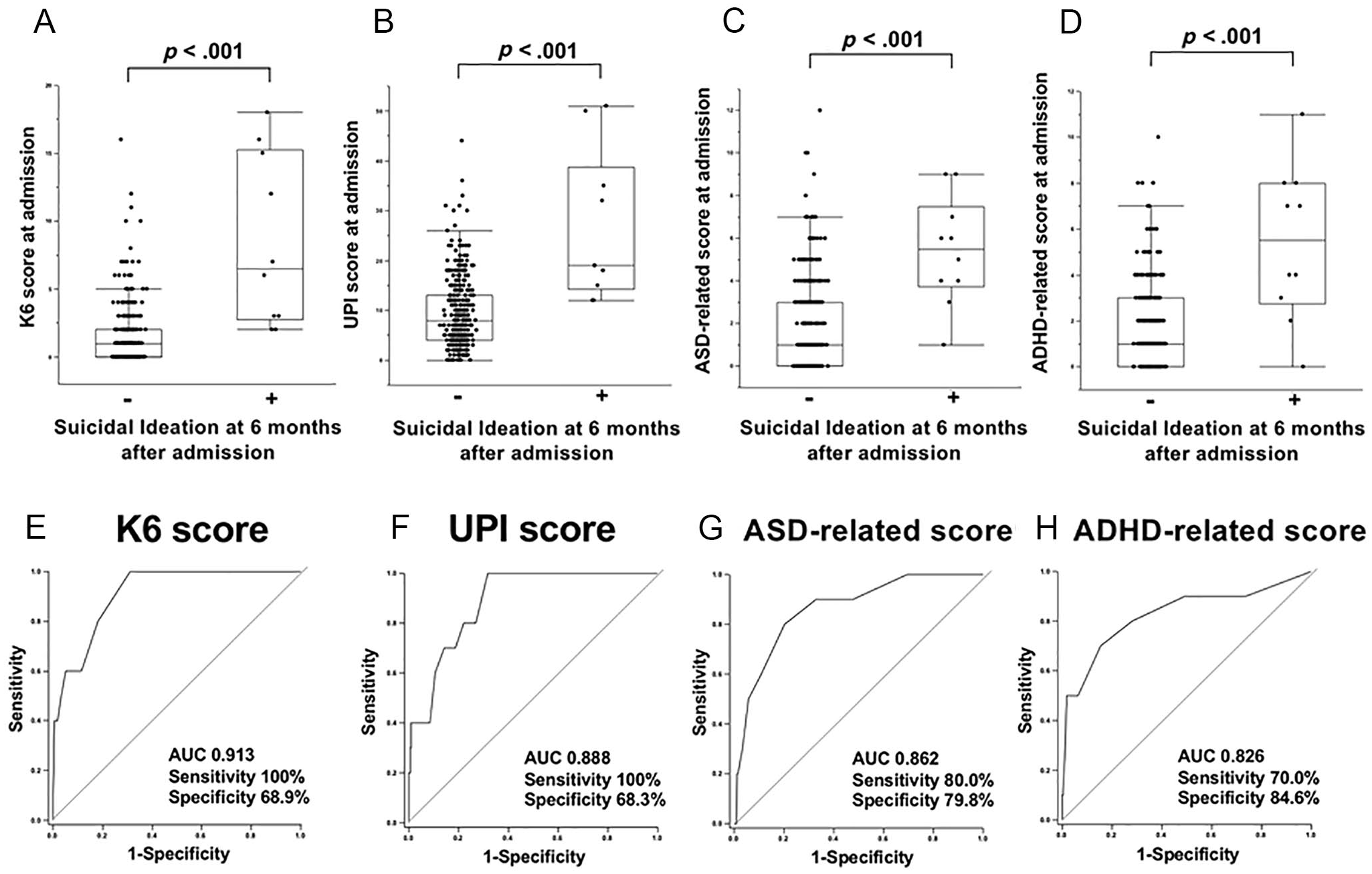
K6 scores at admission differentiated students with suicidal ideation at 6 months after admission.
Relationships Between K6 Scores and the Core Features of ASD and ADHD
ASD and ADHD are sometimes associated with mood/anxiety owing to maladaptation to the social environment. Integrated scores of ASD- and ADHD-related items, including both scores at admission and 6 months after admission, were positively and moderately correlated with K6 scores (ρ = .451, p < .001, Supplementary Figure 2a; ρ = .440, p < .001, Supplementary Figure 2b, respectively). At each time point, K6 scores at admission were moderately and positively correlated with scores on ASD-related items (ρ = 0.401, p < .001; Figure 5A). At 6 months after admission, the correlation between K6 scores and the scores on ASD-related items tended to increase compared with that at admission (ρ = .505, p < .001; Figure 5B). K6 scores at admission were also moderately and positively correlated with scores on ADHD-related items (ρ = .413, p < .001; Figure 5C). At 6 months after admission, the correlation between K6 scores and scores on ADHD-related items also tended to increase compared with that at admission (ρ = .468, p < .001; Figure 5D).

Relationships between K6 scores and ASD- or ADHD-related features.
Relationships Between K6 Scores and AQ Scores
To detect students with ASD, if a student’s score on any ASD-related item was 3 or more, they were asked to complete an AQ questionnaire. K6 scores were positively and moderately correlated with simultaneous AQ scores (ρ = .501, p = .041, n = 17; Figure 6), although this original AQ questionnaire judges these items as binary and this scoring system was different from that in our short questionnaire in the present study (Supplementary Table 1).
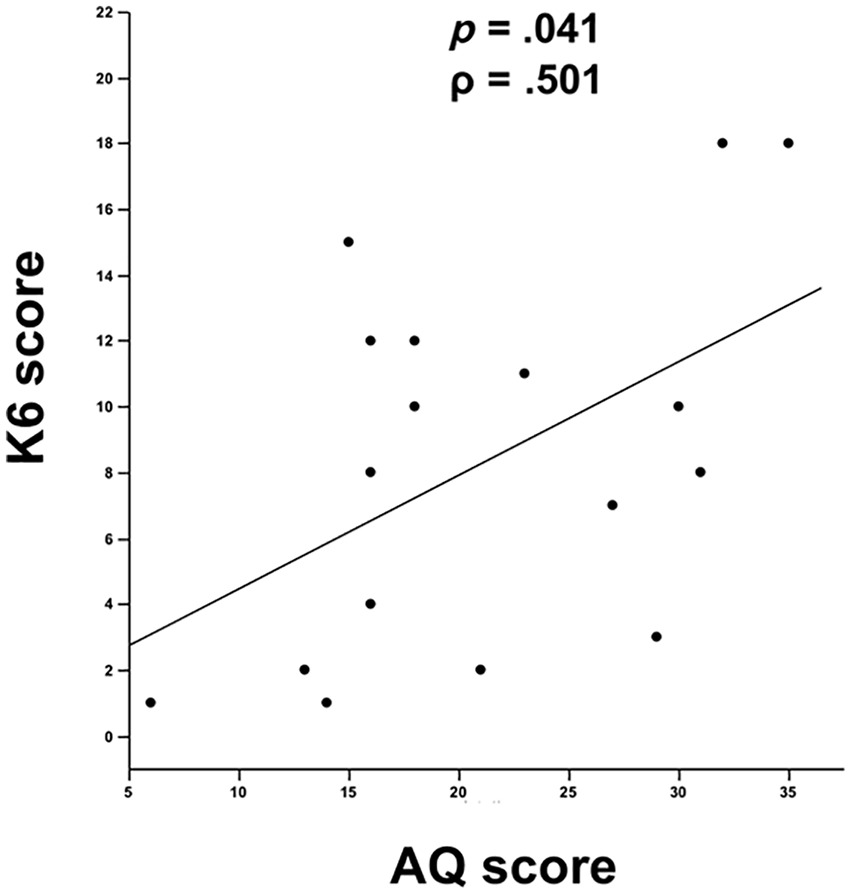
The relationship between K6 and AQ scores.
Discussion
In the present study, we evaluated mental health distress in new university students using the K6 questionnaire, and compared K6 scores with several other parameters. Students with suicidal ideation had significantly higher K6 scores than in those without. K6 scores effectively differentiated students with suicidal ideation from those without, and K6 scores at admission predicted suicidal ideation both at admission and at 6 months after admission. K6 scores were positively correlated with ASD- and ADHD-related scores, particularly at 6 months after admission. Finally, K6 scores were positively correlated with AQ scores. To the best of our knowledge, this is the first report to show the utility of K6 scores for the evaluation of mental health disorders, including autistic traits in university medical students.
Changes in lifestyle and social relationships affect the mental health of new university or college students. Stress resulting from such changes can induce or worsen mental disorders, and 20.3% to 41.1% of university students experience such disorders (Auerbach et al., 2016; Poorolajal et al., 2017). Therefore, early screening for mental disorders is crucial to prevent disease progression and suicide in new students, and to ensure that academic education is not affected (Auerbach et al., 2016; Zhang et al., 2015). Several questionnaires have been used to screen university students, such as UPI (60 items; Kitazoe et al., 2015; Yoshida et al., 1998; Zhang et al., 2015), GHQ-28 (28 items; Poorolajal et al., 2017), and DASS-21 (21 items; Kulsoom & Afsar, 2015). However, these questionnaires are lengthy to complete. In addition, there is no gold standard questionnaire to detect mental disorders in university students. The K6 questionnaire consists of only six items, can be completed in only 1 to 2 min, and has shown good acceptability even in busy situations (Sakurai et al., 2011). Furthermore, the K6 has an excellent capacity to detect mood and anxiety disorders in adults (Furukawa et al., 2008; Kessler et al., 2002; Sakurai et al., 2011) and youth (Ferro, 2019). Kessler et al. tested an initial pool of 612 items using a U.S. national mail survey (n = 1,401) and then reduced these to six items that were tested in a U.S. national telephone survey (n = 1,574) (Kessler et al., 2002). The K6 was subsequently included in the U.S. National Health Interview Survey in 1997 (n = 36,116) and 1998 (n = 32,440), and the scale strongly discriminated between cases of DSM-IV (APA, 1994)/Structured Clinical Interview disorders (AUC = 0.879; Kessler et al., 2002). Moreover, Kang et al. (2015) reported the value of using the K6 for detecting severe mental illness in undergraduates. Therefore, although the K6 is quite a simple questionnaire, its capacity to detect mood and anxiety disorders is reliable regardless of generation. In the present study, we searchingly developed a short and general questionnaire including K6 (Supplementary Table 1) for the first simple screening for mental disorders in new university students. The K6 score tended to be higher in students with several compulsive/paranoid/referential ideas and physical complaints, and with depressive and anxious items at admission. Furthermore, K6 scores were significantly higher 6 months after admission. This may reflect increased mental stress after admission. Higher K6 scores at admission could discriminate students with suicidal ideation not only at admission but also at 6 months after admission. Therefore, we believe that current and future suicidal ideation in addition to severity of anxiety and depressive mood are properly evaluated by the K6 questionnaire, and we can follow up these students thereafter with more specific assessments. As for the severity grades of suicidal ideation, we found a lot of students with suicidal ideation who answered as “a little of the time (Score 1).” The number of these students were 2 to 3 times higher than that of students who answered as “some of the time (Score 2),” “most of the time (Score 3),” or “all of the time (Score 4).” Therefore, to reduce the rate of “false positive,” it is expected to be reasonable that we defined the Scores 2 to 4 as positive for significant suicidal ideation in the present study.
The prevalence of autism is recently increasing (Weintraub, 2011), and both ASD and ADHD are frequently found even in college students (Takahashi et al., 2016). Although the causes of autism have not been fully elucidated, both genetic and environmental factors affect pathogenesis and deterioration (Weintraub, 2011). Jackson et al. (2018) reported that 71.4% of post-secondary students with ASD, mainly Asperger’s syndrome, were studying at 4-year university courses, and over three quarters of such students felt isolated, left out, and lacked companionship. Surprisingly, nearly three quarters of these students showed lifetime suicidal behaviors (Jackson et al., 2018) compared with 3.4% of suicidal ideation in first-year university students (Blasco et al., 2019). Marked changes in lifestyle and social relationships after university/college admission, in addition to substantial study burden, may affect ASD and ADHD conditions. Therefore, increased mental stress generated by these environmental changes may have induced higher K6 scores at 6 months after admission in our participants. The 50-item AQ questionnaire has been widely used to detect autism (Baron-Cohen et al., 2001; Hoekstra et al., 2008; Kitazoe et al., 2015; Sizoo et al., 2015; Woodbury-Smith et al., 2005). In the current study, K6 scores were positively correlated with AQ scores. Therefore, high K6 scores may be able to discriminate students with autistic traits from those without.
This study has several limitations. First, only 341 students were included. Second, participants were drawn from only one medical university. Third, the current results indicated the Score 3 of K6 as a useful cutoff score to differentiate students with suicidal ideation from those without. However, the Score 3 of K6 is deemed to be within normal range (Sakurai et al., 2011), and a future large-scale study is needed to test the reliability of this cutoff score. Finally, full psychiatric diagnoses of ASD or ADHD were not obtained, or ASD- or ADHD-related items on this questionnaire were not validated. A larger collaborative study with precise ASD/ADHD diagnosis in an independent population other than medical university students should be conducted to overcome a lack of statistical power and to determine the utility of the K6 in future.
Conclusion
The present study showed that medical university students with suicidal ideation had significantly higher K6 scores than those without, particularly at 6 months after admission. K6 scores were positively correlated with ASD- and ADHD-related scores. Finally, K6 scores were positively correlated with AQ scores. The K6 questionnaire is easy to administer and could be useful in detecting university students with suicidal ideation or autistic traits. Further studies are needed to confirm the utility of the K6 for detecting mental disorders in university students.
Supplemental Material
sj-pdf-1-sgo-10.1177_2158244021994590 – Supplemental material for Kessler Psychological Distress (K6) Questionnaire Scores Can Predict Autistic Traits and the Current and Prospective Suicidal Ideation in Medical University Students: A Prospective Study
Supplemental material, sj-pdf-1-sgo-10.1177_2158244021994590 for Kessler Psychological Distress (K6) Questionnaire Scores Can Predict Autistic Traits and the Current and Prospective Suicidal Ideation in Medical University Students: A Prospective Study by Yumi Naito, Noriyuki Enomoto, Yosuke Kameno, Hidenori Yamasue, Takafumi Suda and Yoshihiro Hotta in SAGE Open
Supplemental Material
sj-tiff-2-sgo-10.1177_2158244021994590 – Supplemental material for Kessler Psychological Distress (K6) Questionnaire Scores Can Predict Autistic Traits and the Current and Prospective Suicidal Ideation in Medical University Students: A Prospective Study
Supplemental material, sj-tiff-2-sgo-10.1177_2158244021994590 for Kessler Psychological Distress (K6) Questionnaire Scores Can Predict Autistic Traits and the Current and Prospective Suicidal Ideation in Medical University Students: A Prospective Study by Yumi Naito, Noriyuki Enomoto, Yosuke Kameno, Hidenori Yamasue, Takafumi Suda and Yoshihiro Hotta in SAGE Open
Supplemental Material
sj-tiff-3-sgo-10.1177_2158244021994590 – Supplemental material for Kessler Psychological Distress (K6) Questionnaire Scores Can Predict Autistic Traits and the Current and Prospective Suicidal Ideation in Medical University Students: A Prospective Study
Supplemental material, sj-tiff-3-sgo-10.1177_2158244021994590 for Kessler Psychological Distress (K6) Questionnaire Scores Can Predict Autistic Traits and the Current and Prospective Suicidal Ideation in Medical University Students: A Prospective Study by Yumi Naito, Noriyuki Enomoto, Yosuke Kameno, Hidenori Yamasue, Takafumi Suda and Yoshihiro Hotta in SAGE Open
Footnotes
Author Contributions
N.E. contributed in conception and design of the study. Y.N. helped in the acquisition of data. N.E., Y.N., Y.K., H.Y., T.S., and Y.H. helped in the analysis and interpretation, and contributed to the drafting of the manuscript for important intellectual content. All authors reviewed the manuscript and approved for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.