
Abstract
Teachers are often the first persons responsible for identifying children with attention deficit hyperactivity disorder (ADHD) and are increasingly being called on to help manage such children. We sought to assess teachers’ knowledge of and attitudes toward ADHD in Trinidad & Tobago, a small island developing state in the Caribbean region. Based on previously published work, an instrument was adapted and pilot tested. Using convenience sampling, 440 questionnaires were distributed and 277 valid questionnaires were returned (response rate, 63%). Total knowledge scores were low, mean 12.6/26. Both postgraduate education and in-service training significantly improved knowledge scores as did having previously taught a child with ADHD. Attitudes toward children with ADHD were generally positive although most teachers felt children with ADHD should be taught by specialist teachers. Results suggest greater efforts must be made to provide teacher training specifically in the identification and management of children with ADHD.
Attention deficit hyperactivity disorder (ADHD) is reportedly the most pervasive disorder of childhood affecting approximately 3% to 5% of school-aged children with prevalence rates increasing significantly over the past two decades (Pastor & Reuben, 2008; Timimi & Radcliffe, 2005). Children with ADHD experience symptoms of inattention, hyperactivity, or impulsivity above and beyond what is developmentally appropriate. While it is usually first diagnosed in childhood, many children diagnosed with ADHD demonstrate symptoms that persist into adolescence and adulthood (Langley et al., 2010).
Inattention may manifest in social, occupational, and academic settings. Symptoms include difficulty with sustained attention, being unable to complete tasks, not following through on instructions and requests, and inability to complete chores and schoolwork. Symptoms of hyperactivity include fidgeting, inability to sit still in classroom settings, being always “on the go,” and excessive talking, while a symptom of impulsivity is difficulty waiting their turn. It should be noted that in the new Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013) criteria, children can be diagnosed with ADHD up to age 12 and not age 6 as was previously recommended, while several symptoms must occur in more than one setting.
Epidemiological data suggest the incidence of ADHD has significantly increased over the past two decades. This coupled with the fact that over the last 40 years, a preponderance of the research on ADHD has come out of the United States has led many to believe that ADHD is a disorder rooted in cultural and social factors apparently prevalent in the United States (Faraone, Sergeant, Gillberg, & Biederman, 2003; Timimi & Taylor, 2004). However, more and more research is emerging that suggests ADHD is a global concern. Indeed, pooled prevalence rates across several continents suggest a prevalence rate of more than 5% (Polanczyk, Silva de Lima, Horta, Biederman, & Rohde, 2007), a result supported by a recent meta-analysis (Willcutt, 2012). For the purposes of this report though, it is worth noting that little or no epidemiological data exist from the Caribbean region.
Despite these figures, failure to identify the underlying biological deficits, a growing distrust of the medical and pharmaceutical fraternities, and cultural variations ensure that ADHD remains a condition fraught with controversy (Stolzer, 2009). This is not helped by schisms within the research community and among the various stakeholders (Kildea, Wright, & Davies, 2011).
The Role of Teachers
Unfortunately, argument notwithstanding, the disruption produced by ADHD typed behaviors is undisputed. ADHD behavior tends to worsen in environments where attention for long periods of time, quiet activities, and waiting one’s turn is required (APA, 2013). Such behaviors are required within the formal classroom setting, and if other opportunities such as physical activity are not provided to balance learning strategies, behavioral difficulties can often first be encountered in school. Typically, children with ADHD are characterized as being disruptive in the classroom, have conflictual relationships with family and peers, are unable to understand or conform to social cues, and experience academic challenges, which ultimately affect their quality of life (Bender & Smith, 1990; Frick et al., 1991; Hinshaw, Heller, & McHale, 1992). Importantly, while the initial difficulties of inattention and classroom disruption associated with primary school diminish in secondary school, secondary school students with ADHD often experience academic challenges and the frustrations associated with reduced performance (Travell & Visser, 2006). All of these conditions mean that students with ADHD are often at greater risk of school drop-out and academic failure (Bussing, Mason, Bell, Porter, & Garvan, 2010; Merrell & Tymms, 2001).
Such findings highlight the important role that teachers play in identifying children who need additional support, making referrals for their assessment, and being able to manage them in the classroom (Sherman, Rasmussen, & Baydala, 2008). As such, within recent years, there has been an increasing emphasis on teachers’ knowledge and attitudes toward ADHD. Several studies from different parts of the world have found that teachers’ knowledge is at best reasonable and in many cases, insufficient, requiring intervention (Ghanizadeh, Bahredar, & Moeini, 2006; Nur & Kavakc, 2010; Perold, Louw, & Kleynhans, 2010; West, Taylor, Houghton, & Hudyma, 2005).
Due to the challenges that a child with ADHD may present, it is also not surprising that there are reports that teachers’ attitudes toward children with ADHD may be negative. Teachers presented with a description of a child with an ADHD label viewed that child significantly less favorably than a child without an ADHD label in the domains of behavior, intelligence, and personality (Batzle, Weyandt, Janusis, & DeVietti, 2010). Similarly, teachers experienced more negative expectations of children in ADHD labeled vignettes, rating them as having more serious problems and their behavior as more disruptive to the classroom (Ohan, Visser, Strain, & Allen, 2011).
The Local Context
Trinidad & Tobago (TT) is a twin-island republic that lies in the southern-most part of the Caribbean, off the northeast coast of Venezuela (Central Intelligence Agency, 2012). Two major ethnicities make up its heterogeneous population, 40% Indian and 38% African, with the rest hailing from Europe, China, and the Middle East. Considered the wealthiest nation in the Caribbean, due in large part to investments in petrochemicals, natural gas, and steel, TT has become a key player on the global stage and as such is highly influenced by global culture, in particular, North American culture. The education system, which is publically funded, is heavily influenced by its British colonial past. Children enter primary school at age 5 and are required to spend 7 years before writing an examination, which will determine entry into secondary school. There is tremendous competition for places at a few so-called “prestige secondary schools.” This has resulted in a heavy focus on academic development during primary school and extreme demands being placed on the children. In many cases, children attend additional lessons to prepare for the primary school leaving examination.
With respect to ADHD, there is a paucity of research conducted in the Caribbean as a whole (Polanczyk et al., 2008; Pottinger, La Hee, & Asmus, 2009) but the proximity to North America and its cultural influence ensures at least some awareness exists. Awareness, however, does not necessarily mean acceptance, and for the average man on the street in TT, anecdotal evidence suggests that ADHD is viewed as a myth and an excuse for children’s misbehavior. Teachers may not be exempt from this belief. However, because teachers most often are among the first to interface with children experiencing ADHD symptoms, one can hypothesize that they are more likely to accept ADHD as a valid diagnosis. Importantly, formal teacher training is not mandatory prior to beginning service in the education sector. It is also worth noting that in the Caribbean, like in many other parts of the world, discriminatory attitudes still exist with respect to mental and neurological illnesses (Youssef et al., 2014; Youssef et al., 2009).
Given the growing prevalence and recognition of ADHD and the important role that teachers play in first identifying the condition, we sought to assess teachers’ knowledge and attitudes toward ADHD in TT. We believe the significance of this work lies not only in adding to the very limited data set on ADHD in the Caribbean region but also in identifying gaps in the training of teachers. Such information is critical in helping shape teacher training and raising the profile of the condition.
Method
This was a cross-sectional descriptive survey that made use of convenience sampling designed to assess primary and secondary school teachers’ knowledge of and attitudes toward ADHD. Ethical approval for this study was received from the Ethics Committee of the Faculty of Medical Sciences, the University of the West Indies.
Instrument
A self-report questionnaire used in previous reports (Kos, Richdale, & Jackson, 2004; Sciutto, Terjesen, & Frank, 2000) was adapted for use in this study based on the authors’ review and feedback from a pilot study. The final instrument contained three sections. The first (Section A) collected demographic information about each respondent including age, sex, teaching experience, and teacher training. Section B was intended to attain teachers’ actual knowledge of ADHD and contained 26 questions with true, false, and don’t know options. Several questions were worded in the negative to prevent random completion by participants. One point was awarded for each correct answer and the results for each question summed to yield a total knowledge score. The maximum possible score was therefore 26. For this analysis, both wrong answers and don’t know were considered incorrect although the summary of each response is also presented.
Section C assessed teachers’ beliefs about and attitudes toward ADHD by the use of 25 statements. A 5-point Likert-type scale was used in this section with teachers indicating whether they agreed, strongly agreed, neither agreed nor disagreed, disagreed, or strongly disagreed with the statement. Several items were again reverse scored to ensure conscious completion of the questionnaires. For each question, the mean and standard deviation were calculated with scores closer to 1 indicating that participants agreed with the statement and scores closer to 5 indicating that participants disagreed.
Procedure
Schools were selected by convenience sampling based on a prior relationship of the researchers with a teacher in the school. Overall, teachers from 29 schools took part in the study. Four hundred and forty (440) packages were prepared each containing a letter of instruction, a consent form, and a self-report questionnaire. This representative teacher received a number of packages and distributed them to his or her colleagues who were asked to complete them on a voluntary basis. Questionnaires were distributed to and left with potential respondents for a period of 2 weeks, from the time of delivery and collected by the representative and delivered to the research team. For the sake of anonymity, teachers were asked to separate consent forms from questionnaires. Both were then returned to the researcher in separate envelopes.
Data Analysis
Data were collated and analyzed using the statistical software SPSS Version 17.0. To ensure anonymity, raw data from the questionnaires were coded and inserted into the three sections for analysis: (a) general demographic information, (b) knowledge scores, and (c) attitude scores. Descriptive statistics were calculated for each section of the questionnaire (M + SD), and differences in means were tested using a one-way ANOVA. Post hoc analysis was carried out using Tukey’s post hoc test. The alpha error was set at p < .05.
Results
Of the 440 questionnaires distributed, 289 were returned. Twelve questionnaires were discarded because participants did not complete at least one full section of the questionnaire giving a final sample size of 277 and a response rate of 63%.
Demographic Information
The final sample consisted of 277 primary and secondary school teachers from 16 primary (n = 116) and 13 secondary (n = 155) schools drawn from North, East, and Central Trinidad. The age of teachers ranged from 21 to 62 years with a mean age of 39 years (SD = 9.0 years). Of those sampled, 74% (n = 206) were female and 22% (n = 61) were male teachers. Years of teaching experience ranged from 6 months to 41 years with a mean of 14.5 years (SD = 9.5). With respect to having taught a child with ADHD, 48% (n = 132) of teachers responded that they had taught a child with ADHD, while 9% (n = 25) responded that they had not taught a child with ADHD and 42% (n = 116) did not know whether they had taught a child with ADHD. Of the teachers who indicated that they had taught a child with ADHD, just under half or 48% indicated that the diagnosis had been confirmed by a medical professional.
Knowledge of ADHD
Prior to answering the knowledge questions, teachers were asked to indicate using a percentage, their perceived knowledge of ADHD. Responses ranged from 0% to 99% with a mean score of 36% (SD = 26). Twelve teachers (4%) indicated they had no knowledge of ADHD.
Twenty-six questions were used to assess knowledge. Given that this was the first time this instrument was used in our population, we sought to test its reliability; this yielded a Cronbach’s alpha score of 0.86 suggesting good to excellent internal consistency in our population. Overall, the mean total knowledge score was 11.6 (SD = 5.5). This corresponds to 45% of the questions right. Total scores ranged from a minimum of 0 to a maximum of 23 with 12 teachers scoring 0 on total knowledge while 40% of the entire sample had a score of 10 or less. The percentage responses to all questions are summarized in Table 1.
Teachers’ Percentage Response (Total Number of Teachers) to Knowledge Items.

Note. T and F denote which items were coded True and False, respectively. ADHD = Attention deficit hyperactivity disorder.
Several factors seemed to influence the total knowledge score (see Table 2). In particular, there was a significant effect of education level, F(4, 211) = 4.51, p < .01, on the total knowledge score. Teachers with a master’s degree scored the highest and those with no formal training beyond secondary school the lowest. Perhaps more significantly, persons who received training in ADHD while teaching scored significantly higher than those who did not, p < .001. Having taught someone with ADHD also had a significant effect, F(2, 270) = 5.6, p < .01, as did the type of school in which the teachers taught, p < .01. However, gender did not have an effect on total knowledge scores, p > .05.
Difference in Knowledge Scores Based On Key Teacher Characteristics.

Note. ADHD = Attention deficit hyperactivity disorder.
There was a moderate correlation between teachers’ perceived knowledge of ADHD and actual total knowledge score. Pearson’s correlation coefficient was 0.48, and this was significant at p < .001. This trend is summarized in Figure 1.

Teachers’ Perceived Knowledge vs Actual Performance on Knowledge Sub-scale.
Attitudes Toward ADHD
The mean scores for the 25 items are summarized in Table 3. Overall, teachers generally viewed ADHD as a valid diagnosis and a legitimate educational issue (Items 1 and 9). This is also reflected by the response to Items 19, 2, and 25 in which they indicate that children are generally not responsible for their behavior. However, teachers also felt that children with ADHD are disruptive to the class and were best taught by special education teachers (Items 10 and 12).
Teachers’ Attitude Scores (M + SD).
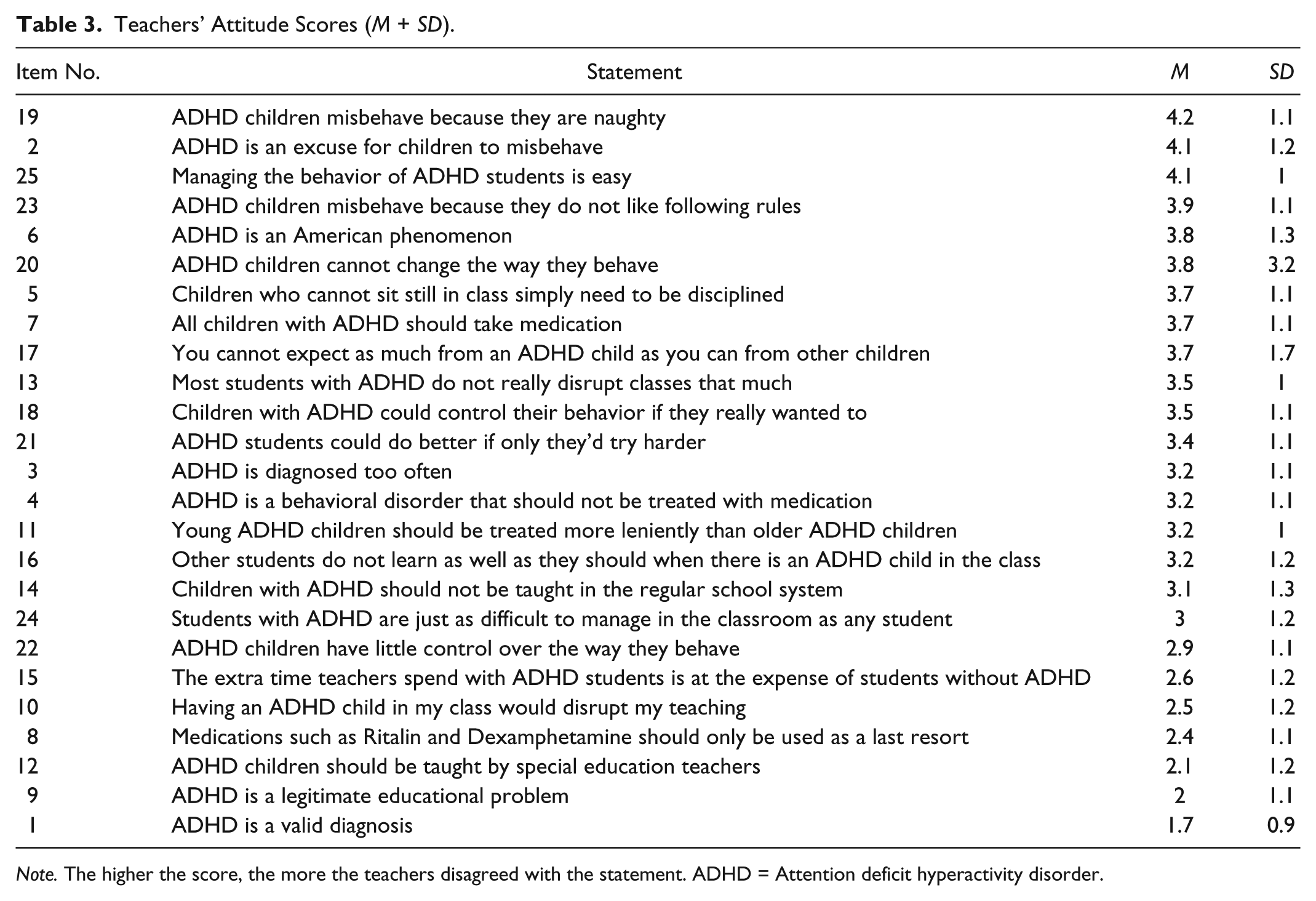
Note. The higher the score, the more the teachers disagreed with the statement. ADHD = Attention deficit hyperactivity disorder.
Discussion
We report that TT teachers’ knowledge about ADHD was low with the mean total knowledge score being less that 50% correct. This is consistent with research conducted in both developed and developing nations. In fact, the scores are remarkably similar to data from South Africa and Sri Lanka, which also report knowledge scores below 50% (Perold et al., 2010; Rodrigo, Perera, Eranga, Williams, & Kuruppuarachchi, 2011). Importantly though, our study found that a majority of teachers chose the “don’t know” option as opposed to incorrect answers, which may indicate a greater level of uncertainty about the facts, rather than a high level of misperception about ADHD. This is a significant point to note for future training purposes as it is often easier to educate persons who do not have inaccurate, preconceived ideas about a subject (DiBattista & Shepherd, 1993).
The exact reasons for these low scores are not clear, but the data do suggest that a lack of education may be critical. Teachers with a master’s level education scored highest, as did those who received training specifically concerning ADHD while teaching. This latter point is especially important as short-term interventions (1 week) and web-based interventions have been shown to rapidly improve knowledge about ADHD, with benefits lasting for at least 6 months (Aguiar et al., 2014; Barnett, Corkum, & Elik, 2012; Jones & Chronis-Tuscano, 2008; Syed & Hussein, 2010). Given that, in our study, teachers’ perceived knowledge was positively correlated with actual knowledge, it suggests that teachers are aware of their lack of knowledge and potentially open to ADHD training.
Having taught a child with ADHD significantly affected knowledge scores, findings in keeping with other research (Kos et al., 2004; Sciutto et al., 2000). Perhaps the challenges of teaching children with ADHD triggered teachers to seek out information and additional training resources, again a very positive finding in the context of future training interventions.
Knowledge scores were also higher among primary school teachers than among secondary school teachers. ADHD is generally considered to be a disorder among younger children, while older children demonstrating ADHD typed behavior are often labeled truant and rebellious (West et al., 2005). Finally, similar to other research (Kos et al., 2004), neither age nor gender was found to have an impact on total knowledge scores. It is noteworthy that although there was no significant difference in knowledge levels between male and female teachers, the sample was overrepresented by female teachers, highlighting the high ratio of female to male teachers within the Trinidadian context. This is not dissimilar to an observation made in Australia, that ADHD, a disorder affecting mainly males, is being dealt with primarily by females (Bekle, 2004).
Attitudes Toward ADHD
Given the controversy surrounding ADHD (Baughman, 2006; Stolzer, 2009; Timimi & Radcliffe, 2005; Timimi & Taylor, 2004), the findings of this study were encouraging, demonstrating that Trinidadian teachers believe that ADHD is a valid diagnosis and that ADHD is a legitimate educational issue. It also appears that low knowledge of the disorder does not affect beliefs in the validity of the diagnosis. This is in sharp contrast to reports from other developing nations in which attitudes were generally more negative (Ghanizadeh et al., 2006; Perold et al., 2010; Rodrigo et al., 2011). Not only is this finding important for future management of children in the classroom but also because teachers can be utilized to help educate parents and the wider society, serving as a human resource cadre for dispelling myths concerning ADHD.
While teachers recognized the validity of ADHD, they tended to believe that children displaying ADHD typed behavior should be taught by special education teachers. This is in sharp contrast to the TT government’s stated objectives to promote an inclusive education system and recent data from the United Kingdom in which teachers were very much concerned that children with ADHD be managed within the general school system (Moldavsky, Pass, & Sayal, 2014). Such unwillingness on the part of Trinidadian teachers to engage children with ADHD probably reflects their belief that they are disruptive in the regular classroom setting, but perhaps, more importantly, an underlying sense of their own inability to manage ADHD behavior in the classroom.
Limitations
Our study is limited by the use of a convenience sample, drawing teachers generally from North, East, and Central Trinidad. Thus, there may be overrepresentation or underrepresentation of some members of the sample, thereby potentially limiting this study’s generalizability. In particular, the southern part of the country and Tobago are more rural and as such, teachers may be less likely to have training with respect to ADHD. Given that scores were already low, this probably would not have altered the findings and conclusions of this report significantly.
The questionnaire used was a self-report questionnaire. While self-report questionnaires are easily administered and relatively easy to analyze, there may be a tendency to respond in keeping with socially accepted norms. However, as highlighted in the article, teachers were very open in admitting their lack of knowledge and their positive attitudes toward ADHD in contrast with the controversy surrounding the diagnosis. Finally, data collection for this study took place before the end of the school term, a time when teachers were more busy that usual with their duties. This reality possibly affected the number of completed questionnaires returned, and within this context, it is possible that the teachers who did complete the questionnaires may have had prior interest in ADHD.
Conclusion
Overall, teachers’ knowledge about ADHD was low. While there is a profound lack of epidemiological data concerning ADHD within the region, there is no reason to presume that prevalence rates are lower in the Caribbean compared with elsewhere in the world. Therefore, there is a need for teachers within the region to become more educated about the condition and better equipped to deal with these children. In-service education concerning ADHD has been found to significantly improve knowledge, attitudes, and management skills among teachers, a finding supported by our data. Given that teachers in our study also demonstrated positive attitudes toward ADHD, we recommend that in-service training concerning ADHD and other childhood developmental disorders be incorporated within the education system. It is expected that such interventions can increase identification of children with ADHD, give teachers greater confidence in their ability to manage these children, and improve overall classroom management within the schools.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The authors thank the University of the West Indies for financial support