
Abstract
Nigeria is the most populous country in Africa and the eight most populous nation in the world. She is currently the largest economy in Africa. Nigeria is considered to be relatively wealthy in terms of oil reserves; however, the level of poverty is still very high because of corruption and mismanagement. This study investigates the impact of public health expenditure on health outcomes in Nigeria, 1985–2019. Empirical results from the Classical Regression Analysis reveal that health expenditure by the government reduces under-5 mortality rate significantly and improves life expectancy. Furthermore, immunization against measles was found to reduce under-5 mortality rate, while prevalence of HIV reduces life expectancy. The study therefore recommends that there is need for government expenditure on health to be targeted at areas that will improve health outcomes significantly. With adequate funding and proper monitoring, a resource-abundant nation like Nigeria, can become healthier. However, if this is not done, the wealthy may not be healthy after all.
Background and Motivation
The major goal of many economies in the world is to achieve sustainable economic growth and development. To accomplish this goal, certain variables which have the capacity of helping the economy to grow and develop will have to be put in place. Good health has been seen as one of the important variables and necessary conditions for the attainment of growth and development of any economy (Hlafa et al., 2019; Ogunjimi & Adebayo, 2018). A healthy workforce is known to be a productive workforce; therefore, the quality of health in the economy determines the kind of economic activities that will be inherent in the economy. Nigeria is the most populous country in Africa and the eight most populous nation in the world. She is currently the largest economy. Nigeria is considered to be relatively wealthy in terms of oil reserves; however, the level of poverty is still very high because of corruption and mismanagement. Taxes are unrequited because benefits provided by the government to taxpayers are not in proportion to their payment, while the corruption perception of the country remain overtime high. The human capital development (health and education) remains weak leading to under investment in health care funding also caused by fluctuation in oil revenue. The country was ranked 27th largest economy in terms of nominal GDP and 24th largest in terms of purchasing power parity in the world with debt to GDP ratio of 16.075% in 2019 by the World Bank.
Many scholars in Africa and Nigeria in particular have linked health to economic growth. For instance, Onisanwa (2014) and Anyanwu and Erhijakpor (2007) found that health indicators influence the growth of the Nigerian economy positively in the long run. Thus, health indicators have a long run impact on the growth of the Nigerian economy. According to Jack (1999), as cited by Agbatogun and Taiwo (2010), one way in which health affects the growth of the economy is by increasing the productivity of labor since the productivity of labor depends on the physical and mental capabilities, investment in human capital (health and education), and so on. Therefore, since health is considered one of the necessities for achieving growth and development of the economy, any policy that will help to improve health in the economy will be very vital.
The general health status and outcomes all over the world and Nigeria in particular is measured by life expectancy, maternal mortality rate, under-5 mortality rate, infant mortality rate, still birthrate, crude death rate, and morbidity rate. According to World Health Organization (WHO, 2016b) statistics, Nigeria is ranked 187 out of 191 countries in its ranking of the world’s health system performance. Nigeria is just better than four countries (Democratic Republic of Congo, Central African Republic, Myanmar and Sierra Leone) out of 191 countries. Countries like Chad (178th), Cameroon (164th), Botswana (169th), Niger (170th), South Africa (175th), and Ghana (135th) are all ranked ahead of Nigeria. According to Tandon et al. (2016), the performance of the countries was based on their ability to achieve a broader set of health system outcomes which include improvement in population health, financing of health care, and so on.
The main reason why Nigeria has a health system that has performed poorly is because the primary health care in Nigeria which is the most important level of care has been left to the weakest level of government and this gave rise to weak and disorganized health care system thus affecting population health (Osain, 2011). To show more clearly the health status of the Nigerian economy, Table 1 compares some health outcome indicators in Nigeria to that of some other developing countries.
Health Outcome Indicators in Nigeria and Some Other Developing Countries.
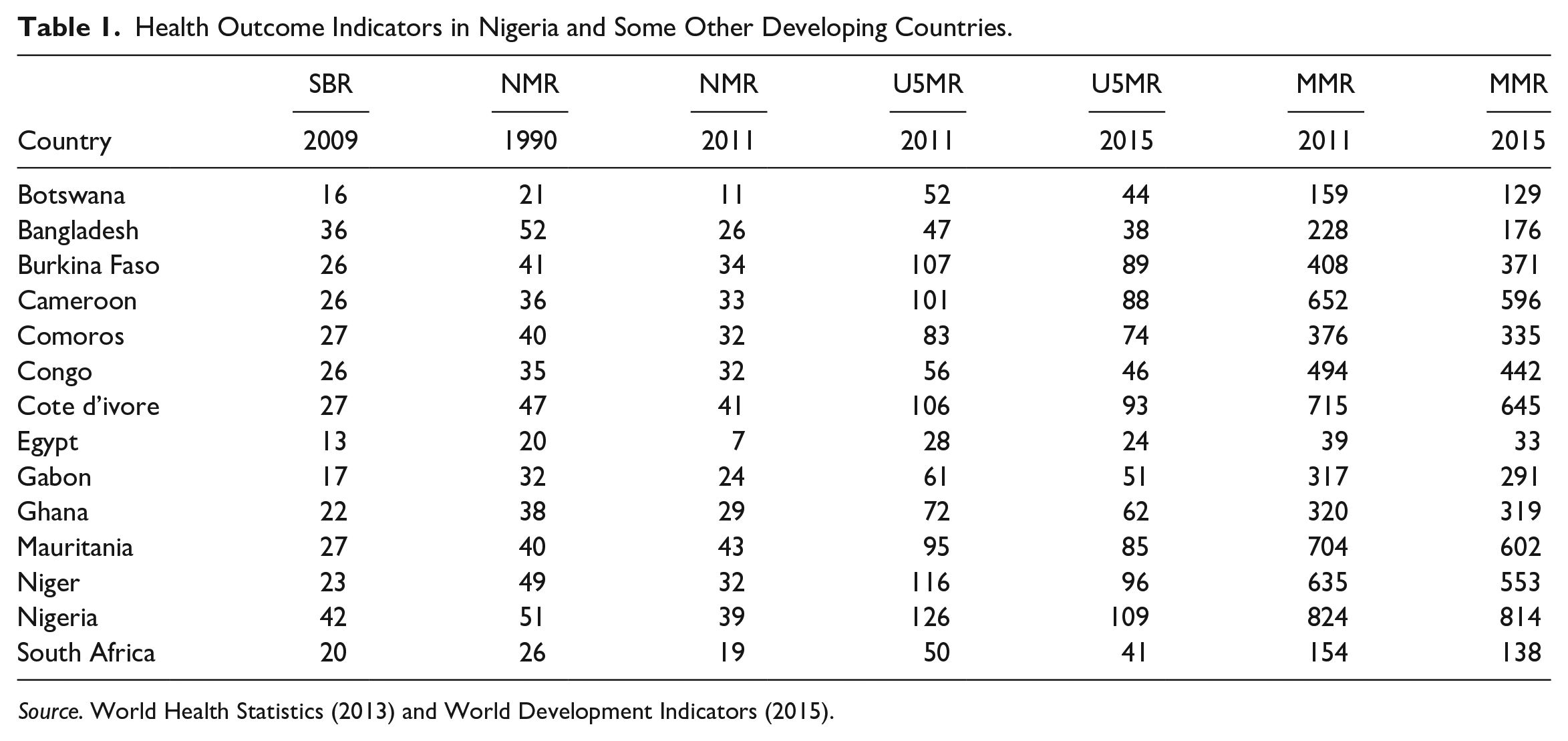
The Table 1 shows the health outcome indicators of some developing economies. SBR represent still birthrate, NMR represent neonatal mortality rate, U5MR represent under-5 mortality rate, and MMR represent maternal mortality ratio. From the Table 1, Nigeria has the highest maternal mortality ratio, highest under-5 mortality ratio and highest still birthrate as compared with other countries in the table. Also, countries like Burkina Faso which is ranked 183, Uganda which is ranked 166, Cameroon which is ranked 153 in health system performance all have better health outcomes compared with Nigeria for the various years from under comparison.
Investment in health, on the other hand, has been shown by many scholars to have a statistically significant effect on health outcome indicators (life expectancy, mortality, morbidity, etc.) of the Nigerian economy. For instance, studies like Okeke (2014), Nwankwo (2012), Orji et al. (2015), Novignon et al. (2012), Anyanwu and Erhijakpor (2007), Makute and O’Hare (2015), and so on have shown that public health spending has a relationship with public health outcomes. However, the nature of these relationships still remains an empirical puzzle that needs to be validated with recent data. Public health spending or public expenditure on health refers to expenditure on health care incurred by public funds. Public funds include that of local, state, regional, and federal Government bodies and social security schemes. Thus, public health care spending has a vital role to play in improving the health status of the Nigerian economy. According to Abimbola (2012), the financing of health care in Nigeria is highly connected to the funds that flow from the federation account. Funds are shared between levels of government following a constitutionally agreed formula. Health care financing in Nigeria is done by both government and private sectors. Public health expenditure in Nigeria according to Lambo (2015) is less than $8 per capita compared with the $34 recommended internationally. Also, according to World Bank Statistics (2016), expenditure on public health as percentage of total government expenditure is 8.1%, public health expenditure as percentage of total health expenditure (both private and public) is 25.1%, and public health expenditure as percentage of GDP is only 3.6%. Out-of-pocket expenditure on health in Nigeria, on the other hand, is 95.7% of expenditure on private health and 71.6% of the expenditure on total health, despite the nature of poverty in the economy (World Bank Statistics, 2016). This shows clearly that financing of health care in Nigeria is mainly out of pocket. This is seen more clearly in Figure 1.
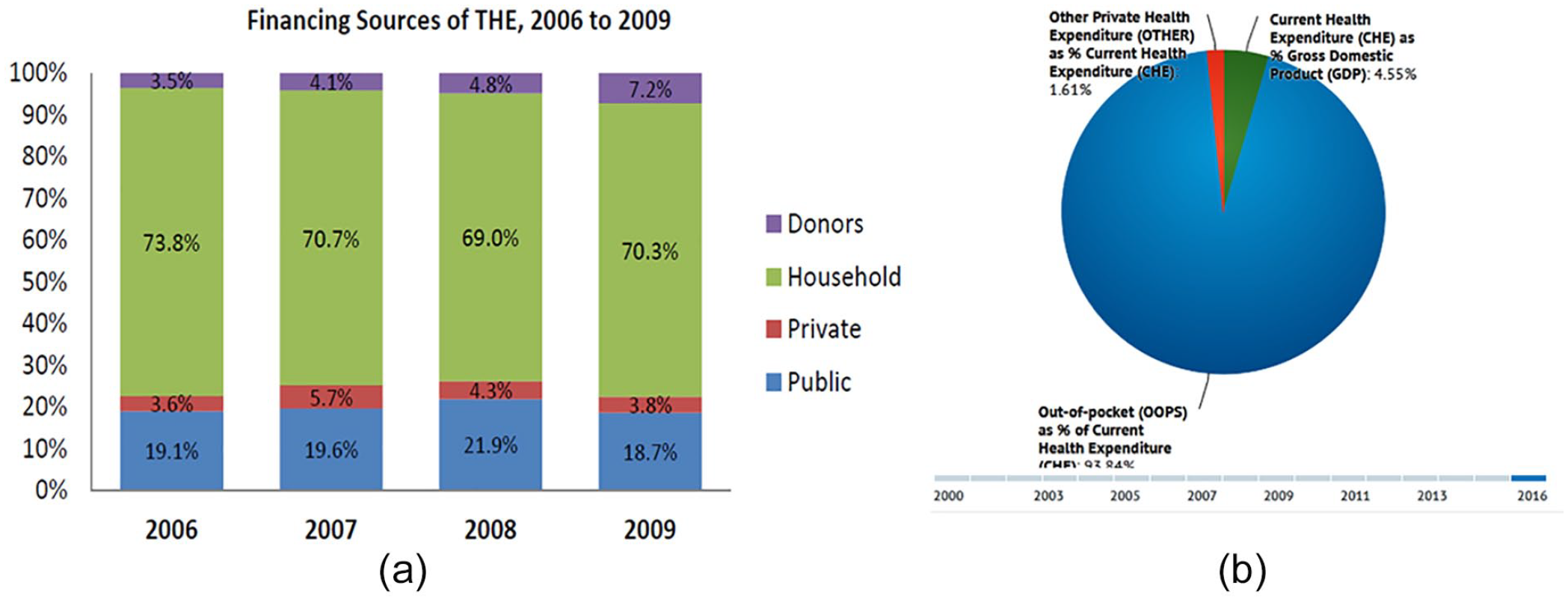
Financing sources of the total health expenditure from (a) 2006 to 2009 and (b) 2000 to 2016.
Out-of-pocket health expenditure (% of total expenditure on health) in Nigeria was 71.67% as of 2014. Its highest value over the past 19 years was 75.23 in 1996, while its lowest value was 60.48% in 2008.
Figure 1a shows the financing sources of total health expenditure from 2006 to 2009, and Figure 2 specifically shows the total public expenditure on health as compared with out-of-pocket expenditure on health in Nigeria from 1995 to 2014. From Figure 1a, out-of-pocket household expenditures made from personal wallets as a percentage of public expenditure on health is the highest with figures ranging from 73.8%, 70.7%, 69.0%, to 70.3% for 2006, 2007, 2008, and 2009, respectively. Second to the highest is public expenditure on health as a percentage of expenditure on total health with figures ranging from 19.1%, 19.6%, 21.9%, and 18.7% for 2006, 2007, 2008, and 2009, respectively. The third and fourth are expenditures from other private sources and donors on public health as a percentage of expenditure on total health in Nigeria with figures ranging from 3.5% to 7.2% for both categories from 2006 to 2009. When we isolate some other sources of health financing we see from Figure 1b that from 2000 to 2016 current health expenditure as Gross Domestic Expenditure on average was 4.55%, while other private health expenditure as percentage of current health expenditure was 1.61%. Interestingly, out-of-pocket expenditure took the largest chunk of 93.84%. However, when we include other sources, this figure reduces. This truly shows that health expenditure in Nigeria is mainly financed out of pocket, meaning that government contribute only small fraction of its resources to financing health in Nigeria and this may be contributing to the poor health system performance that we have in the economy. Figure 2 shows that out pocket expenditure ranged from 72% to 75% (1995 to 2014).

Total public expenditure on health as compared with out-of-pocket expenditure on health in Nigeria from 1995 to 2014.
Moreover, comparing expenditure on public health as percentage of GDP in Nigeria with some other developing nations (on Table 2) also show that Nigeria is one of the lowest country in terms of the value of their Gross Domestic Product devoted to improving health in the economy. Countries like Niger, Ghana, Coted’ Ivore, and so on all contribute more of their resources to health than Nigeria. It is also seen from the table that expenditure on public health as a percentage of GDP in Nigeria declined over the years from 2011 to 2014. It was 1.2% in 2011 but dropped to 1.0 in 2013 and further to 0.9 in 2013 and 2014.
Expenditure on Public Health as a Percentage of GDP in Some Developing Countries.

Source. World Development Indicators (2014).
Note. GDP = gross domestic product.
However, it is very important to note that the fact that we have a poor health outcome in the economy does not mean that Nigerian government is not making any effort to promote the health status of its citizens. Apart from the federal allocations to the health sectors of the economy, Nigerian government has made considerable efforts so far to improve the health status of its citizens. Also, the former Nigerian president Jonathan in 2012 launched the Saving One Million Lives Initiative. The aim of the initiative includes, first, to improve newborn, child health and maternal health. At the primary health care centers, this was to be achieved by providing different support programs. Second, it aimed at promoting access to skilled health care provider, improving routine immunization coverage, eradicating poliomyelitis, and improving child nutrition. Third, it aimed to prevent the transmission of HIV from mothers to children. This was to be achieved by increasing access to quality treatment and counseling to infected mothers, including HIV testing. Fourth, the initiative aimed at strengthening logistics and supply chain management in the health system, increasing access to important medicines in the country, supporting the use of technology and innovations, and finally, it aimed at controlling malaria. This was essentially done by utilizing anti-malaria medications and treated bed nets.
Finally, the Federal Ministry of Health in Nigeria is also making considerable effort to improve the health of the citizens in Nigeria through the establishment of the Nigerian Service Delivery Innovation Challenge (NSDIC) to improve the coverage and quality of Maternal, Child and Adolescent health in Nigeria using innovative means.
According to National Bureau of Statistics (NBS, 2017), the major reasons why these policies have not achieved the stated goals which is to improve population health is because the policies are lopsided in favor of the formal sector of the economy neglecting the informal sector where over 70% of the Nigerians belong to. A good example is the Nigerian Health Insurance Scheme (NHIS) which cover only top government officials and other federal government staff which is just a small fraction of the entire people in the economy. Another important reason why these policies fail to achieve the desired health outcomes is lack of basic education especially among women. According to UNICEF Nigeria (2017), many girls do not have access to basic education in some regions in Nigeria. This is particularly obvious in the northern region. For example, in the North East and North West, up to 80% of the women are considered illiterates and have not really attended schools. Most of these health policies especially the Saving One Million Lives (SOML) initiative and the current Nigerian Service Delivery Innovation Challenge (NSDIC) aim at achieving maternal, reproductive and child health. These policies will do better if the government will empower women and the entire population with the basic knowledge required to be able to access these health care services. Also, according to Osain (2011), the National Primary Health care Development Agency (NPHCDA) in Nigeria has failed to improve health system performance because the primary health care in Nigeria which is the most important level of care, has been left to the weakest level of government. This nonchalant attitude over the health of the populace has given rise to a weak and disorganized health care system thus affecting population health. Political crisis and high rate of corruption in the economy is also one of the major reasons why many health policy fail in Nigeria (Onuoha, 2000, as cited by Pever et al., 2016). Finally, according to Ejughmre (2013), many health policies in Nigeria have failed as a result of the persistent underfunding of the health sector of the economy by the Nigerian government which reflects in the poor health system performance that we have in the economy. In fact, the NBS (NBS, 2017) noted that out of 7.298 trillion of the 2017 budget in Nigeria presented to the national assembly by the president of Nigeria for approval, only 4.17% was allocated to the health sector which is one of the most critical sectors that drive other sectors of the economy. Studies such as Orji and Okechukwu (2015), Orji et al. (2014), and Onisanwa (2014), among others, have been done in the areas of income and health, health and economic growth, among others, but none of the studies cited above focused specifically on public expenditure on health and health outcomes in Nigeria. Against this background and in view of the problems highlighted above, the article investigates the impact of expenditure by the government on health and health outcomes in Nigeria. This is the main objective of this article. Empirical results from the Classical Regression Analysis reveal that health expenditure by the government reduces under-5 mortality rate significantly and improves life expectancy. The rest of the article is structured as follows: The second section dwells on the literature review, the third section is on the methodology, while the fourth section deals with the results and discussion. The final section concludes the article and provides relevant policy recommendations.
Empirical Literature
Several related studies have been done in this area but many researchers have not yet arrived at an agreement on the relationship that exists among the core variables under investigation here. For example, Anyanwu and Erhijakpor (2007) studied the relationship between expenditure on public health, total per capita health expenditure, per capita income, infant and under-5 mortality using panel data. Forty-seven African countries were investigated for the period 1999 and 2004. The study employed robust ordinary least square (ROLS) for the estimation, robust two-stage least square (R2SLS) to account for endogeneity problem, and fixed effect(FE) estimator to account for measurement error and autocorrelation. The results show that total expenditure on health have a statistically significant effect on under-5 and infant mortality. Thus, total expenditure on health is seen as an important factor necessary for health outcome improvement in all countries in Africa. The findings also indicate that other variables like female literacy, HIV prevalence rate, number of physician, and ethnic fractionalization are also crucial for attaining a positive health outcome. HIV prevalence was found to significantly lead to higher infant and child mortality in Africa. This implies that health expenditure alone may not be enough for achieving a good health outcome; there is also need to put all these other variables in place.
In another study, Okeke (2014) found that government expenditure is significant in improving health and expenditure outcome in Nigeria. This was discovered in the study of the impact of expenditure of government on health and education sector outcome. The study, however, employed health and education production function and OLS technique in estimating the parameters of the model. Vector error correction mechanism (VECM) and Engle-Granger was used to check for short run and long run relationship and co-integration between the time series variable. Data for the study are secondary data ranging from 1980 to 2010 and under-5 mortality ratio and total school enrolment rate were used as proxies to measure health and education outcome. The results reveal that the expenditure on health reduces under-5 mortality rate significantly while spending made by government on education had no significant effect on total school enrolment in Nigeria. It was also discovered from the study that female education and per capita GDP has a negative relationship with under-5 mortality rate in Nigeria. This shows that increase or improvement in GDP per capita is necessary for improving health outcomes in the economy. Also from the result educating the females in the economy is suggested to be a powerful tool for reducing under-5 mortality and improving health outcomes in the economy. In another study, Basu et al. (2015) used the OLS and 2SLS techniques to analyze the effect of expenditure of government on infant mortality rate in 31 states in India. The study covered the period 1983–1984 and 2011–2012. Empirically, the results indicate that expenditure on the health of the public as a share of state-level gross domestic product (GDP) is significant for reducing infant mortality rates in India. It was also discovered that increase in literacy rate of the females and the rate of urbanization also supports infant mortality decline.
In South Africa, Hlafa et al. (2019) investigated the association between public health expenditure and health outcomes in South Africa’s nine provinces from 2002 to 2016. Adopting the fixed effects and a random effects panel data estimation technique to control for time effects and individual provincial heterogeneity, the findings elucidated that the relationship between public health expenditure and health outcomes in South Africa varied across provinces depending on provincial management and infrastructure availability. Zahra et al. (2015) developed a model where government health expenditure was interacted with the quality of governance in the nine OPEC countries between 1996 and 2012 and its effect on infant mortality and under-5 was studied. The study showed that expenditure on public health has a negative significant effect on infant and child mortality rate in countries where there is good governance. The equations of the model were estimated using Fully Modified Ordinary Least Square (FMOLS). This analysis from this study implies that in a country where governance is weak, for example, where the level of corruption in the economy is too high, public allocations to different sectors of the economy are likely not going to yield the expected result. This result agrees with the work of Achim et al. (2020), Makute and O’Hare (2015), Yaqub et al. (2012), and Rajkumar and Swaroop (2007).
Furthermore, Arthur (2013) investigated the effect of health expenditure on health outcomes in sub-Saharan African countries from 1995 to 2011, using the Grossman (1972) health capital model in which individuals maximize their utility from the use of health care services. The study also estimates the effect of both the stock of health and investments in health capital on economic growth. The study employed fixed effect model with the Generalized Least Squares Estimator and annual data for 45 countries in sub-Saharan Africa were used. The study used life expectancy at birth, under-5, and infant mortality as proxy for the stock of health and health expenditure as proxy for investment in health capital. The results indicate first that public health expenditure is associated with an improvement in life expectancy and it contributes to reduction in under-5 mortality and infant mortality rate in sub-Saharan African countries. Second, it was found from the study that improvement in health outcomes leads to economic growth in sub-Saharan African countries. Other variables such as disease prevalence (HIV/AIDS, Malaria, and Tuberculosis), poor access to clean water, income (GDP per capita), and immunization against childhood diseases contribute to the poor health outcomes in sub-Saharan Africa. The result on HIV prevalence is in line with the findings of Anyanwu and Erhijakpor (2007) and that of malaria is in line with the findings of Orji et al. (2015). According to Yaqub et al. (2012), expenditure on public health has negative impact on under-5 and infant mortality. The study shows that if corruption reduces there will be an improvement in health status, life expectancy, and reduction of infant and under-5 mortality rate. This implies that for an increase in the expenditure of government on people’s health to be effective in the Nigerian economy, there is the need to address the issue of corruption. The study agrees with that of Zahra et al. (2015), Makute and O’Hare (2015), and Rajkumar and Swaroop (2007).
In Ghana, Azinim et al. (2013) investigated the empirical nexus between health status and expenditure on health from 2001 to 2010 using classical linear regression technique. The findings indicate that expenditure on public health does not have any significant effect on under-5 mortality in Ghana. The result agrees with Kumar et al. (2013) and Filmer and Lant (1999).The study further found that the availability of physician and health insurance are the major determinants of health outcomes in Ghana. Income per capita was found to be insignificant determinant of health status in Ghana and this is in line with the results of Çevik and Taşar (2013). Using panel data from 1995 to 2010 covering 44 countries in sub-Saharan Africa, Novignon et al. (2012) studied expenditure on health care and its effect on population health status in sub-Saharan African countries. Mortality rate of infants, crude death rates, and life expectancy were used as proxy to measure health status or outcomes. Generalized Least Squares (GLS) was used to estimate the random effects model while the pooled least squares was adopted to analyze the fixed effects model. Their results indicate that total health care expenditure significantly influences health status in sub-Saharan African countries by improving life expectancy at birth, reducing infant mortality, and crude death rate. It was also found from the study that private, public, and total health spending all influences health outcomes in sub-Saharan Africa with public spending having a greater influence than private and total health spending. From the result, a 1% increase in public expenditure reducing infant mortality rate by four infants per 1,000 live births and private health expenditure reducing it by two infants per 1,000 live births and total health expenditure reducing it by three infants per 1,000 live births.
According to Makute and O’Hare (2015), public health expenditure has a statistically significant impact in improving health outcomes in sub-Saharan African countries and improvement in the quality of governance enhances the overall impact of public spending on health outcomes in countries with high quality of governance and vice versa. This evidence is in line with the results of Zahra et al. (2015), Rajkumar and Swaroop (2007), and Yaqub et al. (2012). This was discovered in their study which investigated the effect of public health spending and the quality of governance on health outcomes in sub-Saharan Africa. Under-5 mortality and life expectancy were used as proxy for health outcomes. Panel data of 43 countries in sub-Saharan Africa for the period 1996 to 2011 was used and two-stage least square (2SLS) estimation techniques were employed for the study. The results of this study show that the effectiveness of governance plays a key role in determining whether the increase in government health spending will bring about a better health outcome.
In a similar study, Cevik and Tasar (2013) found that the level of income per capita is not significant in reducing under-5 and infant mortality. Other factors like law and order, education level, and population were also found to be positively related to health outcomes significantly apart from public health spending. The results are robust to various specifications. Finally, Cevik and Tasar (2013) noted that increase in public health expenditure is more likely to be needed more in low- and middle-income countries where there is little amount of expenditure on public health. Other studies such as Okeke (2014), Peralta and Deluna (2014), and Zahra et al. (2015) have conducted some studies in this area but the findings are still inconclusive. Thus, there is need for further investigation to ascertain how government expenditure on health impacts on health outcomes in Nigeria. This is the objective of this study. This will enable the government and policy makers to be properly guided in their public expenditure policies especially in the area of health.
Method
Model Specification
The models are specified to achieve the objectives of the study, following the work of Akpan and Riman (2010), Orji et al. (2015), Gaspar et al. (2009), and the theoretical underpinnings comprising Grossman (1972).
According to Micheal Grossman’s model of health demand (1972), each individual is seen as both a producer and a consumer of health. Health in his model is treated as a stock which degrades over time in the absence of investment in health, so health is seen as a sort of “‘capital.” The model acknowledges that health is both a consumption good that yields direct satisfaction and utility (through reduction of sick days) and also an investment good which yields satisfaction to consumers indirectly through increased productivity, fewer sick days, and higher wages. Investment in health is costly as consumers must trade off time and resources devoted to health such as exercising at a local gym as against other goals.
In Grossman’s model, the optimal level of investment in health occurs where the marginal cost of health capital is equal to the marginal benefit, that is MC = MB. With the passage of time, health depreciates at some rate δ. The interest rate faced by the consumer is represented by r. Thus, the marginal cost of health care can be found by adding these variables: MChc = r + δ. Marginal benefit of health capital (MBhc) is the rate of return from the health capital. In this model, the optimal health stock can be influenced by factors like age, wages, nutrients, education, and so on; for instance, δ increases as age increases and thus reduces the stock of health. Health sock, on the other hand, increases with increase in education, nutrient, and wage. Thus, Grossman therefore introduces the idea of investing in human capital (health and education) to improve health outcomes in both the market and non market sectors of the economy. His model is based on human capital theory which states that increase in a person’s stock of knowledge or human capital raises productivity in the market economy. This implies that spending or investment in health and education in any economy leads to positive health outcome or improved health outcome which on the other hand contributes to higher gross national product (GNP). Health as a capital good can be represented with the equation below:

where H is the total stock of health, H(t-1) is the initial endowment of health, δ is rate of depreciation in health, and I is the rate of investment in health. The equation above shows that a person is born with an initial endowment of health stock which depreciates with the passage of time and increases with investment in health. The rate of health production will therefore depend on the efficiency of investment in health.
In view of the foregoing, the variables for the different models were chosen based on insights from the literature reviewed. To avoid simultaneity bias and possible over-parameterization we could not include all the variables used in the two models simultaneously.
To estimate how health outcomes are affected by expenditure on health, we follow Orji et al. (2015) and the work of Akpan and Riman (2010) and re-specify them as follows:

Equation 1 is a health production function where H represents the expected health output, Y is a vector of health care inputs, and X is a vector of exogenous variables.
Mathematically the model is stated thus:

Here, the U5 is the dependent variable, while GHEX, IMM, CO2, and ISF are the independent variables.
Where U5 = under-5 mortality per 1,000 live birth (proxy for health outcome). This is under-5 mortality ratio. This is the probability per 1,000 live births that a newborn baby will die before reaching age 5, if subject to age-specific mortality rates of the specified year. Peralta and Deluna (2014), Azinim et al. (2013) found that high public spending on health reduces under-5 and infant mortality.
GHEX = government health expenditure. This consists of recurrent and capital spending from government budget, external borrowings, grants and health insurance funds to the health sector. Government recurrent health expenditure was used to measure government health expenditure in this study.
IMM = immunization against measles (% of children between 12 and 25 months), CO2 = carbon dioxide emissions (it captures air pollution in the economy) and ISF = improved sanitization facility (percentage of the population with access). This is immunization against measles percentage of children between 12 and 25 months.
CO2 = carbon dioxide emissions. It is used to capture pollution in the economy. It is released into the atmosphere mostly by burning of carbon containing fuels and the decay of wood and other plant matters.
ISF = improved sanitation facilities (% of population with access). Zahra et al. (2015) and many other studies found that improved sanitization facilities also improves child and infant mortality in OPEC countries.
Equation 2 can be specified econometrically as

where εt = the error term (representing the unobserved variables), β0 is the intercept, β1, β2, β3, and β4 are parameters to be estimated, other variables remain as previously defined. The double log-transformation rule is applied to the Equation 3. The essence of applying the double log-transformation is that it provides estimated parameters that can be interpreted directly as elasticity, that is, the sensitivity or degree of responsiveness of under-5 mortality ratio to changes in the explanatory variables included in the model. Thus, taking the natural logarithm of both sides of Equation 3 and still assuming linearity among the variables gives

where all the variables remain as previously defined.
To estimate the impact of government health expenditure on life expectancy in Nigeria and following the steps for the model specification above, we specify the model as

where LEX = life expectancy (the average number of years that a newborn is expected to live if current mortality rates continue to apply), and PreHIV = prevalence of HIV in the economy.
Other variables remain as previously defined.
Equation 5 can be specified econometrically as

Taking the natural logarithm of both sides of Equation 7 and still assuming linearity among the variables gives

where all the variables are as previously defined; β0 is the intercept; βi’s are the slope coefficient, and εt is the error term.
Results and Discussion
Presentation of the Unit Root Test
The study used the augmented Dickey Fuller technique to test for unit root of the dependent, explanatory, and instrumental variables used in the model and the results are presented in Tables 3, 4, and 5. The decision Rule is: If /ADFcal/ > /ADFtab/ in absolute terms, Reject the null hypothesis and conclude that the variable is stationary otherwise the null hypothesis is accepted. The null hypothesis is stated below:
Unit Root Results for All Variables.

Source. Authors’ computation based on E-view output.
Note. ADF = Augmented Dickey Fuller; LEX = life expectancy; GHEX = government health expenditure; CO2 = carbon dioxide emissions; IMM = immunization against measles; ISF = improved sanitation facilities.
Regression Results for Health Expenditure Impact on Under-5 Mortality Rate.

Source. Authors’ computation based on e-views output.
Note. GHEX = government health expenditure; ISF = improved sanitation facilities; CO2 = carbon dioxide emissions; IMM = immunization against measles.
Regression Results for Health Expenditure Impact on Life Expectancy in Nigeria.

Source. Authors’ computation based on e-views output.
Note. GHEX = government health expenditure; CO2 = carbon dioxide emissions; ISF = improved sanitation facilities.
E-View 8 has an option that automatically selects the lag length based on Akaike, Schwarz, and other information criteria. This study used e-views automatic lag length.
Table 3 above shows that under-5 mortality rate is stationary at level while the other variables are not. These variables were differenced at first level to ensure stability. The fact that there exists unit root for some of the variables is a necessary condition for co-integration. Therefore, there is need to carry out co-integration test (which is the unit root test of the residuals of each regression). Co-integration is aimed at testing the long-run relationship of the variables, wherein if it is validated then it means there is a problem that needs to be corrected with the error correction model. From Table 3, the unit root test of the residual carried out on each regression indicates that there is no co-integration in any of the regression since the test indicates that the residuals are not stationary at level. This implies that the sufficient condition for an error correction model is not satisfied; therefore, we conclude that there exists no long-run relationship among the variables and run the regression simply.
Regression Results of Under-5 Mortality
Given the nature of time series data, the probability of violating the assumption of homoscedasticity and autocorrelation is always high. To be sure that the error terms are homoscedastic so as to obtain efficient and unbiased estimates of the parameters, the study therefore tests for heteroscedasticity and autocorrelation before proceeding with the regression. The Breusch Pegan-Godfrey test is adopted for heteroscedasticity and the Breusch-Godfrey (BG) test for autocorrelation.
The Breusch Pegan-Godfrey test of heteroscedasticity
The test follows chi-square distribution with (m − 1) degrees of freedom, where m is the number of regressors in the regression. The hypothesis is stated thus:
The Breusch-Godfrey (BG) test for autocorrelation
The Breusch-Godfrey test follows chi-square distribution with (p) degree of freedom. The statistics is given as (n-P)R2 ~ χ2(p)df, where n = number of observation, p = the order of autocorrelation, χ2(p)df = chi-square tabulated at P(order of autocorrelation) degree of freedom.
From the result obtained for model one (impact of public health expenditure on under-5 mortality rate in Nigeria) (n-2) × R21.785432 < χ2tab = 5.99147; therefore, we cannot reject the null hypothesis and we conclude that there is no serial correlation of any order at 5% level of significance. Having obtained that the assumptions of heteroscedasticity and autocorrelation are not violated, we proceeded to estimate the OLS models.
To achieve Objective 1 of this study, which is to estimate the impact of government health spending on under-5 mortality rates in Nigeria, we ran the regression as specified in “Method” section. The regression results are presented in Table 4.
From the regression result on Table 4, the overall significance of model one is good as the probability value of the F-statistics is very low (0.0000), and the R2 is equally very high (0.941763) suggesting that 94% variations in the dependent variable is being accounted for or is being explained by the variations in the explanatory variables. The value of the Durbin Watson is 1.543300, which falls in the zone of indecision. We can therefore not state categorically that there exist strong positive or negative autocorrelation. The fact that it does not fall on either of the extreme autocorrelated regions permits us to welcome the results. However, the test of autocorrelation conducted in “The Breusch-Godfrey (BG) test for autocorrelation” section indicates no autocorrelation of any order.
The first objective of this study is to ascertain the impact of government health expenditure on under-5 mortality rate in Nigeria. The results above show that there is a significant impact of government health spending on under-5 mortality rate in Nigeria given that the t-statistics is statistically significant at 5% level of significant and the probability value is .0030, which is less than the threshold 0.050 hence significant at 5% level of significance. This result collaborates with the results of Anyanwu and Erhijakpor (2007), Oluwatoyin et al. (2015), Okeke (2014), Arthur (2013), and so on. However, Filmer and Lant (1999), Azinim et al. (2013), and Kumar et al. (2013) found that there is insignificant association between public spending on health and under-5 mortality. The coefficient of government health spending is negative which implies that government health spending reduces under-5 mortality rates in Nigeria. Hence, a 1% increase in government health spending in Nigeria reduces under-5 mortality rate significantly by 0.273456%. This result conforms to a priori expectation that increase in public health spending is expected to improve public health infrastructure which provides the country with the capacity to prevent disease, promote health, and prepare for and respond to both acute (emergency) threat and chronic (ongoing) challenges to health in the economy. Increase in government health spending is also expected to improve public health facilities (like public hospitals, clinics, outpatient care centers and specialized care centers) and increase standards for health workers. All these improvements in health facilities as a result of increase in public health spending should translate to a reduction in under-5 mortality rate in Nigeria, all other things being equal.
Immunizations against measles have a negative relationship with under-5 mortality rate and thus conform to a priori expectation. This result shows that a 1% increase in vaccination coverage against measles in Nigeria will reduce under-5 mortality rate by 12.8142% or approximately 12.8%. This therefore suggests the importance of vaccinating children in the economy and hence reducing the risks of young children or infants dying due to carelessness or neglect. This result is in line with the findings of Zahra et al. (2015) who found immunization against measles to be a significant factor of health outcomes.
Carbon dioxide emissions has a positive relationship with under-5 mortality rate which conforms to a priori expectation. Carbon dioxide emission is expected to have a positive relationship with under-5 mortality rate. The result shows that a unit increase in CO2 emission increases under-5 mortality by 0.567429%. This is because increase in the release of carbon containing fuels, the decay of wood and other plant matters into the atmosphere by burning of carbon containing fuels, is expected to affect child health negatively, thus increasing the rate of under-5 mortality in the economy. However, its effect is statistically insignificant. This therefore means that carbon dioxide emissions significantly impact on under-5 mortality rate in Nigeria suggesting the importance of controlling pollutions in the economy to avoid its adverse effect on population health in the economy. Oluwatoyin et al. (2015) also found carbon dioxide emissions to be a significant factor of health outcomes.
On the other hand, improved sanitization facility has a negative relationship with under-5 mortality rate which also conforms to a priori expectation. The result shows that if increased sanitation facility is improved by one unit, it will lead to approximately 0.07% decrease in under-5 mortality. This aligns with the assumption that improvement or increase in the percentage of the population with access to improved sanitization facilities is expected to improve health outcomes by reducing under-5 mortality rate in the economy. Since improved sanitization facility impacts under-5 mortality rate in Nigeria, this suggests the importance of increasing the percentage of the population with access to improved sanitization facilities to improve health outcomes and thus reduce under-5 mortality in the economy. Zahra et al. (2015) also found some interesting results that partly align with this outcome.
Regression Results of Life Expectancy
To achieve Objective 2 of this study, which is to estimate the impact of government health spending on life expectancy in Nigeria, we ran the regression as specified in “Method” section. As in Objective 1, we tested to be sure that the assumption of homoscedasticity and autocorrelation is not violated.
The Breusch Pegan-Godfrey test of heteroscedasticity
From the result obtained for model two (impact of public health expenditure on life expectancy in Nigeria) n × R2= 5.877690 and χ2tab=9.48773. Therefore, we accept the null hypothesis that the error terms are homoscedastic at 5% level of significance.
The Breusch-Godfrey (BG) test for autocorrelation
From the result obtained for model one (impact of public health expenditure on life expectancy in Nigeria) (n-2) × R21.085002 < χ2tab=5.99147. Therefore, we cannot reject the null hypothesis and we conclude that there is no serial correlation of any other at 5% level of significance.
Therefore, having obtained that the assumptions of heteroscedasticity and homoscedasticity is not violated; we ran the regression as specified in “Method” section. The regression results are presented in Table 5.
From the regression result on Table 5, the overall significance of Model 1 is good as the probability value of the F-statistics is very low (0.0000), and the R2 is equally very high (0.918760) suggesting that 91% or approximately 92% variations in the dependent variable is being accounted for or is being explained by the variations in the explanatory variables. Also the value of the Durbin Watson is 1.708537 which still falls in the zone of indecision; we can therefore not state categorically that there exist strong positive or negative autocorrelation. The fact that it does not fall in either of the extreme autocorrelated regions permits us to accept the results. However, the Breusch-Godfrey test of autocorrelation conducted in “The Breusch Pegan-Godfrey test of heteroscedasticity” section indicates no autocorrelation of any order.
The second objective of this study is to ascertain the impact of government health expenditure on life expectancy in Nigeria. The results above show that there is a significant impact of government health spending on life expectancy in Nigeria given that the t-statistics is statistically significant at 5% level of significant and the probability value is 0.0027 which is less than the threshold 0.050 hence significant at 5% level of significance. The coefficient of government health spending is positive which implies that government health spending is positively related to life expectancy in Nigeria. Hence, a 1% increase in government health spending in Nigeria increases or improves life expectancy significantly by 0.01%. The result shows that the degree of responsiveness of life expectancy to government health expenditure in Nigeria is relatively low compared with that of under-5 mortality. This result conforms to a priori expectation since increase in public health spending is expected to improve public health infrastructure which provides the country with the capacity to prevent disease, promote health, and prepare for and respond to both acute (emergency) threat and chronic (ongoing) challenges to health in the economy. A developed public health infrastructure also guarantees a country of strong and healthy manpower for the production of goods and services. Public health infrastructure includes advanced machines specialist doctors, nurses, and other paramedical professionals, and developed pharmaceutical industry. Increase in government health spending is also expected to improve public health facilities (like public hospitals, clinics, outpatient care centers and specialized care centers) and increase standards for health workers. All these improvement to health as a result of increase in public health spending should translate to an improvement in life expectancy in Nigeria all other things being equal. This result is in consonance with the findings of Oluwatoyin et al. (2015), Arthur (2013), and Novignon et al. (2012) who found that public health expenditure statistically significant positive relationship with life expectancy in Nigeria. Makute and O’Hare (2015), Zahra et al (2015), Rajkumar and Swaroop (2007), and Yaqub et al. (2012) found that the quality and effectiveness of governance indicators is important to consider while planning public health spending, as it play a key role in determining whether the increase in government health spending will bring about a better health outcome.
Prevalence of HIV in the economy has a negative relationship with life expectancy in Nigeria and therefore conforms to a priori expectation. The coefficient of HIV prevalence is also statistically significant at 1% level since its probability value is (0.0086) which is less than the threshold 0.050. This implies that prevalence of HIV in the economy has a statistically significant impact on life expectancy in Nigeria. Hence 1% increase in HIV status reduces life expectancy by almost 0.04%. This therefore suggests that the government of Nigeria need to make effort to reduce the prevalence of HIV in the economy to save the lives of many people in the economy. This result is in line with the findings of Anyanwu and Erhijakpor (2007).
From the results, carbon dioxide emissions has a positive relationship with life expectancy which does not conform to a priori expectation and this can be attributed to the nature of carbon dioxide emissions data available. Carbon dioxide emission is expected to have a negative relationship with life expectancy. This is because increase in the release of carbon containing fuels, the decay of wood, and other plant matters into the atmosphere by burning of carbon containing fuels is expected to affect population health negatively. However, its effect is statistically insignificant since its probability value is 0.1248 which is greater than 0.05. This therefore means that carbon dioxide emissions insignificantly impacts on life expectancy in Nigeria. However, there is still need to control pollutions in the economy to avoid its adverse effect on population health in the economy. Oluwatoyin et al. (2015) also found carbon dioxide emissions to be a significant factor of health outcomes, though their findings conform to economic theory while this study does not.
On the other hand, improved sanitization facility has a positive relationship with life expectancy which also conforms to a priori expectation. Improved sanitization facility is expected to have a positive relationship with life expectancy. The result shows that one unit increase in improved sanitation facility will lead to 0.08% increase in life expectancy. This is because improvement or increase in the percentage of the population with access to improved sanitization facilities is expected to improve health outcomes by increasing life expectancy in the economy. However, its effect is statistically insignificant at 5% level since its probability value is 0.4722 which is more than 0.05. This therefore means that improved sanitization facility significantly impacts on life expectancy in Nigeria suggesting the importance of increasing the percentage of the population with access to improved sanitization facilities to improve health outcomes in the economy. Zahra et al. (2015) also found that improved sanitization facility is a significant determinant of life expectancy.
Conclusion and Recommendations
Conclusion
This research has provided reliable evidence on the impact of government health expenditure on health outcomes in Nigeria. The conclusion to be drawn from this study is that health outcomes (under-5 mortality rate and life expectancy) are responsive to public health expenditure. Government health expenditure has a statistically significant impact on health outcomes in Nigeria. This implies that increasing government health spending will help to improve public health infrastructure which provides the country with the capacity to prevent disease, promote health, and prepare for or respond to both acute (emergency) threat and chronic (ongoing) challenges to health in the economy. It will also help to improve public health facilities (like public hospitals, clinics, outpatient care centers and specialized care centers) and increase standards for health workers.
It is worthy to note that since the Abuja Declarations and Frameworks for Action on Roll Back Malaria was pledged in 2001 by members of the African Union during a conference in Abuja, Nigeria, only very few countries have made significant efforts to address the dire need of the health sector in the various African countries. During the Declaration, the member nations pledged to increase their health budget to at least 15% of the state’s annual budget, and requested Western donor countries to increase their support. There is a serious need for Nigeria and other African Governments to wake up and begin to implement this Declaration judiciously to enhance the performance of the health sector.
Future research agenda could be geared toward investigating why it has been difficult for African Governments to keep their commitment to the Declaration by increasing the yearly allocation made to the health up to 15%.
Policy Recommendations
Public health expenditure is found in this study to have a statistically significant impact on under-5 mortality rate and life expectancy in Nigeria. In light of the findings above, the following recommendations are considered necessary for the short-, medium-, and long-term implementations.
First, the Federal Government of Nigeria should increase the annual allocation to health sector to improve population health. This is because with this result, it is certain that increasing government health spending will help to improve public health infrastructure which provides the country with the capacity to prevent disease, promote health, and prepare for and respond to both acute (emergency) threat and chronic (ongoing) challenges to health in the economy.
Second, the government should partner with universities and other academic institutions to fund researches in the area of health. This will ensure that health policy making will be based on empirical evidence not just on guess works or stereotypes.
Third, there should be joint partnership between the government and the private sector in providing essential public health infrastructure and in making or implementing health policies as it will help to complement government effort toward improving health in the economy. Fourth, serious advocacy should be done by nongovernmental organizations, civil society groups, and other concerned citizens to encourage government to increase health sector funding. Fifth, the government should checkmate the system for channeling fund and distribution of health services to ensure that there is transparency in the system.
Finally, these recommendations if judiciously applied will lead to improvements that will enhance good population health. Again, it will help the country to come up in the world health system performance ranking. It will also translate to growth in productivity since being in good health is both a necessary and sufficient condition for work (a healthy workforce is a productive workforce). With adequate funding and proper monitoring, a resource-wealthy nation like Nigeria can become healthy. However, if this is not done, wealthy may not be healthy after all.
Footnotes
Acknowledgements
We acknowledge the research support of Aniorji U. B.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.