
Abstract
In the United States, African Americans continue to bear a disproportionate amount of risk from HIV and illicit drug use, highlighting the importance of culturally responsive prevention programming. Manualized HIV and substance use prevention curricula that are conceptually African centered are few, and evaluative data of such programs are sparse. This research brief aims to describe a field evaluation of the “Color it Real” (CIR) program, a 6-session, 12-hr HIV and substance use prevention curriculum for African American males and females aged 18 to 24 years. Participants (n = 225) were recruited using convenience sampling from two cities within a high-risk county in Indiana. Attitudes, knowledge, and confidence related to HIV and substance use were assessed before and after the intervention. Wilcoxon and McNemar tests were used to compare pretest and posttest scores, and binary logistic regression models were used to examine sociodemographic associations with outcomes. Among the analytic sample (n = 195), the CIR program was associated with several improved attitudes and increased knowledge related to HIV and substance use, but not with increased confidence in sexual negotiation skills. These findings represent the first published data from CIR since the developers’ original study, and support continued use of the curriculum by our program. Given the positive findings (i.e., attitudes and knowledge) and community receptiveness to CIR, we believe that a randomized, controlled trial of the intervention that includes longitudinal behavioral measurement would be a meaningful addition to prevention research.
Introduction
In 2017, African Americans comprised 43% of new U.S. HIV diagnoses (Centers for Disease Control and Prevention [CDC], 2018a) while only accounting for 12% of the total population. Separately, that same year, African Americans aged 12 years and older were more likely to have used an illicit drug in the past month than White non-Hispanics, Native Hawaiian/Pacific Islanders, Asians, and Hispanic/Latinos (CDC, 2018b). These data suggest that African Americans experience a disproportionate amount of risk from both HIV and substance use. Furthermore, substance use may introduce synergistic risk for HIV transmission and acquisition by altering judgment and sexual decision-making (Baliunas et al., 2010; Justice et al., 2010), and may also reduce prevalence of HIV risk reduction behaviors, as reported in recent research suggesting that use of HIV self-tests prior to sexual activity may be reduced when one or more participants is under the influence of alcohol or drugs (Dolezal et al., 2020).
Manualized prevention programs designed to influence behavior and behavioral precursors (e.g., social behaviors leading to HIV transmission; Cortopassi et al., 2019) can be effective risk reduction tools, especially when conducted among high-risk communities (CDC, 2006). However, though HIV prevention programs have been developed to provide culturally tailored content for African Americans (Raj et al., 2001), a recent review stated that few such programs are truly African centered, a best practice recommendation to meet African Americans’ needs effectively (Perry-Mitchell & Davis-Maye, 2017). “Color it Real” (CIR), a curriculum designed to reduce risks related to HIV and substance use among African American adults aged 18 to 24 years (Zellner et al., 2016), was one of the only four HIV prevention programs meeting every standard for African centeredness (e.g., “promoting culturally traditional means of nurturance and uplift”) in that review (Perry-Mitchell & Davis-Maye, 2017).
Theoretical and Conceptual Basis for CIR
CIR was originally developed by the Wholistic Stress Control Institute (WSCI) in Atlanta, GA, based on content from the Street Smart curriculum (Akintobi et al., 2016). The program activities were reconstructed using the Self-efficacy, Stages of Change, and Health Belief models (Zellner et al., 2016), with the primary goals of increasing prophylactic use and reducing substance misuse and other risky sexual behaviors (Akintobi et al., 2016; Zellner et al., 2016). Proposed mechanisms of action included, but were not limited to, the following:
Knowledge acquisition about HIV/AIDS to modify perceived susceptibility to harm and to personalize risk (Champion & Skinner, 2008), which may be especially important, given recent qualitative evidence that high perceived severity for HIV does not necessarily imply high perceived susceptibility to transmission (Mauer et al., 2019);
Candid discussion about risks posed by alcohol and marijuana use, both as their own mechanisms of action and due to their likely relationships not only with unprotected sex but also with perceived risk of unprotected sex (e.g., Dir et al., 2018);
Group discussion and role play to modify self-efficacy (Champion & Skinner, 2008) and normative beliefs (Fisher et al., 1995).
The developers also culturally tailored each activity using hip-hop (Walston, 2020), Ma’at principles, African American history, and urban cinema (Akintobi et al., 2016). These changes were made at a granular level throughout the curriculum—for example, rather than listening to standard New Age meditation music during a mindfulness exercise, participants listen to soft R&B music from their parents’ generation. The resultant benefit is that each individual aspect of CIR speaks to African American culture.
Although Street Smart, the underlying program, previously was recommended by the CDC’s Division of HIV/AIDS Prevention for use, it has been dropped from the Effective Interventions list in favor of Promise for HIP (CDC, 2019). Similarly, CIR was included in the now-discontinued National Registry of Evidence-based Programs and Practices (NREPP) by the Substance Abuse and Mental Health Services Administration (SAMHSA) but is not presently listed on the CDC’s Effective Interventions list. This is likely because the current published evidence, though promising, is based on a single quasi-experimental study as featured in Zellner et al. (2016) and Akintobi et al. (2016). These changes appear to have left a gap in available evidence-based programming for African Americans. While Promise for HIP is a rigorously designed program, it focuses primarily on the HIV care continuum, with far less emphasis on substance abuse than CIR (CDC, 2020). It also relies heavily on role models and peer advocates, which may be difficult to integrate into programs offered in communities that are just beginning to build their capacity. We have observed that CIR fills a gap among similar programs because of its unique combination of elements: it is African centric, addresses both HIV and substance use, is specifically designed for young adults, and is nongendered. This latter point is notable because heterosexual African American women and men are the fourth and fifth most HIV-affected subpopulations in the United States, respectively (CDC, 2018a).
When the authors received an HIV Capacity-Building Initiative grant in 2016, our community advisory board had located and identified CIR as a preferred program to be rolled out in the project’s catchment area, largely owing to the program’s unique characteristics as described above. At the same time, in our dual roles as public health researchers and individuals invested in the community, we wanted to verify that the purported benefits of the program were reflected in our own measurable evaluation outcomes. Furthermore, even though CIR remains available for purchase as an evidence-based program via the WSCI website, there are no available data on CIR outside of the original study by WSCI. As such, this study had two primary purposes. First, the evaluation itself was conducted to provide information to the community advisory board to assist in determining whether our program should continue using CIR within the community. Second, as members of the broader scientific community, we believed that it was important to publish these results. While not specifically a replication design, this is the only extant study outside of the original validation study to provide data on CIR and may serve as an important “reliability check” for the program (Martin & Clarke, 2017). CIR continues to be made available and sold to communities, and meets many funders’ standards for being evidence based by nature of having published quasi-experimental data showing efficacy, so in the absence of additional data, it is incumbent on us to add to the scholarly record about this program.
Method
CIR Intervention
This study used a one-group within-subjects evaluation design. Participants completed a pretest, attended up to six manualized, 2-hr lessons with local, community-based facilitators, and then completed a posttest at the end of the final lesson. Lessons were delivered sequentially using a program manual developed by WSCI; lesson content has been summarized by Akintobi et al. (2016) and included “(a) hip-hop and its influence on risky behavior, (b) relationships and decision-making, (c) learning the language of HIV, sexually transmitted infections (STIs), and substance abuse and cultural context, (d) HIV risk knowledge, (e) how to use condoms and HIV testing, and (f) recognizing and coping with feelings, and how to solve problems.” The originally published CIR program included a seventh lesson, which was a review and closing ceremony, but this was no longer included in the program by the time we had engaged with the developers, and was not utilized as part of our program. Each CIR program was completed across 28 or fewer days.
All CIR facilitators received a 15-hr “training-of-trainers” (TOT) with the CIR program developers. The 15-hr TOT was shorter than the 28-hr TOT originally provided by the developers (Akintobi et al., 2016) but is the current standard offering by WSCI, and displayed high training quality in our evaluation of content delivery (Agley et al., 2019).
Participants
Young adults (n = 225) between ages 18 and 24 years were recruited from two conterminous cities in Lake County, IN, which ranks in the top three of Indiana’s 92 counties for HIV, hepatitis C, and other STD incidence/prevalence (Indiana State Department of Health, 2019). The selected cities were predominantly African American or Hispanic/Latino, with higher poverty rates than the county or state. Recruitment methods used convenience sampling, including social media posts, flyers, tables at local events (e.g., concerts), and facilitator outreach.
All 225 young adults attended at least one session of CIR between October 1, 2016, and March 27, 2019, and completed the pretest evaluation. Data at pretest and posttest were matched using a random ID card provided to participants, which also served as their means of obtaining gift card incentives. A total of 30 participants failed to complete the posttest instrument and so were excluded from the primary analyses (see the “Steps to Manage Attrition Bias” subsection).
Instrument
SAMHSA’s 2016 National MAI Substance Abuse/HIV Prevention Initiative Adult Questionnaire (SAMHSA, 2019) was administered to measure the program outcomes. Questions not appropriate for this evaluation study or that would not logically be affected by the curriculum were not analyzed. The following categories of items were considered pertinent to this study (see Table 1 for full item descriptions).
Comparisons of Preintervention and Postintervention Scores for Attitudes, Confidence, and Knowledge.
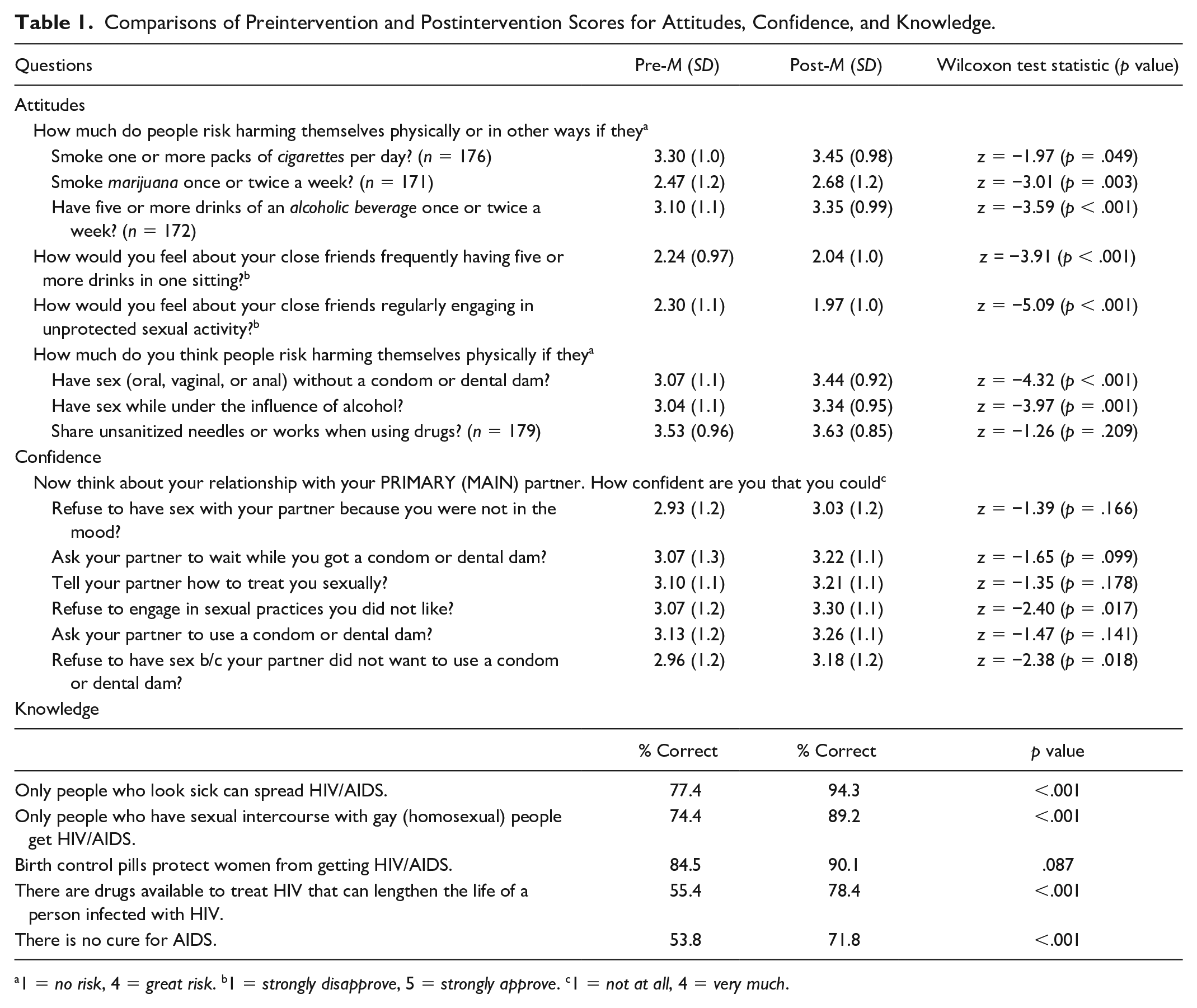
1 = no risk, 4 = great risk. b1 = strongly disapprove, 5 = strongly approve. c1 = not at all, 4 = very much.
Attitudes
Participants were asked six questions on perceived risks of harms from cigarettes, marijuana, alcohol, sex without condom or dental dam, sex while under the influence of alcohol, and sharing needles when using drugs (ranging from 1 = ‘no risk’ to 4 = ‘great risk’); the substance use questions also included the option to indicate that the risk level was ‘unknown’—those responses were not analyzed, but were not treated as missing data. Participants also responded to two questions on their feelings about friends binge drinking or engaging in unprotected sexual activity (ranging from 1 = ‘strongly disapprove’ to 5 = ‘strongly approve’).
Confidence
Participants responded to six items on confidence in sexual negotiation with their primary (main) partner using a 4-point scale (ranging from 1 = ‘not at all’ to 4 = ‘very much’).
Knowledge
Participants were asked five questions on their knowledge of HIV/AIDS. Responses were coded as 0 (“correct”) and 1 (‘incorrect or don’t know’).
Sociodemographic information
Participants reported their gender, year of birth, ethnicity, race, sexual orientation, education level, employment status, experience with detention/jail/prison, and armed forces/reserves/National Guard service.
Steps to Manage Attrition Bias
Attrition bias can occur in longitudinal data collection when individuals who provide data for all study points differ systematically from those who do not (e.g., Winefield et al., 1990). This evaluation contained pretest data from 30 individuals (13.3%) who did not complete a posttest survey. Anecdotally, reasons for incomplete posttests varied widely, ranging from absence at the final session (when posttests were conducted) to needing to leave prior to posttest administration for a competing engagement. However, prior to the primary study analyses, the authors assessed whether participants who completed the posttest differed systematically from those who did not. A binary attrition value (0 = posttest, 1 = no posttest) was assigned to each case, and nonparametric tests of association were conducted between that value and each outcome variable (five knowledge variables, 14 attitude/belief variables) and seven sociodemographic variables, some of which were dichotomized for this analysis (ethnicity, gender, sexual orientation, race, employment status, education level, and history of being in jail). After correcting alpha for multiple comparisons (Bonferroni adjustment; .05/26), there were no significant differences between cases with completed posttests and those without. However, two comparisons would have been significant with uncorrected alpha levels, so we share those data for transparency: approval of friends’ unprotected sex (z = −2.335, p = .020) and correctly identifying that HIV drugs prolong the life of HIV-infected persons (χ2 = 4.24, p = .035). On the basis of these findings, the evaluation employed a per-protocol analysis rather than an intent-to-treat approach; the 30 participants who did not complete a posttest survey were excluded.
Analytic Plan
Pairwise deletion was used to deal with individual instances of missing data (cell level) because missingness was infrequent, with five or fewer instances per variable, or approximately 2.6% missingness or less (e.g., Marshall et al., 2010).
Changes in outcomes
For the 19 variables of interest (attitudes, confidence, and knowledge), pairwise comparisons were used to assess differences between pretest and posttest data. Due to data non-normality, Wilcoxon tests were used for pairwise comparisons of the differences between matched preitem and postitem scores of Likert-type variables. For binary variables, McNemar tests were used for pairwise comparisons. Alpha was corrected to .0026 for the 19 comparisons in the study (Bonferroni correction).
Associations of sociodemographic variables with outcomes
To explore whether sociodemographic variables were associated with improvement in knowledge or attitudes, three binary logistic regression models were prepared using composite outcomes constructed with variables that significantly changed from pretest to posttest. The first had knowledge improvement as the dependent variable (0 = no improvement in knowledge; 1 = at least one question correct at posttest that was not at pretest), the second had increased perception of risk as the dependent variable (0 = no increases in perception of risk; 1 = increased perception of risk for at least one risky behavior), and the third had lowered approval of friends’ risky behavior as the dependent variable (0 = no decrease in approval of friends’ risky behaviors; 1 = decreased approval for at least one behavior). Because of small cell sizes, the independent variables were also dichotomized for these analyses: race (Black or African American/Other), ethnicity (Hispanic or Latino/Other), gender (male/female), sexual orientation (heterosexual/other), employment status (unemployed nonstudent/other), education level (high school or less/some college or more), and history of being in jail (never jailed more than 3 days/other).
The primary metrics of interest measured the overall explanatory power of the models. For each of the three models, this was estimated using (a) improvement (i.e., numeric reduction) in −2 log likelihood (−2LL) from the constant-only model to the full model that included all seven sociodemographic variables, (b) a significant chi-square test of significance for the full model, indicating that the sociodemographic variables, in sum, likely had an effect on the outcome variable, and (c) percentage improvement in cases that the model correctly classified, compared with the constant-only model. In cases where a variable within a model was significant, but the overall model was nonsignificant, researchers computed unadjusted odds ratios (UOR) for those variables at a modified alpha of .017 (.05/3).
All analyses were conducted in IBM SPSS Statistics 26. Ethical approval for the use of these evaluation data was provided by the Indiana University Institutional Review Board, protocol #1708270934.
Results
Of 195 participants, the majority was 18 or 19 years old (n = 99; 51%), male (n = 100; 51%), African American (n = 187; 96%), heterosexual (n = 175; 90%), and non-Hispanic (n = 163; 84%). Approximately 15% (n = 29) of the sample had ever been in prison, jail, or detention for more than 3 days, 88% had a high school education or less (n = 172), and 4% (n = 7) had ever served in the U.S. military forces. Around 17% (n = 33) of the sample was unemployed for a reason other than being a full-time student, and 6% (n = 12) had a college degree. Finally, 10% (n = 20) of the participants had attended fewer than six sessions.
Significant differences in attitudes and knowledge, but not confidence, were observed between pretest and posttest (see Table 1). In most cases, sociodemographic characteristics were not associated with changes in knowledge or attitudes.
Attitudes
At posttest, participants endorsed a greater perception of risks of harm from smoking marijuana once or twice a week (p = .003—though depending on significant digit rounding rules, this may have fallen on either side of adjusted significance), having five or more drinks of an alcoholic beverage once or twice a week (p < .001), having sex without a condom or dental dam (p < .001), and having sex under the influence of alcohol (p = .001), compared with pretest. In addition, participants expressed reduced approval of their close friends frequently having five or more drinks in one sitting (p < .001) or engaging in unprotected sexual activity (p < .001).
Knowledge
From pretest to posttest, there was a 16.9% increase in the percentage of participants who correctly identified as false the statement, “Only people who look sick can spread HIV/AIDS” (p < .001), and a 14.8% increase in the percentage of participants who correctly identified as false the statement, “Only people who have sexual intercourse with gay (homosexual) people get HIV/AIDS” (p < .001). We also observed a 23.0% increase in the percentage of participants who correctly identified as true the statement, “There are drugs available to treat HIV that can lengthen the life of a person infected with (HIV)” (p < .001), as well as a 18.0% increase in the percentage of participants who correctly identified as true the statement, “There is no cure for AIDS” (p < .001).
Sociodemographic Associations
Participants’ sociodemographic profile (race, ethnicity, gender, sexual orientation, history of having been jailed, and employment status) was not associated with general improvement in HIV/AIDS-related knowledge. The full model with seven independent variables did not significantly improve explanatory power over the constant-only null model (χ2 = 8.197, df = 7, p = .316); the improvement in −2LL was minimal (from 285.574 to 277.376), and correct classification of cases improved only 1.4%, with no variables significantly associated with the outcome.
Likewise, participants’ overall sociodemographic profile was not associated with increased perception of risk across six risky behaviors. The full model with seven independent variables did not significantly improve explanatory power over the constant-only null model (χ2 = 12.308, df = 7, p = .091); the improvement in −2LL was moderate (from 288.330 to 276.022), and correct classification of cases improved by 8.2%. However, the adjusted odds ratio for having ever been in jail more than 3 days was significant in this model. We therefore created a separate univariable model with only “history of being jailed” as an independent variable. This model did significantly improve classification of cases (χ2 = 8.578, df = 1, p = .003); the improvement in −2LL was moderate (from 255.491 to 246.913), and correct classification of cases improved 4.7%. The data suggested that never having been in jail for more than 3 days was associated with 3.34 greater unadjusted odds (p = .004, 95% confidence interval [CI] = [1.46, 7.67]) of reporting increased perception of risk for at least one risky behavior after attending the CIR program.
Finally, participants’ overall sociodemographics were not associated with lowered approval of friends’ risky behaviors. The complete model did not significantly improve explanatory power over the constant-only null model (χ2 = 10.858, df = 7, p = .145); the improvement in −2LL was minimal (from 262.903 to 252.045), and correct classification of cases actually decreased by 0.5%. While the adjusted odds ratio for sexual orientation was significant in this model, the CI was extremely wide (95% CI = [1.180, 25.136]) due to overspecification, as only two nonheterosexual individuals had lowered approval, so inference would not be appropriate.
Discussion
Participating in the CIR program was associated with improved attitudes related to alcohol, marijuana, and sexual risk, as well as improved knowledge, from pretest to posttest. At a surface level, these results were conceptually similar to findings from the original CIR validation study. Zellner et al. (2016) and Akintobi et al. (2016) measured knowledge of HIV transmission, condom use/intentions to use a condom, risky sexual behavior, and behavioral intentions about substance use, finding significant, positive differences for all scales but risky sexual behavior. Our evaluation focused on similar behaviors (substance use, condom use, and risky sexual behavior) but collected data for constructs that are hypothesized to mediate and moderate behavioral intentions, such as perceived norms and self-efficacy. Especially given the comparatively short duration of the CIR program (the revised CIR that we administered was shorter than the original version, as noted), we were not confident that measurement of behavioral change, especially recall over the period of the evaluation itself, would produce reliable data. Thus, although data from the original validation study and this field evaluation were not directly comparable, they produced affirmative, theoretically linked findings in most of the same behavioral domains.
Importantly, in our study, not all attitudes significantly improved. For example, the data did not indicate a significant pre/postdifference in perception of risk for sharing unsanitized needles or works when using drugs. This was somewhat surprising because the validation study found that CIR was associated with increased likelihood to use clean needles when injecting drugs (Zellner et al., 2016). At the same time, perception of risk at pretest was high for our program (3.55 of 4, where 4 represents “great risk”), so it is possible that a ceiling effect limited the ability to measure improvement. While not specific to our priority population, other literature has suggested that perceived HIV risk may be higher among individuals who are engaged in relationships where sex, drug use, and needle sharing co-occur than among individuals who engage in condomless sex alone (Koku & Felsher, 2020), and that interpersonal relationships and power dynamics play a meaningful role in how needles are used, and perceived risk thereof (Morris et al., 2019). Thus, it is not unreasonable that individuals’ perception of risk of using unsanitized needles would be high in a given sample, regardless of behavioral intentions related to needle sharing and reuse.
In addition, we observed an association between having spent more than 3 days in jail prior to the CIR program and reduced likelihood of reporting improvements in attitudes toward risky substance use or sexual behaviors. While we cannot know from these data why that might have been the case, prior research has suggested that behaviors such as substance abuse can function as stress management outlets for individuals who have exited the correctional system (Phillips, 2010), and that exposure to violence may be related to HIV risk behaviors (Richardson & Robillard, 2013). Although not the primary focus of this study, further investigation into the degree to which programs like CIR can produce attitudinal or intentional change in individuals exposed to jail or prison may be informative.
This study also identified significant and substantial (>20%) improvements in objective knowledge on four of the five questions. No significant improvement was found for the percentage of participants who correctly answered “Birth control pills protect women from getting HIV/AIDS” (7.6% increase), but the pretest percentage of correct answers for that item was 83.7%, again raising concerns about a ceiling effect.
Finally, no significant associations between confidence in sexual negotiation and CIR program participation were observed. Issues such as condom negotiation and sexual communication are complex and extend beyond communication skills (Peasant et al., 2014). Furthermore, confidence in these behaviors may be suppressed by abusive relationships or intimate partner violence (Bogart et al., 2005). Hence, the degree to which a 12-hr program not exclusively focused on this topic could affect these variables is unclear.
Limitations
This study had several limitations. First, this was a practical field evaluation and did not employ a control group, so there is limited ability to infer causality. At the same time, attitudes about substance use and sexual risk, and objective (e.g., true/false) knowledge about HIV/AIDS are unlikely to change due to secular trends, especially within a short timeframe. Thus, limited outcome attribution to exposure to the program may be reasonable. Second, generalizability was limited to individuals who were recruited via convenience sampling within a defined catchment area (permissible age range: 18–24 years). While in some ways heterogeneous, the sample was overwhelmingly African American (the priority population for CIR) and predominantly heterosexual. Furthermore, this area is known both within the state and the country as being at particularly high socioeconomic need, so the degree to which results might be replicated in more resource-rich environments cannot be inferred. At the same time, measured improvements did not appear to be associated with most sociodemographic variables (with the exception of having spent more than 3 days in jail). Third, some outcome measures were self-reported attitudes, and others were objective knowledge assessment. Knowledge and attitudes generally are acknowledged as contributing to health behaviors, but the degree and mechanisms of the influence of CIR on actual health behaviors are unknown (Kruglanski et al., 2015). Fourth, this analysis did not employ an intent-to-treat approach, but subanalyses indicated that participants excluded due to noncompletion of the posttest did not differ across observed variables from those who did, reducing concerns about mortality threat. Fifth, the short time period between pretest and posttest may have contributed to testing threat, but this is more commonly observed with factual information than with attitudes or perceptions (Onwuegbuzie, 2000), so if present, such a threat would more likely have applied to knowledge variables only. Finally, this evaluation did not control for potential social desirability bias for nonobjective measures.
Implications for Practice and Research
Following development, CIR underwent a quasi-experimental study by WSCI and their colleagues. Based on that study, it was included in the NREPP evidence-based practice system and made available to other communities of practice. The program has evolved since the original published study (e.g., change in TOT length from 28 to 15 hr, and from seven to six sessions).
This article contains the first published evaluation of a CIR program outside of the developers’ initial study. Findings support the association between CIR and improved attitudinal and knowledge outcomes for African American young adults, and thereby the continued use of the curriculum in our catchment area. At the same time, attitudes and intentions are not behaviors, and no study has examined CIR using a highly rigorous experimental design. Based on our positive evaluation and community receptiveness to the program, we believe that a randomized, controlled trial of the CIR intervention that includes longitudinal behavioral measurement would be a meaningful addition to prevention research.
Footnotes
Data Availability
Data used in this article can be accessed by contacting the corresponding author via e-mail.
Statement of Ethical Approval
This study was approved by the Indiana University Institutional Review Board (IRB#1709270934A002).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Funding for the training-of-trainers events with the program developer, Wholistic Stress Institute, Inc. (WSI), was provided as part of the federal Substance Abuse and Mental Health Services Administration (SAMHSA) grant, but none of the authors is affiliated with that organization, financially or otherwise. WSI neither reviewed nor had any input into any portion of this study or article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was conducted as part of the Knowledge for Life program, which is supported by the Substance Abuse and Mental Health Services Administration (SAMHSA) via SP021706. This study does not represent the official views of SAMHSA, nor does SAMHSA formally endorse the content.