
Abstract
All diseases and injuries exert a heavy epidemiological and socioeconomic burden on Kenya. The specific objectives of this study were (a) to estimate the monetary value of disability-adjusted life years (DALYs) from all causes in 2017 with the ongoing implementation of United Nations sustainable development goal (SDG) 3 and (b) to estimate the reductions in the monetary value of DALYs in Kenya, assuming diseases and injuries related to SDG3 targets are achieved by 2030. A variant of human capital (or net output) analytical framework was applied to value DALYs from 162 diseases and injuries into their monetary equivalents. The 17.9 million DALYs from 162 causes in Kenya in 2017 had a total monetary value of Int$ 67,012,790,388. Approximately 57% of the monetary value of DALYs emanated from communicable, maternal, neonatal, and nutritional diseases; 36% from noncommunicable diseases; and 7% from injuries. We estimate that attainment of the five SDG3 targets would lead to an Int$ 21.5 billion (45%) decrease in the SDG3-related monetary value of DALYs by 2030. There is an urgent need for health policy-makers to use this kind of evidence when advocating among public and private sectors for increased spending on health development.
Keywords
Introduction
Kenya is one of the six partner states of the East African Community (EAC) regional intergovernmental organization (EAC, 2019). It has a population of 49.4 million people, that is, 27.6% of the EAC population (International Monetary Fund [IMF], 2019). The country had a total gross domestic product (GDP) of International Dollars (Int$) 192.3 billion and a GDP per capita of Int$3,896.
In 2017, Kenya had a total of 17,856,955 disability-adjusted life years (DALY) from all causes (Global Burden of Disease Collaborative Network, 2018). Out of which, 57% resulted from communicable, maternal, neonatal, and nutritional diseases (CMNND); 36% from noncommunicable diseases (NCDs); and 7% from injuries. Figure 1 portrays the DALYs from all causes by 23 age groups.

The disability-adjusted life years (DALYs) from all causes by age groups in Kenya in 2017.
The substantial loss of DALYs in Kenya could be due to two systemic weaknesses. First, the inefficiently performing national health system. Kenya’s health system consists of a total of 6,655 health facilities, which includes 3,384 (50.8%) owned by the government and 3,271 (49.2%) by the private sector (World Health Organization [WHO], 2017b). The country has a health workforce density of 2.0 medical doctors per 10,000 population, and 15.4 nursing and midwifery personnel per 10,000 population. Kenya’s health workforce densities are lower than the global health workforce density of 15.1 medical doctors per 10,000 population; and 34.8 nursing and midwifery personnel per 10,000 population (WHO, 2019b).
Masters et al. (2014) facility survey of pharmaceutical availability across levels of care in Kenya found 18% of essential medicines were out of stock in referral hospitals, 26% in district hospitals, 29% in subdistrict hospitals, 33% in health centers, and 39% in dispensaries.
In 2016, per capita total current health expenditure (CHE) on health in Kenya was US$ 66 (WHO, 2019a). Approximately US$ 24 per capita was from domestic general government health expenditure; US$ 29.4 per capita from domestic private health expenditure; and US$ 12.9 per capita from external health expenditure. Kenya CHE was below the range of US$ 76 (minimum) and US$ 342 (maximum) per person per year of health systems investment recommended for attaining health sustainable development goal (SDG) 3 (Stenberg et al., 2017).
Second, there is a challenge of suboptimal population coverage of systems that provide services for addressing social determinants of health, for example, education, food and nutrition, housing, water, sanitation, and physical security. Due to inadequate nutrition, the prevalence of stunting and wasting in children under 5 years old was 26.2% and 4.2%, respectively (WHO, 2019b). About 21.3% of adults (ages 15 and older) are illiterate (United Nations Development Programme [UNDP], 2018). About 5.3% of households live in slums (Republic of Kenya, 2013). About 41.5% of the population uses water unprotected from outside contamination, and 70% do not use improved sanitation facilities (UNDP, 2018). In the perceptions of individual well-being survey, 54% of women and 64% of men indicated they felt safe; the homicide rate is 4.9 per 100,000 people (UNDP, 2018).
As a result of under-investment in the national health system, Kenya’s universal health coverage (UHC) index was 57%, implying essential health services (reproductive, maternal, newborn and child health; infectious diseases; NCDs) coverage gap of 43% (WHO, 2019b). This gap calls for unrelenting evidence-based advocacy within the Kenyan government, the private sector, and the external development partners to increase investments into the national health system and the other systems that address social determinants of health.
Some economically developed (Lee et al., 2019; Schofield et al., 2019; Scholten et al., 2014; Tachkov et al., 2017) and developing countries (Kirigia et al., 2017; Kirigia & Mwabu, 2018a) used monetary value of DALY evidence to make a case for increased investment into the health system and health programs interventions. To date, no study in Kenya has attempted to estimate the total monetary value of DALYs from all causes and among all the age groups.
The specific objectives of this study were as follows:
(a) to estimate the monetary value of DALYs from all causes in 2017 with the ongoing implementation of the United Nations [UN] SDG3 on health (UN, 2015);
(b) to appraise the monetary value of DALYs from SDG3-related diseases and injuries targets in 2030;
(c) to calculate the reductions in the monetary value of DALYs in Kenya, assuming diseases and injuries related to SDG3 targets are achieved by 2030.
Methods
Study Site and Disease Categories
The analysis focussed on DALY estimates for all (162) diseases in Kenya in 2017 (Global Burden of Disease Collaborative Network, 2018). These diseases included 39 CMNND; 106 NCDs, which consisted of 30 neoplasms (cancers), 11 cardiovascular diseases, 5 (five) chronic respiratory diseases, 10 digestive diseases, 7 (seven) neurological disorders, 10 mental disorders, 2 (two) substance abuse, 3 (three) diabetes and kidney diseases, 12 skin and subcutaneous diseases, 3 (three) sense organ diseases, 6 (six) musculoskeletal disorders, 7 (seven) other NCDs; and 17 injuries. Figure 2 shows the DALYs in Kenya by disease categories.

The disability-adjusted life years (DALYs) in Kenya by disease categories in 2017.
Murray (1994) defines the DALY as “. . . an indicator of the time lived with a disability and the time lost due to premature mortality” (p. 441). We used DALY estimates for Kenya from the Global Burden of Disease (GBD) 2017 study (Global Burden of Disease Collaborative Network, 2018).
As the ministry of finance policy-makers and the majority of private sector Chief Executive Officers are not public health specialists, they have a challenge understanding public health indices such as the DALY. The dearth of understanding of such an index puts the health sector policy-makers at a disadvantage when advocating for sustaining (or increasing) resource allocations to health as opposed to the so-called “economically productive” sectors (World Health Organization Regional Office for Africa [WHO/AFRO], 2006). Therefore, this study attempts to convert the DALYs into their monetary equivalents to enable health sector policy-makers to use the language that those who control public and private sector budgets understand.
SDG3 Disease-Related Targets
Table 1 contains the disease-related SDG3 targets and expected percentage reductions for Kenya, assuming these targets are attained by the end of 2030. These percentages were used in estimating the monetary value of DALYs losses that would be averted following the implementation of interventions that would lead to the achievement of SDG3 targets 3.1, 3.2, 3.3, 3.4, and 3.6.
Health SDG3 Targets and Expected Percentage Reductions for Kenya.
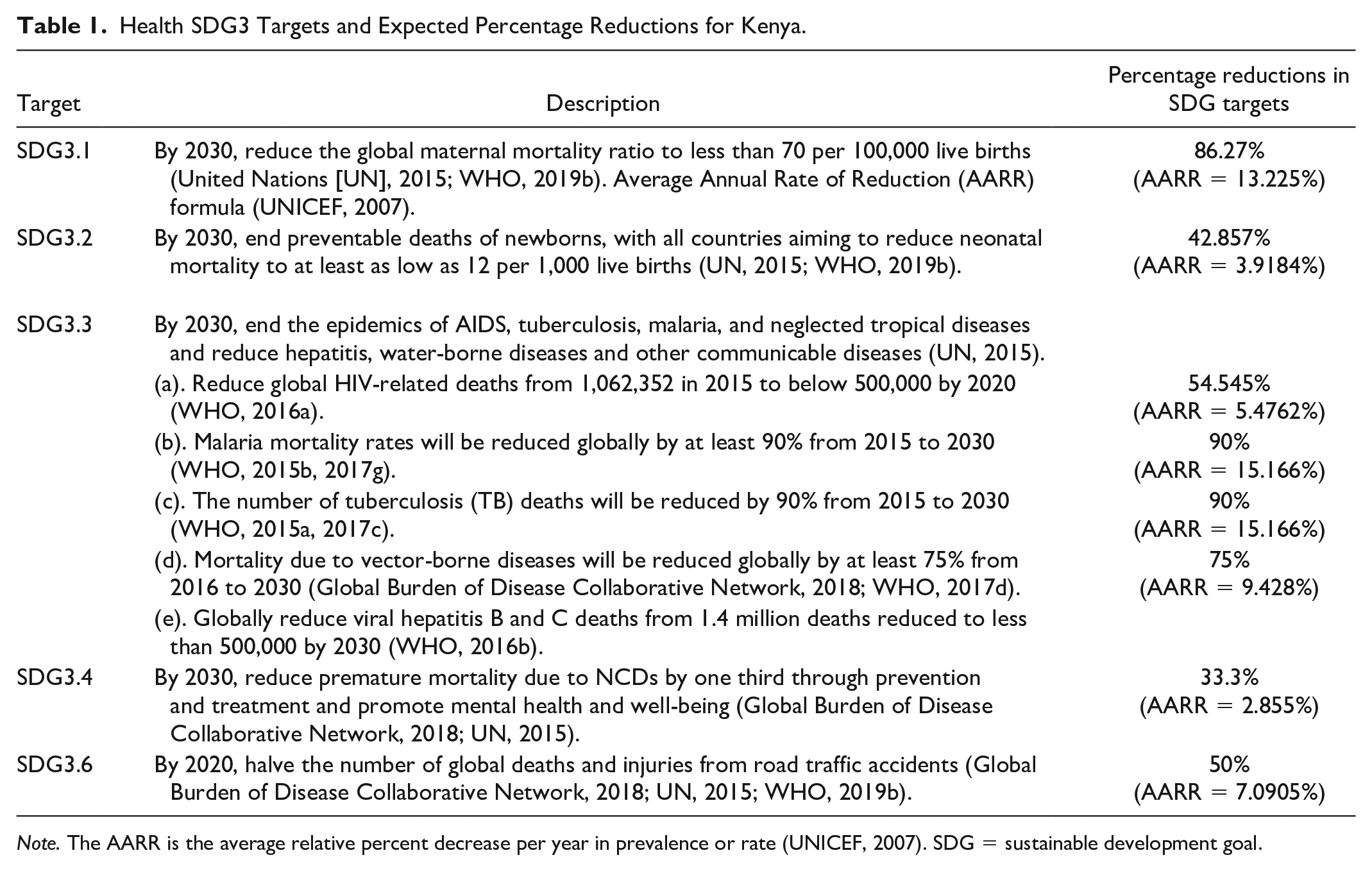
Note. The AARR is the average relative percent decrease per year in prevalence or rate (UNICEF, 2007). SDG = sustainable development goal.
Human Capital Approach/Net Output Analytical Framework
The Organisation for Economic Co-operation and Development (OECD, 2001, p. 18) defines human capital as “The knowledge, skills, competencies, and attributes (including physical, emotional and mental health) embodied in individuals that facilitate the creation of personal, social and economic well-being.” Premature mortality and nonfatal disability from any disease or injury erodes the health stock of Kenyans, and hence, their human capital.
More than 300 years ago, Sir William Petty pioneered the application of the human capital approach (HCA) in valuing human lives (Petty, 1699). Since then, Fein (1958), Mushkin and Collings (1959), Weisbrod (1971), Landefeld and Seskin (1982), Chisholm et al. (2010), and WHO (2009) further refined the theoretical underpinning of the HCA.
We adapted the variant of human capital (or net output) analytical framework developed and applied in the monetary valuation of DALYs among 15- to 59-year olds (Kirigia & Mwabu, 2018a) and the elderly (Kirigia et al., 2017) in Kenya in 2015. Subsequently, the framework was employed to value the DALYs in 2015 within the Arab Maghreb Union (Muthuri et al., 2018), the Central African Economic and Monetary Community (Kirigia et al., 2019), and the EAC (Kirigia & Mwabu, 2018b). A similar framework was applied in estimating the aggregated productivity cost of DALYs in Africa in 2015 (WHO/AFRO, 2019c).
We choose to use the HCA to monetarily value DALYs due to the availability of data on per capita GDP, CHE per capita, and DALYs on all the countries in the African continent (Kirigia & Mwabu, 2018a; WHO/AFRO, 2019c).
Estimation of the Monetary Value of DALYs From All Causes in 2017
Kenya’s total monetary value of DALYs (TMVDALY2017) from 162 diseases and injuries in 2017 was obtained through a summation of the monetary value of DALY from each ith disease or injury (MVDALYi). This was expressed as follows:

where
Estimation of the Monetary Value of DALYs From SDG3-Related Health Conditions Diseases in 2030
Kenya’s monetary values of DALYs in 2030 were estimated assuming the SDG targets for maternal mortality ratio (MMR; Target 3.1); neonatal mortality (Target 3.2); HIV/AIDS, tuberculosis, malaria, neglected tropical diseases (NTDs) and viral hepatitis deaths (target 3.3); NCD mortality (target 3.4); and injury mortality (target 3.6) would be realized. We used Equation 2 to estimate the expected reduction in monetary values of DALYs from each jth SDG3-related health condition (HC):

where MVDALYHCj2030 is the monetary value of DALYs in Kenya from jth health condition in 2030; MVDALYHCj2017 is the monetary value of DALYs in Kenya from jth health condition in 2017; and HCjTARGET is the jth health condition DALYs in 2030 if health condition target is achieved in Kenya. We have assumed that the implied percentage reductions in DALYs would be similar to mortality reductions because the SDG3 disease-related targets are couched in terms of mortality reductions (Kirigia & Mwabu, 2018b).
We illustrate below how the monetary value of DALYs from maternal disorders (MDs) in 2030

Estimation of Monetary Value of DALY Losses Averted by 2030
There are two ways for estimating potential reductions (savings) in the monetary value of DALYs following the full attainment of each of the five SDG3 targets. First, the saving in the monetary value of DALYs from jth health condition

For example, the potential reduction/savings in the monetary value of DALYs from MDs
Data Sources and Software
The DALYs data estimates for the 162 causes for Kenya were from the GBD 2017 study (Global Burden of Disease Collaborative Network, 2018); data on GDP per capita (Int$3,896) from the IMF world economic outlook database (IMF, 2019); and data on the CHE of per person (Int$144) from the WHO Global Health Expenditure Database (WHO, 2019a). The NHGPCInt$ = Int$3,896 − Int$144 = Int$3,752. The analysis of the five equations developed in the preceding subsection was conducted using Excel Software belonging to Microsoft (New York).
Results
Estimates of the Monetary Value of DALYs in Kenya in 2017
All diseases
Kenya had a total of 17,856,955 DALYs among people of all ages in 2017 (Global Burden of Disease Collaborative Network, 2018). Those DALYs had a total monetary value of Int$ 67,012,790,388; and an average value of Int$ 3,753 per DALY. Approximately, 56.6% emanated from communicable, maternal, neonatal, and nutritional diseases; 35.94% from NCDs; and 7.42% from injuries.
Figure 3 displays the monetary value of DALYs from all causes by age groups. The people aged 14 years and below bore DALYs valued at Int$ 25,964,877,620 (38.7%); the 15 to 59 years olds bore DALYs valued at Int$ 32,888,431,641 (49.1%); and those aged above 59 years incurred DALYs valued Int$ 8,159,481,127 (12.2%).

The monetary value of disability-adjusted life years (DALYs) from all causes by age groups in Kenya (Int$ 2019).
Communicable, maternal, neonatal, and nutritional diseases
Figure 4 depicts the monetary value of DALYs related to some CMNND categories. Out of the total monetary value of DALYs from CMNND of Int$37,952,637,789, 28.6% resulted from HIV/AIDS and sexually transmitted infections; 19.8% from maternal and neonatal infections; 19.0% from respiratory infections and tuberculosis; 15.5% from enteric infections; 8.2% from other infectious diseases; 4.9% from nutritional disorders; and 4.1% from NTDs and malaria. Supplemental Additional File 1 presents the monetary values of DALYs associated with individual CMNND health conditions. Five health conditions (HIV/AIDS, neonatal disorders, diarrhoeal diseases, lower respiratory infections, and tuberculosis) alone accounted for 76% of the total monetary value of DALYs from CMNND.

The monetary value of disability-adjusted life years (DALYs) from communicable, maternal, neonatal, and nutritional diseases in Kenya (2019 Int$).
NCDs
Figure 5 shows the monetary values of DALYs from key categories of NCDs. Of the total of DALYs from NCDs valued at Int$ 24,084,582,837, 14.8% were attributed to cardiovascular diseases; 11.0% to digestive diseases; 10.8% to neoplasms (cancers); 10.2% to mental disorders; 8.1% to neurological disorders; 7.3% to diabetes and kidney diseases; 6.9% to musculoskeletal disorders; 5.0% to chronic respiratory diseases; 4.7% to skin and subcutaneous diseases; 4.2% to sense organ diseases; 2.2% to substance use disorders; and 14.8% to other NCDs. Supplemental Additional File 2 contains a breakdown of the monetary value of DALYs from individual NCDs. Congenital birth defects, stroke, ischaemic heart disease, cirrhosis and other chronic liver diseases, and diabetes mellitus account for 31% of the monetary value of DALYs from NCDs.

The monetary value of disability-adjusted life years (DALYs) from noncommunicable diseases in Kenya (Int$ 2019).
Injuries
All forms of injuries resulted in DALYs valued at Int$ 4,975,569,762 (see Figure 6). Out of the total monetary value of DALYs from injuries, unintentional injuries accounted for Int$2.08 billion (42%), self-harm and interpersonal violence for Int$1.6 billion (32%), and transport injuries for Int$1.3 billion (26%). Seventy percent of the monetary value of DALYs from injuries was attributed to road injuries (23%), interpersonal violence (19%), falls (12%), self-harm (10%), and exposure to mechanical forces (6%).

The monetary value of disability-adjusted life years (DALYs) from injuries in Kenya (Int$ 2019).
Monetary Value of DALYs in 2017 From Five SDG3-Related Targets
In 2017 SDG-related health conditions and diseases were associated with 12,627,303 DALY, which had a monetary value of Int$ 47,387,208,551 (70.7%). As indicated in Table 2, NCDs, HIV/AIDS, and neonatal disorders accounted for 86.83% of the monetary value of SDG-related DALYs.
Monetary Value of DALYs in 2017 From Five SDG3-Related Targets (2019 Int$).

Note. DALY = disability-adjusted life years; SDG = sustainable development goal; PPP = purchasing power parity.
DALYs data from IHME database (Global Burden of Disease Collaborative Network, 2018). bMonetary value of DALYs (Int$ or PPP). cPercent are authors estimates.
Estimates of Reductions in Monetary Value of DALY Losses in Kenya if the Five SDG3-Related Targets Are Achieved by 2030
Table 3 presents the monetary value of DALYs in 2017, the monetary value of DALYs in 2030, and envisaged monetary reductions by SDG health conditions.
Monetary Value of DALYs by SDG Health Conditions.
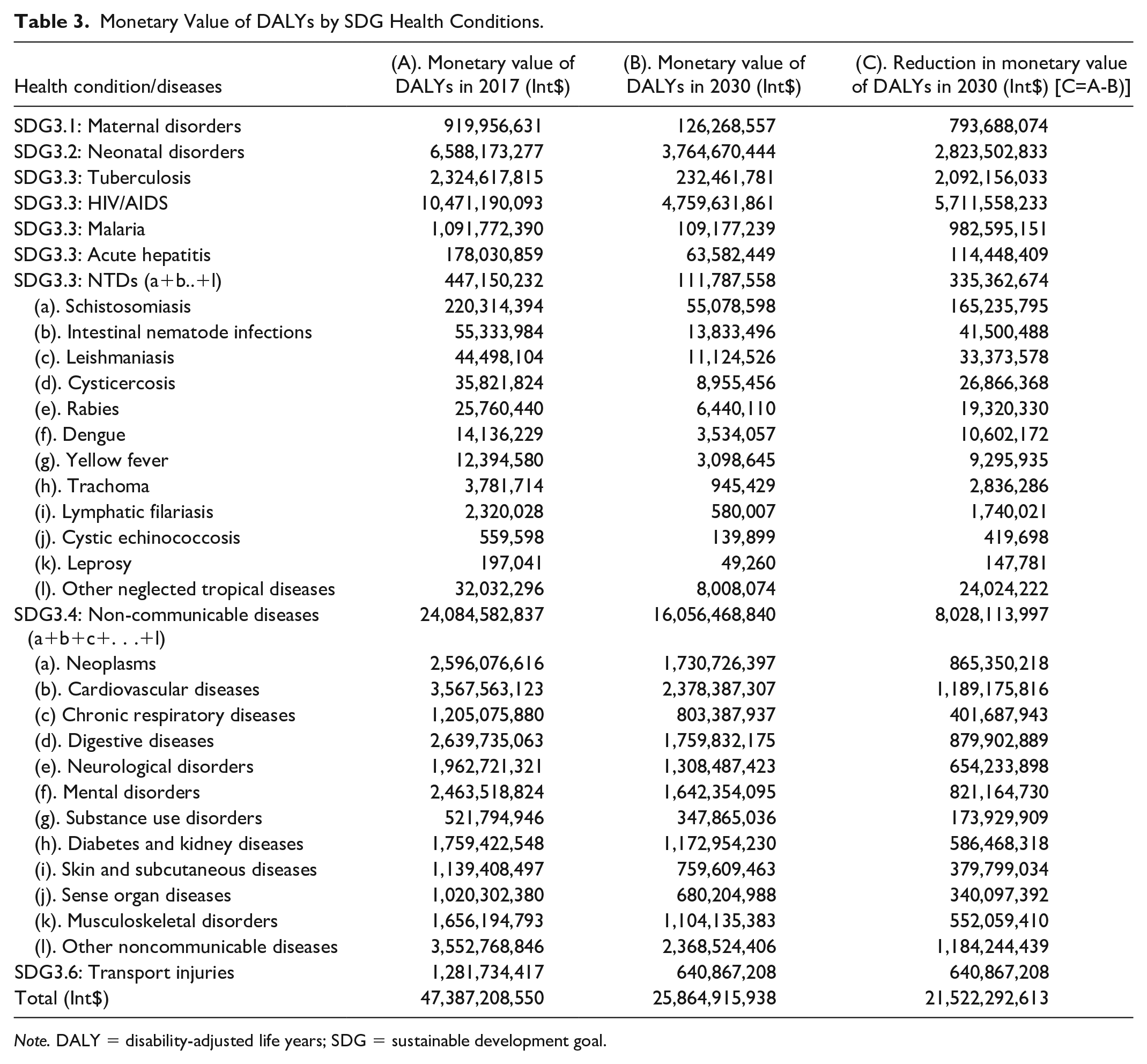
Note. DALY = disability-adjusted life years; SDG = sustainable development goal.
We estimate that the full attainment of the five SDG3 targets would lead to a 45.42% decrease in the monetary value of DALYs by 2030.
Discussion
Key Findings
The 17,856,955 DALYs among people of all ages in 2017 had a total monetary value of Int$ 67,012,790,388. Of these, 56.6% was attributed to CMNND, 35.94% to NCD, and 7.4% to injuries. The 15- to 59-year olds incurred close to half of the monetary value of DALYs. We estimate that the attainment of the five SDG3 targets would lead to an Int$ 21.5 billion (45.4%) decrease in the monetary value of DALYs by 2030.
SDG3.1 and SDG3.2: Maternal and Neonatal Disorders
Were Kenya to attain the SDG targets 3.1 and 3.2 by 2030, the country would annually prevent loss of DALYs with a monetary value of Int$ 793,688,074. That kind of saving might be achieved if both the national road map for accelerating the attainment of the millennium development goals (MDGs) related to maternal and newborn health (Republic of Kenya, 2010c); and the reproductive, maternal, newborn, child, and adolescent health (RMNCAH) investment framework (Republic of Kenya, 2016b) is fully implemented in all the 47 Administrative Counties. The global strategy for women’s, children’s, and adolescents’ health (2016–2030) (Every Woman Every Child, 2015); the United Nations General Assembly (UNGA) Resolutions on the girl child (UN, 2017a) and the right to food (UN, 2017c); and the World Health Assembly (WHA) Resolution on immunization (WHO, 2017f) underpinning the implementation of the national roadmap and framework to end preventable maternal and neonatal deaths.
SDG3.3: Tuberculosis, HIV/AIDS, Malaria, Acute hepatitis, and NTDs
The realization of SDG target 3.3 by 2030 would annually save Kenya DALYs with a monetary value of Int$ 2,092,156,033 from TB, Int$ 5,711,558,233 from HIV/AIDS, Int$982,595,151 from malaria, Int$ 114,448,409 from acute hepatitis, and Int$335,362,674 from NTDs. In other words, the country stands to save DALYs worth Int$7.144 billion.
The saving could be made through full implementation of Kenya’s AIDS strategic framework 2014/2015 to 2018/2019 (Republic of Kenya, 2014a); the HIV and AIDS research agenda 2014/15 to 2018/19 (Republic of Kenya, 2014b); the national strategic plan for tuberculosis, leprosy, and lung health 2019 to 2023 (Republic of Kenya, 2018f); the HIV and AIDS/STI and TB multisectoral strategic plan and implementation framework 2015 to 2020 (EAC, 2015); the malaria strategy 2019 to 2023 (Republic of Kenya, 2018a); the malaria communication strategy 2016-21 (Ministry of Health, 2016); the guidelines for the treatment of chronic hepatitis B and C viral infections (Ministry of Health, 2014a); the national strategic plan for control of NTDs 2016 to 2020 (Republic of Kenya, 2015a); and the national health promotion strategy (Ministry of Health, 2012).
A pertinent legal framework, including the Health Act (Republic of Kenya, 2017a), the Public Health Act (Republic of Kenya, 2012g), the HIV and AIDS prevention and control Act (Republic of Kenya, 2012d), the sexual offenses Act (Republic of Kenya, 2012h), and the malaria prevention Act (Republic of Kenya, 2012f) buttresses the implementation of communicable diseases strategies and plans.
At the global level, the UNGA declared political commitments for the fight against HIV/AIDS (UN, 2016b), malaria (UN, 2018a), TB (UN, 2018c), and NTDs (UN, 2017b; WHO, 2017e), which provide high-level political backing for the implementation of pertinent national policies, strategies, and plans.
SDG3.4: NCDs
If Kenya reduces the epidemiological burden from NCDs by one-third by 2030 (SDG3 target 3.4), it will save DALYs worth Int$ 8,028,113,997. The saving is achievable through full implementation of the national health policies, strategic plans, and guidelines. For instance, the Kenya national health policy 2014 to 2030 (the Republic of Kenya, 2014b); the Kenya health sector strategic and investment plan (KHSSIP) (Republic of Kenya, 2014c); the national strategy for the prevention and control of NCD 2015 to 2020 (Republic of Kenya, 2015b); the national nutrition action plan 2012 to 2017 (Republic of Kenya, 2012e); the mental health policy 2015 to 2030 (Republic of Kenya, 2016a); the national cancer control strategy 2017 to 2022 (Republic of Kenya, 2017b); the cancer screening guidelines (Republic of Kenya, 2018b); the guidelines for cardiovascular diseases management (Republic of Kenya, 2018c); the national diabetes strategy 2010 to 2015 (Republic of Kenya, 2010b); and the physical activity action plan (Republic of Kenya, 2018e) plus the guidelines for healthy diets and physical activity (Republic of Kenya, 2017c).
The WHA resolutions on physical activity (WHO, 2018c); infant and child feeding (WHO, 2018a); rheumatic fever and rheumatic heart disease (WHO, 2018b); cancer prevention and control (WHO, 2017a); global strategy for the prevention and control of NCD (WHO, 2000); and action plan for the prevention and control of NCDs (WHO, 2013) informed the development of Kenyan policies and strategic documents.
Various national legal instruments, such as the Kenya Constitution (Republic of Kenya, 2010a), the cancer prevention and control Act (Republic of Kenya, 2012c), the tobacco control Act (Republic of Kenya, 2012i), and the alcoholic drinks control Act (Republic of Kenya, 2012a) undergird the implementation of NCD prevention and control strategies and plans.
At the global level, in 2018 and 2012, the UNGA committed to providing strategic leadership through whole-of-government and health-in-all-policies approaches for scale-up of the prevention and control of NCDs (UN, 2012, 2018d).
SDG3.6: Transport Injuries
In case Kenya succeeded in reducing by half the epidemiological burden from road accidents, it would reduce DALYs with a monetary value of Int$640,867,208. The country developed the policy on integrated national transport (Republic of Kenya, 2009), the strategy and action plan for road safety (Republic of Kenya, 2015c), and the violence and injury prevention and control action plan 2018 to 2022 (Republic of Kenya, 2018d) to stem the tide of deaths and injuries associated with transport injuries. The national strategy on road safety consists of the following five components (Republic of Kenya, 2015c):
Road safety management: Including road safety coordination and management, mainstreaming, funding, data systems, research, and monitoring and evaluation.
Safer road and mobility: Encompassing development and maintenance of safer roads, and the safeguarding of vulnerable road users.
Safer vehicles: Includes vehicle safety standards, compliance, and public transport regulations.
Safer road users: Incorporating driver training, testing and licensing; road safety legislations and regulations; traffic law enforcement; road safety awareness/public education; and road safety, children, and education.
Postcrash care: Involving availability and accessibility to emergency services and rehabilitation.
Kenya’s national transport and safety authority, Act No. 33 of 2012, provides the legal framework for implementation of the aforementioned national policy, strategies, and plans (Republic of Kenya, 2014d).
Kenya’s road safety policy framework is underpinned by the UNGA resolution A/RES/64/255 that proclaimed the period 2011 to 2020 as the Decade of Action for Road Safety (UN, 2010). The UNGA resolutions A/RES/72/271 (UN, 2018b) and A/RES/70/260 (UN, 2016a) both entitled “improving global road safety” provide further political support for sustained implementation of strategies for curbing transport-related deaths and nonfatal injuries of people.
Limitations of the Study
The study reported in this article has some limitations. First, in Kenya, civil registration of births and deaths is a national Government function based in the Ministry of Interior and Coordination of National Government. The process hinges on a community-based system of civil registration, where assistant chiefs (local government administrators) record in register books births and deaths occurring at home. In contrast, health workers record those occurring at a health facility (Republic of Kenya, 2012b). In some cases, due to ignorance of the Government’s requirement, parents might not report births and deaths that occur at home. Furthermore, even when parents (or next of kin) report deaths occurring at home, the cause of death might be wrong because often there are no inquiries as to cause of death.
For these reasons, the mortality statistics upon which years of life lost (YLL) calculations are based might not be accurate. The completeness of cause of death data in the WHO African region was about 6% between 2009 and 2017 due to weak civil registration systems in countries (WHO, 2019b). The GBD 2017 Mortality Collaborators (2018) and GBD 2017 Cause of Death Collaborators (2018) discuss limitations related to the accuracy of the mortality and causes of death data used the GBD 2017 study. The GBD 2017 Disease and Injury Incidence and Prevalence Collaborators (2018) expounds on the shortcomings of the national data used in estimating years living with a disability (YLD) for various diseases and injuries. Therefore, as explained clearly by the GBD 2017 DALYs and HALE Collaborators (2018), DALY estimates are influenced by the availability and quality of data for YLL and YLD.
Second, unlike the willingness-to-pay/willingness-to-accept approach proffered by some economists, the HCA does not take into account the strength of individual preferences to either avert or accept the risk of incurring a DALY loss (Jones-Lee, 1985; Mishan, 1971). Furthermore, if strictly applied, HCA would value DALY losses occurring among anyone below the minimum work age and past retirement age at zero (Jones-Lee, 1985).
Third, GDP as a measure of the well-being of societies has weaknesses, such as ignoring economic, social, political and ecological inequalities and their ramifications (Stiglitz et al., 2010); does not capture the quality of life, happiness, and well-being; disregards negative environmental consequences of economic production processes (Giannetti et al., 2015; Ivkovic, 2016); omitting nonmarketed services, for example, the contribution of homemakers, including child care, cooking, cleaning, washing, fetching water, hewing firewood, cultivating, inculcating societal values, caring for the elderly, and nursing the sick at home (Card & Mooney, 1977).
Finally, since the SDG3 disease-related targets are framed in terms of mortality reductions, we have assumed that the implied reductions in DALYs would be similar. Of course, the reductions in mortality may not result in equal reductions in DALYs. For example, some of the medical interventions for chronic diseases (e.g., NCDs) may improve health-related quality of life, but may not prolong the life expectancy of persons living with those conditions. Therefore, the use of SDG3 disease-related targets may have led to an overestimation of the expected DALY reductions, and hence, expected monetary savings.
Conclusions
In 2017, the DALYs in Kenya had a monetary value equivalent to 34.8% of the national 2019 GDP. Full attainment of the disease and injuries related to SDG3 targets would lead to a 45.4% decrease in the monetary value of DALYs by 2030. There exists national health-related legislation, policies, strategies, and plans which, if fully funded and implemented, would enable Kenya to strengthen its health system and health programs, and consequently, assure UHC of essential health services related to SDG3 targets.
Therefore, there is an urgent need for health policy-makers to use the kind of evidence reported in this article to advocate among public and private sectors for increased spending on health development to the levels recommended by Stenberg et al. (2017).
Supplemental Material
Additional_File_1 – Supplemental material for The Monetary Value of Disability-Adjusted Life Years in Kenya in 2017
Supplemental material, Additional_File_1 for The Monetary Value of Disability-Adjusted Life Years in Kenya in 2017 by Rose Nabi Deborah Karimi Muthuri and Joses Muthuri Kirigia in SAGE Open
Supplemental Material
Additional_File_2 – Supplemental material for The Monetary Value of Disability-Adjusted Life Years in Kenya in 2017
Supplemental material, Additional_File_2 for The Monetary Value of Disability-Adjusted Life Years in Kenya in 2017 by Rose Nabi Deborah Karimi Muthuri and Joses Muthuri Kirigia in SAGE Open
Footnotes
Acknowledgements
R.N.D.K.M. is very grateful for the support and encouragement of her PhD thesis supervisors (Dr Flavia Senkubuge and Professor Charles Hongoro) at the School of Health Systems and Public Health, University of Pretoria, Pretoria, South Africa. The authors owe profound gratitude to Jehovah Jireh for meeting all their needs in the entire process of the study reported in this paper. The views expressed in this paper are exclusively those of the authors and not for the institutions of affiliation.
Author Contributions
R.N.D.K.M. and J.M.K. designed the study; reviewed pertinent literature; collated data from IHME, IMF and WHO databases; analyzed data, and wrote the paper. Both authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
This study did not involve the use of animal or human data or products. The analysis was based solely on secondary statistical data published in the international databases. Therefore, ethical approval and consent to participate did not apply to the study reported in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Availability of Data and Materials
The secondary data analyzed during this study is publicly available from the following websites:
DALY data from IHME database (Global Burden of Disease Collaborative Network, 2018): http://ghdx.healthdata.org/gbd-results-tool GDP data from IMF database (IMF, 2019): https://www.imf.org/external/pubs/ft/weo/2018/02/weodata/index.aspx Per capita current health expenditure data from WHO Database (WHO, 2019a): http://apps.who.int/nha/database/ViewData/Indicators/en
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.