
Abstract
We draw on Bourdieu’s and Goffman’s theories to elaborate the novel idea of dependency as status in old age, a concept that emerged from our Grounded Theory study conducted with 46 older adults (26 women and 20 men) living in and around Dublin, Ireland. The research participants’ portrayals of (in)dependence and assistance reflected their access to and use of social and symbolic (age) capital. Older adults derived social capital from supportive family relations or trusting relationships with formal care providers, and deployed such capital to signal their status as “cared for” individuals. Age capital—constructions of deservingness drawing on advanced age, age-related disabilities, and lifelong contributions—was used by older adults to frame and justify acceptance of help. We argue that where older adults are able to draw on age capital or social capital, they can signal their position as “cared for” individuals who display and acknowledge their dependency, and transform it into a marker of status. Conversely, some participants were keen to present themselves as independent. These participants made downward comparisons with others whom they saw as “worse off” or, in their view, as insufficiently responsible for their own health and well-being. In the contemporary Western frame, dependency is to be avoided at all costs, but we argue that some older people are able to embrace dependency in a way that reflects and demonstrates their status and agency. Care professionals and members of informal networks can make a significant difference to older persons’ acceptance of help, care, and support by offering services in a manner that affirms the care recipients’ worth and agency.
Keywords
Introduction
Understandings of dependence and independence vary between different cultural contexts, disciplinary traditions, and welfare states (Baltes, 1996; Fraser & Gordon, 1994; Plath, 2009). Even within the Western context where independence tends to be framed as highly desirable, definitions of independence vary and its distinction from autonomy is blurred (Ball et al., 2004). In medical and nursing contexts, dependency is generally understood as an outcome of a temporary or chronic functional disability where an individual is unable to perform a task that they could previously perform alone. In this definition, dependence refers to an objective status that can be instrumentally assessed as an individual attribute (Ball et al., 2004; Ory et al., 1998). Dependence can also be understood as socially induced and constructed, whereby its origins and mechanism lie in social structures and how these are maintained and interpreted by various actors (Baltes, 1996; Barken, 2019; Fine & Glendinning, 2005; Fraser & Gordon, 1994; Held, 2005; Lynch, 2009).
Policy documents and care professionals in the Western context tend to emphasize the importance of independence which is construed as the opposite of dependence (Plath, 2009), but we know that older adults’ perceptions of independence and dependence are more complex and often not binary (Gignac et al., 2000; Hammarström & Torres, 2010). Research on or with older adults in long-term care has focused on institutional settings such as nursing homes and generally highlights the tendency of institutional care to exacerbate, rather than alleviate, the problems of dependency (Ball et al., 2004). Empirical research has examined how older adults living in the community define and relate to the concept of dependency when receiving care services. Research conducted with older persons in Sweden indicated that their reactions to the prospect and realities of receiving home care ranged from “resistance, denial, indifference and self-degradation to reluctantly accepting the situation” (Janlöv et al., 2005, p. 334). Research conducted with home support service users in Australia revealed predominantly individualist understandings of independence that cantered on doing things alone, making one’s own decisions, and having resources, capacities, social standing, and self-esteem (Plath, 2008). Hammarström and Torres (2010) developed a categorisation of older adults in receipt of home care services in the community, based on the extent to which they could reconcile receipt of care, agency, and self-determination. One group reported negative feelings, such as a difficulty tolerating or accepting their condition, perceptions of helplessness, and appraisals that they were not managing or coping well. However, most people in their sample were able to reconcile dependence on care services and a sense of independence. In other words, older adults can make a clear distinction between receiving help and feeling dependent, as well as between being a home care recipient and having agency; these are not necessarily contradictory and some older people can combine them successfully.
Government policy for older people in Ireland is to support them living in their own homes for as long as possible (Timonen & Doyle, 2008). Long-term care services in Ireland are provided by the Health Service Executive (2018) Social Care Division, which funds residential placements in nursing homes and home support services; the latter are frequently referred to as Home Help and Home Care Packages. In this article, we focus on community-dwelling older adults who are receiving some amount of care in their home and/or belong to groups that offer psychosocial supports and activities (such as day centers and peer-support groups). We introduce a concept that, to our knowledge, has not been examined in the literature to date. This novel concept of dependency as status emerged from a Grounded Theory study we conducted in and around Dublin, Ireland, in 2018. While the concept of dependency as status therefore emerged from and is grounded in our data, we draw on Pierre Bourdieu’s and Erving Goffman’s concepts and theory to illuminate it. In Grounded Theory (Conlon et al., 2020; Timonen et al., 2018), this is referred to as retroduction—application of existing concepts, knowledge, and theoretical frames to shed light on emergent findings and concepts. We did not set out to conduct the empirical research with the view to interrogating Bourdieu’s and Goffman’s concepts, let alone to verify them. Rather, we turned to Bourdieu’s ideas of different forms of capital, and to Goffman’s ideas about presentation of self in everyday life, at the data analysis stage, where we found that they chimed with our emergent concept of dependency as status, and helped in elaborating it.
Bourdieu’s concepts of power and capital have been employed in elucidating the significance of social differentiation in active aging (Dumas & Laberge, 2005). Such an approach is in line with Bourdieu’s broader efforts to reveal the extent to which cultural practices embody power relations. Bourdieu’s (1986, 1992) definition of social capital comprises networks of relationships, including both formal and familial ones, which the participants in this research frequently referred to when outlining their experiences of care. Symbolic capital refers to different markers of social status that can be deployed to denote social hierarchies (Bourdieu, 1986). We illustrate how older adults make use of what we call age capital, that is, a form of symbolic capital rooted in advanced age and a history of contributions to society. Conceptualizing dependency primarily as a social construct, we adopt a symbolic interactionist perspective to examine how older adults deploy their dependency, under certain circumstances, as a positive status and conversely, how others hold up their independence as a source of pride and status.
We also drew on Goffman’s (1956) conceptualization of identity construction in the study of human interaction. In his analyses of interpersonal interaction and how individuals “perform” in order to project a desirable image, Goffman uses the theater to illustrate individuals’ contrasting front stage and backstage behavior. When in front stage, an actor is conscious of being observed by an audience and will perform to those watching by observing certain rules and social conventions to project the image/persona they wish to create. The research method we used—focus groups—is particularly well-suited to examining such front-stage performances as focus groups bring together people who have something in common, and hence provide a platform for signaling social positions and statuses to members of a peer group. To apply Goffman’s (1971) terminology, a focus group is an encounter that involves focused interaction and impression management among participants. Because our research encompassed only front-stage “performances” (people talking in focus groups), it is not possible for us to establish whether the participants’ front-stage personas differ from their back-stage presentation. Participants’ views and conceptualization of dependency might be different backstage where no performance (or a different performance) is necessary. Goffman’s (1963) concept of stigma as a relationship of devaluation and disqualification from full social acceptance is also useful for making sense of the ways in which some older adults hold up their status as “independent” in contrast to the stigmatized status of “dependent” care recipients.
Research Method
Our examination of perceptions of dependency and independence among older adults living in the community was situated within a collaborative European research project, and the data we collected and analyzed are derived from the Irish context. Purposive sampling was initially utilized to identify and recruit participants who corresponded to key stakeholder groups, including older adults using or potentially using formal home care services, policy planners, and a range of elder home care service providers (social workers, community nurses, care workers, and their managers). In line with the Grounded Theory method (Conlon et al., 2020; Timonen et al., 2018), theoretical sampling was subsequently engaged to saturate key concepts that were emerging from the data, around the issue of access to care and care provision as that was the focus of the project.
The Ireland-based team recruited 104 participants who took part in 21 focus groups. This sample included 46 older adults living independently, 26 women and 20 men, aged between 50 and 99 years.
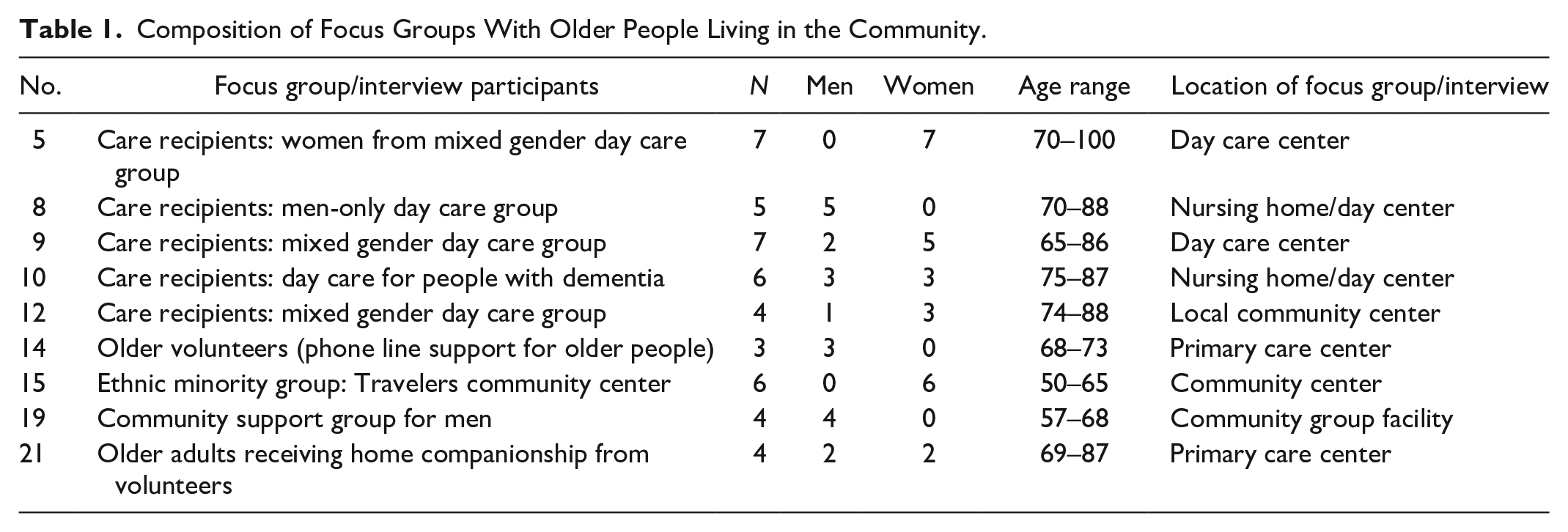
The analysis presented in this article focuses on the older adults’ focus groups only (Table 1) because the purpose here is to investigate older adults’ perceptions and experiences of care. The six older participants in their 50s were from the Traveler minority ethnic group, which has much lower life expectancy than the population of Ireland in general; fertility rates are higher and transition to grandparenthood happens at a younger age among Travelers than in the general population (Central Statistics Office, 2016). Both in demographic terms and socio-culturally, it is therefore appropriate to regard Travelers in their 50s as members of the older population in Ireland. Older people were recruited with the help of project colleagues who first approached gatekeepers at day care centers, social club meetings, and support groups for older adults in Dublin and the surrounding area. The older participants were from diverse socioeconomic backgrounds, and accessed services that were either free or heavily subsidized (we did not sample for individuals using privately paid-for services). Some had extensive social networks; others spoke of feelings of loneliness. Nonetheless, the findings should be understood in the context of those older people who are accessing at least some services and organized activities, and therefore are not experiencing extreme social isolation. Focus groups number 14 and 19 (see Table 1) comprised older adults who were not in receipt of any care or support services, but they could comment on care-related issues as they helped and/or interacted regularly with others in receipt of or seeking care.
Composition of Focus Groups With Older People Living in the Community.
In the focus group discussions, we used a lightly structured interview guide to attain an informal and conversational tone that would encourage everyone to participate. The guide comprised core questions on participants’ experience with formal care services and also associated questions in terms of their satisfaction with and expectations of these services. Because the researchers used a flexible guide as well as prompting and probing, participants were able to bring to the fore their own needs, experiences, and views of seeking and receiving care. One of the research team members would act as a moderator and actively encouraged research participants to take part in the conversation by making eye contact and calling participants by name (all of us wore name tags). There was always an additional member of the research team in the room during a focus group. This person was responsible for audio-recording the session and taking detailed field notes. The duration of focus groups ranged from 60 to 90 min. The number of participants in each group varied between three and seven. The groups were homogeneous, that is, the group members had several characteristics in common (such as old age; attending a particular center or group; living in the area proximate to the where the focus group discussion took place). In almost all cases, the group members had at least superficial knowledge of each other prior to the research event, which might have affected how participants presented themselves to others and sought to portray themselves as “independent” or “well cared for.” The focus group method, especially where group members are known to each other, is aligned with our symbolic interactionist perspective: the participants were able to signal their status not only to us (researchers) but also to other older persons, their peers.
We were aware of the potential for exercise of power in both organizing and conducting the focus groups. The power imbalances between older adults and gatekeepers (such as day center managers) were taken into account in various ways. For instance, we sought and managed to ensure that the focus groups consisted of “naturally occurring” groups such as the weekly meeting of a seniors’ group; this was a strategy for combating “hand-picking” by gatekeepers which might have happened had we asked them to help us to arrange the focus groups entirely separately from the normal structure of the seniors’ groups. The managers and other service providers were not present during the focus groups with the exception of a facilitator in the Travelers’ group, which was deemed important for her role as a trusted party between the researchers and the Travelers.
In presenting ourselves to the groups, we made use of symbols such as serving hot drinks and bringing small gifts of baked goods and, on the occasion of visiting the Traveler group, flowers to convey our gratitude and privilege in being allowed into the group (something that was also emphasized multiple times verbally at the start and end of each research event). When the fieldwork was concluded, the research team produced a small booklet with the help of an adult literacy consultant, using large print and illustrative images, to summarize our findings. A hard copy of this booklet was addressed to each research participant by way of thanking them for their involvement.
All recorded focus groups and observational field notes were professionally transcribed and coded with the aim of identifying patterns, key issues, and concepts. When we examined the data from the sub-sample of 46 older adults, we detected distinctive talk around understandings of independence and dependence, and how these were presented to the group. We embarked on the analysis of the transcripts from the 21 focus groups that these 46 older adults had participated in. The first stage involved line-by-line (open) coding of all transcripts from these focus groups. At this stage, we identified accounts of care as either a positive experience, or as an undesirable occurrence. At the second stage of data analysis, we employed focused coding to consolidate the emergent concepts of “positive” dependence and “desirable” independence. At the final, theoretical coding stage, we engaged Bourdieu’s and Goffman’s concepts that helped us to draw out the core category of dependence as status and its reverse, independence as status. In this article, we focus on presenting and discussing the novel concept of dependence as status, while independence as status provided the foil to dependence as status, the idea of independence as a valued status is not novel and for this reason we pay less attention to it in the exposition that follows. It is worth noting that while it was these striking and vocal “opposites” that caught our attention in the data, this should not detract or disguise the fact that most older adults are “somewhere in between.” We acknowledge that dependency/independence is not a rigid binary. Indeed, an older person might transition slowly, over a period of time, from rejecting any help to welcoming it. However, as our study was not longitudinal, we were not able to tap into such processes over time. Similarly, an older person might feel quite ambivalent about their (in)dependence—we cannot comment on this conclusively here, rather we propose it as a fruitful and exciting agenda for future research.
The main limitation of our research (within the qualitative, micro-sociological framing and methods that we employed) arises from the fact that our sample consists of community-dwelling older adults who were able to mobilize with or without assistive devices. The sample does not contain any older adults who are unable to leave their homes, nor does it contain any living in formal care institutions such as nursing homes. The study sampled only for people who were able to give informed consent, which involved discussing the nature and purpose of the study, and signing the consent form, activities that are not possible for individuals with severe cognitive impairment. Focus Group number 10 was organized in a setting that offers day care for people with early to moderate dementia and additional time was spent here explaining the nature of the study and obtaining informed consent. In other words, when we refer to older adults with care needs, we mean people who have a relatively low level of such needs in terms of physical and cognitive functioning in everyday life. Another limitation pertains to the fact that it is extremely hard to combat or to know the degree of social desirability bias (tendency to agree and to give favorable reviews) in groups that are convened in their naturalistic settings, where such settings are inseparable from the services the participants receive. We took measures to combat this bias by reassuring participants of confidentiality and lack of any connection between the research and the services they were receiving, but it is possible that some of the views expressed still reflect a measure of social desirability bias. Finally, with the exception of the Traveler ethnic minority participants, our sample consists of White Irish research participants, and as such our data cannot inform how other ethnicities or immigrant status might influence experiences of dependency.
Findings
Deploying Social Capital
We invited the older research participants to comment on their experiences with formal home and community care services, but the role of families and other informal supports did feature prominently in their accounts, as can be seen below. This is understandable as informal carers (unpaid family and friends) in Ireland provide the bulk of the care that enables people to live at home (Houses of the Oireachtas, 2018). Older people portrayed dependency in positive terms where a supportive and affirming person was attributing the dependency to them (e.g., if a daughter offered to wash the floors during a visit to her parents’ house). Usually such attribution was implicit and subtle, rather than overt. Descriptions of dependency were positively framed when older adults could refer to a warm figure personally known to them—such as a day center manager—who supported them in receiving and accepting care. The disposition of both people known to them and strangers in approaching them as objects of concern was also meaningful for older adults who held up examples of such concern as signals of respect that reflected their status. Where dependency was attributed by others in a respectful and caring way, it could be openly displayed and construed as a sign of status and worth.
Certain actors in the formal care system emerged as people who could bestow the dependent status on an older person in a compassionate and affirming manner. Due to the fact that this offer to help came from someone in a position of authority, it was perceived as a sign of respect toward them rather than an attribution of weakness. Among these people, we identified the recurrence of “the boss,” “the advocate,” and “the quasi-family” figures. Older adults signaled deference to the senior managers among the care professionals who helped them, and referred to them as “the boss” or the “person in charge.” In our sample, “the boss” was typically a day center or care agency manager. The participants accepted, acknowledged, and even praised the interventions of “the boss” because in many cases, these had enabled them to “get somewhere,” to feel less lonely, meet new people, and to do things that interested them: It’s great like, I’m meeting loads [of people] and they bring you different places and all. You get somewhere, [name of the manager] is great, the boss here. She brings us out everywhere that she can. (Madeline, day centre attendee; emphasis added)
The older adults felt in control when they could deploy their social capital by ringing the “boss” if they had a complaint with formal care. The situation of dependency or someone looking after them could be seen as a sign of status if they had direct access to “the boss”: [name of the manager], the girls [carers] that I have, their boss [. . .] every six months they’re reviewed, their boss reviews and asks you like what way you feel about things. But as I said to [name of the manager], so far so good I’m happy with the carers I have. [. . .] I haven’t had any reason to complain, so far. But if I did [. . .] I’ve only to ring the office [name of the manager] said. (Beatrice, day centre attendee; emphasis added)
Older adults who had recourse to “the boss” portrayed themselves as empowered. They claimed that they decide how things are done in their own home and stressed that they can change the care arrangement if they are not happy by getting in touch with “the boss.” In those cases where formal care services had failed and there was no attempt by care services management to consult them about their experiences, older adults relied on their social capital in the form of a family member to advocate on their behalf. “I told my daughter” and “I’d tell my daughter if I had a problem,” were common responses when we asked participants about their actual or putative actions in reaction to disappointing care services. Tom was not happy with his carer and asked his daughter to intervene, with the result that “my daughter . . . told the district nurse and—goodbye.” Betty explained that she was not happy with her carer being always late and asked her daughter to intervene: . . . my daughter walked in one morning and . . . I was still sitting there with my coat on. And she wasn’t even up, the girl [the carer] wasn’t even up. And my daughter rang in and complained about it. [. . .] “I want someone else coming to my mother” she said “she [the carer] doesn’t even come up; my ma [mother] wouldn’t have a chance to go in and have a wash or anything.” Because I’m not allowed to get in the shower on my own. (Betty, day centre attendee)
In some cases, the advocate was a health or social care professional, who made the case for the older person to get into a day care center or to receive home care. Audrey recounted how “she [Audrey’s social worker] fought for it [home care] and I [now] have carers coming in the mornings.” These participants felt that they had a measure of control over their situation by alluding to concrete ways or strategies through which they could assert a degree of control over their care, with the help of their advocate. The availability of the advocate transformed the experience of care from one of potential dependence to one where the care recipients were able to exercise their agency.
Some participants spoke about those caring for them as providing a highly individualized, person-centered care: “they [staff at day center] look after everyone individually, you know, each person was looked after individually with their particular problem” (Alfred, day care attendee). For instance, if they were “out sick or anything” the manager at the day care centre would phone to check on them and send over their meal. In some cases, the manager had even visited them in hospital. In these cases, it was signaled that the formal care staff were entering family-like roles, that is to say, their behavior resembled the normatively expected behavior of a family member rather than a paid professional. Participants spoke warmly about how attentive a particular nurse or carer could be. For example, Joe spoke about how his carer looks after him as if she was family: . . . she often helps me to shower, things like that. In fact, she’s a real mammy [Irish colloquial affectionate expression for mother], she says: Joe why don’t you leave your clothes on the radiator so you’ll be wearing warm clothes. I go back to my childhood (laughing) so she’s very good. (Joe, day centre attendee)
Among the Traveling community participants, social capital in the form of family networks and supports was taken for granted. The focus group with older Travelers took place at a Traveler-specific primary care building which is set within a halting site that holds 49 caravans (mobile homes). These caravans were situated within bays, each of which had a shed with a bathroom facility. A discussion ensued on how there was little need for formal home help or home care packages in this community as there are relatively few Travelers who reach old age and because family members are the source of personal care. As a result, the services that had been focal point in other group discussions (home help, home care packages, day centers) simply did not feature here. The following extract illustrates the close proximity and constant presence of multiple family members across three generations, a cultural and social context where the lives of different family generations are closely intertwined:
Yea but people don’t tend to live on their own here, so?
Well no.
Well the likes of here there’d be a crowd like here.
Because like just for example, Olivia’s son would live in the bay with her. Like he wouldn’t live in the caravan with her. But he’d live in the bay, so therefore. And then her other son, like Martin is around and David. So, there’s always kind of.
So, family support is there?
And then grandchildren yea. And which is huge for the Traveler community to have that network.
In contrast to the numerous examples of the caring and respectful managers, advocates, and (quasi-)family members, we heard some anecdotes that provided a counterpoint, that is, accounts of situations where the older person’s status had come under threat. Participants singled out people who do not defer to old age and described them as “rude” and “cheeky” people who did not conform to their expectations of respecting an older person. In these descriptions, participants felt powerless and dependent on others to restore normal order. For example, Lena told us about an unpleasant altercation with a taxi driver on her way to a doctor’s appointment. However, once she arrived at the doctor’s surgery, order was restored in the sense that she again became a respected recipient of attention and concern: I got into the doctor’s and the girl [the receptionist] knew by my face there was something wrong, “are you okay Mrs Murphy?” “No” I said “not really you know.” She said “sit down there and I’ll make you a cup of tea.” Made me the cup of tea . . . “Mrs Murphy are you under stress?” “Well” I said “I had a bit of an exciting trip in [the taxi].” “Oh no,” she said “that’s not right.” (Lena, day centre attendee)
Lena finished her anecdote by emphasizing that she would consider it shameful if her grandson behaved in a manner similar to the taxi driver, suggesting that her family is capable of imparting norms of respect for the older person, whereas such norms are breaking down in parts of the wider society.
In summary, older adults’ constructions of dependency and assistance in the context of home and community care services reflected their access to and use of social capital which took various forms: access to family members or senior care professionals was the most valued form of social capital. We now turn to outlining age capital, which was deployed alongside social capital in positive accounts of dependency to justify and legitimize the receipt of care services.
Legitimizing Dependence Through Age Capital
Our concept age capital encompasses various age-related justifications for legitimate receipt of care and support services. Older adults referred to physical impairments or living situations associated with advanced age, such as “I’m on my own” (as a result of the death of spouse), as justifications for deserving and accepting help. Many times participants outlined in great detail the event or incident that had triggered an intervention from the “boss,” family member, or an advocate to refer them to help. Older men often evinced a sense of entitlement on the grounds of their various efforts in paid work, explaining that they have worked hard all their lives and deserve care as a “payback” for their economic contributions.
Participants who relayed an adverse health event as the trigger for care expressed this as an almost self-evident chain of events from cause to effect: “it [home care] all started with a heart attack”; or “I had to have it [pendant alarm], when I fell in the house”; and “it took the accident I had to get me extra carers at home.” John explained how, following a period of illness, he “can do nothing, because the daughters and sons do everything now, I can’t do anything.”
A particular health event and living on their own frequently overlapped as key factors in leading to acceptance of help: “the lady [the carer] comes in the mornings . . . only since I had this accident. Because I’m on my own” (Audrey, day care attendee). In addition to physical care needs, many participants saw living on their own as an important justification for outside intervention. They spoke of the need for companionship and mentioned that they felt “stuck into the house” and this “can be very lonely.” Attending the local center had had a positive impact on the well-being of all research participants who were members of such groups. They enjoyed the social aspect that the center brought to their lives such as “meeting people” and “friends and having a chat with them.” As Elaine explained: [A nurse had said to her]: “Elaine you couldn’t sit here [in her home] all day on your own.” So [the nurse] got me down here [to the centre] [. . .] That’s the only reason [I got help] because I was on my own. (Elaine, day centre attendee)
Research participants who were part of a pilot program for companionship home visits commented that they had accepted the companion service, not because they were dependent but because they were on their own. Brid told us: “I didn’t need the home help because I’m able to cook and do my own things’ but she added that ‘it’s lonely because my husband died five years ago’.”
These examples indicate not only that adverse events and risks are connected to receiving help but also that older people felt they had little choice in the matter—“I had to have it”—as otherwise they would be putting themselves at risk or would not be able to manage their daily life. A small number of participants acknowledged having cognitive impairment—“the brain is fizzling out”—and presented this as a justification for receiving help in old age. The participants’ statements express the notion that their age-related physical and mental impairments legitimize the assistance they receive. Participants commented that they would not be able to manage without help or they would cope “with some great difficulty” especially where family members “are working people” and have little spare time.
Being old per se could also be presented as a central justification for getting help. Despite being able to do things for himself and being overall in good health, Robert accepted home help because of “the age factor . . . I’m 89 [will] be 90 next January.” Although we did not ask for their ages, participants often spontaneously mentioned their age with some pride, implying that a long life confers a status or age capital in itself. Where longevity and a record of various contributions over life time were related to services, there was a clear implication of deserving or being entitled to home care. Male participants in particular felt they had worked hard and provided for their family, and now it was their turn. James suggested that he and others like him—former lifelong diligent taxpayers—were entitled to be cared for: It’s probably right that she [companion] should be there. Like I’ll be 75 now on my next birthday. But I worked all my life, I paid up [social insurance] stamps and PRSI [Pay Related Social Insurance] and all that. Maybe the likes of us should be kind of cared for. We shouldn’t be left on our own altogether. (James, availing of companionship care)
Participants therefore identified various age-related reasons for why they deserve the care and support services: old age per se, living on their own, an age-related health event, or a lifetime of contributions to the state. We label this age capital as these justifications for deservingness are all in various ways associated with personal history and merit across the life course and ultimately, longevity and living situations that tend to accompany it. In older adults’ accounts, longevity equalled contributions and knowledge that could be “exchanged” for or used to justify “deserving care.”
We now turn to discussing how older adults presented the experience and status of dependency when they accepted it, or rejected it.
Older Adults Displaying Dependency as Status
Many participants signaled pride in being surrounded by people who were willing to help them. As outlined above, kind and helpful formal carers and their managers featured prominently. Numerous examples were recounted of helpful adult children and grandchildren, who would “pop into” the house to fix or move things for the older person, or simply to say hello. This social capital allowed older adults to present themselves as not dependent on formal services: they were (relatively) independent to the extent that family help and access to formal advocates facilitated this. The examples of having someone close by—typically sons, daughters, or neighbors—who one can depend on were presented as socially acceptable, even prestigious dependency. For instance, Jack presented himself as an older person who is surrounded by adult children who are “very, very good” to him, and with him “all the time.” He happily accepted help from his sons and daughters to drive him where he needed to go and this ability to rely on help as well as company from his children allowed Jack to “relax” which he framed as “very good”: . . . they [sons and daughters] look after me so well they do, anywhere I want to go they just say do you want to go there Jack . . . which is very good you know what I mean, they are very, very good to me. Because I can’t drive anymore, I can’t even play football anymore you know or play golf you know what I mean I just have to relax. Which is very good you know and they are with you all the time.
In addition to close and supportive family and informal networks, older adults pointed to good quality formal services as the key factor that allowed them to accept help. Where health and social care professionals demonstrated a highly individualized approach, participants felt that they were receiving a superior service and were not shy to emphasize this. Melanie’s comment about her carers—“they do loads of things for me”—both indicate a level of dependency on her part and signal her pride as the “object” of attention and care: One of the carers gave me a list; I couldn’t believe they even know what I like on the telly. And all the things I’m entitled to. Washing you, making a meal for you. [. . .] they do loads of things for me. (Melanie, day centre attendee)
The focus group of older adults who volunteer on a senior (telephone) help line told us that in their estimate, the majority of older people, about 75%, have this type of informal support. The remaining 25% they framed as the abject, pitiable dependent people who need the kindness of strangers, formal care workers, volunteers, or distant relatives who spend time with them as an act of charity. There was a clear implication in their views that there was “bad” dependence and “good” dependence where adults could rely on their social capital, especially where family members feature as the main caregivers or as reliable back-up to formal care. In our focus groups, the accounts of “good” dependency prevailed, as the older participants sought to present themselves as cared-for individuals. Some presented themselves as receiving a lot of attention and regular calls from both formal care workers and informal network members comprising family, friends, and neighbors: I do have the carers coming in and then my two sisters; well they ring during the week days. And maybe sometimes they call out. Any even some of the neighbours they do knock at the door and then I’d be alright. (Patricia, day centre attendee)
Participants flagged their status as older people who are cared about, corroborating this status through anecdotes such as neighbors hurrying to check on them in the case of an emergency: The gas went and the light went, everything. And the neighbours knocked immediately to see if I was alright you know [. . .] Straight away it was only about three minutes and they were knocking in at door, and someone said, “Have you got candles, are you okay?” (Bea, day centre attendee; emphasis added)
By volunteering the information about her forthcoming 100th birthday, Dolores exhibited her age capital, and used humor to signal her position as an older person who has come to terms with the need for daily personal care, and made the whole group laugh at her humorous allusion to intimate care: Yea she’s [care worker] very good; she’s a good girl, yea. I have her for an hour in the mornings, yea. I can’t tell what she does for me because there’s a gentleman here. I’ll whisper you. (All laugh) (Dolores, day centre attendee)
Although in receipt of help and indeed sometimes almost under constant benign surveillance, older adults explained or implied that this was a reflection of being valued and cherished on grounds of their age, disabilities, and deservingness. This association between dependence and status transforms the picture of an older person who is the “object” of care and attention into a prestigious, valued position of the cared-for older person that is (usually implicitly) contrasted to an older person who is left without adequate care.
Independence as Status
Although acceptance of help was perhaps surprisingly easy under the right conditions such as being invited to receive care by a warm person in authority or being surrounded by family members, there were a smaller number of older adults in our sample who signaled pride in not needing help in their own home, or even rejecting it outright. For instance, some participants highlighted an adverse health event and living alone as the only factors that had led to their attendance at a day care. They were keen to present themselves as persons who had “a full life . . . outside . . . other activities,” thereby distancing themselves from the negative image of a dependent or isolated older person.
To illustrate the kinds of subtle signaling of (in)dependence that emerged in the focus groups, we include here two sequences from Focus Group 5, held in a day center in central Dublin. At first, the conversation is led by Cora, a woman who had turned down an offer of support following an adverse health event:
Well I find if you can do something, do it yourself, if you think you can do it, go and do it yourself.
Yea.
Yea.
Instead of depending on somebody else.
Yea and give it to somebody that’s worse off, you know that’s what I said to the nurse. Give it to somebody that really needs it.
Yea.
At the moment I don’t because I. [interrupted]
The way I look at it there’s someone out there worse than I am.
I said that to her.
Worse off than I am.
There is always somebody worse off than you. [. . .] And it’s nice to help people if you can, if you know what I mean.
Cora signals independence and pride in being independent, and several group members affirm her assertion of independence. They also put on a display of magnanimity in identifying themselves as the kind of people who look out for other, “worse off,” older people: the downward comparison group that they contrast to themselves. A sense of righteousness emerges here, before the intervention by Jane who asserts her right to receive help, even though she does not see herself as one of the “worse off”:
Well I have a carer. And I’m not worse, there’s a lot worse than me, but I have one in anyway.
Sure
Jane you can’t walk, so.
Well I can’t walk but.
Yea but even so.
I can talk and tell you.
Ah yea but I mean sure you don’t need a carer for that. (Laughs)
You can give out [complain] as well. (Laughs)
Jane subtly indicates her rejection of what she perceives as self-righteousness of Cora, Agnes, and Felicity. She defines herself as someone who is a deserving care recipient despite not identifying as one of “the worse off.” Jane also signals her ability to be assertive (despite her seemingly dependent status), and Cora quickly points out her physical disability (inability to walk) as a legitimate reason to receive care, before the discussion is humorously diverted to a different, safer topic by group members who have noticed the emergence of a potential conflict of views.
Adele also felt “quite capable” of doing things herself, and she emphasized her agency by adding: “if I wanted help, I’d get help you know.” Lorena (in receipt of companionship care) told us that doing things by herself gave her “something to do.” Mary (day center attendee) told us she felt abandoned by formal care services as she had an ulcer in her leg and nobody had changed the dressing in months. Her son was very upset about this but was unable to do anything. Susan and Estelle subtly indicated disapproval of Mary’s failure to take action on her needs:
I think I’d go to my doctor, especially if I had an ulcer on my leg. And I wasn’t changed for four months.
Your GP (General Practitioner) you mean?
I’d go to the GP, yea. Because I mean to me that’s leaving it wide open to infection and everything, if it’s oozing or anything.
And you did feel it throbbing last week a lot didn’t you? You felt your leg throbbing.
That would be, me I would go to my doctor, my GP.
Susan and Estelle were getting frustrated about what they perceived to be lack of assertiveness and action on Mary’s part. They signaled their status of being more agentic, by emphasizing that they would take action and not become pitiable or dependent by virtue of their own actions and reactions against dependency. These “independent” participants expressed a degree of disapproval of those older people whom they perceived as incapable of looking after themselves, thereby engaging in discourse that can be seen as subtly stigmatizing.
Discussion
The analysis above gives us grounds to challenge the notion that dependency in old age in the Western context is always experienced as negative or at best accepted, and to argue that this premise fails to fully recognize that dependency is socially constructed. Dependency, through the deployment of social capital and age capital, can be differentiated into “positive” and “negative” or “legitimate” and “illegitimate” dependency, or subtle variations of these. Older adults themselves are active, agentic meaning-makers in these processes: the way they think, feel about, and present their situations when in receipt of care matters.
Our findings indicate that, drawing on social capital derived from supportive family relations or trusting relationships with formal care providers, older people can signal their position as “cared for” individuals who openly display and acknowledge their dependency, and transform it into a marker of status. Many of the services the older people in our sample availed of had come to them in the form of professionals such as social workers and public health nurses who had reached out to them in person—and this personal contact had persuaded the older people to take a step such as trying out a day center. The “bosses,” the “advocates,” and the quasi-family members were described as doing all they can (“the whole lot”) and making “all the arrangements” in a manner that enabled the participants to be comfortable with, and even proud of their dependency. Personal knowledge of these people and trust in them were important for acceptance of help. Arrangements made for the older persons to access services were spoken of in a positive light. In relaying these stories of their pathway to a day center or other services, the older people signaled satisfaction and pride in having social contacts who cared about them and acknowledged them as valuable people, despite their need for some care or support. Age capital was deployed to justify and legitimize dependency. Participants saw their old age and declining functional abilities as a legitimization of dependency. Also, important for some participants was the sense of entitlement and deservingness that was illustrated through reference to lifelong contributions to the state.
In contrast to the notion that dependency would be abhorrent or even stigmatizing, most research participants’ accounts indicated that they were comfortable and felt secure in being the “objects” of attention and care. Attention and care can transform an older person who is abject (for instance, because he is no longer able to drive and hence is at risk of social isolation) into a very different picture where his needs are met and he is cherished (because his family members readily offer him lifts anywhere). The figure of the taxi driver emerged in one of the participants’ stories as the counterpoint to the caring professionals and social network members because he lacked the kind of helping attitude and respect that the care services providers generally demonstrated toward older people. The taxi driver was presented as a threatening figure, representing the abhorrent rejection of older adults as people whose status and limitations are taken into account respectfully.
However, a minority of participants in our sample were keen to present themselves as independent. These participants compared themselves to others who were “worse off” or, in their view, had failed to take sufficient responsibility for their own health and well-being. In doing so, they constructed boundaries between socially accepted dependence and people who were pitied, or construed as self-neglecting. In the micro-contexts of their daily routines, actions, and interactions, these older people constructed meanings of independence that reflected their personal circumstances and resources.
Conclusion
In this article, we have challenged some of the dominant ideas on (in)dependence of older adults in receipt of care services in the community and contributed novel insights that emerged from our original empirical data and the application of Goffman’s and Bourdieu’s concepts in analyzing it. We have illuminated how independence and dependence can be intertwined in a manner that transforms dependence into a valued state that can be used to signal status and even presented as prestigious, denoting a respected and cared-for older person. In the Western frame, dependency is to be avoided at all costs, but we argue that some older people choose and are able to embrace dependency in a way that reflects and demonstrates their status and agency—hence the concept of dependency as status. This of course does not mean that people are feigning an “excess dependency” just to access services, only that certain actions can help people who are in need of assistance to accept and access that help. Our application of Bourdieu’s and Goffman’s theories was helpful in developing conceptual tools to understand the social and symbolic (age) capital needed to be in a position to convert—and present to others—dependency as a sign of status.
From Bourdieu, we applied the concept of social capital as it chimes with the older people’s accounts of how they came to appreciate and accept help, care, and support. Furthermore, we adapted Bourdieu’s concept of symbolic capital to the context where older adults took recourse to their age and age-related justifications to legitimize their receipt of care. In addition to Goffman’s concept of stigma resonating with the portrayals by the older people who highlighted their independence, Goffman’s ideas pertaining to how we present ourselves in everyday life helped us to make sense of the ways in which older focus group participants cast themselves as either “cared for” persons or as independent. Of course, to apply Goffman, a confident presentation of “dependence” or “independence” in the company of others does not necessarily translate into confidence in private.
Social capital was an important factor in allowing older adults to accept a level of dependency and to redefine this in their own terms. Conversely, where social capital is not present, it may not be possible to construe dependence in positive terms. Similarly, age capital was valuable symbolic capital in so far as old age and receipt of care could be presented as the rewards for a life well lived. Older people felt they were entitled to care that reflected their long and meritorious life trajectories. Within a macro-context of privatization of care services (André & Hermann, 2009; Lolich, 2019) and a context where the responsibility of aging successfully (Timonen, 2016) is placed on the individual, these claims are more easily available to groups that possess social and economic advantage. For instance, age capital arising from the ability to contribute to the state in the form of taxes and social insurance payments is accessible for those who were in paid formal employment and had long careers. Furthermore, while we think that the expectations about deference are not unique to Ireland, further research across different contexts is needed to advance our understanding of contextual similarities and differences with regard to (in)dependence as status. The ways in which different groups of older people (e.g., men and women, people from different ethnic and cultural backgrounds) view and deploy their status as care recipients are topics ripe for further interrogation.
As our research was not focused on developing specific interventions, we are hesitant to make strong recommendations. Nonetheless, it is clear that both care professionals and members of informal networks can make a difference to older persons’ acceptance of help and care by offering services and support in a manner that affirms the recipients’ worth and agency in deserving and accepting care. Service providers can adopt and engage myriad tools, devices, policies, and phrases that signal to care recipients that they deserve and welcome users of the services they offer. Seemingly, small gestures, such as reassuring an older person that they are entitled, to apply for a service can foster the sense that seeking care is normal and welcome. Ensuring that service users understand and can access communication and complaint channels can give them a greater sense of control and worth. Paying particularly close attention to respectful language, for instance, checking whether they prefer to be addressed by their first name or by a title (“Mr,” “Ms,” “Mrs,” etc.), might be a highly important signifier of status for some older persons. These are just some examples of how services can strive toward a situation where being a care recipient amounts to a valued status for an older person.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data discussed in this article relates to the H2020 SoCaTel Project. This project has received funding from the European Union’s Horizon 2020 research and innovation programme under grant Agreement No 769975. The relevant contents of this publication are the sole responsibility of the authors (Timonen & Lolich) and can in no way be taken to reflect the views of the European Commission.
Ethical Approval
This research was granted ethical approval by Research Ethics Approval Committee in December 2017.