
Abstract
The purpose of this study is to conduct a cross-cultural comparison of perceived public stigma of mental health and views on mental health treatment effectiveness and their effects on service use among the U.S. adult population of White, Black, and Hispanic ethnic backgrounds. The pooled data came from the 2007, 2009, and 2012 Centers of Disease Control and Prevention (CDC) Behavioral Risk Factor Surveillance System (BRFSS) survey, which included unweighted sample sizes of 149,344 Whites, 11,156 Blacks, and 11,072 Hispanic adults aged 55 years old or older. For both 55 to 64 and 65+ age groups, White respondents were most likely to hold greater perceived public stigma. Middle-aged Hispanic adults also showed high levels of perceived public stigma, though not as high as White counterparts. Hispanic adults of both age groups had the least favorable views on the effectiveness of mental health treatment. Among Whites and Hispanics who were not psychologically distressed, unfavorable views on treatment effectiveness significantly reduced the likelihood of seeking mental health services. Given age and ethnic differences in perceived public stigma and views on mental health treatment effectiveness, future efforts aimed at combating stigma should be tailored around various factors for effective intervention strategies.
Keywords
Introduction
Mental disorders are common among older adults, yet often go undiagnosed and untreated. A lifetime prevalence rate of being diagnosed with a mental disorder is estimated at 26.1% among those aged 60 years or more in the United States (Kessler et al., 2005), and the previous 12-month prevalence rate of having a mental disorder among those aged 65 and older is 20.4% (Karel, Gatz, & Smyer, 2012). Mental disorders among older adults (e.g., mood, anxiety, substance abuse disorders, or dementia such as Alzheimer’s disease and vascular dementia) are a significant burden on both an individual’s health and also on society. Depressive disorders not only impair daily functioning and cause great suffering, but research has shown depression to have deleterious effect on the treatment of other chronic diseases (Chapman, Perry, & Strine, 2005) and hinder recovery from an illness (Groessl et al., 2007). Untreated mental disorders may lead to the fatal consequence of suicide. Older men have the highest suicide rate, especially among those aged 75 and older (36 per 100,000 individuals; Centers for Disease Control and Prevention [CDC], 2012a). Despite these grave consequences, older Americans underutilize mental health services (Bartels, Blow, Brockmann, & Van Citters, 2005), especially among ethnic minority elders such as older African Americans with mental health disorders (Conner et al., 2010) and older Latinos (Alegría et al., 2008; Jimenez, Cook, Bartels, & Alegría, 2013).
Mental health and access to mental health services are one of many essential elements to ensure quality of life in the aging process. To better understand the aging process, some conceptual and theoretical frameworks of aging such disengagement theory (Cumming & Henry, 1961), activity theory (Lemon, Bengtson, & Peterson, 1972), and continuity theory (Atchley, 1989) had been proposed in the latter part of the 20th century (Johnson & Mutchler, 2014). Such frameworks evolved into alternative views of later life such as selective optimization with compensation (SOC; Baltes & Baltes, 1990) and “successful” aging (Rowe & Kahn, 1997). The successful aging framework by Rowe and Kahn (1997, 2015) includes three components: low probability of disease and disease-related disability, maintenance of high mental functioning, and active social engagement. In particular, one of three components, “maintenance of high mental functioning,” may be closely associated with older individuals’ ability to access mental health resources and utilize relevant mental health services and programs. Nevertheless, older individuals are faced with multiple barriers to access and utilization of mental health service use such as cost, transportation, lack of insurance, and use of culturally sanctioned services. Stigma and attitude about mental illness have been pointed out as other barriers (Bartels et al., 2005; Substance Abuse and Mental Health Services Administration, 2005). An investigation into mental health stigma among older adults as a possible barrier in their later life would make an important contribution to ongoing efforts to develop and refine interventions and programs aimed at maintaining and enhancing mental health functioning and their qualities of life.
Stigma is defined as having a negative belief about either the self or a group and a resulting prejudiced behavioral response (Corrigan & Watson, 2002). Stigma can be understood through three major theoretical frameworks: social identity, self-stigma, and structural stigma (Overton & Medina, 2008). The first theory is based on the construct of social identity by Goffman (1963) and involves how societies or large groups within societies use socially constructed norms when assessing someone who is different. When applied to mental health, persons with mental illness would be considered “different.” Stigma results from a discrepancy between two identities: “virtual social identity” (how a person is characterized by society) and “actual social identity” (the attributes really possessed by a person) (Goffman, 1963; Yang et al., 2007). The second theory, self-stigma, suggests that stigma occurs as an internal evaluation process whereby individuals judge themselves as being dehumanized, devalued, and inferior and feel shame as a result (Corrigan & Watson, 2002; Overton & Medina, 2008). Finally, structural stigma is an external evaluation of a person with regard to societal norms (Link & Phelan, 2001) that focuses more on the relationship between structural (e.g., discriminatory and/or exclusionary policies and laws) and interpersonal factors (e.g., prejudice and behaviors leading to increased social distance and status loss; Ungar, Knaak, & Szeto, 2016). This type of stigma may mean denying people with a mental illness their entitlement or access to experiences that people who are considered “normal” may easily access. For example, persons with mental illness may face difficulty engaging in empathetic and supportive relationships with others, happiness, participatory citizenship, and peace of mind. Structural stigma further posits that the effects of social processes in the greater sociocultural environment can be observed on an individual level in the form of discrimination.
Building upon the second and third theories of stigma, self-stigma and structural stigma, public stigma of mental illness refers to the extent to which the general population collectively holds negative beliefs and attitudes about mental illness and the degree to which they discriminate against those with mental illness (Corrigan, 2000). As one type of stigma under investigation in the present study, perceived public stigma is further defined as an individual perception of how the public holds stigmatizing attitudes toward those with mental illnesses (Corrigan, 2004). Greater perceived public stigma is known to adversely affect help-seeking intentions and behaviors (Cooper, Corrigan, & Watson, 2003; Gulliver, Griffiths, & Christensen, 2010), particularly among older adults (Conner et al., 2010; Jimenez et al., 2013). Stigma was identified as the fourth leading barrier to accessing mental health services (Clement et al., 2015) and is considered as one of many causes for older adults to not seek mental health treatment (Katona & Livingston, 2000). As a result, the adverse impacts of mental health stigma among older adults have received growing attention (Conner et al., 2010; Karel et al., 2012). Specifically, high levels of perceived public stigma may cause a lack of engagement in treatment as well as lack of help-seeking intention. Rather than seek services for mental health, older adults will turn to primary care, as mental health issues are often accompanied by concurrent physical conditions (IOM, 2012).
Mental health stigma may be more pronounced among older adults from minority ethnic communities due to additional access barriers stemming from their cultural and linguistic background. Cultural values as well as advanced age may deepen stigma and negatively affect mental health treatment-seeking behavior and quality of care among older minority groups (Gary, 2005). Older African Americans were found to have experienced more stigma about mental illness than their White counterparts (Conner et al., 2010). Compared with non-Hispanic Whites, older African Americans tended to hold more negative views of depression and its treatment, considered it socially embarrassing, and were less likely to accept pharmacotherapy and psychotherapy treatments (Anglin, Link, & Phelan, 2006). There is, however, contrasting research by Gitlin, Chernett, Dennis, and Hauck (2012) who reported that less than 33% of older African Americans viewed depression as stigmatizing. African Americans from the 1990-1992 National Comorbidity Survey reported comparable and more favorable views on seeking care for their mental illness than did White respondents (Diala et al., 2001). When it comes to older Latinos, one study indicated that they viewed depression as a sign of personal weakness and reported believing that it would cause several consequences within the family, such as disappointment, burden, shame, or embarrassment (Jimenez et al., 2013). However, older Latinos have also been shown to hold positive perceptions of mental health treatment (Jang, Chiriboga, Herrera, Tyson, & Schonfeld, 2011). Due to conflicting results, the emerging body of literature on the topic remains inconclusive.
As an additional dimension, while many studies have investigated on individuals’ views on seeking mental health treatment, little attention has been given to the views on mental health treatment and its impact on service use. Only one European study was available which found positive association between perceived effectiveness of professional help and increased likelihood of using mental health services (ten Have et al., 2010).
In light of mixed results from previous comparative studies on the perceived public stigma and the paucity of comparative research on views on mental health service effectiveness among non-Hispanic White, non-Hispanic Black, and Hispanic groups of adults, this study attempts to address the following three main research questions, using a national sample of the three groups of adult population aged 55 years or older in the United States:
Method
Research Design and Participants
This secondary survey research design is based on the pooled data from the 2007, 2008, and 2012 Behavioral Risk Factor Surveillance System (BRFSS) surveys by the U.S. CDC (CDC, 2015). Since 1984, the BRFSS survey has been conducted as a monthly cross-sectional telephone survey by state health departments. The BRFSS survey typically collects prevalence data among the adult population aged 18 years or older from all 50 states, the District of Columbia, Puerto Rico, the U.S. Virgin Islands, and Guam on their risk behaviors, preventive health practices, and health care access for chronic disease and injury (CDC, 2015). The BRFSS conducted the survey only using landline telephones until 2011, at which point it began to include cellular telephone–based surveys. For the landline telephone survey, data are collected from a randomly selected adult in a household based on a disproportionate stratified sample (DSS) except in Guam and Puerto Rico which use a simple random sample design. The cellular telephone–based survey utilizes the Telcordia database of telephone exchanges and 1,000 banks to randomly select participants. State health departments conduct the interviews either in-house or by using contractors following guidelines provided by CDC (CDC, 2013).
In 2007, the CDC included an optional module on “Mental Illness and Stigma” that examined mental illness stigma (CDC, 2012b) along with its core components. The “Mental Illness and Stigma” module was repeated in 2009 and 2012; however, the module was not available to all the states and different states participated in the module each survey year. This study draws upon the data on perceived public stigma and attitudes toward mental health treatment effectiveness from adults in data from 21 states (i.e., AK, AR, CO, CT, IL, IN, IA, KY, LA, ME, MN, MT, NH, NM, OH, OK, OR, RI, TX, VA, and WI), the District of Columbia, and Puerto Rico in 2007, 16 states (i.e., CA, GA, HI, KS, MA, MI, MS, MO, NE, NV, SC, TN, UT, VT, WA, and WI) in 2009 (CDC, 2012b), and 13 states (i.e., IL, IA, KS, MN, MO, MT, NE, NV, NJ, NM, NY, OR, and WA) and Puerto Rico in 2012. While it was not a longitudinal panel study, the merged data from three survey years allow for an opportunity to conduct the investigation on the research questions across all of states in the United States. A sample used for this study includes non-Hispanic White, non-Hispanic Black, and Hispanic adults aged 55 years or older who were interviewed in 2007, 2009, and 2012. The unweighted pooled sample sizes were 149,344 Whites, 11,156 Blacks, and 11,072 Hispanic adults.
Measures
Perceived Public Stigma was assessed by one item, “People are generally caring and sympathetic to people with mental illness.” The degree to which respondents agreed or disagreed with this item was used to measure the perception of public attitudes toward persons with mental illness. Five responses ranging from agree strongly to disagree strongly were grouped into two: 0 = the low level (agree strongly or slightly) and 1 = the high level of perceived public stigma (disagree strongly or slightly) including a response category of neither agreed nor disagreed. This measure is consistent with the definition of perceived public stigma by Corrigan (2004) mentioned above. Previously, this single item to measure perceived public stigma was used by both CDC in the United States (2012) and the Scottish Government (2009).
Views on mental health treatment effectiveness was measured by one item, “Treatment can help people with mental illness lead normal lives.” Depending on the level of agreement or disagreement with the item, responses fell into two categories of attitude toward treatment effectiveness: 0 = favorable (agree strongly or slightly) and 1 = unfavorable (disagree strongly or slightly and neither agreed nor disagreed).
Mental health service use was assessed by one question, “Are you now taking medicine or receiving treatment from a doctor or other health professional for any type of mental health condition or emotional problem?” Response categories were “Yes,” “No,” “Don’t know,” and “Refused.” An affirmative response of “Yes” was considered as having used mental health services/treatment. The “Don’t know” and “Refused” responses were treated as missing.
Serious psychological distress was measured using the Kessler-6 scale (Kessler et al., 2003). The Kessler-6 scale assesses the respondents’ self-reported frequency of six items relating to psychological distress in the past 30 days with 0 (none of the time) to 4 (all of the time). Those with a cut-off score of 13 or more were considered as having serious psychological distress.
Frequent mental distress (FMD) was assessed by the number of days in the past 30 days that the respondents’ mental health was not good due to stress, depression, or problems with emotions. Respondents reporting 14 or more days of not good mental health were identified as having FMD (Zahran et al., 2004).
Sociodemographic variables of ethnicity, gender, age, education level, and income were included. Three ethnic groups were identified in the study: non-Hispanic White, non-Hispanic Black, and Hispanic adults. Although two separate questions were asked in the BRFSS survey instrument in terms of ethnicity (Hispanic and non-Hispanic) and race, in this study, all the respondents were initially coded into four groups of non-Hispanic White, non-Hispanic Black, Hispanic, and others. For the present study, the first three groups were selected for subsequent analyses. Age was divided into two categories: “55 to 64 years” and “65 years and older.” Four categories comprised education level: “less than high school,” “high school graduates,” “attended college,” and “college graduates.” Finally, income was measured by the following five categories: “>US$15,000,” “US$15,000 to US$25,000,” “US$25,000 to US$35,000” “US$35,000 to US$50,000” and “<US$50,000.”
Data Analysis
The data analysis procedure was guided by the research questions to be addressed. First, for ethnic and age differences in perceived public stigma and views on mental health treatment effectiveness, descriptive information was reported in terms of percentages, along with chi-square statistics. Second, logistic regressions were performed to identify significant correlates of perceived public stigma and views on mental health treatment effectiveness using dichotomous variables, 0 = agree and 1 = disagree. Third, adjusted odds ratios and the 95% confidence interval (CI) are presented. Finally, multivariate logistic regressions were performed on mental health service use (0 = No and 1 = Yes) to examine the effects of perceived public stigma and mental health treatment attitude on mental health help-seeking behaviors. Income as a correlate was dropped due to its multicollinearity with education. Separate analyses were conducted for each ethnic group. Missing data in the data set were analyzed with listwise deletion. Assumption for binary logistic regression include that two dependent variables are grouped into two categories which are binary. In addition, as the observations did not come from repeated measurements, an assumption of the independence of the observations is met. Finally, after dropping income variable, no multicollinearity among the independent variables was found.
All analyses were conducted without applying the weights to account for the difference in household size and for age, gender, and race distribution of the population. The primary reason for that decision is that there was a difference in the calculation of weights between data from 2007/2009 and 2012. The 2007 and 2009 BRFSS surveys used only landline telephones, whereas the 2012 BRFSS survey began to use both landline telephones and cellular telephones (CDC, 2012c). Therefore, the 2007 and 2009 surveys assigned the final weight based on the formula (FINALWT = STRWT × 1 OVER NPH × NAD × POSTSTRAT), and the 2012 survey was based on the raking weighting methodology consisting of design weight and raking (Design Weight = STRWT*(1/NUMPHON2)*NUMADULT). All statistical analyses were performed using Stata 11. This research was reviewed and approved as exempt by the institutional review board of the institution with which the author is affiliated.
Results
Sociodemographic Characteristics and Mental Health Status
Table 1 presents the descriptive information of sociodemographic characteristics and mental health status of the sample by ethnicity and age. Approximately two thirds of the respondents were female, ranging from 60% for middle-aged non-Hispanic Whites to 69.5% for older non-Hispanic Black respondents. In both age groups, more than half of Black (51.0% and 63.4%) and Hispanic respondents (56.4% and 70.9%) reported an education level of a high school diploma or less. Conversely, the majority of White respondents either attended college or graduated from college (68.9% for 55-64 age group and 54.1% for 65 or older group). In regard to income, slightly more than half of the middle-aged White respondents (52.6%) reported an annual income of more than US$50,000; however, less than one quarter of any other ethnic or age group reported a figure this high. Older Black and Hispanic respondents were more likely to report an income of less than US$15,000 a year, 32.6% and 48.2%, respectively.
Sociodemographic Characteristics and Mental Health Status by Ethnicity and Age.

Note. HS = high school.
Chi-square statistics presented indicate test of independence between ethnicity and sociodemographic characteristics/mental health status. The same analyses were conducted for each age group (55-64 and 65+), and the results (not reported here) were all significant at the p values of less than .001.
K6 score of 13+ was considered as the presence of serious psychological distress.
A report of 14+ day of poor mental health in a month was considered as having frequent mental distress (FMD).
In regard to the mental health status of survey respondents, middle-aged respondents (aged 55-64 years) were more likely than their older counterparts (65 or older) to be clinically distressed across all ethnic groups (3.7% vs. 2.0% for White, 6.2% vs. 3.9% for Black, and 9.9% vs. 5.3% for Hispanic). When it comes to cross-ethnic group comparison, Hispanic adults reported the highest prevalence rate of serious psychological distress in both middle and old age, 5.3% and 9.9%, respectively. This same pattern was observed for another measure of mental health status, FMD (i.e., reporting 14 or more days of not good mental health out of 30 days). A greater proportion of middle-aged respondents had FMD than their older counterparts, and middle-aged and older Hispanic adults reported the highest level of FMD. Finally, regarding the use of mental health services, which was measured by one item asking “whether they are currently taking medicine or receiving treatment from a doctor or other health professional for any type of mental health condition or emotional problem,” both middle-aged and older Hispanic adults reported the highest utilization rate (17.1% and 10.8%), followed by White (16.3% and 10.5%) and Black respondents (12.9% and 9.3%).
Age and Ethnic Difference in Perceived Public Stigma and the Views on Mental Health Treatment Effectiveness
As depicted in Table 2, non-Hispanic White and Hispanic adults tended to hold the highest level of perceived public stigma on mental health. Approximately 45% to 46% of middle-aged non-Hispanic Whites and Hispanic adults disagreed, whereas older adults of respective groups showed much lower level of disagreement at 36.8% and 40.8%, to the statement, “People are generally caring and sympathetic to people with mental illness.” Older non-Hispanic Black adults showed the lowest level of perceived public stigma at 31.2%.
Age and Ethnic Comparison of Views on Mental Health Treatment Effectiveness and Perceived Public Stigma.

Perceived public stigma was assessed by one item, “People are generally caring and sympathetic to people with mental illness.”
“Agree” includes both agree slightly and agree strongly from the original response categories.
“Disagree” includes disagree slightly, disagree strongly, and neither agreed nor disagreed from the original response categories.
Chi-square statistics presented indicate test of independence between ethnicity and two types of stigma in the study. The same analyses were conducted for each age-group (55-64 and 65+), and the results (not reported here) were all significant at p < .001.
Views on mental health treatment effectiveness was measured by one item, “Treatment can help people with mental illness lead normal lives.”
Results for the attitude toward mental health treatment effectiveness measured by the item, “Treatment can help people with mental illness lead normal lives,” indicated that both middle- and old-aged Hispanic adults showed the highest level of disagreement to the statement (i.e., the most unfavorable attitude), at 12.8% and 13.9%, respectively. In contrast, non-Hispanic White adults in general showed the lowest level of disagreement at 4.2% and 7.3%.
Correlates of Views on Mental Health Treatment Effectiveness
Results from multivariate logistic regressions on the views on mental health treatment effectiveness (1 = disagree, that is, having an unfavorable view on the treatment) are presented in Table 3. Across the three ethnic groups, the following correlates appear to increase the likelihood of having an unfavorable view on mental health treatment effectiveness: being female, being serious psychologically distressed, and suffering from FMD. Only among White respondents was advanced age (65 years or older) significantly associated with an unfavorable view toward mental health treatment effectiveness (odds ratio = 1.52, p < .001).
Multivariate Logistic Regression (LR) Results: Correlates of Attitudes Toward Mental Health Treatment Effectiveness.

“Agree” (favorable attitude) combines two categories of agree slightly and agree strongly and “Disagree” (unfavorable attitude) combines two categories of disagree slightly and disagree strongly from the original response categories for one item, “Treatment can help people with mental illness lead normal lives.”
p < .05. **p < .01. ***p < .001.
Correlates of Perceived Public Stigma
Table 4 shows multivariate logistic regression results on the correlates of perceived public stigma. Across all three ethnic groups, being female was significantly less likely to disagree to the statement “People are generally caring and sympathetic to people with mental health,” indicating for a lower level of perceived public stigma than their male counterparts (odds ratios = .61 for White, .78 for Black, .73 for Hispanic at the level of p < .001). In contrast, having a higher level of education increased the likelihood of reporting perceived public stigma than those with less than high school educational level. The effect of education was the most pronounced among the most educated group of Hispanic adults (i.e., college graduates), who were 2.82 times more likely to show perceived public stigma than those with less than high school education (odds ratio = 2.82, p < .001).
Multivariate Logistic Regression (LR) Results: Correlates of Perceived Public Stigma.

“Agree” (lower level of stigma) combines two categories of agree slightly and agree strongly, and “Disagree” (high level of stigma) combines two categories of disagree slightly and disagree strongly from the original response categories for one item, “People are generally caring and sympathetic to people with mental illness.”
p < .05. **p < .01. ***p < .001.
Also reported in Table 4 is the effect of serious psychological distress and FMD on the level of perceived public stigma. The presence of both psychological distress and FMD was significantly associated with a greater likelihood of reporting perceived public stigma. Non-Hispanic White adults with serious psychological distress were about 55% more likely than those without distress to hold perceived public stigma (odds ratio = 1.55, p < .001), compared with 28% for both Hispanic and non-Hispanic Black adults. Similarly, White adults reporting FMD were about 41% more likely than those without the distress to hold perceived public stigma (odds ratio = 1.41, p < .001).
The Effects of Views on Mental Treatment Effectiveness and Perceived Public Stigma on Service Use
A final step in the analysis was to examine the effect of views on mental health treatment effectiveness and perceived public stigma on mental health service utilization, while controlling for their correlates. Tables 5 and 6 present subgroup analyses on the effect of (a) views on mental health treatment effectiveness and (b) perceived public stigma on mental health service use, respectively. Results from multivariate logistic regressions on the use of mental health service (1 = Used) are reported in each ethnic group. Adjusted odds ratios with their 95% CIs are shown in the tables.
The Effects of Views on Mental Health Treatment Effectiveness on the Use of Mental Health Service: Multivariate Binary Logistic Regression (LR).
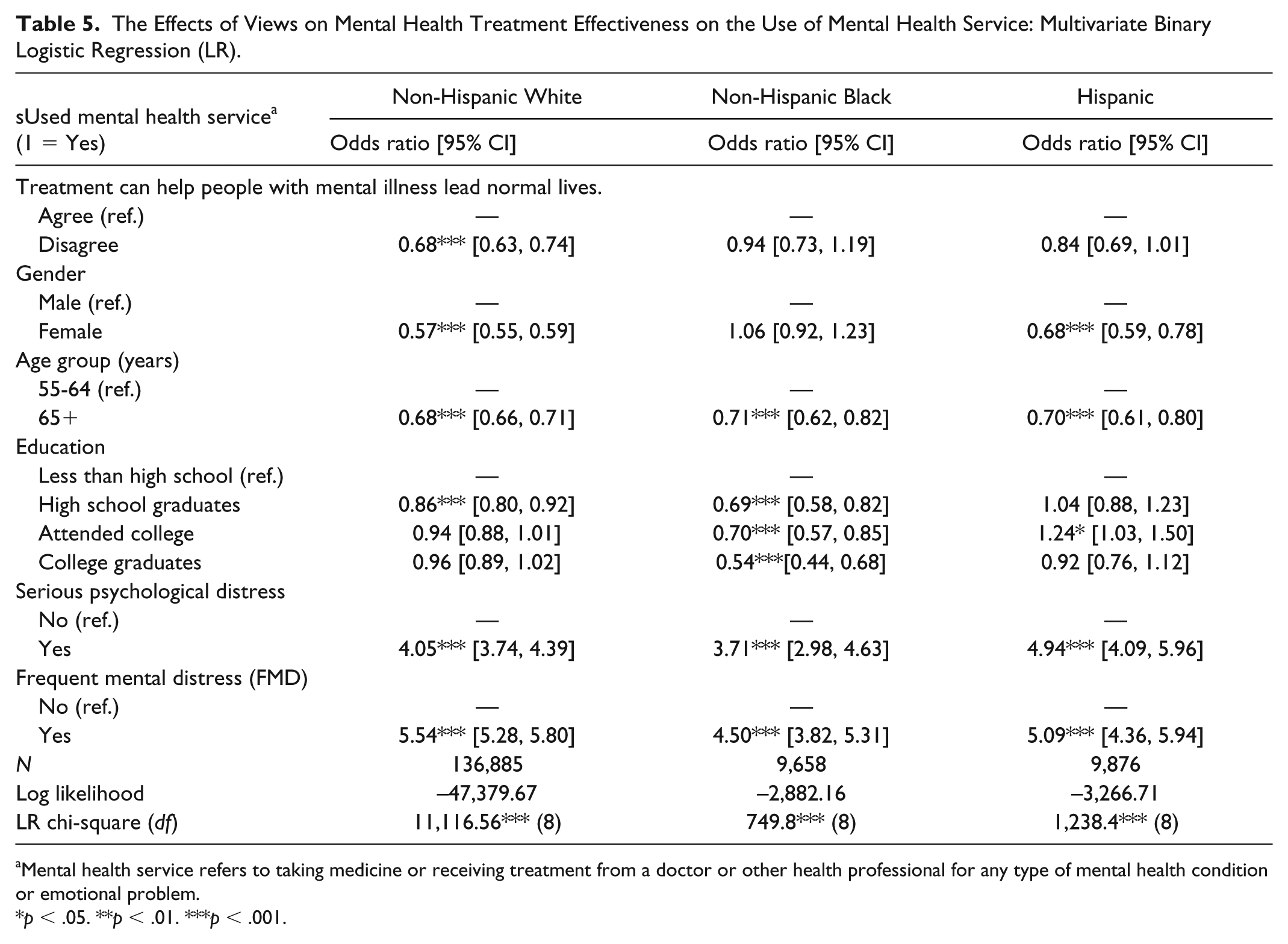
Mental health service refers to taking medicine or receiving treatment from a doctor or other health professional for any type of mental health condition or emotional problem.
p < .05. **p < .01. ***p < .001.
The Effects of Perceived Public Stigma on the Use of Mental Health Service: Multivariate Binary Logistic Regression (LR).

Mental health service refers to taking medicine or receiving treatment from a doctor or other health professional for any type of mental health condition or emotional problem.
p < .05. **p < .01. ***p < .001.
First, as reported in Table 5, views on mental health treatment effectiveness had a significant effect on mental health service utilization only for non-Hispanic White adults (odds ratio = 0.68, p < .001), after controlling for all other covariates. Non-Hispanic Whites with an unfavorable views on treatment effectiveness were significantly less likely to use mental health services than those with the favorable views, that is, by about 32% less likely to seek mental health service.
With regard to the effects of perceived public stigma on mental health service utilization, as shown in Table 6, the effect of perceived public stigma on mental health service use was significant for all ethnic groups, even controlling for the presence of serious psychological distress as well as other correlates. Respondents with a higher level of perceived public stigma had a greater likelihood of seeking mental health help than those with a lower level of perceived stigma (odds ratio = 1.32 for non-Hispanic Whites, 1.22 for non-Hispanic Black, and 1.29 for Hispanic).
Discussion
The present study examined age and ethnic differences in perceived public stigma and views on mental health treatment effectiveness, identified their correlates, and investigated their potential effects on mental health service use. Age was divided into two groups, adults aged 55 to 64 years and 65 years or older, and the U.S. participants were of three ethnic backgrounds—White, Black, and Hispanic. Results from the study indicated that (a) age and ethnic differences were significant in perceived public stigma and views on mental health treatment effectiveness; (b) gender, age, and education level turned out to be significant correlates of perceived public stigma and views on mental health treatment effectiveness; and (c) an unfavorable view was associated with lower level of mental health service use, whereas greater perceived public stigma was related to higher level of service use.
First, older Black adults reported a significantly lower level of perceived public stigma than other ethnic groups. This appears to be consistent with previous studies reporting more tolerable views of mental illness among older Black adults (Anglin et al., 2006; Gitlin et al., 2012). Among older Hispanics, the level of perceived public stigma was lower than that of older Whites. However, these results are at odds with recent findings on older Hispanics reporting greater shame or embarrassment of having a mental illness than non-Hispanic White counterparts (Jimenez et al., 2013). The inconsistency of this finding may be attributed to the fact that Jimenez et al. (2013) measured a different type of stigma than the one assessed in the present study.
Although this study may be the first to report on attitudes toward mental health treatment effectiveness across different ethnic groups, Jang et al. (2011) have previously looked at the attitudes of older Hispanics alone. The study reported somewhat an unfavorable attitude of older Hispanics toward mental health treatment effectiveness, as the results indicated that Hispanics perceived counseling to cause anger or sadness. Results from the present study appear to confirm such previous findings among Hispanic adults, who reported the most unfavorable views on mental health treatment effectiveness. However, when these results are considered in an international context, Hispanic’s overall rate of unfavorable attitudes about treatment effectiveness of 6% (ranging from 3.2% to 8.1% for middle-aged and older adults, respectively) was substantially lower than that of 32.2% reported in one European study (ten Have et al., 2010).
Second, gender, age, and level of education were found to be correlates of views on mental health treatment effectiveness and perceived public stigma among middle- and old-aged adults in the United States. These findings are somewhat consistent with previous studies on attitude toward mental health help-seeking behaviors (Riedel-Heller, Matschinger, & Angermeyer, 2005; ten Have et al., 2010). The present study found that females, older age group, and those with lower level of education were more likely to show favorable views on mental health treatment effectiveness and have a lower level of public perceived stigma. In contrast, males, younger age groups, and adults with a higher education level tended to have higher levels of perceived public stigma. The finding on the relationship between age and perceived public stigma appear to be consistent with previous research which suggests that older adults showed more positive perceptions of help seeking than their younger counterparts (Mackenzie, Scott, Mather, & Sareen, 2008). It should be noted that contrary to previous studies reporting that those in lower socioeconomic status (SES; income, or education) tend to express higher level of stigma are higher (Eisenberg, Downs, Golberstein, & Zivin, 2009; Evans-Lacko, Brohan, Mojtabai, & Thornicroft, 2012), this study found the association to be the opposite. As the perceived public stigma was measured by one single item in the study due to the constraints of the available data, direct comparison with other previous studies is not possible, but this shows a complex nature of the construct in the relationship between SES and mental illness stigma (Holman, 2015).
Finally, having an unfavorable view on mental health treatment effectiveness significantly decreased use of mental health services among Whites and Hispanic adults in this study. These results are congruent with one research in Europe showing that perceived effectiveness of professional help increased the likelihood of using mental health services (ten Have et al., 2010). However, the relationship between perceived public stigma and mental health help-seeking behaviors has previously been inconclusive: While Golberstein, Eisenberg, and Gollust (2008) and Lally, Conghaile, Quigley, Bainbridge, and McDonald (2013) found no such relationship, Vogel, Wade, and Hackler (2007) reported an effect of perceived public stigma on psychological help-seeking behavior, but the effect was mediated by internalized stigma. It would seem logical that significant perceived stigma would reduce the tendency to seek mental health help or service. However, this study found that a higher level of perceived public stigma corresponded to a greater use of mental health services, which appears to be counterintuitive. Nevertheless, the similar result was reported by Conner et al. (2010) in their study of internalized stigma. They found that contrary to their hypothesis, higher levels of internalized stigma were significantly associated with greater intention to seek mental health treatment. They attributed their counterintuitive findings to the observation that older adults who perceived the most stigma also had the highest level of psychiatric symptoms. Conner et al. (2010) concluded that even with high levels of stigma and negative attitudes, they were more likely to intend to seek treatment due to having a greater need. Jang et al. (2011) also reported the paradox that even with positive attitudes toward mental health services, older Hispanic adults underutilized these services. The present study showed similar paradoxical results consistent with previous research (Conner et al., 2010; Jang et al., 2011) even among those three different ethnic groups and lower rates of serious psychological distress or FMD. This could be in part because perceived public stigma was measured by a single item rather than a multi-item scale. Moreover, as noted above, different types of stigma (self-stigma vs. perceived public stigma) could have different effects on mental health service utilization or help-seeking behaviors.
While the present study is expected to contribute to the growing body of literature on mental health stigma, the following limitations should be noted. First, geographic location may have had an effect on the responses to perceived public stigma and views on mental health treatment as the place of residence may be a proxy measure of underlying socioeconomic conditions. As such, the 2012 CDC report based on 2007 and 2009 data included state-level information from other data sources in its analysis. However, it should be noted that neither state-level predictors nor geography was included in this study. The decision to exclude the geographical information was based on two reasons: (a) some states participated in two survey years and (b) there was a different sampling frame used in 2007/2009 (landline-based telephone only) versus 2012 (landline and cellular telephone–based survey). In addition to geography, contextual or environmental factors such as perceived discrimination or acculturative stress experienced by non-White respondents may influence not only their perception of stigma and views on mental health service but also their tendency to seek or not seek appropriate services. However, such contextual or environmental factors were not available in the data. Second, this study used a single-item measure each to assess the level of perceived public stigma and views on mental health treatment effectiveness. While multi-item scales of perceived public stigma do exist, only a one-item measure was available due to the nature of BRFSS as a surveillance or monitoring tool for population health. The use of a single-item measure might not have captured complex psychosocial construct of attitude or the stereotypes. This may also influence the study findings in a way that is not consistent with the previous studies that utilized the multi-item scales of stigma. For example, while non-Hispanic Black adults reported somewhat lower level of perceived pubic stigma compared with the other two groups, it may not indicate they have less stigma in general. Given the use of a single-item, this study cannot establish whether they internalize more stigma than other groups. Third, there is an absence of information on national origin for Hispanics. Mexican American and Puerto Rican Latinos often report very different perceptions about mental health and satisfaction with mental health services, which may influence the findings of the study. Lumping all Hispanic respondents together may represent heterogeneity of the group, limiting our understanding of their perceived stigma and views on mental health service effectiveness. Such differences might have accounted for the somewhat counterintuitive findings reported on perceived stigma and mental health-seeking behaviors. Finally, with a cross-sectional sample, since information at one point in time is used, it is possible for the individuals receiving treatment to perceive more stigma.
Conclusion
The results of this study suggest that perceived mental health stigma and views on treatment effectiveness are a function of a complex array of correlates such as age, ethnicity, gender, education level, and psychological distress status, which in turn affects service utilization. Community-level interventions aimed at reducing public stigma should take such correlates into account by customizing public messaging for intended groups, utilizing community health persons indigenous to the target group, and tailoring assessment and programming around the correlates. The development of a clear and accurate message about available mental health treatment and its effectiveness, unique to each ethnic background and age group, will be an important way to address barriers to accessing mental health services and will lead to better mental health outcomes across a diverse spectrum.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.