
Abstract
Differences in social status might impede teamwork and cooperation among health professionals. Against this background, we study the social interaction between health professionals using a simple experimental tool from behavioral economics (the dictator game). In our setup, physicians, nurses, and student nurses had to allocate monetary endowments between themselves and recipients, whereby the professional status of the recipient (physician, nurse, and student nurse) was varied. This way, we obtain insights into the prosocial motives of health professionals. Our results indicate a considerable amount of pure altruistic concern for the welfare of others among health practitioners, which also reaches across professional boundaries. These findings put concerns expressed in the literature on the doctor–nurse relationship such as a potential lack of team identity, in-group favoritism, and overly strict hierarchies along professional boundaries into perspective. Our study also paves the way for further experimental research on the relationship between social status and cooperation in the medical sector.
Introduction
It has long been recognized that the quality and efficiency of patient care crucially depend on the social interaction among health professionals. In medical settings and environments such as medical practices and hospitals, distinct professional groups like physicians, nurses, or student nurses have to coordinate their efforts to obtain optimal health outcomes of their patients. Hence, factors undermining effective teamwork across professional boundaries such as communication failures, disconcerted conceptions of professional identities, and responsibilities, as well as a lack of trust in the professionalism of colleagues pose serious threats for high-quality patient care and good patient outcomes (e.g., Baggs & Schmitt, 1997; Fewster-Thuente & Velsor-Friedrich, 2008; Gordon et al., 2011; Lingard et al., 2004; Muller-Juge et al., 2014). Evidence for the importance of teamwork on health outcomes abounds (cf. Leonard & Frankel, 2011). For instance, Powell and Davies (2012) find that professional boundaries between medical and nursing professions hindered the implementation of a new routine of acute pain service in U.K. hospitals. Curley, McEachern, and Speroff (1998) observe that improvements in interprofessional teamwork shorten the average length of stay by patients and reduce the average costs of these stays in a large teaching hospital in Ohio. Several studies also find significant effects of efforts to improve interprofessional collaboration among doctors and nurses on mortality rates (cf. Inglis et al., 2006; Martin, Ummenhofer, Manser, & Spirig, 2010; Schraeder, Shelton, & Sager, 2001). Overall, Schaefer, Helmreich, and Scheidegger (1994) estimate that around 70% to 80% of errors in medical practice stem from deficits in teamwork across professional boundaries.
Past research has highlighted that status differentials among the professions might impede teamwork in medical settings. Especially with respect to the interaction between physicians and nurses, it has been argued that strict hierarchies, based on the higher social status of the former in comparison to the latter, hinder effective cooperation across professional boundaries (cf. Feiger & Schmitt, 1979; Institute of Medicine, 2003; Schmitt, 1990). Two main mechanisms drive this negative effect of hierarchical structures in medical settings. First, pronounced status differentials hinder the development of shared identity as a team that cuts across professional boundaries and promote in-group favoritism (e.g., Liebe & Tutić, 2010; Tajfel & Turner, 1986) based on profession (e.g., Burford, 2012; V Lloyd, Schneider, Scales, Bailey, & Jones, 2011; Weller, 2012; Weller, Boyd, & Cumin, 2014). The second important mechanism refers to inefficient communication. That is, nurses might be prevented from contributing their expertise openly and communicating their ideas freely. Instead, low-status nurses tend to adopt specific communication styles that avoid any implicit questioning of the authority of the high-status physicians; this feature of communication in medical teamwork has been intensively studied by Stein (1967), as well as Stein, Watts, and Howell (1990) under the heading of “the doctor-nurse game.”
Critics have argued that due to changes in the organization of hospitals, the heuristic value of the doctor–nurse game has declined, and instead, the physician–nurse relationship should be conceptualized as a negotiated order (cf. Allen, 1997; Svensson, 1996) that allows for a more direct and hence productive communication among the professions. Nevertheless, status differentials still appear as a barrier for effective cooperation in medical settings. 1 For instance, Powell and Davies (2012) provided clear evidence that both within and also between the medical and nursing professions, status differentials impact patterns in communication and cooperation: “The main problem we had was getting somebody out of hours. Some of them [anaesthetists] were really rude, very nasty, but that was dealt with. I can’t say they [the pain service] didn’t sort it out because they did” (Nurse cited in Powell & Davies, 2012, p. 811). Similar evidence can be found in a number of other studies (e.g., Edmondson, 2003; Nembhard & Edmondson, 2006; Tucker & Edmondson, 2003).
In this article, we take a more fundamental stance on the problem of interprofessional teamwork in hospitals. Specifically, we study the question if and to what extent status groups such as physicians and nurses differ systematically in their prosocial preferences and behavior. We conducted so-called dictator games in several German hospitals. In a dictator game are two players. The so-called dictator receives a certain amount of money from the experimenter (in our case, each dictator received 10 Euro) and is told to split this amount of money between himself and the so-called recipient. Importantly, the recipient has no influence on the outcome of the game. The resulting allocation of the money is solely due to the decision of the dictator; the recipient is simply informed about the decision of the dictator and receives the money. The dictator game is a very simple and well-accepted measure for altruistic giving (Camerer, 2003). The higher the so-called donation, that is, the greater the proportion of the money the dictator allocates to the recipient, the more the dictator cares about the well-being of the recipient, that is, the stronger the altruistic preferences of the dictator regarding the recipient. Three types of medical and nursing professions participated in our study: physicians, nurses, and student nurses. Each participant played three dictator games in the role of the dictator; the status of the recipient—physician, nurse, or student nurse—varied such that each participant faced each possible type of recipient once.
This experimental design allows us to observe if status and professional groups differ regarding their altruistic preferences. Do the professional groups demonstrate a significant in-group bias in their altruistic giving? That is, are nurses more inclined to donate to other nurses than to doctors and do physicians donate more to other physicians than to nurses? Do the professions overall differ in their altruistic preferences?
We believe that answers to these questions are helpful in understanding the social processes that might block effective teamwork across professional boundaries in at least three respects. First, as already indicated, previous research on the physician–nurse relationship suggests that breakdowns in interprofessional collaboration are partly due to the fact that actors do not primarily conceive themselves as part of a team that cuts across professional boundaries, but identify themselves more with their respective professional in-group. Our experimental setup allows detecting any kind of in-group favoritism in altruistic giving. Second, the aforementioned negative effect of strict hierarchies based on status differentials seems to be also caused by the attitude of the physicians toward nurses, as well as the perception of these attitudes on part of the nurses. That is, if nurses are sanctioned repeatedly by physicians when communicating in a looser manner, it will diminish their eagerness to engage in this kind of interaction. Hence, prosocial, and in particular altruistic, motivations of physicians toward nurses should be considered a strong mediator for the effects of social stratification on communication and cooperation across professional boundaries. Finally, studying altruistic preferences of professional groups is also suggested by another perspective on teamwork in medical settings. Although all members of a team of medical professionals in charge of the health status of a specific patient benefit from improvements thereof, irrespective of the individual contributions made by each team member, the team effectively faces the problem of providing a public good. It is well-known that prosocial preferences of the actor are to be highly instrumental to overcome this social dilemma that precisely arises due to the fact that purely egoistic actors do not take the beneficial consequences of their contributions for the other team members into account. Therefore, also from this theoretical point of view, knowing more about the extent of altruistic motivation among health professionals is highly desirable.
The remainder of this article is organized as follows: section “Data, Experimental Design, and Hypotheses” describes our sample, the experimental design, and protocol, as well as measurements of key variables. In section “Results,” we present our results, and section “Concluding Remarks” concludes the article.
Data, Experimental Design, and Hypotheses
Data
The experiments were conducted in two hospitals and one school of nursing in a major city in Saxony and one hospital in a medium-sized town in Saxony-Anhalt, Germany, during the time period from March 2009 to June 2009. As other federal states in East Germany, Saxony and Saxony-Anhalt suffered from high underemployment rates of 19% and 21% in 2009, respectively. However, the health sector is one of the main employment sectors in both states, and there was and still is a shortage of doctors and nurses in hospitals (Fritzsche, Fuchs, Orth, Sujata, & Weyh, 2015). However, in 2009 and today, there was and is a rather high willingness of nurses and doctors to work abroad (Blum & Löffert, 2010), and hence, there was and is both out-migration and in-migration in the health sector (Kopetsch, 2008). Yet, in the hospitals in which we conducted our experiments, the overwhelming majority of employees did not have a migration background. A total number of 157 subjects participated in the experiments. The participants had different occupational backgrounds, 68 of them being student nurses, 65 working as nurses, and 23 of them being physicians. Data were originally collected by the authors and are available for replication upon request. Table 1 presents an overview of the composition of each occupational category with regard to sex, age, and educational background.
Occupational Groups and Socioeconomic Status.

Note. ISEI = International Socioeconomic Index of Occupational Status; SIOPS = Standard International Occupational Prestige Scale.
The participants played the dictator game three times, each time enacting as the part of the donor. They were asked to divide an amount of 10 Euro between themselves and one other person, the so-called recipient. In each of the decision situations, the occupational position of the recipient was varied.
Experimental Design
The documents including the instructions, the paper-and-pencil experiment, and one additional questionnaire were distributed to the physicians and the nursing staff during the weekly staff meetings. The student nurses received the materials during a school lesson.
The supervisor in charge of the experiments laid out the ground rules of the dictator game before distributing the documents. The participants were told that they had to make three allocative decisions on how to distribute 10 Euro between themselves and one other person. In doing so, they were able to give up any amount between 0 and 10 Euro to the other person and keep the remaining money to themselves. Emphasis was put on the fact that the other person was also employed in a hospital, however not within the same locality. Adding to that, it was expressed that the other person would never come to know of who had been in charge of the allocation. These instructions were also part of the written documents. Therefore, the anonymity of the decision was repeatedly underlined. To ensure anonymity toward the other participants and the supervisor, the filled out documents were returned in an envelope.
The nursing school participants filled out the documents on the spot, whereas the nursing staff and the physicians had 1 week to complete the papers and returned them to the supervisor during the next staff meeting. With this design, we cannot rule out that participants, in particular nurses and physicians, talked with each other about the experiment before or after taking their decision. Yet, this communication is restricted to communication within each occupational group and never occurs with a potential recipient or dictator. This should reduce concerns that communication did affect giving behavior as previous research only provides evidence for increased altruism among dictators if communication is allowed between dictator and recipient who actually interact in the game (Andreoni & Rao, 2011; Yamamori, Kato, Kawagoe, & Matsui, 2008). Moreover, if communication within an occupational group had an effect on the outcomes of our experiment, then it should have only led to increased giving to recipients of the same status group, but it did not affect giving behavior in interactions with recipients of different occupational groups.
The participants received their payments in accordance with the decisions they had made. Before taking a decision, they were informed about the following payout mechanism: Not all, but just one of the three decisions would have an influence on the determination of the payout. Which one of the allocations was going to be used for determining the disbursement would be decided at random by the supervisor at the end of the experiment. 2 Participants then received the amount that they had allocated to themselves in this particular round of the game. The payment was made in an anonymous envelope that could solely be assigned to the respective participant by a randomized number.
In the following, the exact wording of one of the three allocative decisions will be given: You receive the amount of 10 Euro. You can distribute these 10 Euro between yourself and another participant who is working as a nurse. What do you decide? Please pick full amounts of Euros such as 0,1, 2, 3, 4, 5, 6, 7, 8, 9, or 10 Euro Out of the amount of 10 Euro I am keeping Euro to myself and I am giving Euro to the nurse.
In the other two versions, solely the occupational position of the recipient was varied (student nurse and physician). To prevent effects due to ordering, the order of the decisions was completely randomized.
It has to be acknowledged that the recipient is fictional, meaning that the donations were not allocated to another person participating in the experiment. All of the participants were exclusively acting as dictators; the participants were deceived with respect to the existence of a recipient. This deception was mostly due to pragmatic reasons. For one thing, the formation of experimental pairings across schools and hospitals would need a lot of effort, which in turn would make it difficult to find participants. For another thing, the decision situation is a lot more credible when the participants get their money instantaneously (that was at least the case among the student nurses).
The acceptance of deceiving participants varies with the respective scientific discipline (Barrera & Simpson, 2012). Our overall approach is oriented to the common practice of sociological and sociopsychological experiments (e.g., Piff, Kraus, Coté, Cheng, & Keltner, 2010; Piff, Stancato, Côté, Mendoza-Denton, & Keltner, 2012) and is thereby in compliance with the ethical guidelines of psychological research (American Psychological Association, 2002).
Empirical Hypotheses
Even though our study is primarily explorative, it is still useful for the organization of our empirical analyses to formulate some hypotheses. As explained in the introduction, we aim at identifying if and to what extent the medical professions show differences in prosocial motivations. In this regard, both the literature on the specific interaction between medical professions and the literature on the interplay between socioeconomic status and prosociality suggest theoretical expectations.
Starting with the latter, first note that the medical professions under consideration show vast differences in socioeconomic status. Occupational positioning is assumed to be the key dimension of social stratification and determines income, class affiliation, and social recognition (Ganzeboom & Treiman, 1996; Hoffmeyer-Zlotnik & Geis, 2003). When measuring socioeconomic status, it is possible to apply a measurement as the International Socioeconomic Index of Occupational Status (ISEI; Ganzeboom, De Graaf, & Treiman, 1992). ISEI results range from 16 to 90. The occupational positions of student nurses, nursing staff, and physicians exhibit widely differing values with student nurses occupying the lowest level with 38 points, nursing staff being in the middle with 43 points, and physicians clearly occupying the highest level with 88 points, thereby being very close to the highest possible outcome.
The hierarchical ordering in terms of social prestige is similarly distinct. When applying the Standard International Occupational Prestige Scale (SIOPS) that ranges from 12 to 78, the rank of a physician obtains the maximum value of 78. The occupational prestige of the nursing staff that obtains the value 43 is markedly lower and followed by the student nurses who occupy the lowest rank with a scale value of 38 (Ganzeboom & Treiman, 1996). These differences in status were also reflected by the data we collected on the status variables education, age, and sex (see Table 1).
In the context of social class analysis, our approach is in line with the literature that calls for disaggregation of class analysis at the unit occupational level (Grusky & Sørensen, 1998; Weeden & Grusky, 2005). This literature suggests a close link between occupational groups and social status or class if occupational settings result in social closure, distinct attitudes and lifestyles, and so on. This seems especially relevant in the case of Germany as “[in] systems of this sort, workers must invest in a single trade early in their careers, and the correspondingly high costs of retraining produce relatively closed occupational groupings” (Grusky & Sørensen, 1998, p. 1220).
Thus, the medical professions under consideration form an unambiguous status hierarchy and allow for us to draw on the aforementioned literature on the effects of socioeconomic status on prosocial behavior. Whether higher social status comes with increased concern for the welfare of other actors or not is the cause of some controversy. For instance, Benenson, Pascoe, and Radmore (2007), Korndörfer, Egloff, and Schmukle (2015), Liebe and Tutić (2010), and Bekkers (2007, 2010) provide evidence that high-status actors act more prosocial than low-status actors. However, Piff et al. (2010; Piff et al., 2012) demonstrate that reversed relationship, that is, high-status actors act more egoistical and even unethical than low-status actors. On theoretical grounds, several mechanisms are discussed in the literature, of which, two are in the center of the debate. For instance, Liebe and Tutić (2010) argue that observed differences in prosocial behavior between high- and low-status actors do not necessarily need to be due to differences in prosocial orientations between the strata. Even in absence of such differences in prosocial motives, high-status actors might simply act more prosocial because of the microeconomic income effect. That is, high-status actors control more resources than low-status actors, and the “consumption” of the good “act prosocial” should theoretically rise with greater income. Piff et al. (2010; Piff et al., 2012), however, argue that the very fact that status differentials come with differences in material and nonmaterial resources makes high-status actors more independent from their social environment than low-status actors. Recurring on sociopsychological research on contextualism (Kraus, Piff, & Keltner, 2009), Piff and colleagues reason that because of this greater independence from others, high-status actors tend toward being less empathic than low-status actors. Although empathy is a strong predictor for prosocial behavior (Eisenberg, 2002), this theoretical mechanism suggests a negative relationship between status and prosocial behavior. Due to a lack of satisfying empirical indicators in our data, we abstain from testing these competing mechanisms directly and instead focus on the following two contradictory hypotheses:
These hypotheses relate donating behavior to the status of the donor. The literature (Liebe & Tutić, 2010) also discusses how the social status of the recipient affects donations in the dictator game. Interestingly, two important forms of prosocial preferences suggest different effects regarding the status of the recipient (Kolm, 2006). That is, pure altruistic actors derive benefit from promoting the welfare, whereas impurely altruistic actors derive benefit from observing themselves promoting the welfare of others (Margolis, 1982). The latter motive is often referred to as the warm glow of giving (Andreoni, 1989, 1990). Although subtle, this difference in motivation suggests that purely altruistic actors are more concerned with the efficiency of their prosocial acts than impurely altruistic actors. Hence, donations to richer recipients are less appealing to purely altruistic actors than donations to poorer recipients, where the status of the recipient should not matter at all for impurely altruistic actors. This reasoning provides two conflicting hypotheses regarding the status of the recipient:
The huge literature on professional boundaries in medical settings indicates, among other things, that in-group favoritism among occupation groups is a major obstacle for efficient patient care (e.g., Burford, 2012; V Lloyd et al., 2011; Weller, 2012; Weller et al., 2014). In our study, in-group favoritism breaks down to the following hypothesis:
H1 to H5 describe various ways in which donations in the dictator game might be influenced by the status hierarchy among health professionals. However, donations in the dictator game are known to be impacted by additional variables such as sex and age, which, in turn, might be correlated with the relative status of health professionals (Engel, 2011). To at least partly deal with this problem of unobserved heterogeneity, we will include essential control variables in our multivariate analyses. Most importantly, we will control for two strong determinants of prosocial behavior, that is, (generalized) trust and the subjective utility of money. Past research has demonstrated that these two variables cast reliable effects on prosociality (e.g., De Cremer & Stouten, 2003; Irwin, 2009; Tang & Chiu, 2003; Tang & Liu, 2012). With respect to our setting, these findings suggest the following two hypotheses:
In the following, we will organize our empirical analyses around these seven hypotheses.
Results
Below, we are going to present the ways in which the professional status of donor and recipient influences the contributions in the dictator game in a descriptive manner. Subsequently, we will compare the distributions of donations by the three occupational groups. Concluding this section, the validity of our theoretical expectations will also be tested at the individual level by means of multilevel regression analysis while controlling for possibly interfering third variables.
Descriptive Results
All in all, the participants in our experiments showed behavior similar to what preceding research on dictator games let us expect (Camerer, 2003; Falk & Fischbacher, 2006). In 23.9% of the allocative decisions, nothing is given away. Most of the donations vary between 0 and 5 Euro (66.5%). Donations of more than 5 Euro are, however, rather rare (9.6%). The average donation amounts to 3.62 Euro.
However, the decisions on distribution were clearly influenced by the professional status of donor and recipient. Figure 1 states the average donation (with 95% confidence intervals) depending on the professional status of the donor (graph on the left) and alternatively depending on the occupational group of the recipient (graph on the right). Student nurses give an average of 2.54 Euro and receive an average of 4.67 Euro. The average donations increase with an increase in professional status of the donor. Physicians donate even more than half of the 10 Euro to the recipient. The occupational group of the recipient also plays a decisive part in determining the allocative decisions: With an increase in professional status comes a decrease in donations.

Average donation in EUR by members of occupational groups (left panel) and to members of occupational groups (right panel).
With reference to the status of the donor, the distributive pattern corresponds to the theoretical expectation of a positive correlation between status and prosocial behavior. Thus, our findings confirm H1 and refute H2.
Now, we turn to the question how the status of the recipient affects donations in the dictator game. Drawing upon the “warm glow of giving” assumption, we had expected that the professional status of the recipient would not have an influence on the donations. However, H4, and hence the assumption of impure altruism, is clearly refuted by our data. Moreover, we observe that actors with lower professional status receive higher donations than actors with higher professional status, just as predicted by H3 and the assumption of pure altruistic preferences. Hence, donors do not exclusively derive intrinsic benefit from observing themselves promoting the welfare of others: It also matters which value the donation has for the recipient.
The above-stated differences in average distributions between donor and recipient were tested for significance by means of t-tests. Table 2 shows that the pairwise differences in average donations given by donors of the different occupational groups, as well as the pairwise differences in the distinct amounts obtained by recipients, are all statistically significant.
Comparison of the Donations—Mean, Median, and Wilcoxon Signed-Rank Test.
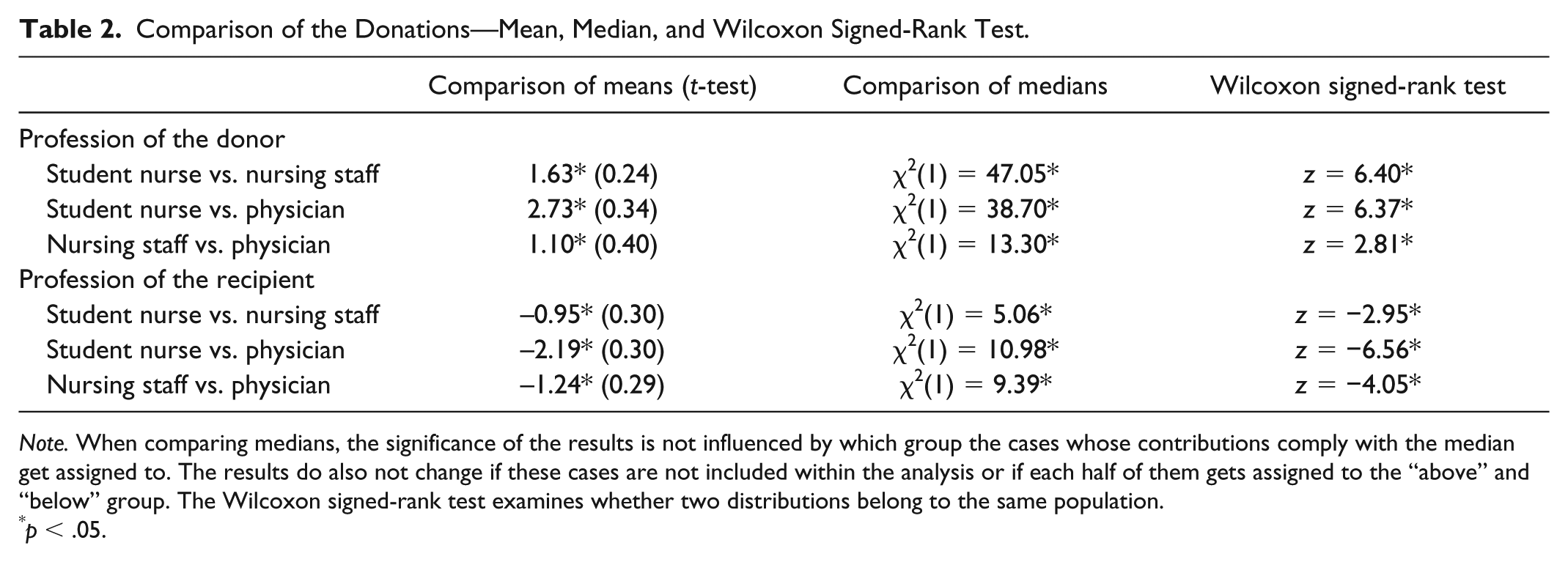
Note. When comparing medians, the significance of the results is not influenced by which group the cases whose contributions comply with the median get assigned to. The results do also not change if these cases are not included within the analysis or if each half of them gets assigned to the “above” and “below” group. The Wilcoxon signed-rank test examines whether two distributions belong to the same population.
p < .05.
Adding to that, the comparison of the medians and the Wilcoxon signed-rank test also show a significant difference in distributive decisions with respect to occupational groups in the hospital. The same applies for the influence of the recipient’s professional status on the decision of the donor.
Multivariate Analysis of Individual Allocative Decision-Making
Preceding research exhibits that both sex (Eckel & Grossman, 1998) and age (Engel, 2011) of the donor have an influence on decision-making in the dictator game. Women give on average more than men, and older participants show higher degrees of altruism than younger participants. The status variable within our study is correlated with these two sociodemographic characteristics. For example, there are a much higher number of men among physicians compared with nursing staff and student nurses. Student nurses, however, are on average much younger than nursing staff and physicians (see Table 1). In the following, we are going to present the results of a multivariate analysis that control for the confounding influence of age and sex of the donor. 3
Each participant of our study takes part in three rounds of allocative decision-making. The data are therefore hierarchically structured (i.e., three decisions per decision-maker). Whereas country-comparative or educational research usually relies on hierarchal models to analyze persons who are nested in classes, school, or countries, these models are also widely used in psychology, for example, to analyze within-person variability in psychological states (e.g., Nezlek, 2007). To take this hierarchical structure into account, we are estimating linear multilevel models for explaining the decision-making (Hox, Moerbeek, & van de Schoot, 2010; Rabe-Hesketh & Skrondal, 2012) using STATA’s (version 13) xtmixed command. Neglecting the hierarchical structure might lead to a misinterpretation of the empirical results, as especially the standard deviations might be underestimated. Estimating multilevel models allows modeling the mutual dependence of the explaining factors on the level of decision-making (especially the status of the recipient) and the explaining factors on the higher level of decision-makers (especially the status of the donor and his or her sociodemographic characteristics). From a minimum number of 50 cases on the higher level, the multilevel models provide reliable results, from a number of more than 100 cases their application is assumed to be without compunction (Maas & Hox, 2005).
We first estimate a so-called empty model (model 1; Table 3), in which no explanatory variable is included. It is used to determine how the variance between decisions is attributable to the person and how much is attributable to the decision context, that is, the recipient. The intraclass correlation (ICC) states which share of the overall variance has to be assigned to the higher group level. In our case, 44% of the overall variance is to be ascribed to the characteristics of the donor (p < .05) and the remaining 56% of the overall variance is to be ascribed to the characteristics of the decision situation. These figures support the grouping of the data and justify the application of multilevel models.
Contribution of the Dictator—Linear Multilevel Regression.
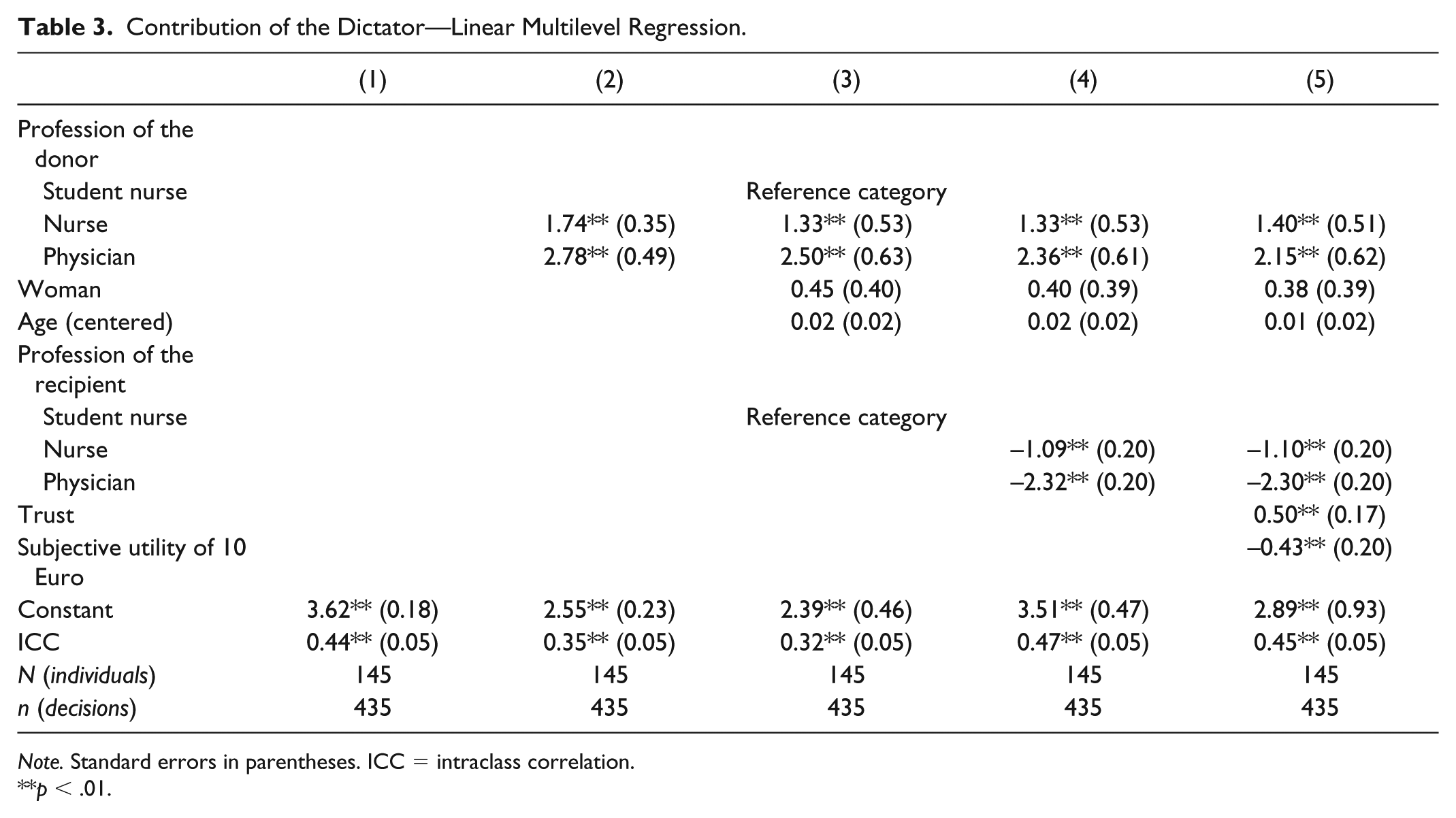
Note. Standard errors in parentheses. ICC = intraclass correlation.
**p < .01.
Which part plays the professional status of the donor for the allocative decision-making? In model 2 in Table 3, we include the occupation of the donor as an explanatory variable, and model 3 further controls for sex and age. It can be seen that a female student nurse of average age with a secondary school degree (Realschule) donates on average 2.55 Euro. The donation made by a female nurse is on average 1.74 Euro higher and a female physician gives on average 2.78 more than a student nurse, thereby donating an average of 5.33 Euro. These results are clearly lending support to H1, stating that donations are increasing with an increase in status of the donor. At the same time, we can exclude the effects of professional status of the donor to be retraceable to the age and sex of the donor. The effects of the control variables do show in the expected direction—women gave away more than men and older participants more than younger participants; yet, the effects were not statistically significant, which might be due to the small number of cases and the limited variance of the age variable. More than that, the change in estimated status differences that occurred between models 2 and 3 suggests that a part of the professional status effects that had originally been observed is related to differences in sex and age. Thus, for example, the difference between the (predominantly male) physicians and the (predominantly female) student nurses increases when controlling for the differences in sex and when acknowledging that men give generally less than women.
In model 4, we examine whether the occupational group of the recipient has an influence on the amounts that the donors give away. The professional status of the recipient is the only information on the level of the decision situation that we can use for explaining the differences in donations. However, it has to be considered that the professional status of the recipient is also the only objective difference between the decision situations.
As the descriptive results already suggested, we find that the occupation of the recipient does play a decisive part in determining donations. A member of the nursing staff receives on average 1.09 Euro less than a student nurse and physicians receive on average even 2.32 Euro less than student nurses. These findings thereby refute H4 and rather support the assumption of pure altruism (H3).
We have also theorized on potential in-group favoritism, that is, donors give more to members of their own professional group compared with members of other professional groups. However, the study at hand does only find little evidence in support of H5. 4 Student nurses do indeed give more to other student nurses than to nursing staff or physicians and also members of the nursing staff give more to other nurses than to physicians. This favoritism of the own group toward another group can, however, only be observed when the professional status of the other group is higher than the professional status of the own group. In allocative decision situations with recipients of lower status, all the donors give more to the out-group than to members of their in-group. The empirical evidence that would speak in favor of an in-group bias thereby overlaps with the predictions of the pure altruism hypothesis. As pure altruism moreover gives a correct forecast of the allocations that contradict in-group favoritism, we consider pure altruism to be the more suitable explanation for the distributive decision-making observed in our study.
Finally, model 5 includes two additional control variables, that is, trust and the subjective utility of money. Trust is measured with a commonly used 5-point scale ranging from 1 (You can’t be too careful) to 5 (Most people can be trusted). In addition, we measure the subjective utility a respondent attaches to 10 Euro. Respondents were asked to imagine that they would lose 10 Euro and should then rate how badly they would be affected by such a loss on a 4-point scale. We recoded the variable so that higher values mean a higher subjective utility of 10 Euro. Our results replicate the commonly observed effects of generalized trust and the utility of money on prosocial behavior (H6 and H7). More importantly, because the coefficients for the status variables do not differ considerably between models 4 and 5, we find that the effects of the status hierarchy among health professionals on giving in the dictator game are not primarily due to differences in generalized trust and the subjective utility of money.
Concluding Remarks
Past research has revealed that patient care and favorable outcomes of medical treatments crucially depend on the social interaction among health professionals. In particular, two obstacles for effective teamwork in medical settings have been discussed in the literature. First, members of different occupational groups such as physicians or nurses might primarily identify with their own group, thereby hindering the development of team identity and promoting in-group favoritism. Second, if strict status hierarchies are enforced by high-status actors such as physicians, actors with lower professional status such as nurses might be deterred from contributing their expertise in an open and efficient manner.
Against this background, we conducted an experimental study that aims at studying prosocial motivations among health professionals and at revealing potential in-group favoritism. Our results are clear-cut. We find that all professional groups under consideration, that is, physicians, nurses, and student nurses, show a considerable amount of prosocial preferences. Moreover, the altruistic concern for the welfare of others is rather pure than impure in the sense that actors in health care indeed have an intrinsic interest in the well-being of their coworkers and are not merely motivated by the warm glow of giving. Also, these prosocial motives are not at all restricted to other actors of equal professional status, but reach across professional boundaries, that is, we find no evidence for in-group favoritism. Although physicians, nurses, and student nurses do take the professional status of their interaction partner in account, they give more to those having less. Also, actors with higher social standing donate significantly more than low-status actors. Both the effect of the status of the donor and the effect of the professional status of the recipient point rather toward counterbalancing than toward reinforcing status hierarchies.
Taken together, these observations shed a rather benign light on the social interaction among health professionals. Certainly, teamwork in medical settings is ripe with problematic social situations, that is, dilemmas in which what is best for the individual is in partial conflict with what is best for the team as whole and, hence, patient care. Still, the absence of in-group favoritism and the prevalence of pure altruistic motivations among health professionals suggest that essential preconditions for overcoming these obstacles for effective teamwork in terms of human and social capital are met.
As a side note, we want to stress that our findings are also informative for the literature on the relationship between social class and prosocial behavior. Our results are generally in line with previous work by Korndörfer et al. (2015), Liebe and Tutić (2010), and Bekkers (2007, 2010), who found a positive effect of class on prosociality and are in stark contrast to the findings by Piff et al. (2010; Piff et al., 2012), which point toward a negative effect of class on prosocial behavior. Against the background of conflicting evidences, it is important to demonstrate the robustness of findings across a wide variety of social settings, and our study does so by shedding light on the important social realm of health professionals.
Practitioners and others might now possibly argue that our results are of rather limited interest, because it remains somewhat unclear how altruistic behavior in dictator games relates to cooperative behavior in real-life medical settings. Granted, in comparison with studies observing in much detail the everyday practice of social interaction among medical professionals, our approach of using artificial interaction situations seems rather detached from social reality. However, from our point of view, these approaches should not be seen as substitutes but as complements. We certainly do not argue that more traditional and in particular qualitative research on the relationship between nurses and physicians should be abandoned in favor of our experimental research strategy. However, we advocate further experimental studies to facilitate our understanding of the social interaction among health professionals for at least two reasons. First, although artificial decision situations like the dictator game might seem overly simplistic, these games capture the very gist of real-life interaction situations. Also, many forms of real-life interaction that prima facie appear to have only little in common often share the same incentive structure at their core. Hence, abstracting from the details of social reality allows unveiling the common core of seemingly unrelated forms of interaction and thereby promotes our understanding of the medical field. Second, using experimental tools such as dictator game to study the interaction among health professionals integrates the specialized literature on health professions in the broader canon on interdisciplinary action theory and prosociality. This way, theoretical ideas such as pure and impure altruism as well as stylized facts from other social settings such as status effects become readily applicable to the study of the interaction among health professions.
We would like to stress again that we did not directly measure teamwork and communication behavior. Future research could apply experiments with the same, but also different, occupational status groups and employ team and communication tasks. This will help to understand and explain under which conditions and to what extent prosocial behavior across professional boundaries will directly have positive impacts on teamwork and communication across professions. Future research might also benefit from replicating our study in different medical contexts. Albeit we have carried out our experiments in different hospitals, it has to be shown how generalizable our findings are and whether they depend on characteristics of the hospitals (e.g., size of hospitals, specialization, and cultural context). Furthermore, our approach can also be applied within hospitals using the sociometric status of professionals as a reference. In addition to the “objective” professional status of each participant, it can be studied how the informal status of participants (e.g., measured by social approval of co-workers) determines prosocial behavior and cooperation. We hope that our study paves the way for further experimental research in this direction. Such experimental studies can help to uncover the interplay between social status and prosociality in medical (field) settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.