
Abstract
Family caregivers are the main source of support for survivors of traumatic brain injury (TBI) while they transition from pediatric to adult care service and support systems. Yet there is little research that examines the needs of these caregivers during the transition phase. The aim of this qualitative phenomenological study was to examine the lived experiences of family caregivers of young adults with TBI who had recently transitioned from services for children and adolescents to adult care service and supports. The study sample comprised 15 family caregivers of young adult TBI survivors who had transitioned to adult services in the last 5 years. They were recruited from two large hospitals and a caregiver support center in a city in Western Canada. Semistructured interviews were conducted with the caregivers and the data were analyzed using Colaizzi’s approach in developing an essential structure of the phenomenon of caregiving. Fifteen themes emerged from the analysis and these are discussed under two broad domains: (a) caregivers’ experiences and challenges with their relative at the time of transition; (b) caregivers’ challenges with services and supports systems during transition. Findings suggest that there is a wide gap between what caregivers need and what is available to them to support their young adult relative through the transition process and beyond. Most caregivers reported that the transition phase is overwhelming and has a profound and pervasive impact on their lives. Implications of the findings and recommendations for policy and practice are discussed.
Introduction
Traumatic brain injury (TBI), which is an injury to the brain caused by an external force, is one of the leading causes of death and disability throughout the world. Every year in Canada alone, 11,000 people die from a TBI, and as many as 6,000 persons experience permanent disability due to this condition (Alberta Centre for Injury Control and Research [ACICR], 2014). TBI occurs across all age groups, but those most at risk of sustaining TBI are young males between 15 and 24 years, followed by individuals between 5 and 14 years (Franulic, Carbonell, Pinto, & Sepulveda, 2004). The range of impairments following TBI is contingent on the nature and severity of the injury. This is classified in terms of mild, moderate, or severe depending on the depth and length of the coma and the duration of posttraumatic amnesia (Finfer & Cohen, 2001). Depending on the nature and severity, TBI can affect the injured individual’s cognition, behavior, and emotional states to varying degrees (Wilde et al., 2012). Cognitive losses can affect memory, visual perception, attention, concentration, information processing, problem solving, abstract reasoning, planning, information processing, and organization (Mrazik & Sattler, 2014). Physical effects may include visual deficits, dizziness, balance problems, fatigue, bowel and bladder dysfunction, seizures, and sensory impairment (Lezak, 1995). Psychosocial changes following TBI can impact both behavior (e.g., poor self-awareness, impulsivity, agitation) and personality (e.g., dependency and low self-esteem; Cunningham et al., 1999). Mental health difficulties following TBI may include depression and anxiety. Substance abuse, particularly common among young TBI survivors, can exacerbate symptoms of depression and anxiety, increase suicide risk, compromise compliance with treatment regime, and/or reduce the effectiveness of prescribed medication (deGuise et al., 2008).
Caregiving for Young Adults With TBI
The changes following TBI have a significant impact on close family caregivers, especially parents who are often thrust into this role without adequate training, information, and support (Albert, Im, Brenner, Smith, & Waxman, 2002; Gagnon, Swaine, Champagne, & Lefebvre, 2008). Several studies have demonstrated the presence of subjective burden and emotional distress (i.e., clinically significant levels of anxiety and depression) among family caregivers, including during the transition from hospital to home (Kreutzer, Rapport et al., 2009; Livingston et al., 2010; Turner, Fleming, Ownsworth, & Cornwell, 2010). In addition, family caregivers can experience social changes that include shifts in their roles, relationships, financial situation, and social interaction (Fraser, 1999; Kolakowsky-Hayner, Miner, & Kreutzer, 2001).
The World Health Organization has identified the needs of children and youth who have experienced TBI as a priority area for research (Carroll, Cassidy, Holm, Kraus, & Coronado, 2004; Hung et al., 2014). Because their needs may be spread over several years and are contingent on several factors—age, cognitive assets, and motivational factors of the survivor—close family may be involved in caregiving for a long time. Several recent studies have examined the needs of TBI survivors and their family caregivers at different phases during the recovery process, referred to as “transition.” Transition is viewed as “an ongoing process of change in the health status of individuals with TBI, their role relations and expectations, and in the caregiving capacity of close relatives who live with these individuals” (Engström & Söderberg, 2011, p. 253). Past studies have examined the transitions of individuals with TBI from different perspectives and contexts: (a) transitions in patterns of daily life, (b) transitions in relationship, and (c) transitions in social life (Engström & Söderberg, 2011, p. 253). Nalder, Fleming, Cornwell, and Foster (2012) examined the transition process from the hospital to the home of individuals following a TBI. However, there is limited research that has examined the transition of TBI survivors from pediatric to adult health care and community services. With increasing numbers of young people with TBI surviving into adulthood, there is an urgent need for more research that focuses specifically on this transition, especially in Canada where empirical studies specific to this transition are scarce. Transition in this context is defined as “a purposeful, planned process that addresses the medical, psychosocial and educational/vocational needs of adolescents and young adults with chronic physical and medical conditions as they move from child-centered to adult-oriented healthcare systems” (Blum, Garell, Hodgman, & Slap, 1993 p. 570). A report, “Getting it right for young people” (Child Health and Maternity Services Branch [CHMSB], 2006) highlights that young TBI survivors are among the least well-served groups after they leave the pediatric system of care. Resources for rehabilitation and reintegration into the community are scarce for this group, and there is a lack of a management protocol for dealing with transition (Lefebvre, Pelchat, Swaine, Gelinas, & Levert, 2005). Young people with TBI often have multiple problems and require support from specialists from several disciplines and sectors, including medical, educational, vocational, and social (Wade, Zhang, Yeates, Stancin, & Taylor, 2016). Often it is difficult to identify anyone willing to take on the task of coordinating the medical care as well as disability, vocational, and financial supports and advise these young people and their caregivers on what they need and where such resources can be found. Yet it is known that depending on the severity of TBI and subject to the availability of appropriate rehabilitation and professional support, young people with TBI can make significant rehabilitation gains such as returning to work and study and living independently (Shames, Treger, Ring, & Giaquinto, 2007).
Family caregivers are the main source of support for TBI survivors during the transition phase, particularly when the young person lacks the maturity or cognitive ability to cope with complicated information. In the absence of a coordinated transition plan that involves a multidisciplinary and multiagency team approach and a single-entry point for information, it is important to know how family caregivers access needed services and supports, identify and access practical information, and develop rapport with health care, disability, vocational, and other support systems. It is also equally important to assess caregivers’ capacity to provide the support and how they address their own health and well-being during the transition process.
Research Question
To address these pressing questions and knowledge gaps, the current study examined the experiences and challenges of family caregivers whose relative with TBI has transitioned from pediatric to adult care services. The research question was as follows
Method
The methodology most suitable to address the research question is a qualitative design informed by descriptive phenomenology. This approach is uniquely suited to studies on life experience and enables description of an experience in terms of “what” they experienced and “how” they experienced it (Husserl, 1913/1962; Moustakas, 1994). In the context of the current research, this approach would allow for an in-depth descriptive analysis of the lived experiences of caregivers, as they moved through the transition process in terms of the challenges they faced, the contexts and conditions surrounding their challenges, and their coping and resilience through the process (Creswell, 2007). In a descriptive phenomenological approach, the assumptions require that the essence of an experience be captured without influence from the researchers. To achieve this, bracketing is used to hold ideas, preconceptions, and personal knowledge in abeyance when listening and reflecting on the experiences of participants (Moustakas, 1994).
Participants
Using a purposive sampling strategy, 15 family caregiver participants were selected from two large hospitals and a caregiver support center in a city in Western Canada. The caregiver had to have a child who (a) had suffered a TBI in childhood or adolescence and (b) had undergone transition from pediatric to adult health and community care settings within the past 5 years. Consultation with our community partners confirmed that transition is a multistage process that begins approximately at the age of 16 years or earlier and is contingent on planning initiated by the family, and health care and community services personnel. Throughout this process, the transfer to health and/or community support services (vocational and educational, legal, etc.) may occur at different ages. Transition planning for school, community services, and funding shifts begins around the age of 17 years. The age at which youth are discharged from pediatric care is generally 18 years old. The age at which the entire transition process is expected to be completed is around 21 years. The following strategies were used to recruit family caregivers: (a) study information material was disseminated via designated team leaders at the three sites; (b) notices about the study were posted at various locations within these centers; and (c) study presentations were offered to service personnel at the three centers to increase their awareness about the study and help with recruitment of potential participants.
A semistructured interview guide, developed in consultation with team members who had expertise in the areas of brain injury and transition, was used for data collection. There were two key areas of enquiry: (a) Family caregivers’ perceptions of the difficulties experienced by the young adult TBI survivor during transition from pediatric to adult care services and the resulting challenges for family caregivers; (b) the experiences of family caregivers with services and support systems during transition and the supports they need. Examples of questions included caregivers’ perception of injury; their child’s strengths and challenges; level of care needed; kinds of supports and services their child needed from various service providers; barriers and facilitators during transition; caregivers’ experience of helping their child to transition; their recommendations for improving support during transition; the caregiver’s needs and where they are in their life as a caregiver.
The interviews commenced after ethics approval was obtained from the University Research Ethics Board. Prior to the interview, participants were provided with information about the study and their informed written consent was obtained. In depth interviews were conducted by the first author and a trained research assistant. All interviews were audio-recorded with the permission of the participant and transcribed verbatim for data accuracy. Each interview lasted for about 120 min. To ensure that bracketing was achieved, the researchers used field notes and a diary (Wall, Glenn, Mitchinson, & Poole, 2004) throughout all stages of the study: data collection, analysis, and writing. Rigor, in terms of data collection and analysis, was ensured through member-checking, peer checking for reliability of coding, and maintaining an audit trail.
Data Analysis
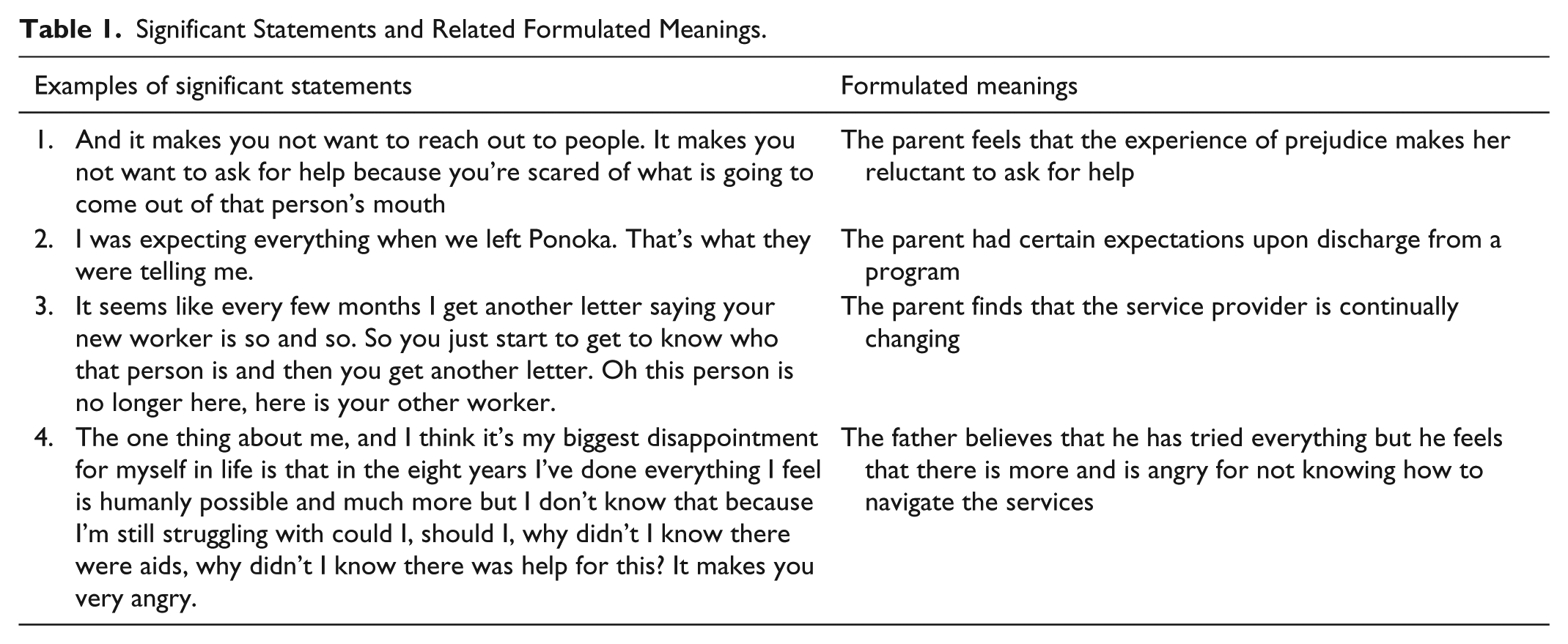
Interviews were analyzed using Colaizzi’s (1978) method which provides a structured and systematic account of the procedural steps involved in the analysis of phenomenological data. This method can increase the confirmability and dependability of the results. In keeping with this approach, the following steps were followed: (a) Each transcript was read at least 2 times by the first author and a research assistant to familiarize themselves and identify some themes; (b) significant statements from each transcript that pertained directly to the lived experiences of the caregiver were identified; (c) meanings were formulated from each of the significant statements; (d) formulated meanings were organized into clusters and themes were created from them; (e) the clusters and themes were used to exhaustively describe the caregiving experience. The analysis brought to light 85 significant statements and 50 formulated meanings from which 15 theme clusters emerged. As a final step, the first author and the research assistant approached nine participants a second time to validate the findings. Table 1 gives examples of significant statements and related formulated meanings. Table 2 provides two examples of theme clusters that emerged from their associated meanings.
Significant Statements and Related Formulated Meanings.
Examples of Theme Clusters.

Note. TBI = traumatic brain injury.
Results
Except for one caregiver father and a female sibling caregiver, most of the participants were mothers. One caregiver was from an indigenous background and two caregivers were immigrants from the Middle East. The latter could communicate well in English. All other caregivers were Caucasian. The caregivers were in the 45 to 65 age group except for the sibling caregiver who was 25 years old. Most of the caregivers worked part-time and had made changes to their work schedules and career goals to accommodate their caregiving responsibilities. In the case of the TBI survivors receiving care, 13 had experienced severe TBI and three had experienced moderate TBI as reported by their health care providers who referred the participants to the study. At the time of injury, five survivors were in the 10 to 12 age group, five were in the 13 to 15 age group, and six were in the 16 to 18 age group. At the time of the caregiver interviews, all the 16 TBI survivors were in the 18 to 25 age group. Nine TBI survivors had transitioned within 5 years to adult support services, two had just crossed 5 years, and 5 had transitioned in the previous year. The two survivors who had just crossed the 5-year eligibility mark were included as their hospital files were open and they were still accessing some services. As stated earlier, although the age at which youth are discharged from pediatric care is generally 18 years, the age at which the entire transition process is expected to be completed is around 21 years. Table 3 provides a list of the themes that emerged from the analysis of the qualitative interviews with the number of interviews where each theme was observed. The themes are discussed under two broad domains: (a) parents’ experiences and challenges with their child at the time of transition; (b) parents’ challenges with services and supports systems during transition.
Theme List With Number of Interviews Relating to Each.

Note. TBI = traumatic brain injury.
Parents’ Experiences and Challenges With Their Child at the Time of Transition
Theme 1. Challenges for parents during transition arising from TBI survivor’s sensory, physical, and cognitive limitations
Many of the TBI survivors at the time of transition to adult care services experienced ongoing sensory, physical, and cognitive limitations and were dependent on their parents for various kinds of support. A mother reported that her young adult child had lost his sense of smell and taste while another said that her child had become blind since the accident and was fully dependent on her for care. One young survivor could manage only simple self-care tasks such as preparing easy foods like cereal or hot chocolate and depended on his parent to prepare his meals. Some survivors experienced difficulties with dexterity and balance. As described by a mother, “Her hand locks up all the time so grabbing onto things or writing is very difficult for her.” Others could no longer participate in sports or drive after the accident. Some parents had observed that their child tired very fast. One parent stated that her daughter’s energy level was only adequate for half a day and this had a significant impact on her capacity to study. This parent expressed concerns that her daughter would experience a setback in her recovery because she did not recognize signs of fatigue. The limitations in their young adult child’s abilities imposed heavy demands on parents. Among other roles and activities, they had to drive their child for medical appointments, and/or social and recreation activities, be constantly vigilant so that their child did not have another accident and monitor their child’s daily schedule to ensure that they did not get excessively tired.
Many TBI survivors also experienced ongoing cognitive difficulties. These included difficulties like remembering past incidents or the timing of events, including the memory of the accident, forgetting a recent discussion, following a conversation, concentrating and completing tasks on their own. One parent shared that her daughter could plan but had difficulty matching her plans with subsequent behaviors. This parent was having trouble convincing her daughter that many of her behaviors did not match her plans and were detrimental to her well-being. Another parent said that he could not get his daughter to plan for anything because she did not see “that far” and had difficulties with memory. In his words, “I cannot get her to try and get better today based on something that happened yesterday because quite often, she did not remember yesterday.”
Theme 2. Challenges for parents during transition arising from personality changes in survivor
Parents had noted personality changes in their children following the TBI, some of which were positive while others negative. Parents expressed pride when discussing the positive personality changes. Some young survivors who had been shy and withdrawn prior to the accident had become outgoing and outspoken. As described by one parent, “She never stood up for herself before. If she wasn’t happy with something, she’d stay quiet . . . Now if she doesn’t like something, she’s more than willing to tell you.” Another parent, whose son had made a remarkable recovery, highlighted how her son’s accident and subsequent dealing with being bullied by peers in school resulted in him becoming a public speaker: “X could never get up in a group of people. Then when he had his accident, he started speaking. The way he explains it, it’s his new adrenaline rush.” Another parent had noticed that his daughter had become more compassionate and sensitive toward others, especially those with a disability and showed much more gratitude for the things people did for her and the efforts they made to help her.
The negative personality changes included loss of motivation, mood swings, bouts of anger/rage and irritability, making inappropriate comments and loss of interest in maintaining proper hygiene. A mother explained how her son, despite attending counseling sessions, gets easily frustrated, anxious, and irritable and would suddenly leave or go to bed when they had visitors, even if they comprised only extended family and close friends. Reflecting on her daughter’s motivation and mood before and after the accident, one mother noted, Because of how much we built up that year. She’s been on the cheer team for two years. This was going to be her final year. She was going to graduate with her friends. She was really, really excited about that year. Then it was . . . as she puts it, “It was taken from me mom.” It feels like that’s all she concentrates on. It was taken from her. She doesn’t have a second chance is what’s going through her head right now. She doesn’t want to be 21 and graduate.
Theme 3. Caregivers’ dilemma over changes
While the positive personality changes in their child were encouraging to all parents, they were also in a dilemma because they could not make sense of their child’s splintered functioning. For example, the parent whose daughter showed much compassion and sensitivity toward others after the accident could not understand why his daughter’s moods were like “bipolar illness,” and why she displayed “extremely negative attention seeking behaviors,” especially with him or why she was sometimes disrespectful toward some people. He was having a difficult time discerning if his daughter was “sometimes pretending to play stupid just to get him.” The mother whose daughter had become very outspoken and bold after the injury could not understand why she had lost all her motivation and drive to achieve her goals after the accident. Parents wondered if the changes in emotions and loss of motivation, negative perceptions, and unresolved feelings were related to the accident. They were unsure if the changes in their child’s functioning were the result of TBI or part of the normal developmental process of moving from adolescence into adulthood. Another parent wondered if her son’s episodes of raging anger were a “developmental problem or a personality problem or rather an after effect of the accident.”
Theme 4. Parent’s experiences of interactions with their adult child and shifts in family relationships
Parents’ experiences of their interactions with their young adult child during transition were mixed. Some parents perceived that their child had become emotionally distant with them. As expressed by one parent, “he used to always hug—So now I have to tell him, come give me a hug, and then he will.” One parent shared that, unlike before when she could discuss anything openly with her daughter and at any time, she now had to pick a time because her daughter had become distant and very moody. She shared, “it seems there is a line my daughter has drawn that I cannot cross.” Some survivors had developed stronger bonds with their parents after the accident and needed the parent’s support and approval for everything they did because they lacked confidence in their abilities. These parents shared that the strong bond and trust their child had in them was an important factor in their journey of recovery, which was not easy for the parent or their adult child. As explained by a mother who had experienced very difficult times after her daughter’s accident, With her I am very involved right. She kind of demands that I am-you are the kind of go to gal and she does need support, especially emotional support and reinforcement that she is doing the right thing and things like that-she’s got self esteem and confidence issues. I think we would have been close anyways but definitely it (the accident) made it closer just because of the what we’ve been through. There were times where you know we had struggles-in our relationship especially when she was on the street. But if I did not maintain or hadn’t maintained a close relationship, I am not sure where she would be. It was a necessity for her survival.
In some cases, the closeness that the TBI survivor previously shared with other family members, especially siblings, was affected. While some siblings understood why their parents needed to give extra attention and support to their TBI relative, others did not. One parent who was caught in such a situation shared, “They think (Y) is special to me, she’s more special because of the accident, and I give her freedom because of the accident, I worry about her.” They became hostile toward their sibling and angry with the parent and in some cases distanced themselves from their sibling with TBI. Some of these parents blamed themselves for this situation. In one case, a younger sibling had taken to drugs and bad company and the mother expressed that this was because much of her time was spent meeting the needs of her older son with TBI.
Theme 5. Concerns about loss of peer relationships
Parents noted that TBI had significantly impacted their child’s peer relationships. In many cases, school mates who were close friends with the TBI survivor before the injury had drifted away because the survivor found it difficult to either communicate with them or share similar interests. One extremely distressed parent shared, “When it comes to former friends coming over, she’s not ready because she feels out of place because of her scars, because she can’t walk as well as they can, she can’t run like they can.” Another parent shared that the new friends her daughter made at school were superficial relationships unlike her previous ones. In one case, the survivor was attending social programs but they were with people much older than herself. Some parents expressed concerns that the loss of peer friendships had resulted in their child “taking to social media and becoming a ‘facebook-a-holic,’ texting all the time” as a way of coping with social isolation, while others were worried that their child could engage in negative and/or abusive relationships to compensate for the loss of intimate relationships and peer networks. As expressed by the parent of a 22-year-old TBI survivor, Two of her three (ex-boyfriends) have ended up with restraining orders. One actually-took her for about $4,000 cash. So, you know she’s not a good judge of characters. My fear is people easily take advantage of her. Again, it’s because she wants to be loved. She wants to be with someone and it’s very tough.
Parents wanted their child to develop close and lasting relationships that extend beyond “mom and dad.” Many were worried that not having other supportive and safe relationships would leave their child without any support when they were away at work or no longer able to offer care due to parental aging, illness, or death. In keeping with these concerns, some parents were proactively engaged in setting up peer networks for their child.
Theme 6: Working proactively with their child
Many parents were also working alongside their adult child to help them achieve other goals like learning to be responsible, maintaining safety, recognizing and managing fatigue, managing money, and learning to live independently. This was a demanding process that called for much patience and perseverance. Parents had to be attentive to their child’s needs, find resources that can help, provide encouragement, know when and how to push their child, while also managing their own frustrations and anxieties when their child was falling behind or making mistakes. The following excerpt illustrates a mother’s efforts and determination to help her 22-year-old son relearn the skills needed to be independent and the strategy she used: I am not gonna get him to fall behind, and I am not expecting him to be at the same level as everyone else. I get that, and I expect that, but at the same time, I want to push him so that he doesn’t fall behind. I want him to get somewhere. I have taken him to WW ( Mall), and we shop, and I pretend to be lost, don’t know what entrance to go in, and he has no idea. I tell him, you gotta watch those numbers you gotta remember, to try to get him to remember.
In summary, most parents at the time of transition were providing various kinds and levels of instrumental, psychological, emotional, and confidante support to their adult child and were using several strategies to help them become more independent. While a few parents were happy with the progress their child had achieved, others were aware that recovery from TBI can be long and arduous process.
Parents’ Experiences and Challenges With Services and Supports Systems at the Time of Transition
Theme 7. Expectations versus reality
Most parents reported that the transition from childhood to adult care services was uncertain and overwhelming. They used various phrases to describe their transition experience: “Confusing,” “lost and not knowing what to do,” “frustrating,” “left in the dark,” and “scared with a pit feeling in the stomach.” Parents needed professional advice and support to deal with their child’s psychological, emotional, and behavioral difficulties and cognitive limitations. Many parents were aware of the kinds of support their child needed for their ongoing recovery and transition into a stage of less dependence on them. But getting information about these and navigating through the maze of adult care services and their eligibility criteria were daunting tasks for several reasons discussed in the following sections.
In many cases after discharge from pediatric services, parents were expecting a service provider to provide follow-up support for their child but no one did. One parent who had taken time off work to provide full-time care for her daughter recalled, “I was expecting help. I was expecting to be back at work by now. It’s difficult. [Our daughter] was expecting to be active, not just nonchalantly walking around.” Another parent reported feeling totally isolated and lost. She shared, “I was kinda scared- wow, what am I going to do, what if something comes up.” Some parents had not received any information about services and supports they could access for their child after discharge from pediatric services. Those who had received some information at the time of discharge reported feeling overwhelmed. One of these parents recalled, “I received a lot of literature about TBI, but it was kind of all thrown at us, we have a big binder six inches thick and you know, where do you even start.” Another parent shared, “You just go with the flow and I don’t know how much I actually took in to keep it in my brain to say, Oh okay that’s what the services, I’ll go back and use that now. It doesn’t really go in you know? When she got out of the (hospital) I kind of felt like I was left holding the bag—do you know what I mean?”
Theme 8. Difficulty getting information about available services
Parents had a lot of questions about what services were available and which ones would be suitable for their child but were uncertain about where they could get this information. They were ill prepared for the reality of interacting with the adult care service systems. The following excerpt describes the frustrations experienced by one of these parents: I was upset, she’s in my mind, she’s my daughter, but I don’t know where to go. I keep asking for help, but nobody gives me a hand. At times, it was very frustrating—kind of like I was left in the dark and I was left to figure things out on my own from time to time. I had to ask a lot of the questions. I had to look for the information—honestly, I think it should be a given.
Some parents reported feeling pushed around from one service to another in their attempts to find answers to the questions they had: “They keep pushing me to somebody else . . . It’s constant . . . by the time I get thousands of answering machines, no call backs. I got a lot of no’s, a lot of doors close, “No we don’t have that.” Why do you have it in your pamphlet? Why are you offering services you do not have?” Parents needed answers to specific questions from service providers, but these either took too long or were inaccurate and not useful. One parent shared that general practitioners lacked the knowledge and expertise to deal with young adults with severe and multiple TBI-related disabilities like her son, who “needed a team approach and access to home care services on discharge from the pediatric environment, something that most families did not know.” Parents wanted honest answers from service providers about what their child could or could not do and whether their child would be eligible for certain services. But service providers would talk around the issue. As described by one parent, Well if they don’t know, please say I don’t know. Don’t give me a story to make it look good. Then I can move on and ask somebody who does know. It’s frustrating. It’s the same thing over and over and over.
One caregiver father who had struggled for 8 years to find suitable services for his daughter expressed his frustration and anger toward the service system in the following terms: The one thing about me, and I think it’s my biggest disappointment for myself in life is that in the eight years I’ve done everything I feel is humanly possible and much more but I don’t know that because I’m still struggling with could I, should I, why didn’t I know there were aids, why didn’t I know there was help for this? It makes you very angry. I’m angry at the government. I’m angry at the hospital. I’m angry that no doctor ever said “you have the ability to get an aide.” I know that’s not their place but when I look at some of the things that we’re talking about here around the change in her, those are the things because the reading, the social behaviors, the anger management, those are things that for any brain injured person, I think you’re going to have to have something in place for.
Theme 9. Conflicting information
A dilemma that some parents and their child faced was conflicting information from service providers of different disciplines about what their child could and could not do. One of these parents shared, I had to confront both [service providers] to figure out which . . . PT and OT to see which one was giving him false information. They had to clear it up with him that according to his body, yes he could play hockey in September-The one that works with the brain told him, “No you cannot play hockey in September because of your brain injury.” Once that was clarified, then it kind of sunk his will a little bit I guess, his will power.
Theme 10. Frequent changes in service providers and loss of continuity of information
Another source of frustration was frequent changes in service providers. Parents reported that often when their child had just started to settle down with one service provider, they would get a letter from the service agency that their child had been assigned a new worker and this happened every few months. While investing in a new relationship was often a challenge for many TBI survivors, another consequence of this frequent change in service providers was loss of continuity of information. One parent shared that to avoid repeating information to the next service provider and loss of information, she made sure that all the paperwork and reports on her daughter were available and transferred to the new service provider for review.
Theme 11. Racism and discrimination
One parent from an indigenous background shared her experiences of racism, discrimination, lack of respect, and unfairness from some service providers when she tried to obtain services for her daughter. She felt treated so poorly that she was reluctant to seek any further help. The following excerpt summarizes her experience: I’ve been judged because I’m Native. That’s not fair. I’ve been told that to my face. “Because you are Native, I can’t help you.” “Why can’t you?” “Because you don’t qualify.” “Why don’t I qualify? I’m human. She’s human.” It’s just the way it is—Just because I’m Native, I didn’t qualify for a lot of things: housing, clothing, food. Certain things that you do every day I could not get when I first got back to [the city].
Theme 12. Parents taking over service provider roles
Frustrated with the poor response from service providers, some parents took it upon themselves to look for services using their own knowledge and resources. One parent who had given up work to look after her child with TBI explained that she started reaching out to contacts she had established while working in the disability sector as an employment counselor. Another parent had contacted several employers in her area to give her son an opportunity to work in their organization. Finally, she was successful in finding a sympathetic employer who agreed to offer a few hours work for him. The lack of services for young adults with TBI led one parent to comment that the service system lacked awareness of the kinds of services young adult children with TBI need for their ongoing recovery. Parents reported that they had to actively advocate and sometimes “fight to receive services for their child.” Some parents had to apply multiple times to get disability income support for their child because their child was deemed “not disabled enough.” One parent had to fight for disability support services for her child: We found once he transitioned into the adult, we had to fight for PDD (disability support services) and we were denied the first time, so we had to appeal and go to a mediator. We were denied again so we had to go into full mediation.
Likewise, another parent had to fight with hospital service providers for a letter that would allow her son to access ongoing medical support from his own family doctor. Parents shared that fighting for support services was often demeaning because it involved constantly acknowledging their child’s incapacity.
Theme 13. Some good experiences
A few parents described good experiences with some service providers. One parent described how some service providers had gone out of their way to help her daughter. The following excerpt highlights a caregiver’s experience of how one service provider went “beyond her own responsibilities” to ensure appropriate care for the child. In the words of this parent, {X} was like you know going down all kinds of bad paths but like I said, the psychologist who was the one who found us {K }(source of support) all-so I’m forever grateful for that, she did take it upon herself without me asking her to try and find somewhere for {X} to go and called me afterwards and said, “Hey this is a place I think.” It turned out to be the place just the best place and yeah- it is a spectacular.
Theme 14. Caregiving during transition is filled with multiple roles and is demanding on parents’ health and well-being
Parents reported that the multiple tasks they had to undertake during the transition phase took a heavy toll on their physical, psychological, and emotional resources. Parents whose child had suffered a TBI in their late teens were still dealing with their own and their family’s grief from the recent accident. One such parent shared, “it was difficult and frustrating, especially because we were still in the process of healing. That made it even more difficult because he hadn’t plateaued yet. He was still on a slow, gradual climb to healing.” For another parent, the impact of her child’s injury was so overwhelming that it prevented her from going in search of information that was needed for her daughter’s recovery. Many parents were unable to attend to their own and their family’s needs. One parent shared, Exactly, all these appointments, all this stuff, who’s got time?-you know, constantly, I have to get stuff ready for appointments, I gotta make sure he’s got everything he needs . . . You’re so busy thinking and doing, you don’t have time to think, Darn it, I should have been making supper, ok we’re gonna have to eat out, or grab something up on the way. So you’re not properly eating and it happens it seems more so, now that I’m working, because I don’t have time to cook and if he’s got an appointment whatever, and I have to come home early for it, . . .
Another parent could not sleep and “kept tossing and turning” and felt that there was “no downtime for her brain” because of continuous thoughts of where she could go or who she should contact or talk to so that her son could get part-time work. For many parents, their own needs for self care had become secondary. One parent talked about caregiver burnout in the following terms: Burnout, caregiver burnout is such a big, big, big, thing. I don’t know . . . as parents we burn out but yet we don’t call it burnout you know. We are raising our children. We don’t say parental burnout. You don’t say it when you’re a parent but you do burn out more so because you’re totally responsible for that person.
Many parents were exhausted and asserted the importance of relaxing to fulfill their role as a caregiver. However, finding time to relax was difficult. Aside from physical exhaustion, the caregiving process had affected the mental health of parents. Many attested to be living in a perpetual state of anxiety because of fears that something could happen to their child. One parent described her condition as follows: I could not do it. I suffer panic attacks, huge anxiety attacks. I don’t know how to get through them half the time. I have migraine headaches every third day. I honestly feel like my body is shutting down on me with all the stress and stuff I’m going through.
Some parents suffered from unresolved feelings of self blame and guilt. One parent whose daughter had suffered the injury in her late teens expressed how the whole experience had completely changed her, had left her “hurt, angry, closed in and socially isolated.” She did not feel like talking to friends anymore, going out, and wanted to “literally shut out the world.”
Theme 15. Supports needed during transition
Parents identified several supports they had difficulty accessing during transition. These were either not available or those available were unsuitable for their child. Table 4 identifies these supports and some of the reasons why parents had difficulty accessing them.
Supports Needed During Transition That Parent Caregivers Had Difficulty Accessing.

Note. TBI = traumatic brain injury; PDD = persons with developmental disabilities.
Discussion
This study examined the experiences and challenges faced by family caregivers of young adults with TBI who have recently transitioned from services for children and adolescents to adult supports and services. Emerging findings confirm that this transition can be challenging for many young TBI survivors and their caregivers (Kirk, 2008) and that many experience this process as overwhelming, depersonalizing, and condescending (Kirk, 2008; Soanes & Timmons, 2004). In keeping with previous studies (Gan, Gargaro, Brandys, Gerber, & Boschen, 2010; Gauvin-Lepage & Lefebvre, 2010), factors that family caregivers cited as most stressful include communicating across different health care systems, locating and organizing support from community services, and locating vocational service providers who understand the special needs of people with TBI.
Transition from pediatric to adult care services can be challenging for several reasons. First, the two service sectors espouse different philosophies that affect the structure of service delivery (Kirk, 2008). Adult support care services, unlike child and adolescent care settings, do not provide the level of comprehensive and developmentally appropriate clinical care for people who have specific types of health issues (Kennedy & Sawyer, 2008). Second, within adult settings, young people are required to have a high degree of autonomy, knowledge, and the capacity to manage their own health as well as social and vocational needs; in contrast, in child care settings parents are relied on heavily to take on these responsibilities along with service providers (Kennedy & Sawyer, 2008). The findings of this study suggest that many young TBI survivors at the time of transition may not have the level of autonomy and independence required in adult settings and are dependent on their family caregivers for a longer time compared with survivors with other medical conditions. Third, although the support required is contingent on the stage of the recovery process, age, cognitive assets, and motivational factors of the TBI survivor, many caregivers suddenly find themselves taking on service provider roles because of a lack of a tailored approach relative to individual needs and a poorly planned transition with several gaps in service coordination and continuity. While a well-planned seamless transition can improve clinical, vocational, and social outcomes, a poorly planned transition can be associated with increased risk of noncompliance with treatment, poor social and vocational outcomes, and increased risk of morbidity and mortality (CHMSB, 2006) for TBI survivors. In the case of family caregivers, the long-term impact of caregiving can be associated with increased stress and negative health and mental health outcomes.
Since caregiving can have a pervasive role with a profound effect on the life course of family caregivers, the life course theory can be used to contextualize and understand the findings. Life course theory is a paradigm for examining the patterns of lives and how the life course is shaped by social, cultural, and historical influences (Elder & Giele, 2009). Caregiving and transition are important aspects of the life course theory. Family members’ lives are linked and interdependent (Elder, 1995; Elder & Caspi, 1990), and caregiving is described as a life contingency that illustrates this interdependency within families (Moen, Robison, & Fields, 1994). Elder and Giele (2009) identified four principles in the life course approach: These include (a) time of life course (importance of investigating the timing of life events or transitions within context of the life course). People coordinate responses to the timing of external events such as loss of employment to undertake actions that use available resources most effectively, (b) human agency (considering individuals motives to satisfy personal needs and their influence on decision-making) and therefore the organization of lives around goals within the constraints of their environment, (c) linked lives (the life of a person is interwoven with the lives of significant others) and (d) historical time and place refers to the social, historical, and geographical factors that influence human experiences e.g., social and cultural variations, social hierarchies, and historical events. Some of the strengths of the life course theory include the emphasis it places on the interdependence of human lives and family relationships and the acknowledgment of people’s strength, innovativeness, and capacity for change.
Many of the principles of the life course theory are evident in the participants’ descriptions of their transition experience. The findings highlight that most participants were ill prepared for the transition and many had to make lifestyle changes to address the needs of their relative during transition. This principle of interdependence of human lives and families was heightened as the young adults with TBI transitioned from child to adult care service systems. Because they had not yet acquired the capacity to manage their own health, social, and vocational needs at the time of transition, their caregivers had to take on these responsibilities, which had a significant impact on their own life course. The lack of support from service providers resulted in many caregivers, especially parents having to put their personal lives on hold while they attended to the multifaceted aspects of caregiving that encompassed locating health care, disability services, and/or advocating for their child’s condition. What sustained the caregivers’ motivation, despite frustration and emotional distress, was the hope that their loved one would get the resources needed to lead as normal and independent life as possible. These findings are in keeping with previous findings on individuals with TBI and their family caregivers (Nalder et al., 2012). For many caregivers a return to “as normal and independent life as possible” for their young adult relative meant taking on roles that are in keeping with social expectations. These included among others returning to school, taking up suitable employment, and developing a social network. The occurrence of these events for their relative would allow caregivers to resume their own personal and work lives, which provides further evidence of linked lives. Another principle of life course theory that is evident in the experiences of parents was human agency. For the caregivers in this study, assuming the caregiver role and all the responsibilities associated with it was a natural decision based on their relationship with the individual with TBI. Their commitment as caregivers to get resources for their relative’s recovery led to several initiatives such as strongly advocating with service providers and care systems, successfully appealing decisions made by service providers, and contacting people in their own networks for advice and information. Thus, caregivers directed their own life course in response to the environment (i.e., considering the limited options for support for the individual with TBI; Nalder et al., 2012).
Implications for Service Delivery and Policy
The findings of this study underscore the importance of supporting parents and the family system during transition (Kreutzer, Stejskal et al., 2009) through a proactive and well-developed transition plan and system of support. Proactive transition planning will ensure continuity of information and care for the transitioning individual, thereby minimizing the risk of secondary disabilities and family strain arising from a lack of appropriate services. The following section discusses practice and policy recommendations for a proactive seamless transition based on the findings.
Information manual
Many parents stressed the importance of being provided with vital information about services and supports that their young adult child with TBI would need and could access as they transitioned into adult care services. This could be in the form of a manual, online information booklet, or folder specific for survivors of TBI and their caregivers. It could provide a list of available services like income and disability support, transport, employment support programs, and trained aides. The booklet should be comprehensive and include information on how TBI could affect the brain and the individual in their daily activities, their roles as TBI caregivers, what these roles would involve, tips on how to navigate available services, and ideas on what would be helpful in their role as caregivers. The latter could include ideas on how caregivers could deal with common behavioral, emotional, social, and cognitive problems that TBI survivors experience.
Parents also suggested that there should be a hotline number that parents could call to get instant TBI-specific advice on how to deal with behaviors or where to access support. It was felt that providing this information booklet or online resource at the time of preparation for transition would give parents sufficient time to review and process the information and ask questions. Some parents suggested that a training course on transition should be available for caregivers to educate them about the different services and supports their child may need and be eligible for and the roles of different service providers and stakeholders (e.g., speech pathologists, lawyers, and doctors).
Preparing the young adult and family for transition-Developing a transition plan
An effective strategy for a seamless transition was advance preparation and the development of a transition plan. This transition plan would be tailored to the needs of the child based on the nature and severity of their injury impact, their strengths, level of disability, risk of subsequent accidents, and the behavioral, emotional, and cognitive issues that could arise. It would be developed by the service provider in collaboration with the family caregiver and would include the list of various services and supports needed for recovery and how these could be accessed. Parents were also keen for information on day programs that their child could attend for social stimulation. Some parents expressed that transition preparation should also include nurturing their child’s competencies and assessing his or her readiness to undertake study or work.
Appointing transition coordinator to oversee the transition process
Given the negative and often frustrating experience in navigating the transition, parents emphasized that having a service provider in the health system who knew their child and who they could approach for information and consultation would be of great help. Previous studies suggest appointing a transition coordinator for young adults with complex needs who are transitioning from pediatric to adult care services (Kingsnorth et al., 2011; Reiss, Gibson, & Walker, 2005). The transition coordinator could link the young adult with targeted services and supports, ensure minimal disruption of service and continuity in the information that is exchanged between parents and service providers, and facilitate consistent information on a continuous and up-to-date basis to successive service providers (Reiss et al., 2005).
Achieving coordination between services and supports
TBI survivors who are transitioning to adult care services and support systems often require a range of community services, including income support, home care, transportation and accommodation supports, vocational assessments, and employment support services. Given the traditionally poor collaboration among these service systems, many family caregivers often felt “pushed around” and subjected to a lack of coordinated services and as such had to repeat the same information to several service providers or fight for services for their child. Sloman (2005) suggest that a team approach to transition can help to achieve improved collaboration and coordination across different service providers. The transition team, which would include treating professionals like doctors, nurses, and social workers, could ensure that the required information for assessing eligibility and providing services are available to the respective service providers, thereby relieving the family caregiver of the stress involved in advocating for and navigating these services. In this context, it will also be important to provide training to service providers from different sectors on TBI and its impact on young adults and families.
Creating support systems and networks for caregivers
It is essential to create caregiver networks for family caregivers of TBI survivors in different locations across the local vicinity as this can help with parent to parent exchange of information about available supports. Because many caregivers may be unable to attend prescheduled events in regionalized in-person support groups, relevant organizations could consider distributing newsletters to families with information on brain injury, what parents need to know, how to run groups, and/or offer other forms of support for young adults with TBI. An online caregiver support group for parents of young adults with TBI may also be an important resource for consideration. In addition to caregiver support networks, previous research has highlighted that counseling and respite services are crucial for family caregivers of TBI survivors (Rotondi, Sinkule, Balzer, Harris, & Moldovan, 2007; Turner et al., 2010).
Study Limitations and Ideas for Future Research
Despite the significance of the findings, the study has limitations. First, the findings are based on a small cross section of 15 family caregivers from one city in Western Canada. While the sample size is appropriate for a phenomenological study (Creswell, 2007), this sample comprised mainly Caucasian caregivers with only one indigenous and two immigrant caregivers. Future studies must strive to recruit more caregivers from culturally diverse backgrounds to provide more representative findings. Second, of significance is that this study focused only on family caregiver experiences as they are the main sources of support for the TBI survivors. Firsthand account of the experiences of transitioning young adults with TBI is equally important and is recommended in subsequent studies, as are longitudinal studies that document shifts over time as well as interventional studies that test innovative supports to see ameliorative impact for individuals and families impacted by TBI. Third, despite the strengths of the life course theory which was used for contextualizing and understanding the findings, this theory has its limitations as it does not provide clear evidence to prove the link to macro systems and how these may influence caregiver behaviors. Furthermore, this theory does not sufficiently discuss issues related to diversity-in this case, issues of racism and discrimination and how these may influence behaviors. Finally, the descriptive phenomenological approach used in this study to understand the lived experience of family caregivers can be enriched by supplementing the information obtained with objective measures of caregiver health and quality of life.
Conclusion
The findings of this study offer important insights that convey that caregivers of TBI survivors are at significant risk for unending responsibility and strain, with possible deleterious health and mental health outcomes given the lifelong demands for parental caregiving. These findings suggest that there is a wide gap between what parents need and what is available to them to support their young adult child through the transition process and beyond. Most parents reported feeling unprepared and unsupported during the transition process. They want service providers and policy makers to listen to their concerns and offer several suggestions that can ease navigational concerns of finding resources within health care and other settings for their young adult TBI survivors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received funding from Policy Wise Alberta Canada.