
Abstract
The rapid increase in health information requires that learners exert some degree of self-control in learning to make an appropriate selection of what to learn about healthy living. The objective of this study was to determine the students’ level of self-control in learning for healthy living. A questionnaire adapted from the self-control subscale of the Self-Directed Learning Readiness (SDLR) Scale developed by Fisher, King, and Tague was used in determining the levels of self-control in learning for healthy living among students in Enugu State College of Education (Technical), Enugu, Nigeria. The study revealed that the students’ level of self-control was a little less than the recommended level. A significant difference was found in the male and female students’ level of self-control in learning for healthy living with the male students possessing a higher level of self-control. Significant differences also occurred in the students’ level of self-control in learning for healthy living when the students were classified based on their courses of study. The students’ level of self-control in learning for healthy living at the College of Education (Technical), Enugu, needs to be improved. Educators at the college should employ self-control-enhancing strategies to improve the level of self-control in learning among the students.
The proliferation of health-related information (some of which are based purely on selfish interests of the providers) calls for self-control in learning for healthy living. Conflict of information, sometimes, occurs in health-related information provided through several means. Some cues from the competing pressures may impel an individual to engage in behaviors while others may act to prevent the individual from taking action (Mann & Ward, 2007). The problems that plague individuals in many societies have some degree of self-control failure as a central aspect (Weir, 2012). The increase in health information requires that learners exert some degree of self-control in learning to make appropriate selection of what to learn about healthy living. Seeking for, and obtaining, the right kind of information is essential for healthy living, because only accurate health information empowers individuals for healthy living. Although the United Nations Convention on the Rights of the Child (CRC) emphasized the need for young people to have access to information and services that will promote their total well-being, it is also important to point out that only accurate and reliable health information is beneficial to young people (Nwalo & Anasi, 2010).
Sources of health information abound in Nigeria. Outside the formal school system, learners get information about health from the media, the Internet, family members, friends, advertising agents, peers, counselors, and people who have had similar health experiences, among others (Nwalo & Anasi, 2010; Obasola & Agunbiade, 2016). Of course these varied sources of information are not in themselves bad as they enable self-directed learning (SDL), which is being emphasized in the contemporary school systems (Guglielmino et al., 2009; Rubin, 2001). This emphasis is based on research findings that have shown that students learn better when the learning environment is learner-centered than when it is teacher-centered (Neo & Kian, 2003). However, learners should be able to select appropriate and relevant knowledge for healthy living.
Health care and general living conditions in Nigeria are poor, leading to persistent high disease burden (World Health Organization, 2015). With the high burden of disease, individuals turn to any available health information source to seek redress from diseases. The education system in Nigeria has not helped the issue. The standard of education in Nigeria, as noted by some researchers, has fallen. The teacher-factor has been identified as one of the factors associated with academic decline in Nigeria (Arong & Ogbadu, 2010; Duze, 2011).
Teachers exert strong influence in almost every aspect of the society. All professionals and workers in the society passed through the guidance of teachers at one time or the other. Many of what they do are direct outcomes of what teachers inculcated in them including how to seek information on healthy living.
Because no nation rises above the quality of its teacher, colleges of education where teachers are trained should undertake to provide solid training of teachers in basic skills within educational environments that are friendly and encourage SDL. Effective teacher education programs that are capable of translating into needed skills, knowledge, and attitudes that will meet not only the learning needs of the teacher but also that of the society are needed in Nigerian colleges of education (Olaniyan & Okemakinde, 2008).
A teacher can only give what he or she has to learners. If the students are guided to take charge of their learning environment through self-control in learning for healthy living, they will invariably transfer this quality to those who will be placed under their care as learners in the future. It is, therefore, pertinent to identity the students’ level of self-control in learning for healthy living as an important step to developing an SDL program for colleges of education in Nigeria.
SDL as a method of instruction is suitable for teaching and learning in tertiary education institutions (Fisher, King, & Tague, 2001). Self-control is an attribute of SDL that enables the learner to take responsibility for his or her own learning. Thus, the learners take control, taking decisions on what to learn or not to learn based on their learning needs. To engage in the critical processes that are necessary for self-control, the learners have to be fully conscious of their activities. Self-control practice provides learners with the critical thinking skills necessary to achieve autonomy (Massecar, 2008).
Self-control has become a hot topic, both for scientists interested in understanding the roots of human behavior and for practitioners who want to help people live healthier lives (Shekarkhar & Gibson, 2011). Self-control performance can be better in individuals with subjective vitality. This subjective vitality is enhanced in individuals who feel supported to become autonomous (Muraven, Gagné, & Rosman, 2008). Educators can, therefore, guide learners to become dependent on the educator or can help the learners to develop skills that make them independent and capable of autonomous learning (Peine, Kabino, & Spreckelsen, 2016). This assertion is supported by the self-determination theory.
The self-determination theory by Deci and Ryan (Deci & Ryan, 2008) portrays the difference between controlled and autonomous motivation. Controlled motivation occurs when an individual is motivated to act by external control. The purpose of such act is to make others happy or to receive a contingent reward from the external control. Autonomous motivation, in contrast, means doing things for intrinsic reasons or for one’s self. In other words, it could be called self-determined motivation. Self-control increases learners’ motivation to adhere to the goals of learning (Sanli, Patterson, Bray, & Lee, 2013). Self-controlled practices lead to enhanced learning because they are more consistent with the learners’ needs (Sanli et al., 2013). Deeper information processing takes place when an individual is confident that he or she is in control of the learning (Zamani, Fatemi, & Soroushmoghadam, 2015). Again Teixeira, Carraça, Markland, Silva, and Ryan (2012) observed that behaviors that are intrinsically motivated are associated with increase in commitment and maintenance while behaviors that are governed by introjections are unstable in terms of maintenance.
Self-control is synonymous with self-regulation and self-discipline. They all refer to the control of one’s conducts based on motives related to goals or ideals that the individual has for himself or herself. The motivation and ability to control or regulate self are positively associated with school achievement (Duckworth & Seligman, 2006; Suchodoletz, Trommsdorff, Heikamp, Wieber, & Gollwitzer, 2009). Specific components of self-controlled learning could contribute to gender differences in school achievement (Duckworth & Seligman, 2006; Kuhl & Hannover, 2012). Gender and culture have also been identified as an interesting factor in the motivation of self-controlled learning (Mclnerney, 2008; Meece & Painter, 2008). Gender differences are precursors to students’ use of certain forms of SDL. Course of study as a factor categorizes students into specific training programs. The value the students place on each course of study and the roles that educators play in these courses may differ and could influence the students’ self-control in learning for healthy living. These factors could act to control motivation or to enhance autonomous control. Zimmerman and Schunk (2008) noted that the issue of cultural or ethnic group differences in students’ use of SDL processes and motivation has received relatively little attention to date. It is on this premise that this study was conducted to determine students’ self-control in learning for healthy living.
Rosenbaum (1980) developed the self-control schedule—a scale that is commonly used to measure self-control in education. The scale assesses the ability to delay immediate gratification, apply problem-solving strategies, and control emotions. Rosenbaum (1990) later renamed the self-control schedule as learned resourcefulness. Similar scales designed to measure self-control include self-control questionnaire by Rehm et al. (1981) and the self-control questionnaire by Brandon, Owscher, and Loftin (1990).
Rosenbaum’s (1980) self-control schedule is a broad measuring scale that measures problem solving and pain tolerance in addition to other dimensions of self-control. The self-control questionnaire by Rehm et al. (1981) was designed to measure self-control deficits associated with depression. The self-control questionnaire by Brandon et al. (1990) was designed to measure behavioral outcomes suggestive of self-control. None of these scales, therefore, was designed to measure self-control in learning and particularly learning for healthy living. This study, therefore, adapted the self-control subscale of the Self-Directed Learning Readiness Scale (SDLR scale) developed by Fisher et al. (2001).
To appraise the increasing health information through the media and the Internet, the learners need adequate self-control to enable them to make the right choices in patronizing health facilities and services. There is a need to identify students’ learning needs for the educator to implement teaching strategies that will best suit such needs. Understanding students’ levels of self-control in learning for healthy living is important in designing and the implementation of any health education intervention programs for healthy living.
The Purpose of the Study
The purpose of the study was to investigate the students’ level of self-control in learning for healthy living as an indicator of their readiness for SDL for healthy living.
Research Questions
Hypotheses
Method
Participants
The target population comprised all the students at the College of Education (Technical), Enugu, in Enugu State of Nigeria. Yamane’s (1967) formula for determining sample size was used to determine the sample size for this study. A sample of 168 students was selected from the five schools in the college using the stratified random sampling technique. The stratification was done based on gender and course of study. A random sample proportionate to a stratum’s size was taken from each stratum. The schools in the college were as follows: School of Science Education, School of Education, School of Technical Education, School of Vocational Education, and School of Business Education. The students were informed that they were to partake in a study. Anonymity was ensured, and students were informed that they can opt out if they so wished.
Instrument for Data Collection
A questionnaire adapted from the self-control subscale of the SDLR scale developed by Fisher et al. (2001) was used in the collection of data for this research. The items on the original subscale on self-control were modified to suit learning for healthy living. The modifications were based on Fisher et al.’s (2001) caution that in using the SDLR scale, it would be inadvisable to assume that a person who possesses high levels of readiness for self-direction in a given situation would still possess the same amount of readiness in a new and unfamiliar context. They, therefore, suggested that measuring SDL readiness needs to be done within a specific context.
The internal consistency for the self-control subscale was estimated by Fisher et al. (2001) to be .83 using Cronbach’s coefficient alpha. The modified scale was face validated by three experts from the Departments of Health and Physical Education, University of Nigeria, Nsukka, Nigeria.
One hundred and sixty eight copies of the questionnaire were administered to the students and collected back on the spot. The students were asked to indicate on a 5-point Likert-type scale, the extent to which the items were descriptive of their own characteristics. Out of these 168 copies of the questionnaire, only 164 copies were adequately completed. This represented a response rate of 98%. Only these were used for data analysis.
Method of Data Analysis
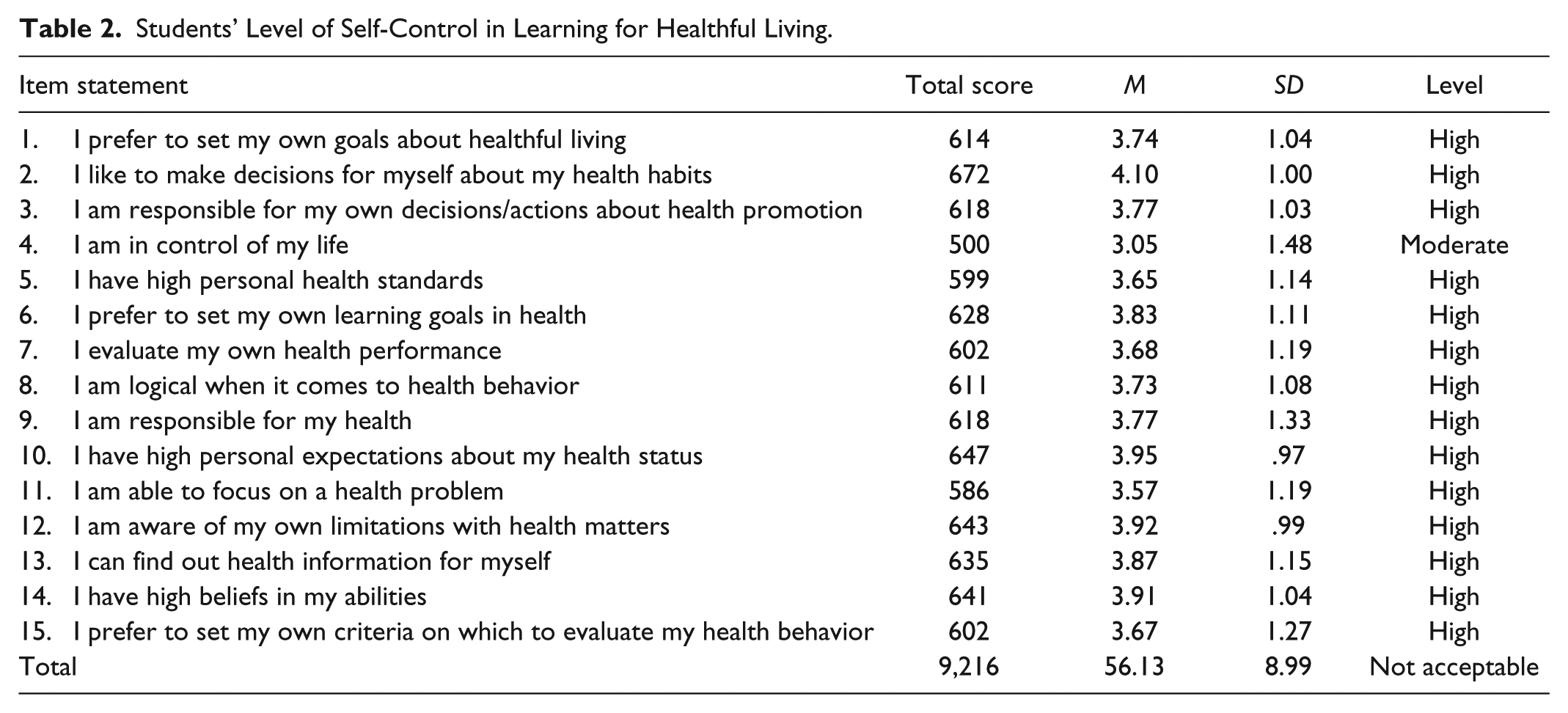
The student responses to the items in the questionnaire were all weighted on a 5-point Likert-type scale as follows: 5 for strongly agree, 4 for agree, 3 for undecided, 2 for disagree, and 1 for strongly disagree. To determine the level of self-control in learning for healthy living, means and standard deviations were obtained. Klunklin, Viseskul, Sripusanapan, and Turale’s (2010) criteria for interpreting readiness on a 5-point scale recommended that a score of 4.50 to 5.00 is the highest level of readiness, 3.50 to 4.49 is high level, 2.50 to 3.49 is moderate level, 1.50 to 2.49 is low level, while a score of 1.00 to 1.49 is the lowest level of readiness. This criterion was adopted in interpreting the students’ mean scores on the various items on the self-control scale. This item-by-item analysis of data would yield the relevant data that will enable the development of appropriate intervention in a subsequent project.
To interpret the aggregate scores, Fisher et al. (2001) recommended that for the 40-item SDLRS, a mean score greater than 150 should be considered an acceptable level of SDL. This accounts for a score of 75% and above. Because this study used only a subscale (self-control subscale), which had only 15 items, we adopted Fisher’s 75% score and above which in this case is equal to a mean score of 56.25. Therefore, in this study, an aggregate score less than 56.25 was not an acceptable level of self-control in learning for healthy living.
To compare the levels of self-control in learning for healthy living between male and female students, the independent sample t-test analysis was used. Analysis of variance (ANOVA) was used to compare self-control in learning for healthy living across schools of study.
Results
Only the 164 adequately completed copies of the questionnaire were analyzed and used for the study. The demographic information extracted from the questionnaire shows that 38 (23.17%) students were males while 126 (76.83%) were females. The distribution of the students from the various schools is shown in Table 1. The means and standard deviations of the students’ response to the items were determined, and the result is shown in Table 2. The highest mean score was on the item “I like to make decisions for myself about my health habits” (
Descriptive Statistics for Study Variables.

Note. SSE = School of Science Education; SED = School of Education; STE = School of Technical Education; SVE = School of Vocational Education; SBE = School of Business Education.
Students’ Level of Self-Control in Learning for Healthful Living.
Summary of t-Test Analysis of the Differences in Male and Female Students’ Level of Self-Control in Learning for Healthful Living.

Note. n = 164, df = 162.
Significant at .05 level of significance.
Summary of Analysis of Variance of the Differences in Students’ Level of Self-Control by School of Study.
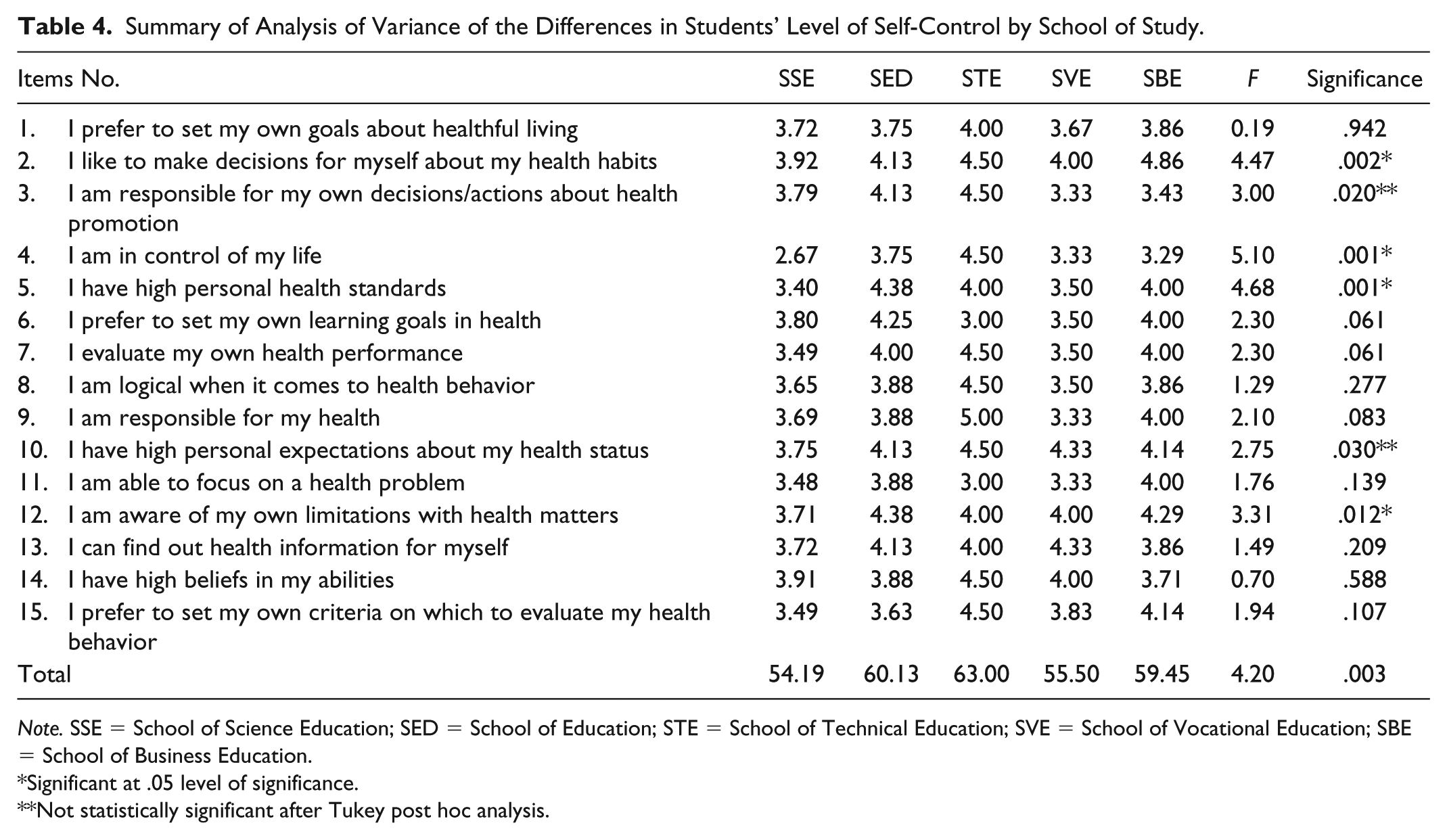
Note. SSE = School of Science Education; SED = School of Education; STE = School of Technical Education; SVE = School of Vocational Education; SBE = School of Business Education.
Significant at .05 level of significance.
Not statistically significant after Tukey post hoc analysis.
The results also revealed significant differences in Items 2, 3, 4, 5, 10, and 12. The Tukey Honestly Significant Difference (HSD) post hoc test was further used to analyze Item 2, “I like to make decisions for myself about my health habits,” and it yielded significant differences between the School of Science Education and School of Business Education (p = .001), and also between School of Science Education and School of Vocational Education (p = .047). When we applied the Tukey HSD on Item 3, “I am responsible for my own decisions/actions about health promotion,” there was no significant difference between any of the paired groups. The Tukey HSD post hoc test yielded significant differences on Item 4, “I am in control of my life,” between the School of Science Education and School of Education (p = .009) and between School of Science Education and School of Technical Education (p = .020). For Item 5, “I have high personal health standards,” the Tukey HSD post hoc test showed statistically significant differences only between the School of Science Education and School of Education (p = .001). Again, for Item 10, “I have high personal expectations about my health status,” the Tukey HSD post hoc test showed no statistically significant differences between any of the paired groups. Finally, for Item 12, “I am aware of my own limitations with health matters,” the Tukey HSD post hoc test showed statistically significant differences only between the School of Science Education and School of Education (p = .023). When the Tukey HSD post hoc test was applied to the aggregate mean scores of the students from different courses of study, it yielded statistically significant difference only between the School of Science Education and School of Education (p = .026).
Discussion
We examined the students’ levels of self-control in learning for healthy living and compared these across gender and course of study. The results showed that students at the College of Education (Technical), Enugu, possessed below the acceptable level of self-control in learning for healthy living. Using Klunklin et al.’s (2010) criteria, they had high level of self-control on all items on self-control in healthy living except for the item “I am in control of my life” (Table 2). The students had their highest mean score for the item “I like to make decisions for myself about my health habits” (
The finding of this study differed from that of Williams et al. (2013) who found that undergraduate paramedic students from four Australian universities had acceptable levels of SDL readiness on the three subscales of the Fisher et al. (2001) SDLR scale. This difference could be attributed to the differences in the method of teaching in these institutions. Peine et al. (2016) asserted that educators can guide learners to become dependent on the educator or can help the learner to develop skills that make them independent and capable of autonomous learning.
The male students in this study indicated a greater level of self-control on all the items than the female students except for the item “I am responsible for my own decisions/actions about health promotion.” This finding differs from previous studies, which had shown that sex is one of the most robust predictors of self-control and that girls score higher on a variety of measures of self-control (Chapple, Vaske, & Hope, 2010). It is pertinent, however, to note that most of these previous studies were on drug abuse and crime involvement, and not on learning. The present study, however, investigated self-control in learning, and so it is not surprising that the findings differ from those on self-control in deviant and criminal behaviors.
The present finding could be attributed to a socialization process in the area of study. Females in Nigeria are generally trained to be submissive (Abegunde, 2014) and dependent, and, thus, lacking autonomy. Gottfredson and Hirschi (1990) had earlier identified the parental socialization process as a cardinal factor determining a person’s level of self-control. Parental acceptance such as giving psychological autonomy to children; using nonphysical, fair and consistent discipline; and providing a balanced level of monitoring have been shown in literature to have positive effect in generation of self-control (Gibson, Sullivan, Jones, & Piquero, 2010; Nofziger, 2008; Ratchford & Beaver, 2009; Vaughn, DeLisi, Beaver, &Wright, 2009).
Self-control is needed for such activities as controlling thoughts and emotions, regulating task performance, and making decisions. Self-control can be depleted (Muraven & Baumeister, 2000; Weir, 2012). Due to unbalanced pressures and expectations placed on them, female students may be using up their self-control on such activities as controlling against deviant behaviors and crime. This could be so because literature indicated that girls score higher on self-control with regard to deviant behaviors (Gottfredson & Hirschi, 1990), and consequently, they may be depleting their reserve of self-control, which is also needed in learning for healthy living.
Students from the School of Technical Education had the highest mean score on self-control followed by those from Schools of Education, Business Education, Vocational Education, and Science Education. Tukey HSD post hoc test yielded statistically significant differences only between the School of Science Education and School of Education (p = .026). This was quite unexpected. It was expected that students from the School of Science Education will have the highest score since they are the students who study health-related courses. The result, however, could be attributed to differences in the instructional techniques adopted in teaching various courses of studies. For instance, Prabjandee and Inthachot (2013) in a similar study found that different majors possessed different self-directed learning readiness. This goes to buttress the point that self-control can be learned and improved on.
Implications for Teaching and Learning for Healthy Living
The findings of this study have portrayed the students’ level of self-control in learning for healthy living at the College of Education (Technical), Enugu. The difference in the levels of self-control between male and female students and among students from different courses of study has been revealed. The female students had unacceptable levels of self-control in learning for healthy living. As such, health educators and other lecturers at the college should identify ways of helping the students, particularly the female students, to be responsible for their own learning especially for healthy living. This is of paramount importance because educating a woman has an implication on the level of knowledge of her children. More so, it has been shown that educated women are more likely to influence their future positively, contribute positively to the socioeconomic status of the society, take good care of their families, are healthier, and tend to have greater self-esteem and self-confidence. The student should be assisted through programs that help improve self-identity and decision making. The female students should be encouraged to develop some degree of autonomy that will enable them to feel confident to take decisions about what to learn and what not to learn for healthy living. Health educators should encourage the student to take responsibility for their lives and not just accept whatever knowledge is presented to them. They should also assist students to set high health standards that are attainable and to pursue achievement of the same through a variety of sources found to be credible based on existing scientific facts. Strategies such as supportive learning environment, providing constructive feedback, encouraging self-assessment, using self-reflection, providing opportunities to engage in their own learning processes, and developing goal-orientation values are helpful in enhancing SDL (Smedley, 2007) and so should be adopted by educators at the college to increase self-control in learning for healthy living.
Appropriate guidance is needed to enhance self-control in learning in students. Such strategies as acceptance of students by teacher/educators, fairness and consistency in discipline, and providing a balanced level of monitoring have been shown in literature to have positive effects in generation of self-control (Gibson et al., 2010; Nofziger, 2008; Ratchford & Beaver, 2009; Vaughn et al., 2009). They, therefore, should be employed in training of students.
Limitations of the Study
This study relied on the participants’ perception of their level of self-control rather than their actual behaviors. This could have influenced the result, and so the interpretation should be done with caution. Again, the limited sample of students from the College of Education (Technical), Enugu, could skew the results and may not allow for generalization of the findings. Future studies should use larger sample sizes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.