
Abstract
Asset-Based Community Development (ABCD) appears to be a promising way to supporting people with long-term health problems but there is currently a lack of evidence to support this approach. Taking a realist approach, a review and concept-mapping exercise of ABCD approaches to improve health were conducted with a view to providing a better understanding about these approaches, how they work, and who they work for. Totally, 29 papers were deemed relevant and included in the review. The realist synthesis and concept mapping helped to identify concepts most commonly associated with ABCD but found no papers focused on long-term conditions (LTCs) and thus no evidence that this approach improves health outcomes for people with LTCs. While there is a lack of clarity about how to implement ABCD or how to evaluate it, this article offers a clearer theoretical framework about the essential ingredients needed to activate ABCD.
Keywords
Background
Long-Term Conditions and Self-Management Support
Socially and economically deprived populations experience disproportionately higher levels of long-term health problems, and the prevalence of long-term conditions (LTCs) are increasing along with rates of multimorbidity (Barnett et al., 2012; Lopez & Murray, 1998; Marmot, 2010; World Health Organization, 2010). There have been calls for more targeted self-management interventions for disadvantaged populations (Griffiths et al., 2007; Marmot, 2010) and it has proved difficult to implement self-management support for people with LTCs in traditional primary care settings (Kennedy et al., 2013). There is general acceptance that there is a need for alternative ways to support people with LTCs (Trappenburg et al., 2013).
The Marmot review (Marmot, 2010) advises that meeting the health needs of disadvantaged populations and tackling inequalities in health requires a broader focus on creating and developing healthy and sustainable communities. A key recommendation includes engaging with the third sector and community groups and empowering individuals and local communities to improve health and well-being outcomes. Similarly, a major component of the influential Chronic Care Model is to mobilize community resources and form effective partnerships with community organizations to meet patients’ needs (Wagner, 1998). This links with evidence that social networks play an important role in health management and that engagement with meaningful activity can significantly influence health outcomes (Reeves et al., 2014; Vassilev et al., 2013). A recent trial which tested an intervention which facilitated access to local community resources showed significant improvements in health outcomes for patients with Stage 3 Chronic Kidney Disease (Blakeman et al., 2014). This highlights the potential benefits of widening the types of support offered to people with LTCs, in particular by shifting the emphasis toward supporting access to community resources and personal networks of support (Blickem et al., 2014).
Asset-Based Community Development
Asset-Based Community Development (ABCD) was originally conceived as an approach to support community development in deprived inner-city populations in the United States in the early 1990s (Kretzmann & McKnight, 1996). The focus of ABCD in these original formulations was empowering communities to identify and address their own problems through the local assets available to them. Since implementation would be by local actors/nonspecialists using local resources, less attention was paid to the evaluability of ABCD than to outlining ABCD processes in ways that would be accessible to local activists. While there are implicit and identifiable theories driving ABCD processes and interventions, the potential requirements of policy makers in making external support available were given less consideration (Kretzmann & McKnight, 1996). There has been a resurgence of interest in ABCD in the context of global public health and particularly in the United Kingdom where it is seen as a way to address growing concerns over the widening gap in health inequalities (J. Foot & Hopkins, 2010; Marmot, 2010; Morgan & Ziglio, 2007). ABCD is seen as a way of tackling the social determinants of health and reducing health inequalities and has been described as a move from a disease prevention model targeting morbidity and mortality to a more positive approach targeting general health and well-being (Morgan, Ziglio, & Davies, 2010). Hence there are two challenges in adoption and promotion of ABCD by civic institutions (councils, public health, primary care, etc.); first to understand and present ABCD in ways amenable to policy makers, second to understand what is distinctive in ABCD in order to make sure this is preserved when institutions and external agencies become involved.
There have been many community development and empowerment models where the health need is identified by the community and they mobilize themselves into action (O’Mara-Eves et al., 2013). These models are similar to ABCD because they often aim to enhance mutual support and collective action to mobilize support. However, ABCD approaches to health and well-being are distinctive because they focus on identifying and building on the strengths, or “assets” of individuals and communities (J. Foot & Hopkins, 2010). However, currently ABCD lacks conceptual and methodological clarity and there is a very limited evidence base for its effectiveness in supporting people with long-term health problems. Hence, the effectiveness of ABCD interventions and the populations and contexts for which they are most suited are not well understood. Therefore, as a first step toward addressing this knowledge gap we describe a review of ABCD approaches in relation to LTCs with a view to providing a better understanding about these approaches, how they work, and who they work for (Morgan & Ziglio, 2007; Pawson, Greenhalgh, Harvey, & Walshe, 2005; Pawson & Tilley, 1997).
Realist Synthesis
This review was informed by realist methods (Wong, Greenhalgh, Westhorp, Buckingham, & Pawson, 2013). This was because we anticipated finding a complex and diverse literature which may not lend itself to traditional methods of review where the phenomenon of interest, the populations, interventions, and outcomes are all well specified (Wong et al., 2013). Our early understanding of ABCD was that it could be a term used loosely to describe a wide range of community initiatives and we suspected that using the term ABCD had become a popular catchall, or trend term, rather than a clearly defined methodology.
Realist Methods
Realist methods are useful in these circumstances because it permits an organic process which fits better with emergent and exploratory review questions (Dixon-Woods et al., 2006). Our initial review questions were broadly defined to allow inclusion of literature that may describe ABCD concepts and approaches but may use different terminology. We aimed to identify a coherent literature on ABCD in relation to health and well-being and generate understanding about:
What is ABCD?
What are the underpinning program theory/theories associated with ABCD?
Describe underlying mechanisms about how ABCD project/interventions are meant to work for people with LTCs?
What outcomes they are expected to have in relation to LTCs?
Realism and ABCD
Realist synthesis explicitly concerns itself with producing implementation and evaluation evidence, particularly in complex interventions, in a form amenable to gaining support of policy makers and evidence-based medicine (EBM; Pawson, 2002). It approaches this by close attention to describing relationships between context, mechanism, and outcome (C, M, O). In moving from a community-driven approach to an institutionally supported community approach, the evidence base required of ABCD is clearly changing. ABCD is explicitly concerned with context (C); however, as outlined above, mechanism (M) has been less fully articulated. Outcome (O) is also potentially problematic, while clear outcomes have been described in the literature, ABCD anticipates wider and potentially longer-term process benefits that may also need to be captured and appreciated to describe the full benefits. ABCD may well present a problem in that it explicitly favors interpretation through the value frameworks brought into being through its process by which the participants, local communities, and actors understand outcomes. These localized value systems may be difficult to translate into the value frames required of central policy makers. Within the realist tradition, however, this can be captured through its orientation to complexity, particularly in the work informed by Pawson and Greenhalgh (Pawson, Greenhalgh, Harvey, & Walshe, 2004).
Pawson’s Realist synthesis is arguably oriented to theory driven approaches to interventions initiated by policy makers rooted in wider conceptions of EBM, research translation and knowledge transfer (Pawson, 2002). Contemporary realist syntheses have recently become increasingly codified—a “full” synthesis requiring articulation of midrange theory developed through thorough articulation and interrogation of context, mechanism, and outcome (Wong et al., 2013). At first sight this may present problems with realist synthesis in evaluating community-driven approaches such as ABCD. We anticipated that these problems would play out through the realist evaluation process. While recognizing some accommodations may need to be made, we nevertheless concluded realist synthesis would be possible and moreover would ultimately be the most appropriate method to articulate the value of ABCD in terms amenable to policy audiences which would be the required next step for ABCD in areas such as LTCs management.
Method
In developing our search and synthesis strategy, we have followed the Realist And MEta-narrative Evidence Syntheses: Evolving Standards (RAMESES) guidance (Wong et al., 2013). Because of the iterative nature of this review and following realist principles, our search strategy was in two stages. First, we conducted a scoping review which was international, examining ABCD approaches to improve health outcomes of a given population. Articles that focused on ABCD and aspects of health and/or well-being were considered eligible for inclusion in the data extraction and quality assessment. We performed a preliminary scoping search using Google Scholar which was carried out by two members of the research team (S.D. and A.M.) to retrieve reports, thesis, key articles and any relevant websites to help inform our formal search strategy. This was followed by searching bibliographies of known articles to check for additional references. In addition, citation searches of all these key articles were carried out in Google Scholar. These initial searches yielded 19 relevant papers (see Table 1).
Scoping Review Papers.

The ABCD literature on health which emerged was diverse with a range of definitions for theory, methodology, and outcomes. We found ABCD was a term which could be used interchangeably with “Asset-based approaches” and these approaches used many common and overlapping definitions and it was unclear if these were used consistently. Therefore, in keeping with the realist synthesis (RS) method, the authors mapped the key concepts articulated by the authors associated with ABCD within the 19 papers and used these as search terms to identify definitions of “ABCD” and associated concepts (Trochim, 1989; see Table 2). Concepts associated with ABCD found in the initial searches were used in a comprehensive literature search using systematic methods carried out using the following databases: MEDLINE, EMBASE, and CINAHL. A practical limitation was imposed on the searches which were restricted to papers published after January 1990 to November 2016 as ABCD does not appear in the literature until the 1990s). Papers not published in English were excluded. We piloted searches by testing identification of known articles and modified accordingly. Searches were first run in MEDLINE and adapted for EMBASE and CINAHL (see Figure 1 PRISMA diagram). We then looked for empirical evidence combined with theoretical understanding to explain what are the underlying concepts of ABCD and assumptions about what effects they are expected to have in relation to LTCs. The review questions were modified to include the following questions:
a. What concepts underpin ABCD approaches to health in the existing literature?
b. What approaches and methodologies (mechanisms) are described to achieve ABCD in relation to health?
c. Is there evidence for the impact (outcomes) of ABCD in terms of LTCs?
Search Terms/Concepts for ABCD.

Note. ABCD = Asset-Based Community Development.
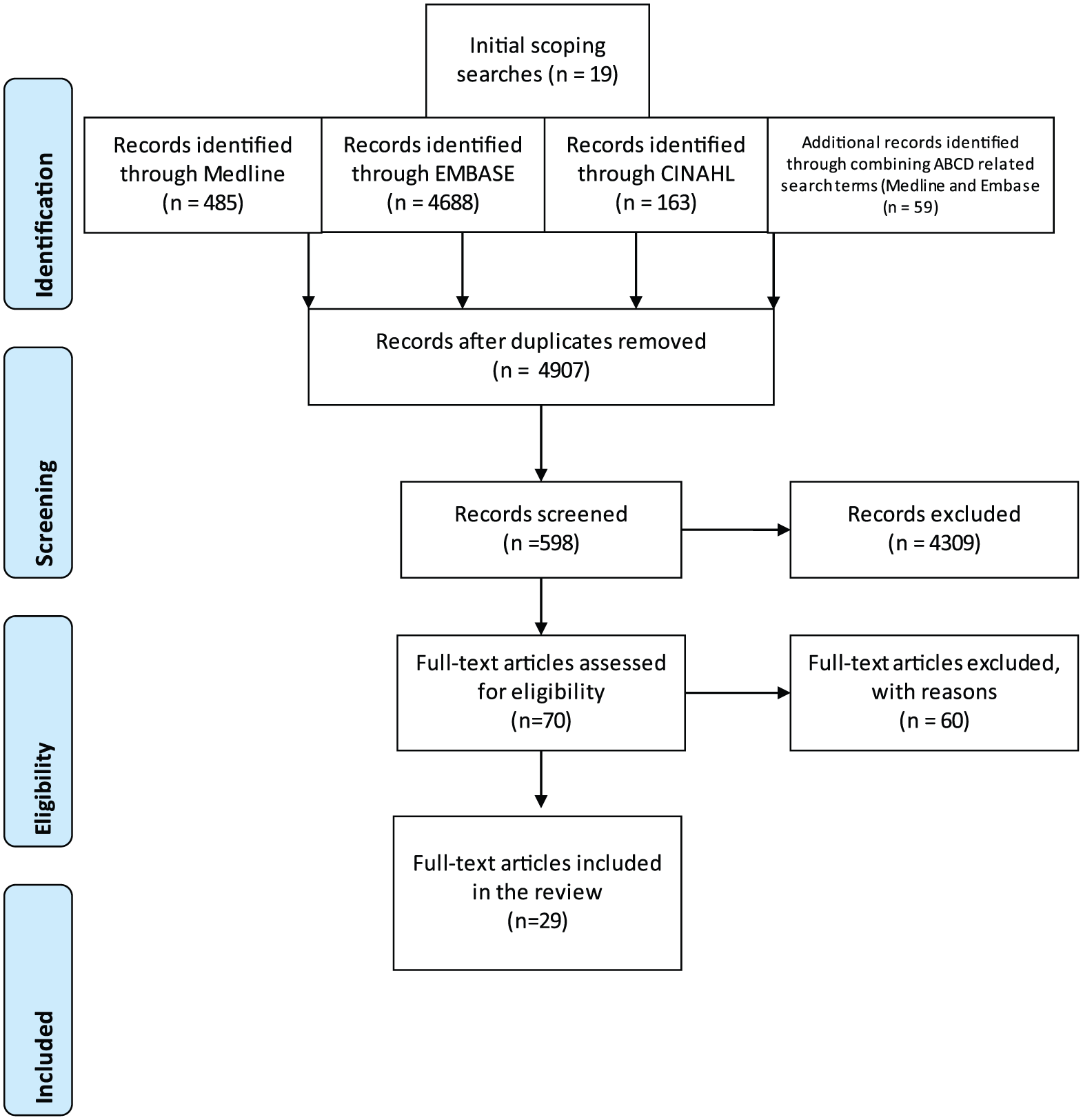
Flowchart on article selection for inclusion.
Selection Criteria and Synthesis
Members of the research teams each screened a portion of the titles and abstracts (S.D., A.M., J.L., C.B.). The potentially relevant records identified by individual members of the research team were then discussed with the other authors to confirm eligibility. This was followed by screening the full text of potentially relevant studies to determine eligibility for inclusion. The searches yielded no papers which focused on LTCs. Therefore, papers were included if they contained two or more concepts on the concept map and the focus of the article was on health. In total, an additional 10 articles were found and added to the review giving a total of 29 articles deemed relevant for ABCD in the context of health (see Table 3). Overall, our searches found 18 academic peer-reviewed articles (including 11 journal articles, one editorial, and six research/empirical papers), three professional journal articles, six reports, one book chapter, and one dissertation. We then proceeded with an evidence synthesis and concept-mapping exercise for all 29 articles (Trochim, 1989). We gathered multiple theories and concepts contained within the articles into identifiable strands as seen in Table 4. It presents a second-order synthesis organizing the first-order ABCD concepts articulated by authors translated through the lens of realist methods as (Assets) context, (Methodology) mechanism, and outcome. It is evident examining Table 4 that outcomes (in reference to ABCD) overlap to some extent with mechanisms. This is a reflection of the orientation of ABCD to acknowledging wider process benefits.
Systematic Review Papers.

Distribution of Concepts Across Articles.

Note. ABCD = Asset-Based Community Development.
Results
The concept-mapping exercise helped to identify concepts most commonly associated with ABCD and some of the key concepts which authors considered to underpin ABCD. The underlying program theories are also identified and are discussed in terms of their theoretical traditions and how these relate to types of assets, social theory (contexts), methodology (mechanisms), and outcomes. Box 1 gives a breakdown of these concepts and how they can be grouped.
Key Concepts Associated With ABCD.

Note. ABCD = Asset-Based Community Development.
Types of Assets and Social Theory (Contexts)
Examination of “assets” reveals some of the theoretical traditions which ABCD has drawn upon. ABCD appears to embrace (a) psychological theories which inform ideas about individual assets and (b) social theories which inform ideas about collective assets. Individual assets are often described as positive personal attributes of individuals such as self-efficacy, personal motivation (Bandura, 1977), and salutogenesis (Antonovsky, 1996), or “origin of health” which emphasizes the importance of personal characteristics as key factors for managing health. Other important individual assets (or attributes) include social competence, resistance, skills, commitment to learning, positive values, self-esteem, and a sense of purpose (Morgan & Ziglio, 2007). Other examples include positive reframing of personal identity (Pattoni, 2012).
ABCD also stresses the importance of social capital as a cornerstone of sustainable community engagement. For example, collective, community, or social assets such as connectedness, social networks, and reciprocity are seen as necessary for supporting and sustaining good health as well as producing meaningful outcomes for communities (J. Foot & Hopkins, 2010; J. H. Foot, 2012; Glasgow Centre for Population Health, 2012; Morgan & Ziglio, 2007; see Box 2 for a summary of types of assets). These assets have been described as three sets of “building blocks” which are, (a) personal assets as the “primary building blocks,” (b) collective assets as the “secondary building blocks,” for example, tangible community assets, for example, parks, libraries, and so on; and (c) “potential building blocks” which are the assets originating outside the neighborhood and controlled by outsiders such as access to social welfare (Ennis & West, 2010; Kretzmann & McKnight, 1996). These are all seen as “protective factors” to support and sustain health and well-being (Ennis & West, 2010; Fisher, 2011; Glasgow Centre for Population Health, 2012; Morgan & Ziglio, 2007; Box 2).
Types of Assets and Social Theory.

Methodology (Mechanisms)
ABCD sees populations as “coproducers” of health rather than consumers (Morgan & Ziglio, 2007) and this idea of the “collective” or partnership approach is central to both the methodology of ABCD and also the desired outcomes of ABCD. Methods for ABCD included “asset mapping” which is described as a process of documenting tangible physical assets such as parks and community centers as well as personal assets such as the skills and knowledge of the population (J. Foot & Hopkins, 2010; J. H. Foot, 2012; Glasgow Centre for Population Health, 2012). Asset mapping is often described as a grassroots, bottom-up process which sees assets as “building blocks” (Ennis & West, 2010; Keeble, 2006; Lohoar, Price-Robertson, & Nair, 2013; Mathie & Cunningham, 2003; Morgan & Ziglio, 2007; Nelson, Campbell, & Emanuel, 2011). Asset mapping draws on a number of techniques including capacity inventory, appreciative enquiry, action research/participatory research, and participatory appraisal.
These mapping techniques are often found in models of organizational development. For example, appreciative enquiry is a significant theory within organizational research developed from social constructionist theory and seen as an alternative to deficiency models which focus on problems and solutions (Bushe, 1999). Appreciative inquiry looks at the social potential of a social system and begins with appreciation, followed by collaboration, and this process should be proactive and applicable (Bushe, 1999). These techniques are seen as alternatives to “diagnosing problems” and instead focus on a “positive conversation.” This is considered a “strengths-based” approach to change, another concept adopted by ABCD. Action research is similar in that it adopts a collaborative approach to organizational change and a process of “planning, acting and fact-finding” (Lewin, 1958). Participatory enquiry has origins in rural development which is described in similar ways as a process owned by communities who are empowered to set the agenda for change and improvement (Chambers, 1994).
Asset mapping is also intended to encourage engagement and promote cooperative relationships within communities which is also a key outcome associated with ABCD. Hence, asset mapping is both a methodology intended to locate assets and also a step in the process toward a collective sense of “empowerment” and producing meaningful outcomes for a community.
ABCD Outcomes
Outcomes are generally imprecise and are often described as nurturing positive relationships, engagement with communities, improving social relationships and social networks, and coproduction. These are the desired outcomes which are not well-evidenced. These engagement processes appear to be intermediate steps toward more tangible health and well-being outcomes but this is not very clear. Further outcomes are described as “protective and promoting factors,” “cohesion,” and “sustainability” (Ennis & West, 2010; J. Foot & Hopkins, 2010; Keeble, 2006; Lohoar et al., 2013; Mathie & Cunningham, 2003; Morgan & Ziglio, 2007; Nelson et al., 2011).
Evidence for ABCD Approaches to Health
It is difficult to assess whether ABCD achieves the outcomes above or any other reported outcomes because the quality of the empirical studies is poor (as interpreted through the lens of EBM) and because there appears to be no published study which explicitly sets out to implement and evaluate an ABCD “model” of delivery. Many of the intended outcomes tend to be quite ambiguous anyway. For example, Bull et al. and Aronson et al. try to evaluate the benefits of assets approaches to health but only conclude that material and physical resources are important for health and well-being (Aronson, Wallis, O’Campo, & Schafer, 2007; Bull, Mittelmark, & Kanyeka, 2013). Lohoar et al. report reductions in use of alcohol and drugs in young people and improved emotional and life skill, but this is in reference to a number of small projects and it is difficult to assess the quality of the research conducted (Lohoar et al., 2013). See Box 3 for a summary of the empirical studies and their reported outcomes.
Summary of Reported Papers and Outcomes.

Of all the published research in the area of ABCD and health, Rütten (Rütten, Abu-Omar, Frahsa, & Morgan, 2009) appears to come closest to identifying and describing a project which has some tangible ABCD qualities and reported health outcomes. This study reports on a project in Germany to improve opportunities for physical activity among women described as being in difficult life situations. The project involved the formation of focus groups and workshops involving the women, policy makers, and local experts. The women were tasked to identify local assets for physical activity and decided there was a need for affordable aerobic classes and the local school was seen as an ideal place. However, they encountered restrictions on using this site due to public policy rules. There was some political debate with the women receiving support from the local council and a temporary solution was achieved and the fitness class was deemed a success. As a result of this project, the women now have representation on the local council.
Hence, the Rütten study (Rütten et al., 2009) demonstrates the following qualities of an ABCD approach (see Box 4).
Rütten (Rütten, Abu-Omar, Frahsa, & Morgan, 2009) Qualities of ABCD.

Note. ABCD = Asset-Based Community Development.
Discussion
This review was conducted to understand what the underlying concepts of ABCD are, and what evidence there is about impacts they are expected to have in relation to LTCs. A realist synthesis approach was adopted because we anticipated finding a complex literature which would not lend itself to traditional methods of review. As expected, initial searches yielded a small literature, but these papers gave some useful insights into many concepts associated with ABCD which informed a further search. There were no papers which focused on LTCs, but there were papers which provided useful insights into ABCD in the context of general health and well-being. ABCD appears to integrate a number of loosely related concepts and definitions from a range of theoretical traditions to describe, or make sense of, a broad-based approach to improving public health.
Common understandings of ABCD approaches to public health and well-being involves “asset mapping” or locating resources/strengths within a community and using these assets for sustainable community development. Assets can include skills, knowledge, or connections in a community (J. Foot & Hopkins, 2010). Recent initiatives to establish assets models as a sustainable approach to public health tend to highlight positive capability, changes in attitudes and values, personal and collective empowerment, and raising self-esteem and resourcefulness of individuals to improve and sustain their own health (J. Foot & Hopkins, 2010). Our conceptual review and synthesis (Table 4) demonstrated that assets, ABCD methodology, and outcomes can be mapped to contexts, mechanisms, and outcomes. It also suggests that ABCD may be amenable to realist evaluation and that CMO may provide a potent conceptual bridge between the evidence requirements of EBM and fuzziness and complexity accepted in more community-oriented publications. Importantly it highlights how assets, methods, and outcomes in ABCD rest on a process orientation that may be difficult to adequately capture in conventional EBM evaluation approaches and timescales. Our introduction outlined how the primary valuation frames of ABCD are those coconstructed by participants. The case study by Rütten (Rütten et al., 2009) demonstrates how ABCD helped the participants to organize and legitimate their health needs through engagement in the local political sphere. The act of organizing and the development of a community identity allowed the women to successfully voice this localized value frame against the alternative valuation frame articulated by external financial interests which previously held sway. Engagement and interplay between institutional forms (society) and community forms (Tonnies & Loomis, 1963) is becoming more common in the health arena, particular through widespread requirements for patient and public involvement. The synthesis presented here highlighted some of the issues with the differential orientation to knowledge production, verification, and ownership characteristic of the traditional community society dichotomy and tentatively suggests some ways forward (Tonnies & Loomis, 1963). Although outcomes were often not well described in the studies included in this review, we demonstrated here that there is a degree of potential to translate the fuzzier outcomes of approaches such as ABCD into the more instrumental Context, mechanism, outcomes (CMO) requirements of approaches such as realist synthesis. In doing so, we had to attend to the full scope, history, and philosophical roots of realist synthesis as well as recognizing recent codifications and requirements arguably necessary to preserve the veracity and quality of the realist field (Wong et al., 2013). In particular our conceptual review and synthesis step was necessarily perhaps more akin to meta-ethnography (Noblit & Hare, 1988). This was necessitated by the review aims and material and we would argue along with Wong et al. (2013) that tailoring methods inductively to review circumstance is both necessary and intrinsic to the realist approach.
However, the findings from this review raise some questions about the relative importance of some assets compared with others. For example, empowered and motivated individuals seem to be an essential precondition to begin and sustain this process. There also needs to be cooperation of political powers, and of course there needs to be tangible physical assets to work with. ABCD as an approach to improving health, therefore, appears to need the existence of these assets for any progress to be made. Therefore, it seems that the key mechanisms for ABCD to work could be (a) engagement with the target population, (b) engagement with political powers, and (c) identifying collective goals of all parties. Understanding these preconditions may help to develop a clearer definition of ABCD and key criteria so that application of this approach may be more easily achieved (see Box 5).
Potential Criteria of ABCD to Improve Health and LTCs.

Note. ABCD = Asset-Based Community Development; LTCs = long-term conditions.
Crucially, however, this review found no evidence that ABCD “works” in relation to health and LTCs, with only six empirical studies identified, all of which reported anecdotal findings (because either outcomes were not well described or because the quality of the methods were poor). The Rütten study (Rütten et al., 2009) is the strongest and closest in terms of describing an ABCD project that “works” to improve health. Although there were no findings directly relevant to LTCs, ABCD does have potential in this context. The strength of this review is how we have unpacked ABCD as a complex intervention and revealed that it lacks evidence of impact.
However, the overarching objective of ABCD to improve health by stronger engagement with communities and understand how they define their needs and goals in relation to health has potential. Supporters of ABCD present this approach as a radical solution to improving the health and well-being of deprived communities which utilizes a range of methods to achieve desired outcomes (J. Foot & Hopkins, 2010; Morgan & Ziglio, 2007; Morgan et al., 2010). For example, empowered individuals, tangible physical resources, and strong social networks can all play significant roles to improve health outcomes (Bull et al., 2013; Morgan & Ziglio, 2007; Rütten et al., 2009; Whiting, Kendall, & Wills, 2013). However, it appears that ABCD relies heavily on the skills and motivation of the individuals of the population of interest and, therefore, ABCD is only likely to gain momentum through engagement with the target population. This has been a major criticism of ABCD; that it is too focused on a narrow range of psychological constructs such as positive thinking and resilience and avoids complex structural factors associated with material deprivation and health (Friedli, 2013). ABCD has been likened to therapies that aim to change how people think, for example, it is more important to be positive than to have an accurate perception of reality (Friedli, 2013). ABCD approaches have also been accused of avoiding debate about the imbalance of power between public services, communities, and corporate interests and the decline of statutory, state provision of both public services and public health (Friedli, 2013). ABCD is understandably quite politically attractive because it is inexpensive, requiring less financial investment for communities, with an emphasis on “people must help themselves.” ABCD could be described as an umbrella approach to a set of problems with complex causes which operate on the macro, meso, and micro level, while trying to primarily offer micro-level solutions through a framework that is undertheorized and lacking in conceptual clarity.
Therefore, debate about whether ABCD can tackle the realities of social deprivation and the impact of social and economic inequality continues and it is questionable if it is possible for communities to have any significant and sustained impact on their lives without major structural changes which are beyond their control. The Rütten study demonstrates some of these difficulties (strong opposition from corporate interests in the sport and leisure industry who felt threatened by the proposal from the group), which arguably exposes power imbalances and the lack of influence many people have on their surroundings relative to corporate or political interests.
Conclusion
The question as to whether ABCD as an approach can improve health and LTCs remains unresolved, but while many questions remain, the central notion of social capital as an essential ingredient for the general health and well-being of communities is well supported in other studies (Kawachi, Kennedy, & Glass, 1999). Studies have shown that social networks play an important role in supporting people with long-term health problems (Vassilev et al., 2013) and that engagement with meaningful activity such as employment or social clubs is associated with positive health and well-being outcomes (Reeves et al., 2014). Therefore, approaches which seek to build capacity within communities and which promote connectedness may have some potential to improve the health and well-being of its citizens. But enthusiasm and rhetoric must be backed by a clear set of objectives and procedures to ensure a rigorous and effective methodology. There also needs to be some clarity about the limits of personal attributes such as self-efficacy in this context with the understanding that many people in deprived circumstances who have a history of neglect and disengagement will find it very difficult to participate in these types of undertakings. Hence, arguably, there needs to be significant investment to support these populations and to understand the impact of social and economic deprivation for ABCD to have a long-term, sustainable impact.
Footnotes
Acknowledgements
The authors would like to thanks Anne Rogers and Anne Kennedy for their contributions to this study. The data sets used and/or analyzed during the current study is available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.B. designed the study, conducted the analysis, and wrote the paper. S.D. designed the study, conducted the searches and analysis, and wrote the paper. A.M. designed the study, conducted the searches and analysis, and wrote the paper. I.V. contributed to the analysis and gave feedback on drafts of the paper. R.H. conducted searches and gave feedback on drafts of the paper. S.K. contributed to the analysis and gave feedback on drafts of the paper. P.B. contributed to the analysis and gave feedback on drafts of the paper. J.L. designed the study, conducted the analysis, and wrote the paper.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was funded by the Liverpool Clinical Commissioning Group.