
Abstract
It is not clear whether the 16% unmet need for contraceptives in Nigeria indicates a success story. This study assessed the contraceptive prevalence rate (CPR), total contraceptive demand, and unmet needs and determined the distribution, determinants, and barriers to contraceptive demands and unmet needs in Nigeria. The fertility, breastfeeding, and contraceptive use information provided by 27,829 women who were either currently married or in a sexual union in the 2013 Nigeria Demographic and Health Survey (NDHS) were extracted. Associations between having unmet needs and the demographic, socioeconomic, and reproductive profiles of the respondents were assessed using bivariate and multiple logistic regression at 5% significance level. Multiple response data analysis techniques were used to assess barriers to nonuse of contraceptives. Data were weighted to reflect differentials in the population of in-union women in each geographical state. The modern CPR was 9.8% while total demand for contraception was 31.2%, consisting of unmet need at 16.1% and met needs at 15.1%. Unmet need for family planning was higher among rural women compared with urban women (16.8% vs. 14.9%); younger women (adjusted odds ratio [aOR] = 4.29; confidence interval [CI] = [3.03, 6.07]), women belonging to poorer economic status (aOR = 2.27, CI = [1.92, 2.68]), and women with no education (aOR = 3.23, CI = [2.60, 4.02]) had higher odds of unmet needs. The low unmet need should not be mistaken for a good progress in family planning programming in Nigeria; the success is better measured using the level of total demand for contraceptives and CPR. Interventions to improve the socioeconomic status of women, increase the knowledge of modern contraceptives, and improve women’s decision-making power should be prioritized.
Introduction
In recent times, campaigns for improved sexual and reproductive health of women through the use of contraceptives have been one of the world’s major public health interventions. It has been advocated by international organizations, governments, and nongovernmental organizations as well as charity and community-based organizations. Worldwide, several million women who desire contraceptives are not using it despite huge investments in contraceptives. Prior to 2009, it was estimated that about US$3.1 billion was spent annually on education, promotion, production, and distribution of various family planning (FP) methods to about 600 million people who use modern contraceptives worldwide (Kent, 2010; Singh, Darroch, Ashford, & Vlassoff, 2009). The Gates Foundation had stressed that voluntary FP remains one of the most cost-effective investments a nation can offer its present and future and that “every $1 spent on FP translate to $6 savings to be expended on other livelihood services” (The Gates Foundation, 2015). In Nigeria, US$603 million has been budgeted to achieve full-scale FP program for 2013–2018 (Federal Government of Nigeria, 2014). Compared with 3% in 2003, 22% of the 2015 Nigeria government total expenditure went on public health of which contraception is a major component (U.S. Agency for International Development [USAID], 2015). The big question is “does the level of unmet need of FP in Nigeria justify the budget it has attracted in recent time”?
The worldwide campaign for use of FP is borne out of the fact that adoption of FP can help improve sexual and reproductive health. If used properly and regularly, some FP methods such as condoms prevent the transmission of HIV and other sexually transmitted infections (Adebowale, Fagbamigbe, & Bamgboye, 2011). FP also reduces unwanted pregnancy and the demand for unsafe abortion (Martinez, Copen, & Abma, 2011; Martinez, Daniels, & Chandra, 2012). The long-term benefits of using FP include securing the well-being and autonomy of women, enhancing health and development of communities and nations, reduction of infant and maternal mortality, reduction of incidence of HIV, empowering people, ensuring better education, and making population growth slower (Ezire, Oluigbo, Archibong, Ifeanyi, & Anyanti, 2013; Fagbamigbe, Adebowale, & Olaniyan, 2011; Martinez et al., 2011; Wellings et al., 2006).
These benefits necessitated the inclusion of contraceptive prevalence rate (CPR) as one of the indicators of the Sustainable Development Goals (SDG) 5 (Adebowale et al., 2011; Ezire et al., 2013; Fagbamigbe et al., 2011, Federal Government of Nigeria-Millennium Development Goals, 2014; PATH, 2008; United Nations, 2011; World Bank, 2013; World Health Organization [WHO], 2012). Evidence suggests that unwanted pregnancies are common among women at the beginning and later end of their reproductive age (Becker, Wolf, & Levine, 2006; Kent, 2010; Klima, 1998). Unwanted pregnancy has also been reported to be strongly associated with maternal mortality through unsafe abortion and pregnancy complication factors (Klima, 1998; Singh, Darroch, Ashford, & Vlassoff, 2009). According to reports from the Gates Foundation, about a quarter of the 80 million unplanned pregnancies in developing countries were aborted in an unsafe manner in 2012 (The Gates Foundation, 2015). Later in life, products of unwanted pregnancies may have higher negative outcomes than those who were not and their poverty gap may get wider (Gelband, 2001; Marston & Cleland, 2003).
Although contraceptive use has increased globally, its use has remained very low in sub-Sahara Africa, Nigeria inclusive (Ashford, 2003; Darroch, Sedgh, & Ball, 2011; World Bank, 2010). The world CPR rose from 54% in 1990 to 57% in 2012 and from 23% to 24% in Africa over the same period (United Nations, 2011; WHO, 2014). National surveys in 2012 and 2013 have placed CPR in Nigeria at about 15% which was the same with 2007 estimate (Federal Ministry of Health Nigeria, 2013; Federal Ministry of Health [FMoH], 2007; National Population Commission [Nigeria] and ICF International, 2009; National Population Commission [Nigeria] and ICF International, 2014).
Despite high knowledge rate and increasing overall levels of contraceptive use across the globe, existing significant gaps between the women’s desire to delay or stop childbearing and their actual use of contraception have remained unchecked. By the end of 2009, as many as 15% of the 1.4 billion of women of childbearing ages (15-49) in developing countries wanted to avoid pregnancy but are not using an effective means of contraception (Kent, 2010; Singh et al., 2009). According to World Health Statistics, approximately one in every eight currently married or in-union women aged 15 to 49 years across the globe had an unmet need for FP compared with one in four in the WHO African Region (WHO, 2011; United Nations, 2011; WHO, 2012, 2014). Unmet need for contraception is a major indicator of FP among the SDG (United Nations, 2011; WHO, 2012) and shows the gap between the reproductive intentions of currently in-union women and their contraceptive behavior (Demographic and Health Surveys [DHS], 2015; Measure Evaluation, Population and Reproductive Health [PRH], 2015; WHO, 2013). Reduction of unmet need would decrease unwanted pregnancies and abortion which is higher among poorer women, thereby improving their socioeconomic status (Gelband, 2001). The predominantly high fertility in Nigeria could be reduced significantly if unmet needs are met.
Although no linear relationship has been established between reduction of the unmet need for FP and increasing the CPR, reducing unmet need has been reported to be positively associated with increased contraceptive use and decreasing total fertility rates (TFRs) (Becker et al., 2006). Unfortunately, the two indicators are both low in Nigeria. While the 2013 CPR estimate in Nigeria is 15%, the unmet need for FP is 16% (Federal Ministry of Health Nigeria, 2013; National Population Commission [Nigeria] and ICF International, 2014) compared with Indian estimates which reduced from 25.4% in 1990 to 20.4% in 2015 in India (New, Cahill, Stover, Gupta, & Alkema, 2017).
Literature is replete with factors affecting the unmet need for FP. Women with little or no educational attainment have been reported to have higher odds for unmet needs for FP compared with those with higher education (Abdel & Amira, 2013; Choudhary, Saluja, Sharma, Gaur, & Pandey, 2009; Population Reference Bureau, 2012a). Also, unmet needs have been documented to be significantly influenced by place of residence, FP knowledge, wealth quintile, partner education, religion, number of surviving births, and media exposure (Bradley, Croft, Fishel, & Westoff, 2012; Choudhary et al., 2009; Rafiqul, Ahmed, & Mosiur, 2013; Widman, Noar, Choukas-Bradley, & Francis, 2014). Accessibility, affordability, adequacy, and proper use of FP methods have been cited also as risk factors of unmet need (Assefa & Fikrewold, 2011; Saurabh, Prateek, & Jegadeesh, 2013).
There are divergent views on the definition and measurements of unmet needs. It has been measured using assumptions which are often imprecise and controversial (Cleland, Harbison, & Shah, 2014). Until recently, the definition proffered by Westoff and Ochoa (1991) has been used in determining levels of unmet needs for contraception. The authors stated that fecund women who want their next child within the next 2 years, or currently pregnant or amenorrheic women who were using contraception at the time they became pregnant with the current/last or whose pregnancy was reported as intentional, are not to be considered as having unmet need. Critics of the Westoff and Ochoa method identified its four major limitations in that allowances were not made for married or cohabitating women who abstain from sex. Also, those never-married or formerly married women were not included in the computation; users of traditional methods are treated as nonusers because it is less effective and that male partners were excluded from computations of unmet need estimates (Cleland et al., 2006; Cleland et al., 2014).
According to United Nations, the women with unmet needs are (a) in-union pregnant women whose pregnancies were unwanted or mistimed at the time of conception, (b) in-union postpartum amenorrheic women who were not on contraceptives and whose last birth was unwanted or mistimed, and (c) all in-union fecund women who were neither pregnant nor postpartum amenorrheic, and who either want to limit family size or want to space births, but were not on any contraceptives (United Nations, 2014). Bradley et al. (2012) defined unmet need as a proportion of fertile and sexually active in-union women who are not using contraceptives but would have preferred to limit or space the birth of next child. In this study, we adopted the definition proposed by Bradley et al. which has also been reported earlier (Measure Evaluation, PRH, 2015).
The aim of the current study is to assess and compare the prevalence of contraceptive demand and unmet needs across social-demographic characteristics and autonomy of the women, and determine the distribution and determinants of unmet needs as well as the barriers to contraceptive demands in Nigeria. Women autonomy is particularly important to use of contraceptives as reported in previous studies that decision making is associated with increased likelihood of contraceptive use and a decreased likelihood of unmet need (Austin, 2015; Letamo & Navaneetham, 2015). Although estimates of unmet need and CPR in Nigeria were published earlier using the same data (National Population Commission [Nigeria] and ICF International, 2014), our study provides a reanalysis and additional estimates across the characteristics of the respondents which were not provided in the earlier report. Knowledge of the level of unmet need and its determinants could spark up interventions that could help increase contraceptive use, lower fertility and reduce the likelihood of maternal and children deaths (Khalil, Alzahrani, & Siddiqui, 2017). We hypothesized that women background characteristics and reproductive behavior would significantly influence the levels of the unmet needs for contraceptives in Nigeria. The outcomes of this study will assist in strengthening FP programming in Nigeria and other sub-Sahara African countries.
Method
Study Area
This study was carried out among women of reproductive age in Nigeria. Nigeria with an annual growth rate of 3.2% currently has about 180 million inhabitants (Akande, 2014; Fagbamigbe et al., 2015; Godswill, 2016; Population Reference Bureau, 2014). Nigeria is the most populous nation in Africa and one of the most populous countries in the world (Gupta et al., 2014; Population Reference Bureau, 2012b) with the possibility of becoming fifth largest in 2050. Nigeria has a predominant young population with a high fertility rate of 5.5% (National Population Commission [Nigeria] and ICF International, 2014). Recent nationally representative surveys have put Nigeria CPR at 15% with unmet need for FP at 16% (Federal Ministry of Health Nigeria, 2013; National Population Commission [Nigeria] and ICF International, 2014). Nigeria has 36 states and a Federal Capital Territory (political divisions), grouped into six geopolitical zones. Nigeria has more than 50 ethnic groups among which Yoruba, Hausa/Fulani, and the Igbo are the dominants while Islam and Christianity are the predominant religions practiced.
Study Design and Data Collection
We used the data from 2013 Nigeria Demographic Health Survey. This was a cross-sectional analysis of nationally representative secondary data. The data were collected from women of reproductive age residing in noninstitutional dwelling units in Nigeria. The survey used the sampling frame to detain the enumeration areas (EAs), local government areas (LGAs), states, and zones in Nigeria as prepared in the 2006 Population Census of the Federal Republic of Nigeria. The sample used for the interview was selected using a stratified three-stage cluster design spread over rural and urban areas in Nigeria. Detailed sampling design has been documented earlier (National Population Commission [Nigeria] and ICF International, 2014).
Outcome Variable
We extracted fertility, breastfeeding, and contraceptive use information provided by 27,829 women who were either currently married or in a sexual union. The contraception includes both the traditional and modern methods. The modern methods were male and female sterilization, pills, intrauterine device (IUD), injectables, implants, male condom, female condom, and lactational amenorrhea method (LAM). The primary outcomes in this study were demand and unmet need for contraceptives. We defined demand for contraceptive as the totality of needs for contraceptive, either met or unmet. Unmet need was based on recent definitions by Bradley et al. (2012), as a proportion of fertile and sexually active in-union women who are not using contraceptives but would have preferred to limit or space the space the birth of next child. In this study, we adopted the procedure in Figure 1 for computing the number of women of reproductive age, either married or in a union, who have an unmet need for FP. As shown in Table 1, breastfeeding history of the previous child was used to determine whether pregnancy occurred during breastfeeding (postpartum amenorrheic).

Definition of unmet need among currently married women.
Need and Demand for Family Planning Among Currently Married Women by Their Characteristics.
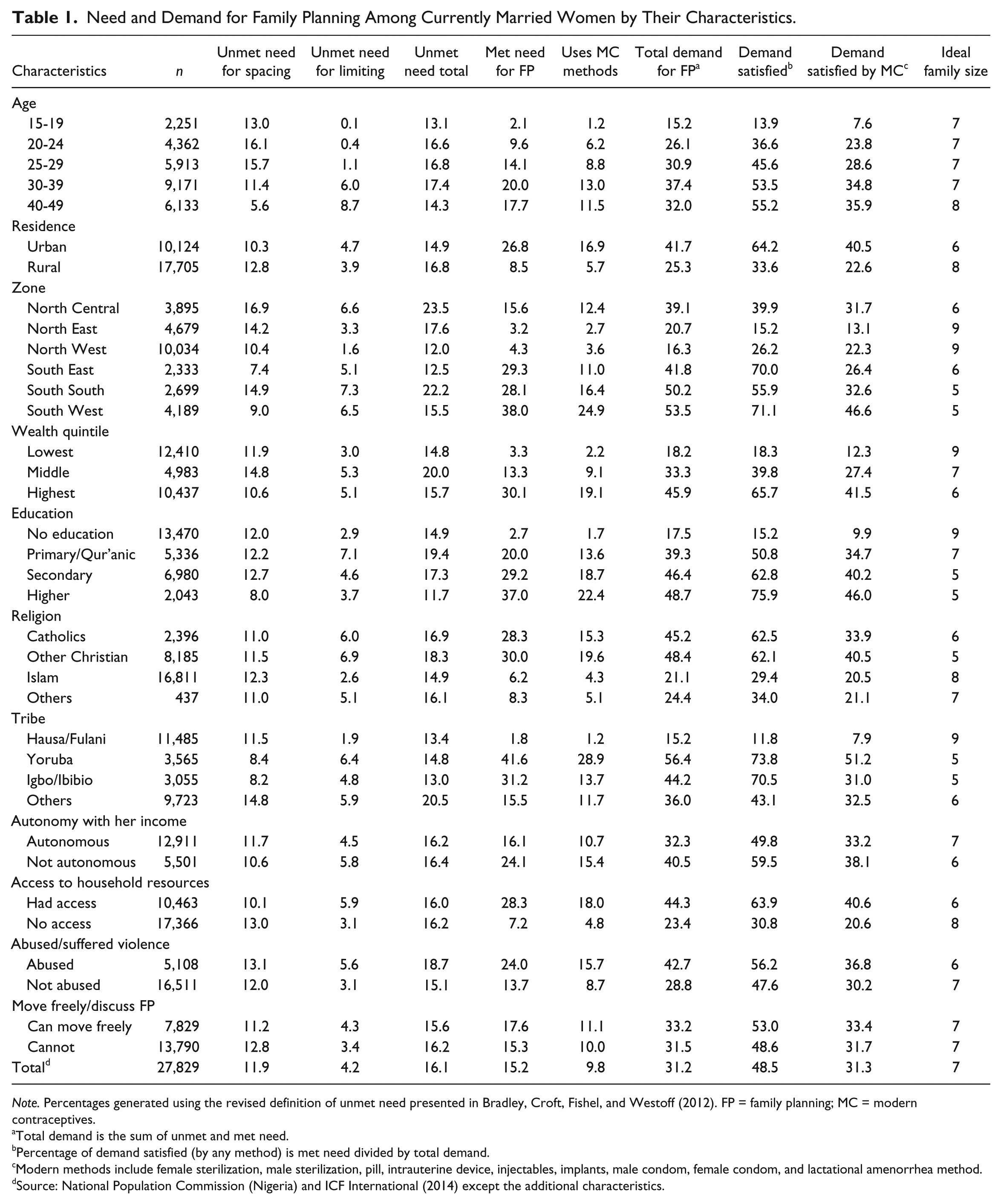
Note. Percentages generated using the revised definition of unmet need presented in Bradley, Croft, Fishel, and Westoff (2012). FP = family planning; MC = modern contraceptives.
Total demand is the sum of unmet and met need.
Percentage of demand satisfied (by any method) is met need divided by total demand.
Modern methods include female sterilization, male sterilization, pill, intrauterine device, injectables, implants, male condom, female condom, and lactational amenorrhea method.
Source: National Population Commission (Nigeria) and ICF International (2014) except the additional characteristics.
This model was used in the final computation of unmet needs, and our estimates are presented in Table 1. Details have been reported earlier (Measure Evaluation, PRH, 2015) where it was recommended that contraceptive demand and unmet needs are better computed using responses to questions on desire for additional children and desired length of birth interval; current use of contraceptive; current fecundity, pregnancy, and amenorrhea status for noncontraceptive users; number and time planning status of the current/last pregnancy for women currently pregnant or amenorrheic; and contraceptive use as at the time of the current/last pregnancy (Measure Evaluation, PRH, 2015).
Independent Variables
The independent variables include geographical zones of residence, wealth quintile, educational attainment, religion, place of residence, religion, and ethnicity. The factors have been identified in the literature to have an influence on demand and unmet need for contraceptives (Austin, 2015; Horney, 2003; Letamo & Navaneetham, 2015). To determine whether autonomy of women can explain differentials in demands and unmet need for contraceptives, we explored four variables. They are whether a woman is allowed to decide by herself how she spends her income, whether a woman has access to household resources and can make decisions, whether a woman has suffered abuse or violence, and whether a woman can move about freely without being monitored and can discuss FP.
Data Analysis
We estimated the demand for contraceptives (addition of number currently using contraceptive and number with unmet need divided by number of all in-union women), prevalence of both types of unmet needs: limiting (number with unmet need for limiting divided by number of all in-union women) and spacing (number with unmet need for spacing divided by number of all in-union women), the total met needs by modern contraception (modern contraceptive users divided by number of all in-union women), and all contraception methods (all users divided by number of all in-union women) by background characteristics using descriptive statistics. Unmet need for spacing is defined as the noncurrent use of FP despite the desire of eligible couples’ desire to delay the next birth by at least 2 years while “unmet need for limiting” occurs when eligible couples are not currently using a method of contraception and want to stop childbearing. The “total unmet need” is the addition of both the unmet need for spacing and limiting (Austin, 2015; Bradley et al., 2012; Bradley, Schwandt, & Khan, 2009; Khalil et al., 2017; PATH, 2008).
We examined the associations between having unmet needs and the demographic, socioeconomic, and reproductive profiles of the respondents using bivariate and multivariate logistic regression at 5% significance level. We used multiple response data analysis techniques to assess barriers to nonuse of contraceptives among those who had unmet demand. Data were weighted to reflect differentials in the population of in-union women in each state as recommended by DHS.
Ethical Approval
Ethical approvals for the study were obtained from the National Health Research Ethics Committee assigned number NHREC/01/01/2007 as earlier documented (National Population Commission [Nigeria] and ICF International, 2014).
Results
Among the 27,829 in-union women included in the analysis, total demand for contraception in Nigeria was 31.2%. This was made up of unmet need at 16.1% (11.9% for spacing and 4.2% for limiting) and met needs at 15.2% as shown in Table 1. The overall CPR was 15.2% while modern CPR was 9.8%. Almost a half (48.5%) of the total contraceptive demand was satisfied by any method. The 9.8% modern contraceptive prevalence reduced the total contraceptive demand satisfied by modern contraceptives to 31.3% compared with 48.5% demand satisfied by all methods. Unmet need for FP was higher among rural women compared with urban residents (16.8% vs. 14.9%) and among women who cannot move around freely without being monitored by their spouses than those who were freer (16.2% vs. 15.6%). The rate of unmet need was higher among women with either no education (12.0%), primary or Quranic (12.2%), or secondary (12.7%) compared with women with higher education at 8.0%. Also, unmet need was higher among respondents who experienced violence than those who did not (18.7% vs. 15.1%; Table 1).
Demand for contraceptives increased with age of the women but declined among those aged 40 to 49 years. The total demand in urban areas nearly doubled that of rural areas (41.7% vs. 25.3%). There were variations in zonal demand for contraceptives, highest in the South West (53.5%) and least in the North West (16.3%). While 65.7% of the demands for FP among women in highest wealth distribution were met by any method of contraceptives, only 18.3% were met among those in the lowest wealth distribution. On the proportion of total demand satisfied by modern contraceptives, 41.5% were found among the women in highest wealth distribution compared with 18.3% among those in the lowest category. Also, women who had access to their household’s resources had a higher rate of FP demand satisfied by modern contraceptives (40.6% vs. 20.6%). The average ideal number of children desired by the women was 7, and it varied slightly across women’s characteristics as shown in Table 1. Women in urban areas desired fewer children compared with those in rural areas, five among those with secondary education or higher compared with nine among those with no formal education.
Results of the bivariate logistic regression showing unadjusted odds ratios were presented in the first panel of Table 2. Younger women living in northern parts of Nigeria, practicing Islam, from rural areas, having little or no education, and from households in poorer wealth quintile, had higher odds of unmet needs. In the multiple logistic regression (reported in the second panel of Table 2), we controlled for other variables in the model and computed the adjusted odds ratios (aOR). We found younger women had higher odds of having unmet needs than the older women (aOR = 4.29; confidence interval [CI] = [3.03, 6.07]). Women residing in North East had higher odds of unmet needs compared with South West (aOR = 1.68, CI = [1.31, 2.16]). Being an Islam faithful (aOR = 1.81, CI = [1.48, 2.21]), belonging to lowest wealth distribution (aOR = 2.27, CI = [1.92, 2.68]), and having no education (aOR = 3.23, CI = [2.60, 4.02]) increased odds of unmet needs as shown in Table 2. Similarly, women who had free chance to determine how their income is spent and those who had unhindered access to family resources were 43% times more likely to have unmet needs (aOR = 1.43, CI = [1.24, 1.65]) while those who cannot move freely or discuss FP were 21% times more likely to have unmet need (aOR = 1.21, 95% CI = [1.08, 1.19]).
Determinants of Unmet Needs Among Sexually Active Women With Family Planning Needs in Nigeria.

Note. OR = odds ratio; aOR = adjusted odds ratio; CI = confidence interval; FP = family planning.
Reference.
p < .05
Using analysis of multiple response techniques in Stata, version 12, we aggregated all reported barriers to 100% and identified main barriers to contraceptive use to include opposition by the women or their spouses to use of contraception (32%), health concerns and side effects (23%), and poor awareness of sources and methods of contraceptive (15%). Other reported barriers to use of contraceptives include “leaving chances to God” (9%), “religious prohibition” (7%), and “accessibility and affordability” (6%), whereas “others” reasons indicated in Table 2 consisted of menopausal, hysterectomy, opposition by relatives or other persons, preferred/No method not available, perceived subfecundability, and inconvenient to use constituted 8% put together as shown in Figure 2.

Barriers to contraceptive use among in-union women with unmet needs.
Discussion
In this study, we investigated the distribution, associated characteristics, barriers to demand, and unmet needs of contraception among sexually active in-union women in Nigeria with the aim of providing evidence-based information that will help strengthen contraceptive programming in Nigeria. We analyzed the contraceptive information provided by currently married or in-union women in the 2013 NDHS. We found that total demand for contraceptives in Nigeria is generally low as only a third of the respondents had a demand for contraceptives. Only about a half of the demands were met while the second half was unmet. The unmet needs differed by individual, household, and community characteristics of the women surveyed. While the demands for contraceptives are low, the supply is equally low as evidenced by the level of unmet needs. This is in agreement with earlier reports (Austin, 2015). Also, the major barriers to demand and unmet need of contraceptives were found to be opposition by the women or their spouses, health concerns and side effects, and poor awareness of sources and methods of contraceptive. These findings are similar to the reported distribution of reasons preventing women from using contraceptives in sub-Sahara Africa (Darroch et al., 2011).
The estimated 16.1% unmet need for contraceptive use found in our study is higher than the rate of 9% in Botswana (Letamo & Navaneetham, 2015), at par with the reported level of 15.5% in Zimbabwe in 2005/2006 but relatively low compared with 26.6% in Zambia in 2007 (Bradley et al., 2012). The low level of unmet need in Nigeria could be ascribed to several factors including the demand and supply of contraceptives and also barriers prohibiting individuals from accessing the commodity (Austin, 2015; Ezire et al., 2013; Letamo & Navaneetham, 2015). The low unmet need in Nigeria is also accompanied by only half of the met needs. Less than one third of the women demanded contraceptives compared with 80% reported in Botswana (Letamo & Navaneetham, 2015). It is not certain whether the low HIV prevalence of 3.4% reported in Nigeria (Federal Ministry of Health Nigeria, 2013) compared with over 30% rate in Botswana (Letamo & Navaneetham, 2015) could possibly explain the differentials in contraceptive demand in the two countries. However, literature is replete on the fact that high prevalence of contraceptives may not affect HIV as most contraceptives except condoms do not prevent HIV and are more common among older women than younger women who actually have a higher contribution to HIV epidemics (Horney, 2003; Letamo & Navaneetham, 2015).
Nevertheless, the high TFR of 5.5 (National Population Commission [Nigeria] and ICF International, 2014) and the desire for large family size found in the current study are fallouts of unmet needs and low demands for contraceptives. This assertion is intuitive because low fertility levels reported in certain countries have been linked to higher demands for contraceptives (Letamo & Navaneetham, 2015), although research gap existed as to whether the purpose of the high contraceptive use was to control births or prevent HIV. We found that an average sexually active in-union woman in Nigeria desired seven children which varied across individual characteristics. However, there were unmet needs for demands for contraception to space births (Austin, 2015). Austin (2015) affirmed that contraceptive campaigns in Nigeria could only be successful if it is not targeted at limiting childbearing but rather on birth spacing and improvement of the health of the mother and child as the former might not be culturally acceptable (Austin, 2015). Across the board, unmet need for spacing was higher than the unmet need for limiting number of births.
We found the age of sexually active in-union women to be associated with levels of unmet need. While the unmet need for limiting increased as women get older, unmet need for spacing peaked among those aged 20 to 24 years and declined thereafter. This finding corroborated earlier reports (Assefa & Fikrewold, 2011; Kent, 2010), and it is an indication that FP intervention must be targeted at the girl child as they enter reproductive age so as to prevent unwanted births. Also, the unmet need for limiting was higher among urban dwellers than rural dwellers, but the reverse was the case for the unmet need for spacing. These findings are in consonance with reports elsewhere (Adebowale & Palamuleni, 2014; Assefa & Fikrewold, 2011; Letamo & Navaneetham, 2015; Saurabh et al., 2013). The likelihood of having unmet need also differed across geopolitical zones where the women reside in Nigeria.
The levels of demand for contraceptives and unmet need by the respondents also differed by their educational attainment and wealth status with less educated and poorer women been the worst hit. Conversely, those with higher economic status had higher contraceptive demand, higher demand satisfied, and lower family size desire. These findings are similar to other previous documentation (Adebowale & Palamuleni, 2014; Austin, 2015; Letamo & Navaneetham, 2015). The nearly 50% demand for FP satisfied with modern methods found in our study is low compared with indices in India which rose from 59% in 1990 to 72% in 2015 (New et al., 2017). The significance found among education, economic status, demands, and unmet need for contraceptives suggested that women should be adequately empowered not only in terms of finance but also in education so as to improve knowledge and awareness of methods and sources of contraceptives which has been cited as a major barrier to contraceptive use (Adebowale & Palamuleni, 2014).
We found higher demands for contraceptive among sexually active in-union women practicing Catholic and other Christian religions than the Muslims who coincidentally had higher odds of unmet needs compared with other religions. This is consistent with the previous finding that Muslim women, who live mostly in the Northern part of Nigeria, were less likely to have demand for contraceptives as they usually desire large families (Austin, 2015; Doctor, Findley, Afenyadu, Uzondu, & Ashir, 2013). To worsen the situation, the low contraceptive demands by these women were rarely met. As other studies have shown, the involvement of women in household decisions and particularly in decisions that affect their health can improve contraceptive demands and lower unmet needs (Austin, 2015). Women should have autonomy to spend their income and have free access to family wealth and also be allowed to move freely and discuss FP unhindered. This is of high importance as male spouses have been found to oppose the use of contraceptives (Adebowale & Palamuleni, 2014).
Regarding barriers to contraceptive demands, we found opposition by either the women or their spouses to use of contraception, health concerns and side effects, and poor awareness of sources and different methods of contraceptive to be the commonest reasons why women in Nigeria have unmet demand and in some cases have no demands for contraceptives. Similar reasons have been reported elsewhere (Adebowale & Palamuleni, 2014; Austin, 2015; Bradley et al., 2012; Bradley et al., 2009; Letamo & Navaneetham, 2015; Sedgh & Hussain, 2014) although with different magnitudes. Opposition to the use of contraceptives by women and their spouses constituted a great challenge to use of contraceptives in Nigeria. This is probably due to the fact that they both wanted large family sizes. This suggests that men are not push-overs in sexual and reproductive outcomes of their spouses. Sexual and reproductive health programming should target both men and women for meaningful changes to be achieved.
The reported health concerns and side effects to use of contraceptives could lead to eventual discontinuation of methods by users and none uptake of methods by nonusers. Therefore, there is an urgent need for proper reorientation of women, their spouses, and the community at large through a functional contraceptive education and promotion, and behavioral change communication programs as the current high knowledge of contraceptives in Nigeria did not translate to usage. The education and promotion will overcome the barriers of carefree attitudes, leaving chances, religious prohibition, myths, misconceptions, and hearsays. We found accessibility and affordability of contraceptives as other threats to increased demand and met contraceptive needs in Nigeria. This is consistent with reports of a Burkina Faso study (Adebowale & Palamuleni, 2014) and an earlier study in Nigeria (Ezire et al., 2013; Fagbamigbe et al., 2011). The Gates Foundation has also identified “insufficient donor and funding in developing countries, lack of appropriate FP methods that meet users’ needs, unreliable distribution systems, cultural and knowledge barriers” as hurdles to scale in eradicating unmet needs (The Gates Foundation, 2015).
Strengths and Limitations
The use of DHS-approved computation of unmet needs has given credence to our findings compared with other estimates before now. However, the exclusion of sexually active but not in-union women in the computations might have strongly underestimated the burden of unmet need for contraceptives. All the indicators used in computing the demands and unmet needs were self-reported by the respondents which might have suffered recall bias. However, the largeness of the data, its national representativeness as well as the high response rates coupled with pretested, consistent, and standardized data collection procedures might have eliminated the potential effect of any recall bias.
Conclusion
Although unmet need among the women was low, the met needs and the total demand for contraceptives were also low. The poor, uneducated, and rural women are at greatest risk of low contraceptive demands and unmet needs. This poses a damaging effect on attainment of good sexual and reproductive health for women. Despite high knowledge of contraceptives in Nigeria and the political will by the Nigeria government, CPR has remained low at 15%. Considering the high fertility desire among the women and the low contraceptive demand, the low unmet need in Nigeria should not be mistaken for a good progress in FP. The success of FP programming in Nigeria is better measured using CPR, level of contraceptive demands, and the proportions of demand satisfied.
Recommendation
To achieve a remarkable and desired increase in the CPR, cost barriers should be removed so that the very poor can have unlimited access to contraceptives provided all other barriers have been dealt with effectively. Government and other stakeholders should do more in ensuring accessibility and affordability as well as ensuring an increased effectiveness of FP programming in Nigeria. There is need to reverse the unabated population growth in Nigeria through fertility control. This can only be achieved by combined efforts targeted at encouraging households to lower their desired number of children which would, in turn, improve demands for contraceptives while unmet needs for contraceptives are been eliminated. For Nigeria to meet the goal of 36% contraceptive prevalence rate by 2018, interventions to enhance formal education and improve women’s decision-making power should be embraced urgently.
Footnotes
Acknowledgements
The authors acknowledge the National Population Commission (Nigeria) and ICF International for granting them access to the data. They also acknowledge the technical support received from the Consortium for Advanced Research Training in Africa (CARTA). CARTA had trained the first author in research methodologies.
Author Contributions
AFF conceived and designed the study, analyzed and wrote the results, and partook in writing the introduction, methodology, and discussions. ARF and ESA partook in study design and writing of the introduction and discussions. All authors proofread the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.