
Abstract
The objective of the study wasto identify factors associated with use of services for adolescent mental health problems in an Australian community-based sample. Logistic regression analysis was conducted on data collected from 636 parents and their adolescent child to identify individual and family variables predicting parent report of service use for mental health problems in the adolescent 12 months later. The services most reported by parents to have been accessed were school-based ones. Multivariate analysis found that the following were associated with service use 12 months later: the adolescent being female, parent report of peer problems and hyperactivity, single-parent household, the parent being Australian born, and prior service use by the adolescent. Parental overcontrol was associated with reduced likelihood of service use at follow-up. No association was found between service use at follow-up and parent gender, socioeconomic status, number of siblings, parent psychopathology, family social connectedness, and prior service use by the parent. No association was also found for family environment factors, parental attachment, or for the adolescent’s emotional competence or use of social support. The results indicate that families provide a potential target for interventions aimed at increasing use of professional services for adolescent mental health problems.
Introduction
Adolescence has been identified as a critical life stage in the development of mental health problems (Patel, Flisher, Hetrick, & McGorry, 2007), as mental disorders commonly have their first onset during this stage of life (Kessler et al., 2005). Increasing autonomy and individuation from the family are defining features of adolescence as a developmental period (Allison & Sabatelli, 1988), resulting in reduced dependence on the family unit. Yet, research shows that adolescents continue to depend on parents as a primary source of support and advice throughout this developmental phase (Steinberg, 2001). It is evident that pre-adolescent children often rely upon a significant adult (usually a parent) to facilitate service use should they experience a mental health problem (Kazdin, Holland, & Crowley, 1997). However, this reliance is likely to reduce as a young person matures into adolescence. Nonetheless, family and parent factors (herein referred to in combination as family factors for simplicity) are still likely to be influential in this process, although which of these factors and how has yet to be established.
A demonstrated gap between mental health service need and service use has resulted in a body of literature examining what factors in addition to need influence whether a young person receives mental health services (Logan & King, 2001; Rickwood, Deane, & Wilson, 2007). Proposed models of the process of accessing mental health services for a child and/or adolescent derive from existing models of adult help-seeking, adapted to incorporate features of the family (Costello, Pescosolido, Angold, & Burns, 1998; Logan & King, 2001; Srebnik, Cauce, & Baydar, 1996). Although quite diverse and often somewhat complex, these models identify a number of common factors. To varying degrees, they derive from the behavioral model of health service use developed by Andersen and colleagues (Andersen, 1995; Andersen & Newman, 1973). The Andersen model classifies individual determinants of service use into three broad categories: need-related, predisposing, or enabling (or inhibiting) factors (Andersen, 1995; Andersen & Newman, 1973).
Figure 1 provides a visual representation of some of the factors common to the three identified models of professional service use for mental health problems in young people (Costello et al., 1998; Logan & King, 2001; Srebnik et al., 1996), organized according to Andersen’s model. Examination of the influence of these identified factors has yet to be rigorously conducted with a sample restricted to adolescents, although a number of studies have used samples that included both children and adolescents (e.g., Burns et al., 2004; Ford, Hamilton, Meltzer, & Goodman, 2008). Furthermore, a number of existing studies have not controlled for the young person’s mental health symptoms in examining the influence of predictors on youth service use (e.g., Villagrana, 2010). As many of these variables are known risk factors for the development of mental health problems in young people (Fergusson, Horwood, & Lynskey, 1994; Hoeve et al., 2009), results may be confounded by the indirect influence that these factors have on the development of the problems for which help is being sought.

Factors identified in existing literature as associated with use of services for adolescent mental health problems, organized according to the Andersen and Newman (1973) model.
There is some existing Australian research investigating predictors of service use for adolescent mental health problems (Fallon & Bowles, 2001; Lyneham & Rapee, 2007; Sawyer, Miller-Lewis, & Clark, 2007); however, these studies have a number of limitations, such as investigation of only a small number of predictors (Lyneham & Rapee, 2007; Sawyer et al., 2007), and investigation of help-seeking for a range of problems rather than mental health problems specifically (Fallon & Bowles, 2001). A significant portion of this literature has also assessed help-seeking intentions of young people as the outcome variable (Rickwood, Deane, Wilson, & Ciarrochi, 2005), which is only weakly correlated with actual help-seeking behavior (Wilson & Deane, 2005).
Need-Related Variables Included in Models of Service Use for a Young Person
Models of service use for young people emphasize the importance of the parents’ perception of need in this process (Costello et al., 1998; Logan & King, 2001; Srebnik et al., 1996). Parent perception of need is very important in young children because they are unlikely to have an understanding of what emotional or behavioral symptoms may possibly benefit from professional intervention, or knowledge of professional services appropriate and/or available (Costello et al., 1998; Srebnik et al., 1996). Adolescents, however, may have some understanding relating to mental health. The degree to which parents’ perception of need prevails over the perception of the adolescents in influencing the professional help-seeking process for the adolescent has yet to be clearly established (Costello et al., 1998). Parents potentially could be the initiator of help-seeking from professional services once they perceive a need in their adolescent child, or they may be influential in encouraging the adolescent to seek help independently (Logan & King, 2001). The presence of identifiable antecedents to psychological distress, such as negative life events, also has the potential to generate perception of need in either the adolescent or other family members.
Predisposing Factors Included in Models of Service Use for a Young Person
Sociodemographic factors
In addition to sociodemographic characteristics of the young person such as age and sex, models of service use for young people also include socioeconomic characteristics of the family such as ethnic background and income. Adolescent girls have been shown to be more willing to access professional services for mental health problems than adolescent boys (Rickwood et al., 2005). However, once the presence of mental health symptoms has been controlled for, an effect for the sex of a young person on mental health service use has not been demonstrated (Angold et al., 1998; Costello et al., 1998). Sociodemographic characteristics of the family, such as the parents’ income and education, are identified by the models proposed by Costello et al. (1998) and Srebnik et al. (1996) in the process of accessing help for children and adolescents. Logan and King’s (2001) model identifies the family’s instrumental resources (e.g., money, time, available transport) as influential in parent facilitation of service use for adolescent mental health problems. Low socioeconomic status (SES) has been shown to be associated with service use in other countries, once mental health symptoms of the young person were controlled for (Feehan, Stanton, McGee, & Silva, 1990; Zahner & Daskalakis, 1997). An Australian study, however, failed to find a significant association between parent educational achievement or household income and use of services for adolescent mental health problems (Sawyer et al., 2007).
Being from an ethnic minority group has been identified as a potential barrier to use of professional services by young people (Rickwood et al., 2007), and has been shown to predict lower use of services for young people in a number of countries. Studies from the United States have shown that being from an ethnic minority is associated with reduced use of mental health services for young people (Zahner & Daskalakis, 1997; Zimmerman, 2005), although this association has not always been demonstrated (Cohen & Hesselbart, 1993; Teagle, 2002). One study from the United Kingdom also found that ethnicity was associated with service use for young people (Ford et al., 2008), and two studies from the Netherlands also failed to find an effect for ethnicity (Douma, Dekker, Ruiter, Verhulst, & Koot, 2006; Verhulst & van der Ende, 1997). To our knowledge, no studies have investigated whether ethnic background is associated with service use for an adolescent in an Australian community-based sample while controlling for mental health symptoms.
Family illness variables
The models proposed by Costello et al. (1998) and Logan and King (2001) both include family history of psychopathology, with the Logan and King model suggesting the family history of service use operates independently of family history of psychopathology. Srebnik et al. (1996) also include parent psychopathology, but differ in specifying it as need-related, in that its influence is exerted through the parents’ perception of the young person’s behavior as problematic. Indeed, the presence of mental health symptoms in a parent has been shown to predict service use for a young person (Feehan et al., 1990; Mojtabai & Olfson, 2008), as has a family history of use of mental health services (Zimmerman, 2005). These associations, however, have not been consistently demonstrated once mental health symptoms in the young person are controlled for (Jensen, Bloedau, & Davis, 1990; Teagle, 2002).
Social structure variables
Predisposing variables relating to social structure can be further broken down to those within the family and those relating to the social networks within which the family is embedded (Costello et al., 1998). A family’s social structure can influence the help-seeking process through the availability of social supports as well as through the transmission of social norms. Family size and structure are included in the models by Costello et al. (1998) and Srebnik et al. (1996). Structural features of the family shown to increase the likelihood of service use for a young person include being from a single-parent household (Ford et al., 2008; Zahner & Daskalakis, 1997), and the young person having fewer siblings (Ford et al., 2008; Jensen et al., 1990). The size of a family’s social network can also be identified as a factor that could predispose the family to accessing services for an adolescent (Costello et al., 1998).
Enabling and Inhibiting Factors Included in Models of Service Use for a Young Person
Family environment variables
All three identified models of service use for young people include factors relating to the family environment or parent–child relationship; however, again they differ in how they propose these factors exert their influence. Logan and King (2001) and Srebnik et al. (1996) both categorize factors of environment of the family or parent–child relationship quality as need variables, in that they impact a parent’s ability to recognize when the young person is experiencing a problem. Alternately, the model proposed by Costello et al. (1998) categorizes these characteristics of the family as enabling variables, because a function of the family unit is to provide social and instrumental support to its members. This approach is more in line with Andersen’s original model, which views social relationships as enabling resources (Andersen, 1995). As there is no established guideline regarding what problems experienced by an adolescent are best managed within the family and which would benefit from professional help, these decisions are guided by family norms (Costello et al., 1998; Srebnik et al., 1996). Existing studies investigating the influence of family environment and parent–child relationship quality on service use have produced conflicting results (Ezpeleta et al., 2002; Ford et al., 2008; Zwaanswijk, Van der Ende, Verhaak, Bensing, & Verhulst, 2005).
Coping style of the young person
The model by Costello et al. (1998) includes the coping style of both the young person and the parent as influential in the help-seeking process. Australian research focused on ascertaining barriers and enablers to adolescent help-seeking has identified the adolescent’s emotional and social competence as important in this process (Rickwood et al., 2005). Emotional competence refers to an individual’s ability to recognize and describe emotions in themselves and others, as well as their capacity to understand emotions and manage them effectively (Salovey & Mayer, 1989). Low emotional competence has been shown to be associated with reduced willingness to seek help from professional sources for emotional problems (Ciarrochi, Wilson, Deane, & Rickwood, 2003). This association was found by another study to be mediated by the adolescent’s level of social support (Ciarrochi, Deane, Wilson, & Rickwood, 2002), which has been shown previously to be associated with help-seeking by adolescents for emotional problems (Rickwood & Braithwaite, 1994). Therefore, in addition to the availability of social resources as indicated by the social structure, an adolescent’s capacity to recognize when use of social supports may be beneficial, as well as the adolescent’s capacity to use these supports appropriately, may potentially enable or inhibit use of professional services for mental health problems.
Summary
In summary, a large number of family factors are identified as influential by models of service use for a young person for mental health problems. However, whether these factors play a role in service use for adolescents specifically has yet to be established. Furthermore, very little research has been conducted using an Australian sample, in which characteristics of the mental health care system differ from those in other countries. The current study seeks to address these gaps in the existing literature by evaluating family and individual factors identified by models of service use for young people in an Australian community-based longitudinal study of adolescents.
Based on existing evidence, as well as proposed models of service use for young people, it was hypothesized that service use would be predicted by the adolescent being female, parent report of mental health problems in the adolescent, lower SES, single-parent household, the adolescent having fewer siblings, being from an ethnic minority, parent psychopathology, adolescent use of social supports, and previous service use by family members. As current evidence regarding the association between factors relating to the family environment and service use is contradictory, and investigation of the impact of the family’s level of social support on service use is preliminary (Bussing et al., 2003), examination of the impact of these factors on service use at follow-up by the current study was exploratory.
Method
Data used for the current study was collected as part of a longitudinal evaluation of a school-based intervention (Australian Clinical Trial Registry Number 012606000399594). The Resilient Families Intervention (RFI) was designed to support young adolescents and families to promote the young person’s psychological well-being during his or her high school years. More detailed description of this program and the evaluation study can be found elsewhere (Toumbourou, Gregg, Shortt, Hutchinson, & Slaviero, 2013). Briefly, 39 schools in Melbourne Victoria were approached to participate, 24 of which agreed. Participating schools were randomized into either the intervention or control group. All students in Year 7 in 2004 were invited to participate in the study, with new students joining this cohort in Year 8 in 2005 also invited to participate at Wave 2. The adolescents completed surveys in class time. Parents and carers (hereafter referred to in combination as “parents”) were also invited to participate via a mail-out survey. Ethical approval was obtained from the University of Melbourne’s Human Research Ethics Committee, as well as from relevant education bodies. Parents gave written consent for their adolescent and themselves and adolescents provided written consent for each time point that data were collected. Participants were followed up at Wave 2 (Year 8, 2005), approximately 1 year after Wave 1. Further waves of data were collected for the initial RFI evaluation, but were not analyzed for the current study.
Participants
Of the 4,404 adolescents eligible to participate in the study, 2,128 completed both Waves 1 and 2 surveys. Completed surveys for both waves were returned by 1,160 parents. Data analyzed for the current study were from a subgroup of 636 parent–child dyads for whom complete data were available at both Waves 1 and 2 of the study. The average age of the adolescents was 12.3 years, and 54.25% of the adolescent participants were female. Further descriptive statistics on the sample can be seen in supplemental file 1a.
Questionnaires
Separate survey packages were provided to parents and adolescents who were similar for the two waves of the current study. The parent and adolescent survey packages included questions regarding demographics, the adolescent’s emotional and behavioral problems, and a range of parenting and family environment variables. Adolescents also responded to questions relating to a range of individual competencies identified in existing literature as associated with use of services for mental health problems. An overview of included scales can be seen in supplemental file 1a.
The outcome variable for the current study was parent response at Wave 2 to the question: “In the last 12 months, has your Year 8 adolescent received professional assistance for any emotional or behavioral problems (e.g., problems with attention, anger, fears, worries, sadness)?” A follow-up open-ended question was asked to parents responding “yes” to this first question: “If yes, please describe.” Predictor variables were drawn from Wave 1 data from both parents and adolescents.
Demographic information gathered from parents included their gender, age, and relationship to the child (parent or carer). Parents also provided information about the structure of the household (i.e., whether both parents of the adolescent lived in the house, or whether the family was a step-family, single-parent family, or other), the annual household income, the highest level of education of the parent and any partner, and whether or not they were born in Australia as an indicator of ethnicity. Although indigenous status as an additional indicator of cultural background was assessed in the survey, too few participants identified either themselves or a family member as being of Aboriginal or Torres Strait Islander descent to allow for meaningful comparisons to be made (Toumbourou et al., 2013). Demographic information gathered from adolescents included their gender, age, and the number of siblings they have.
Emotional and behavioral problems in the adolescent were reported by parents on the Strengths and Difficulties Questionnaire (SDQ; Goodman, 2001; Zimmerman, 2005). The Emotional Symptoms, Conduct Problems, Hyperactivity, and Peer Problems subscales were included in the current study. The adolescents completed the Conduct Problems subscale of the self-report version of the SDQ as a measure of behavioral problems, and the Center for Epidemiologic Studies–Depression scale (CES-D; Radloff, 1977), as an indicator of emotional problems. The adolescents also responded to the question, “Have you been bullied recently (teased or called names, had rumors spread about you, been deliberately left out of things, threatened physically, or actually hurt)?” on a 4-point scale as an indicator of the degree to which they had recently been bullied. Negative life events were assessed by adolescents reporting whether or not they had experienced 1 of 12 adverse events in the previous 6 months (see supplemental file 1b for a summary).
The adolescent’s perception of family conflict and parental attachment were assessed with scales drawn from the Communities That Care (CTC) survey, which has been validated previously (Arthur, Hawkins, Pollard, Catalano, & Baglioni, 2002; Glaser, Horn, Arthur, Hawkins, & Catalano, 2005). Parental attachment combined the two subscales of Attachment to Mother and Attachment to Father for the current analysis. Parental overcontrol measured with a scale developed for the RFI adapted from the Parental Bonding Instrument (Parker, Tupling, & Brown, 1979), assessing the degree to which the adolescent felt that his or her parents exert excessive psychological and behavioral control over them (see supplemental file 1b).
Adolescent emotional competence and use of social supports were assessed with scales developed for the RFI, which drew items from existing scales. The emotional competence assessed the degree to which the adolescent is able to effectively manage negative emotions, with items drawn from the Self-Efficacy Questionnaire for Children (Muris, 2001) and the emotional control scale of the CTC. The Social Support Scale was made up of items from the “Seeking Social Support” subscale of the Self-Report Coping Strategies subscale, with one item omitted (Kochenderfer-Ladd & Skinner, 2002). This scale measured the degree to which the adolescent used seeking social support as a strategy for coping with problems (see supplemental file 1b for descriptions of these two scales).
Parent report of the family environment was measured with the Cohesion and Conflict subscales of the Family Environment Scale–Third Edition (FES-III; Moos & Moos, 2002). The FES-III is a measure of the socio-environmental characteristics of a family, with the Cohesion subscale assessing the degree of support, commitment, and help family members provide to one another, and the Conflict subscale assessing the amount of expressed anger or conflict within the family. Parents also completed a shortened version of the Depression, Anxiety, and Stress Scale (DASS; Lovibond & Lovibond, 1996) adapted for the RFI study as a measure of mental health symptoms in the parent. Parents were also asked “If in the last 12 months have either you (or your spouse/partner) sought professional assistance for any emotional problems (e.g., anxiety, depression, anger) or problems in your relationships (marital relationship, family relationships)?” to assess prior service use by a parent. Adolescent and parent perception of the family’s level of social connectedness were measured with scales developed for the RFI that assessed the degree to which the family is involved with community groups outside of the family (see supplemental file 1b).
Statistical Analysis
Logistic regression was used to examine the association between adolescent-and parent-reported predictor variables at Wave 1 and parent report of professional service use for the young person’s emotional and/or behavioral problems in the past 12 months at Wave 2. Univariate analysis was conducted for all predictor variables, then multivariate analysis was conducted with all predictor variables run in the model simultaneously. Odds ratios and confidence intervals were generated to provide comparison of relative effects, with interquartile odds ratios calculated for continuous predictor variables to allow for comparison with categorical variables. Interquartile odds ratios provide an estimate of the relative likelihood of those upper and lower quartiles of the distribution of continuous variables, thereby compensating for the scale-dependent characteristic of the statistic (Mackinnon, 1992).
Parent report of household income and education level were combined to generate a single variable of SES for analysis. This variable was an average of standardized scores for parent and spousal education and four levels of household income. The household structure variable was also dichotomized to parent–parent versus “other” for analysis. Because two parents returned surveys for 54 of the adolescents, a multiple regression was run adjusting for clustering at the family level to control for multiple responders. This analysis adjusted for family clustering produced findings that reflected those of the model unadjusted for family clustering. Results described here are from the unadjusted analysis. Statistical analysis was conducted using STATA version 11.
Results
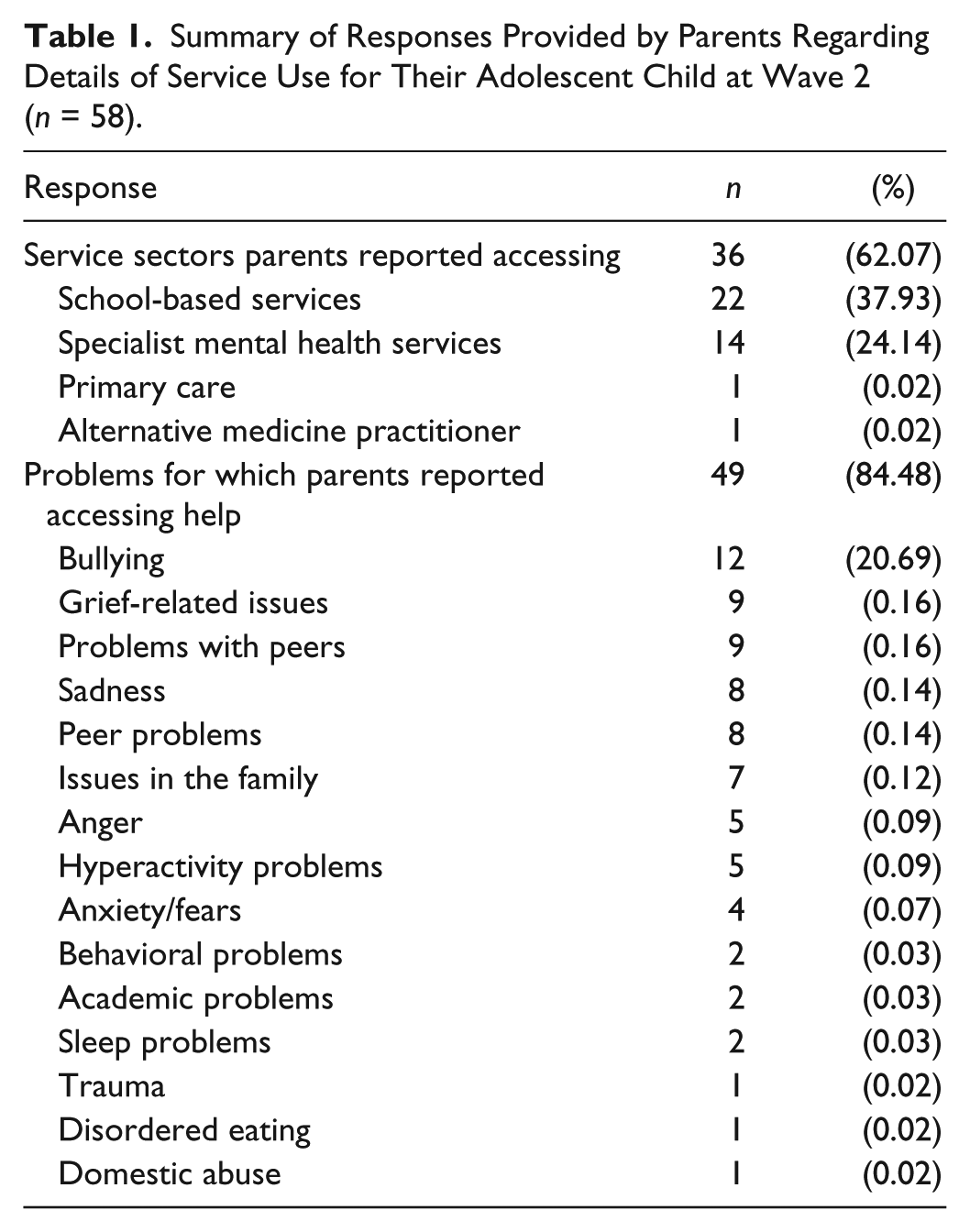
In all, 59 of the 636 parents in the sample reported accessing services for their adolescent’s emotional or behavioral problems at Wave 2. Of this number, 58 gave an answer to the follow-up question asking for details, with responses describing the source of help accessed, giving a brief description of the problems the adolescent was experiencing, or both. Two parents reported accessing more than one source of help, and 13 described more than one type of problem for which help was accessed. Table 1 provides a summary of responses given by parents.
Summary of Responses Provided by Parents Regarding Details of Service Use for Their Adolescent Child at Wave 2 (n = 58).
Bivariate correlations between all variables included in the analysis indicated that multicollinearity was not present in the data, and the correlation matrix for all variables can be seen in supplemental file 2. Results from the univariate and multivariate regressions are shown in Table 2. Hosmer–Lemeshow goodness-of-fit tests were non-significant for all models, indicating that the models were an appropriate fit for the data (Fagerland, Hosmer, & Bofin, 2008).
Odds Ratios for Longitudinal Associations Between Wave 1 Predictors and Parent Report of Accessing of Professional Services for Emotional or Behavioral Problems in the Adolescent at Wave 2.

Note. OR = odds ratio; CI = confidence interval; CES-D = Center for Epidemiologic Studies–Depression; DASS = Depression, Anxiety, and Stress Scale.
<0.05, **<0.01, ***<0.001.
Once all predictor variables were included in the model, factors that were significantly associated with increased use of services for an adolescent were the adolescent being female, parent report of hyperactivity and peer problems, being from a single-parent family, the parent being Australian born, and use of services for the adolescent in the previous year. Adolescent report of high parental overcontrol was associated with reduced odds of receiving services once the influence of all other variables was taken into account.
Need factors for which no significant association was found with service use at Wave 2 in the multiple regression model were adolescent report of depressive symptoms, behavioral problems, being bullied and negative life events, and parent report of emotional and conduct in the adolescent. No association was found between service use at follow-up and predisposing factors of sex of the parent, SES, number of siblings, parent psychopathology (DASS score), family social connectedness, and previous use of mental health services by the parent. No association was found for enabling factors of the family environment, adolescent attachment to parents and family conflict, the adolescent’s emotional competence or use of social support, parent report of family conflict and cohesion, parent and adolescent report of social connectedness, parent use of services in the previous year, SES, and exposure to the RFI.
Discussion
Results from the current study demonstrate that, of a large number of predisposing, enabling, and need-related variables investigated, the adolescent being female, parent report of hyperactivity, and peer problems, prior service use by the adolescent, being from a single-parent family, and the parent being Australian born predicted service use at 12-month follow-up. Adolescent report of parent overcontrol was also found to be associated with a reduced likelihood that the adolescent would receive services once other variables were controlled for. School-based services were the predominant source of professional help reported by parents as accessed, suggesting these services may be particularly important in both addressing problems in young adolescents, and as a potential referral source for when problems require more specialized services.
That parent report of hyperactivity problems in the adolescent was found to predict service use over and above the presence of other mental health symptoms suggests that the parent’s perception of clearly observable and potentially disruptive problems is particularly important for professional service use. This finding supports those of previous studies that have found that the impact of a young person’s mental health problems on the parent is an important predictor of service use (Angold et al., 1998; Ford et al., 2008). The association found here between the parent’s report of peer problems and use of services indicates that parents may be more likely to recognize when their adolescent child is experiencing mental health problems when there is an identifiable antecedent to them. This influence, however, may be more prominent in a school setting, considering that school-based services were the predominant professional source of help. That adolescent report of bullying does not retain significance in the full model also suggests that parents continue to have the predominant influence in the decision to access help for an adolescent of this age.
Of predisposing variables examined in this study, the adolescent being female, being from a single-parent family, being from the dominant ethnic group, and previous service use by the adolescent were found to increase the likelihood of professional help-seeking. The finding of greater service use by females is consistent with previous research showing that they are more willing to seek help and may also indicate that parents are more predisposed to seek services for them.
Although the association between being from a single-parent family and service use for young people is relatively established (Verhulst & van der Ende, 1997; Zahner & Daskalakis, 1997; Zimmerman, 2005), the mechanisms underpinning this association have yet to be examined empirically. One hypothesis is that when there are less social resources available within the family, the family is more likely to seek out professional help. That no association was found between the level of social connectivity of the family and service use suggests that this association is unlikely to be mediated by the availability of informal help sources to the family. Furthermore, as measures of the adolescent’s social competence and use of social support for coping were not related to service use, it is likely that service use by single-parent families is driven more by the parent than the adolescent.
Being from an ethnic minority is an established barrier to service use; however, this is the first study to our knowledge to demonstrate that this in an Australian community-based sample using service use behavior as an outcome measure. Research from the United States suggests that the influence of culture operates through beliefs about mental health (Lau & Takeuchi, 2001); however, other factors that may contribute to this association include English language difficulties, lack of awareness of services available, and a perception that services are unlikely to be able to accommodate diverse cultural beliefs and practices. Interestingly, only the adolescent’s history of service use, and not the parent’s, predicted professional help-seeking, suggesting that knowledge of adult mental health problems and services does not necessarily generalize to understanding about adolescent mental health problems and appropriate help sources. This result, however, may be a reflection of the substantial use of school-based sources reported in the current study.
The only enabling variable identified as associated with service use was the adolescent’s report of parent overcontrol. Although this factor has been shown to be associated with an increased risk for adolescent emotional problems (McLeod, Weisz, & Wood, 2007), this is the first known study finding that this variable is a predictor of lower service use. This finding identifies parental overcontrol as an important focus for early intervention and prevention efforts for mental health problems in adolescents. It also highlights the importance of developing a clear representation of how an overcontrolling, or more importantly an “appropriately controlling,” parenting style is operationalized to inform such interventions.
The current study has a number of limitations that should be acknowledged. First, reliance solely upon parent report of service use means that any service use initiated by the adolescent or other referral source that may have occurred without the parent’s knowledge is not counted. The study would have also benefited from a more detailed measure of service use, including systematic assessment of types of help accessed for the adolescent’s problems, as well as the types of problems for which help was sought. Another limitation is the lack of uniformity in parent-and adolescent-reported measures. Validated, parallel measurement tools designed for multiple informants of family environment and parenting factors, as well as for the adolescent’s mental health symptoms would have improved the quality of this study. Furthermore, although the current study used a community-based sample, the small proportion of eligible parents who participated in the study limits generalizability. Despite these limitations, the findings improve understanding of professional help-seeking in the Australian context, by using a community sample and a diverse range of predictor variables. Use of a longitudinal design is also a strength of the current study.
In conclusion, findings from the current study indicate that, as proposed by existing models of service use for mental health problems in young people, factors relating to the family are important. These findings suggest that the family is a valuable potential target for interventions aimed at improving service use.
Footnotes
Declaration of Conflicting Interests
A potential conflict is noted in that Professor Toumbourou holds intellectual property responsibility for the Resilient Families intervention.
Funding
The data collection was completed with funding from the National Health and Medical Research Council (Project Grant Nos. 251721), the Alcohol Education and Rehabilitation Foundation, and the Grosvenor Settlement Philanthropic Trust. Professor Toumbourou was supported by a VicHealth Senior Research Fellowship and Professor Jorm was supported by an NHMRC Australia Fellowship. Parent recruitment was supported by pro bono work from the staff of Beaton Wellmark. The authors declare their independence from the funders and from any tobacco, alcohol, pharmaceutical or gaming industries or anybody substantially funded by one of these organizations. The funding bodies impose no contractual constraints on publishing.