
Abstract
This article explores the strategic challenges associated with launching and managing a cross-sector collaboration that confronted Aligning Forces for Quality of South Central Pennsylvania (AF4Q-SCPA), which was established to improve health care quality in partnerships with patients, providers, employers, and community organizations. It draws upon the work of scholars from the fields of public administration, public health, organizational theory, and business strategy. It synthesizes previous contributions to create a new model called the Collaboration Cube, which links the likelihood of success of initiatives to intended outcomes and collaborative structures. With respect to methodology, it takes an inductive approach and uses the insights from the case study to offer nine generalizable propositions that readers may find relevant to collaborative organizations operating in any field. Finally, the article offers thoughts about possible lines of future research.
Keywords
In recent decades, decision makers in all professions and all sectors have become increasingly aware of the growing complexity in the environments that confront their respective organizations (IBM Institute for Business Value, 2010). In that context, collaboration among some combination of participants from the government, for-profit, and not-for profit sectors has become an accepted way of tackling tough issues. Bryson, Crosby, and Stone (2006), scholars in the field of public administration and experts in this form of organization, offer the following characterization:
We . . . define cross-sector collaboration as the linking or sharing of information, resources, activities, and capabilities by organizations in two or more sectors to achieve jointly an outcome that could not be achieved by organizations in one sector separately. (p. 44)
However, they offer the following caveat.
[C]ross-sector collaborations are difficult to create and even more difficult to sustain because so much has to be in place or work well for them to succeed. The challenge of designing and implementing effective cross sector collaboration is daunting . . . The normal expectation ought to be that success will be very difficult to achieve . . . (p. 52)
The challenges associated with launching and effectively managing an organization dedicated to initiating cross-sector collaboration (CSC) among a range of parties are illustrated in the experiences of Aligning Forces for Quality of South Central Pennsylvania (AF4Q-SCPA), an organization that was established to improve health care quality in partnerships with patients, providers, employers, and community organizations. AF4Q-SCPA came into existence in 2007, when a multistakeholder community group led by the WellSpan Health System of York, Pennsylvania, successfully secured funding from the Robert Wood Johnson Foundation (RWJF) under its Aligning Forces for Quality grant program. Under the terms of the grant, AF4Q-SCPA was expected to initiate collaborative processes among health care stakeholders to help influence the determinants of community health. AF4Q-SCPA had early success and was subsequently awarded three additional grants: two for a term of 2 years, and a third for a term of 3 years. In each instance, those grants served as the primary source of funding for the collaborative, representing approximately 90% of its operating budget. The remaining resources came from in-kind contributions by AF4Q Leadership Team members including WellSpan Health, Family First Health, Memorial and Hanover Hospitals, and others. By 2013, AF4Q-SCPA had managed to attract participation by a broad range of organizations. Nevertheless, as of 2013, the fourth and final grant from RWJF was slated to terminate in 2015. Given their historical dependence on those grants, the Leadership Team of AF4Q-SCPA had to decide whether to shut-down the organization or to find a path forward; if the latter, the team had to formulate a medium-to-long-term strategy.
In the name of transparency and to promote clarity, the authors of this article acknowledge that they were asked by AF4Q-SCPA to serve as consultants; that is, they received compensation to provide background information, a framework for analysis, and suggestions that would help the Leadership Team better weigh their strategic options. In that capacity, during the first 6 months of 2013, they met 3 times with the AF4Q-SCPA staff; conducted 17 separate interviews with key stakeholders; read documents generated by AF4Q-SCPA; reviewed publicly available secondary data sources; reviewed interorganizational network, cross-sector collaborative, community health partnership, and business strategy literatures; and presented the Leadership Team with a written report that summarized their findings.
The purpose of this article, however, is neither to replicate the final report the authors submitted to AF4Q-SCPA nor to lobby for the recommendation made therein. Instead, the goal is to share insights from that work about the challenges confronting AF4Q-SCPA that may be of use to researchers and practitioners involved in the health care field or in other settings.
This study primarily takes an inductive approach to exploring issues. That is, it does not start with a set of hypotheses but instead analyzes the experience of AF4Q-SCPA within the context of theoretically based frameworks of analysis to offer some generalizable propositions. Of note, the frameworks used in the article reflect the theory-building and empirical work of academic leaders in the fields of public administration, public health, organizational networks, and business strategy. The inclusion of traditional business strategy in the mix of frameworks gives the analysis, models, and propositions of the article a special hue that complements insights from the other fields of study. The article does, however, develop a new framework for thinking about collaboration, one that is a hybrid of the work of other scholars.
Health Care Context
As documented in the academic and professional literature, U.S. health care policy ultimately supports strategic initiatives dedicated to achieving a comprehensive goal: improve in an equitable way the health of all members of society as measured by increases in the quality and years of human life (see Figure 1).
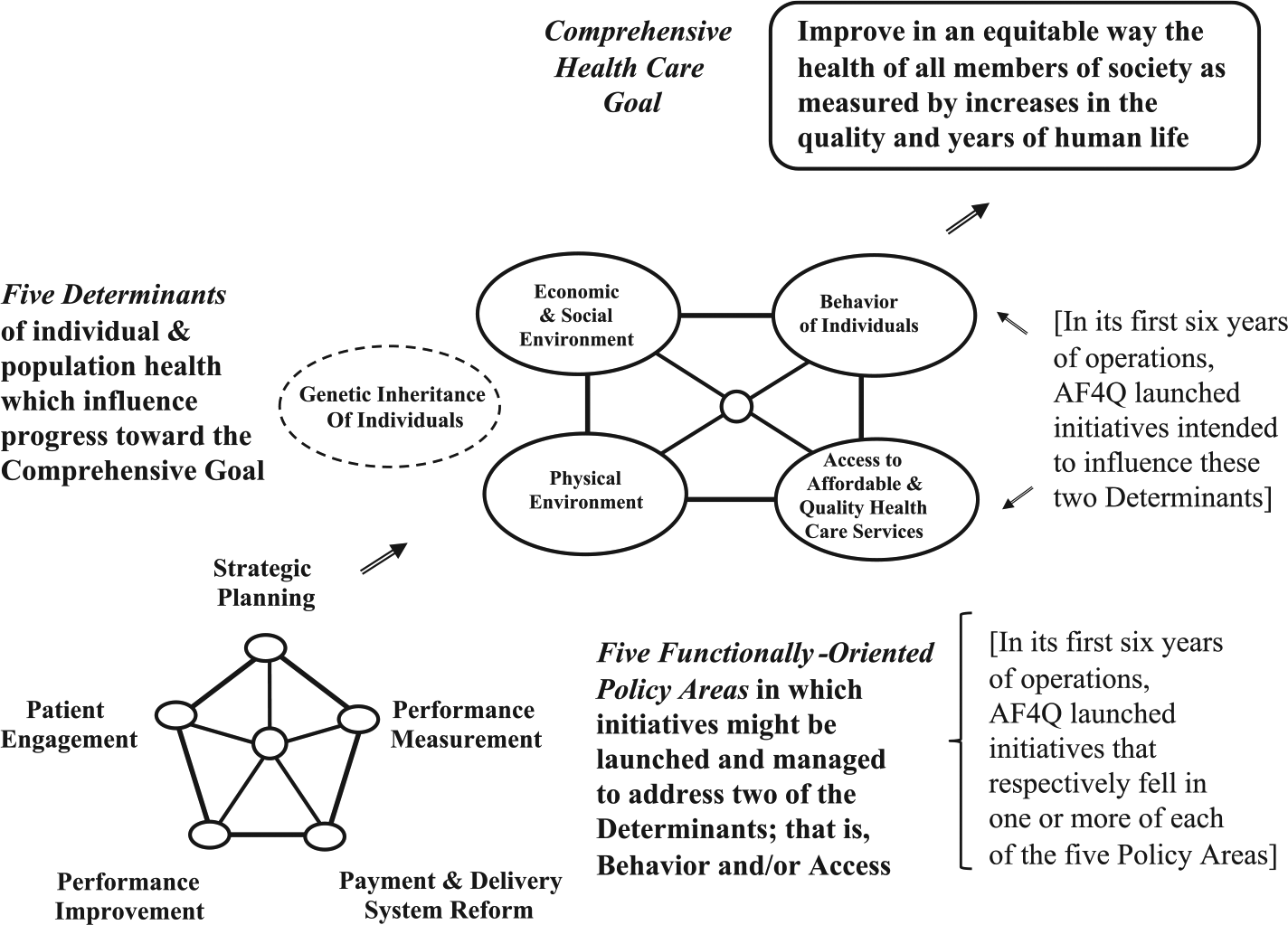
Functional policy categories, determinants, and goals of community health care.
The ability to achieve that goal is influenced by a group of five interrelated determinants: Individual Genetic Inheritance, the Social and Economic Environment, the Physical Environment, Behavior on the Part of Individuals, and Access to Affordable and Quality Health Care Services. No policy initiative can change the genetic inheritance of any individual. Furthermore, efforts to influence the second and third determinants just listed involve broader concerns that concentrate on fundamental issues and take time to improve. They might include advocating for universal health care, or attempting to eliminate disparities across population segments by creating equitable education or employment opportunities (Roussos & Fawcett, 2000). Those two determinants lie beyond the scope of programs undertaken by AF4Q-SCPA.
To elaborate, as of 2013, the purpose of AF4Q-SCPA, as captured in its mission statement, was to influence the remaining two determinants of high-level goals depicted in Figure 1: Access to Affordable and Quality Health Care Services; and Behavior on the Part of Individuals. Toward that end, during its first 6 years of operation, AF4Q-SCPA launched initiatives that respectively fell in one or more of five functionally oriented policy areas: Patient Engagement, Performance Measurement, Performance Improvement, Payment and System Delivery Reform, and Strategic Planning. Those categories are reflected, for example, in the work of the highly respected Network for Regional Healthcare Improvement (2014).
Specific examples of initiatives might include some of the following. Programs that discourage smoking seek to alter the Behavior of Individuals. Programs that encourage immunization may seek to increase Access to Affordable Health Care Services. Programs that address system-related issues such as service quality and service payment certainly seek to enhance Access to Affordable Health Care Services, but may improve patients’ perceptions of experience, and thus, as a secondary effect, make them more likely to seek health care services and thus influence Patient Engagement.
A Bit of Jargon
This article refers to an organization that is responsible for convening and managing multisector relationships as a cross-sector collaboration organization (CSCO). This term is in line with the description of a “network administrative organization” provided by Provan and Milward (2001), the label “bridging organization” used by Selsky and Parker (2005), and the notion of a “backbone organization” introduced by Kania and Kramer (2011). Nevertheless, this article uses the label CSCO to highlight the notion that in collaborative structures, there is a bit of hierarchy. For example, foundations such as the RWJF, which via their financial contributions make possible a collaboration, have a role to play in the hierarchy. So too do the configuration of stakeholders who come together under the prompting of the CSCO to launch and manage activities. Bryson et al. (2006) refer to that group of stakeholders as the CSC. Participants in the CSC will include people employed by participating organizations, including full-time employees of a lead organization, such as AF4Q-SCPA. To push this one step further, given that AF4Q-SCPA was engaged in the health care sector, the authors label it a health care cross-sector collaboration organization (HC-CSCO.)
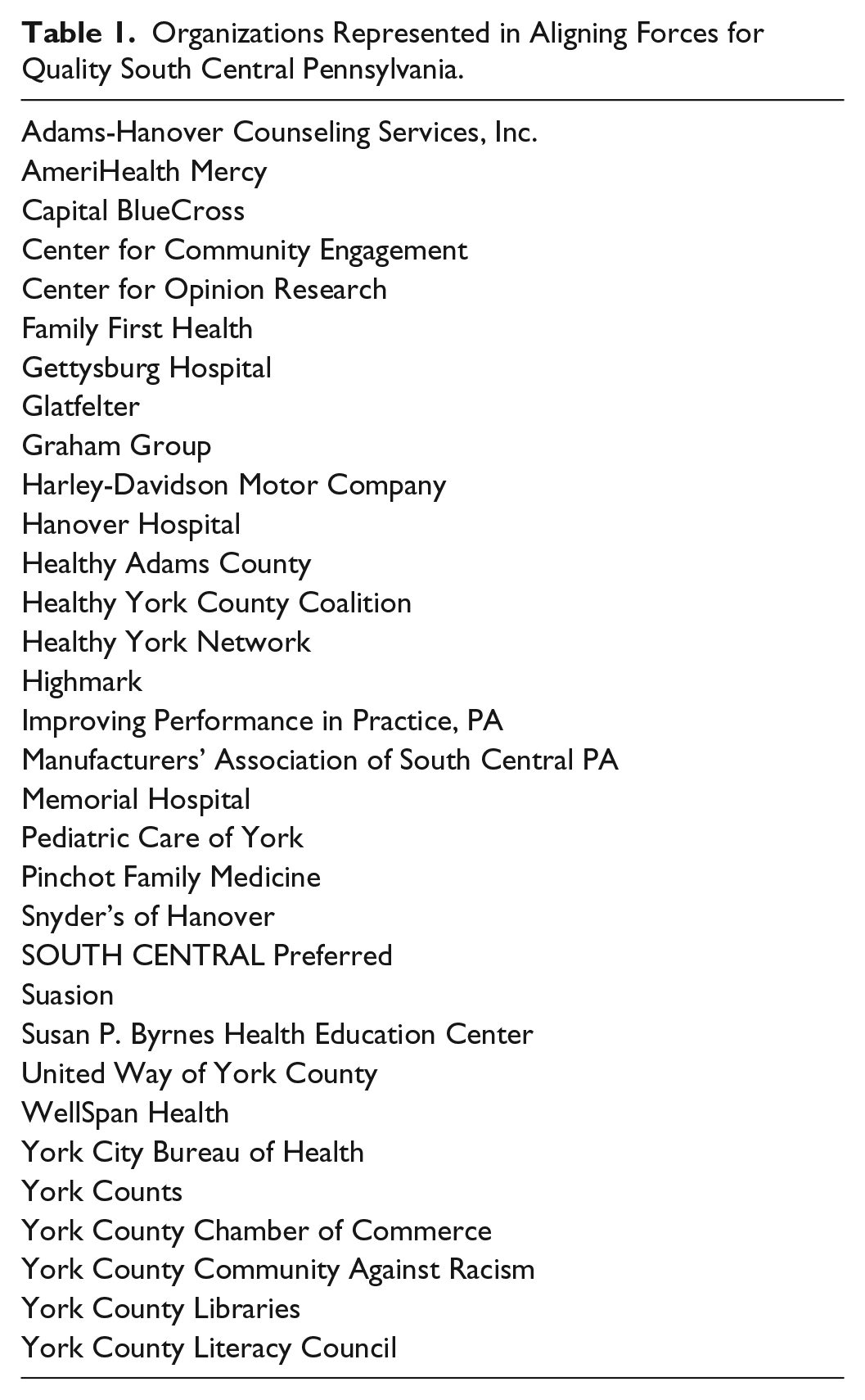
From the outset, AF4Q-SCPA successfully played the role of a HC-CSCO. In its first 4 years of operation, AF4Q-SCPA concentrated on Adams and York counties, which reflected the service areas of Leadership Team members. Thus, this article labels AF4Q-SCPA during those 4 years a community health care cross-sector collaboration organization (CHC-CSCO). In the following 2 years leading up to 2013, AF4Q-SCPA enlarged the geographic scope of its engagement and the number of participating organizations (Table 1). That is, it not only managed initiatives at the two-county level but simultaneously helped organize forums that included participants from across the 10-county region of South and South Central Pennsylvania. Taken together, those two arenas of engagement lead this article to label AF4Q-SCPA in the latter period a hybrid, that is, a community-focused and regional in scope health care collaboration organization (CHC/RHC-CSCO).
Organizations Represented in Aligning Forces for Quality South Central Pennsylvania.
Accomplishments
In retrospect, in the two-county service area, by 2013 AF4Q-SCPA had undertaken three sets of initiatives. First, to promote Patient Education and Engagement, it had established the Health Literacy Learning Collaborative, a Web Page Project, and the I Can! Challenge, which was a 12-week, step-by-step program that taught participants how to set health goals in partnership with their doctor, improve their diets, and engage in regular exercise. Second, to promote Performance Measurement, it launched a Community Check-Up Initiative. The Initiative encouraged transparency and sharing of information about the progress being made by patients to better control their heart disease or diabetes. The website associated with the Initiative allowed the public to compare data from various doctors’ offices and clinics about blood pressure, blood sugar, and low-density lipoprotein (LDL) cholesterol levels, and about the percentages of patients who were taking a daily aspirin or aspirin alternative and were having their body mass index monitored. Third, to help make progress toward Performance Improvement, it led efforts to create a Patient-Centered Medical Home (PCMH) collaborative. In that model, PCMH patients would receive accessible, continuous, comprehensive, and integrated care from their primary care provider, who would lead and coordinate the efforts of a team of health coaches, in hope of reducing fragmentation in the health care system, enabling better communication, and improving health care quality.
At the regional level, AF4Q-SCPA launched two sets of initiatives. First, to promote Payment and Delivery System Reform, AF4Q-SCPA facilitated creation of the PRICE Working Group. That effort brought together nine health systems, eight health plans, a third-party benefits administrator, the PA State Employees Benefit Trust Fund, and several larger employers to work collaboratively to develop new models of health care payment. As of 2013, the group adopted common definitions and measure-sets for bundled payments for hip and knee replacements and coronary bypass graph surgery, as well as common definitions and measure-sets appropriate for PCMHs. Second, to promote Strategic Planning, it had helped create the Executive Leader Group.
As a point of comparison, the community-focused initiatives called for a much greater degree of direct, hands-on involvement by the management team than did the initiatives launched at the regional level, and thus called for a somewhat different managerial focus and set of activities. Regardless of arena, however, interviews with several stakeholders (not included in this article) suggest that all efforts were appreciated.
Leadership and Management
Given the range of initiatives noted above, one might say that AF4Q-SCPA was indeed a success. In part, that success was due to a knowledgeable leadership team and dedicated staff. As of 2013, a Leadership Team that included a handful of professionals from the not-for-profit, state, and for-profit sectors provided oversight of AF4Q-SCPA. The Team met on a regular basis.
They had first-line responsibility for charting strategic direction, for enlisting new members to the organization, and for overseeing activities. (At the time, a Regional Steering Group was under consideration.) The organizational structure of AF4Q-SCPA (not depicted in this article) consisted of four primary councils (Transition of Care Council, Quality Improvement Council, Consumer Engagement Council, and PRICE Council). Each focused on a policy area of the type illustrated in Figure 1 and described above. In turn, each council included two to four subsidiary structures, each of which was associated with a separate initiative.
With respect to day-to-day activities, AF4Q-SCPA employed a full-time Project Director, who was a member of the Leadership Team. The Director was responsible for oversight of all initiatives and was responsible for the PRICE Council. It also employed an administrative assistant, and three full-time staff members whose respective responsibilities were, for the most part, aligned with one or more of the other three Councils or subsidiary structures that had been launched by the organization at either the community or regional level. Essentially, that group served as part of what this article labels the Management Team. Something very important is that the Executive Director had a seat on both the Leadership Team and the Management Team and therefore helped ensure consistency between strategy formulation taking place in the CSCO and strategy implementation by the CSC.
Strategy: A Working Definition
When a HC-CSCO is established, it will, ideally speaking, provide a neutral, trusted mechanism through which all the key health care stakeholders—physicians, hospitals, health plans, employers, and patients—in a defined service area will find common ground. They will do so to plan, facilitate, and coordinate initiatives designed to influence the determinants of the comprehensive goal noted above. To launch and coordinate initiatives, the leaders and managers of the HC-CSCO will need to guide vision and strategy, provide support to align actions, establish shared measurement practices, build public will, advance policy, and mobilize funding. In that context, Bryson (1995) offers the following helpful definition of strategy:
A strategy may be thought of as a pattern of purposes, policies, programs, actions, decisions, and/or resource allocations that defines what an organization is, what it does, and why it does it. A strategy, therefore, is the extension of the organization’s mission, forming a bridge between the organization and its environment. (p 130)
Bryson’s definition of strategy has a few strengths: It is inclusive of all sectors, and it incorporates internal and external perspectives about strategy, both of which are relevant to appreciating the complex interplay of organizational structures, processes, and the environment. As well, it implies relationships between strategy formation and strategy implementation.
Culture, Strategy, and the Competitive Environment
The success of AF4Q-SCPA was in part also due to another set of considerations. In a paper that concentrates on an individual not-for-profit hospital, Fratantuono and Sarcone (2008)—who synthesize the work of Schein (1985), Kotter and Heskett (1992), and Porter (1996)—describe factors which contribute to successful strategy formulation and implementation. They posit that for an organization to be successful, two minimal conditions must hold: First, the culture of the organization as defined must serve as the foundation for its competitive strategy, and second, the culture and the related strategy of the organization must fit its competitive environment. Thus, the model sketched in their paper is consistent with Bryson’s definition of strategy and provides a basic template for understanding the success of AF4Q-SCPA.
As a caveat, however, the two minimal conditions are just that, and do not imply that efforts launched by an organization that fulfills those criteria will necessarily be a success. Other considerations come into play. For example, as noted at the outset of this paper, Bryson, Crosby, and Stone say that successfully managing a CSC is a daunting task. Furthermore, as suggested by Adner (2012), those involved in an organization dedicated to product or process innovation face a combination of co-innovation risk (other participants in the same ecosystem must each make needed change), adoption-chain risk (organizations upstream or downstream from the innovator in a supply chain must make needed change), and execution risk (associated with effectively launching and managing initiatives or activities). All three types are certainly relevant to collaborative initiatives in the health care sector.
With respect to strategy, after reviewing printed material and audio-recordings of interviews, the authors created Table 2 and Figure 2. Informed by Porter (1996), in Table 2, the authors identify what they took to be five high-level strategic themes and 24 supporting activities. Furthermore, this article asserts that those running the HC-CSCO will, in conjunction with a health care cross-sector collaboration (HC-CSC), launch and manage initiatives and activities in one or more of the five functionally oriented policy areas depicted in Figure 1, and will do so in hope of influencing a determinant of the comprehensive health care goal. Given that assertion, Table 2 links each activity to one or more of the policy areas.
Strategic Themes and Activities of Aligning Forces for Quality of South Central Pennsylvania.


Activity system of AF4Q-SCPA.
Figure 2 translates the themes and activities from Table 2 into a molecule-like activity-system map of AF4Q-SCPA of the type advocated by Porter. As elaborated below, the activity system of Figure 2 suggests that even though AF4Q-SCPA was a CSCO dedicated to facilitating interactions among a range of stakeholders, the two minimal conditions for an effective organization identified by Fratantuono and Sarcone (2008) did hold. That is, cultural values imbued both the high-level themes and supporting activities, and the themes and activities enabled the organization to fill effectively a niche in the complex environment. Taken together, the themes and activities suggest that it would be difficult for another organization to replicate the competencies of AF4Q-SCPA or to create similar magnitudes of economic and social value for health care community stakeholders.
With respect to the notion of organizational culture as described by Schein (2010), over the course of three 2-hr conversations, the members of the management team shared ideas that the authors interpreted as five core values that had informed the efforts of the team. (a) Access to affordable and quality health care is the foundation of a strong community. (b) The creation and dissemination of knowledge are critical to individual and organizational development. (c) Effective collaborative initiatives are based on trust, which can only be earned when all parties are treated with respect, when arrangements are regarded as equitable, and when communication is clear and transparent. (d) To be effective, individuals and organizations must be able to combine an entrepreneurial spirit with strategic patience. (e) To find consensus and create social and economic value, leaders of a collaborative initiative must be able to relate the interests and actions of individual agents to wider, system-level relationships.
With respect to the health care environment, during the formative years of the organization and into 2013, the people in the 10-county region of South Central Pennsylvania enjoyed a superior population health status ranking relative to other Pennsylvania regions. Furthermore, service providers had managed via individually taken steps to achieve cost-levels for care below commonwealth and national averages, and economic returns that ensured short- to medium-term sustainability of individual practices and health care systems. That economic success, however, tended to weaken any shared perception of the need for systemic change.
Nevertheless, three other sets of factors also suggested that stakeholders would benefit from the existence of an effective HC-CSCO. First, there was little evidence in the 10-county region that non–health care leaders in the private sector, such as major employers, were actively pressuring regional health care institutions to alter the local health care industry. Second, in the years leading up to 2013, although health-related organizations in the public and nonprofit sectors throughout the region were engaged in numerous reform efforts focused on multiple determinants of health, those efforts had at times been duplicative, often lacked the resources required to meet stated goals, and had not attempted to extend beyond municipality and/or county boundaries. Third, while stakeholders at both the regional and state levels recognized the need for greater information connectivity, the large health systems and the large health plans tended to act independently from one another, even as they attempted to respond to the Commonwealth’s bottom-up Health Information Exchange (HIE) development strategy.
Organizational and Operational Analysis
Mandell and Keast (2008) introduce another relevant and helpful set of considerations for helping to explain the success of AF4Q-SCPA. They point to three possible nested levels of analysis. First, is the macro-level of analysis. At that level, one might focus on an entity that sits apart from (or some might say “above”) a system, but nonetheless plays an important role, perhaps as a sponsor or provider of necessary funds for the CSCO. The RWJF played that role in helping to give birth to AF4Q-SCPA. This article does not, however, This article focuses on two of that level of analysis nore does it examine the motivations or actions on that type of actor.
Instead, this article concentrates on the other two levels of analysis introduced by Mandell and Keast: organizational and operational levels of analysis, and links across those two levels. As it does so, it focuses on AF4Q-SCPA as a HC-CSCO, and on full-time staff who helped manage particular activities and thus were affiliated with the supporting CSC. Given those two levels of analysis, this article says that as leaders of a HC-CSCO go about business, they will need to leverage organizational and operational capabilities. This article offers the following definitions of those two terms, which draw heavily on the work of Kotter (1990, p. 6).
Organizational Leadership and Management Capabilities are most relevant to creating an agenda and developing a human network for achieving the agenda, which in turn respectively call for special management (planning and budgeting; organizing and staffing) and leadership (establishing direction; aligning people) capabilities. Operational Leadership and Management Capabilities are relevant to execution, which, with respect to management, involves controlling and problem solving; and with respect to leadership, involves motivating and inspiring.
To illustrate factors that contribute to the likelihood of success of initiatives launched by a CSCO in conjunction with a CSC, this article introduces a framework called the Collaboration Cube (Figure 3). It depicts the likelihood of success of activities launched under different types of organizational structures in pursuit of different types of desired outcomes. Essentially, the framework integrates both the organizational and operational levels of analysis. The framework draws upon Agranoff (2003), who addresses outcomes and structures for intergovernmental networks; Mandell and Steelman (2003), who examine networks of agents from any sector; and Bryson et al. (2006), who explore collaborations among agents from different sectors.
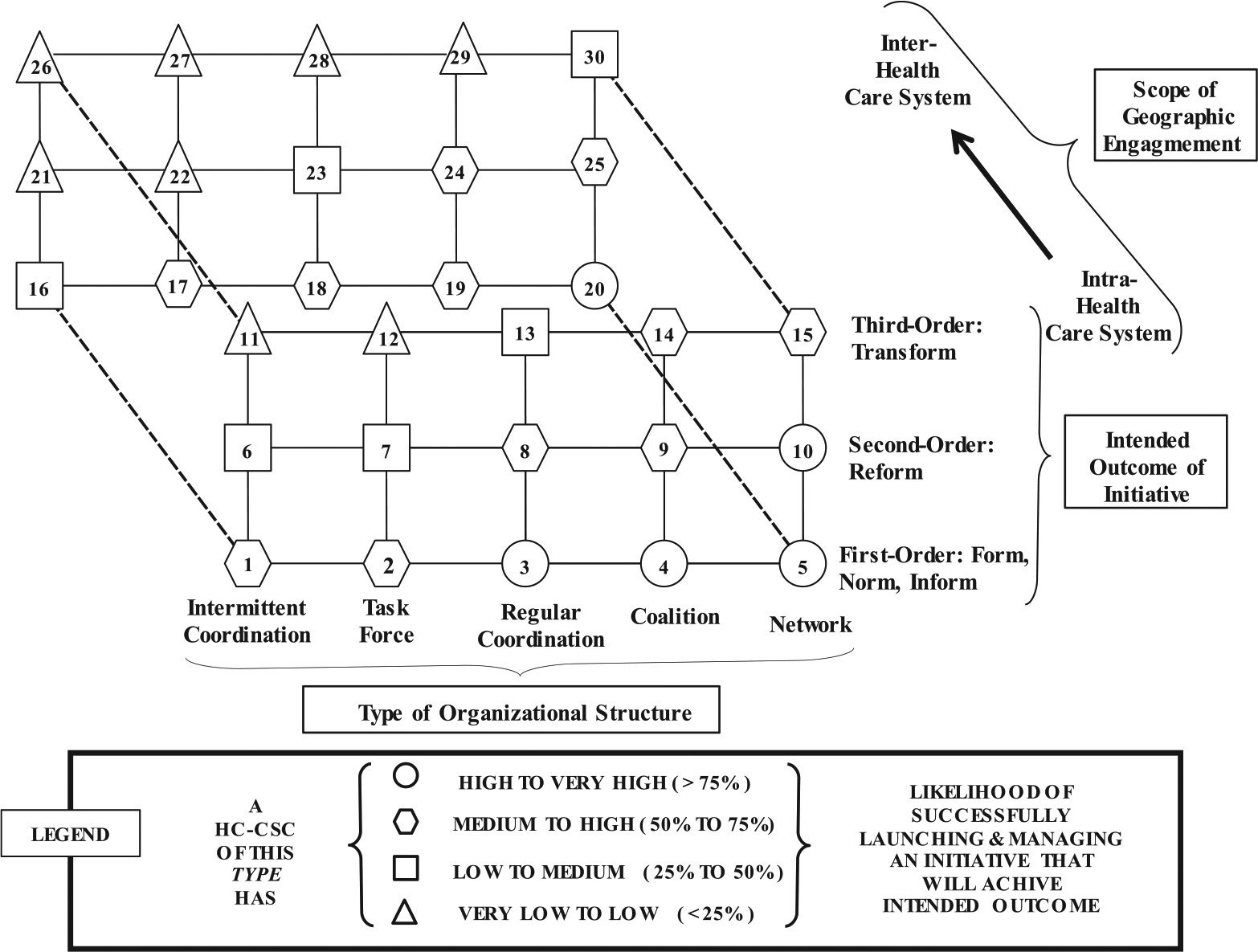
CSC structures, intended outcomes, and the likelihood of success of initiatives: The “Collaboration Cube.”
Types of Organizational Structures
Mandell and Steelman (2003) create a rubric based on six subsidiary questions relevant to any collaborative structure. Their six questions address the perspective of participants about the problems to be addressed and the degree to which participants are committed to common goals, the breadth of membership and the degree of interdependence among the participants, and the complexity of the problem tackled and scope of change intended by participants. With the rubric in hand, they identify five different organizational types.
Intermittent Coordination occurs when the policies and procedures of two or more organizations are mutually adjusted to accomplish each organization’s objectives. The participants tend to view problems and seek solutions that are relevant to their respective organizations, involve a narrow set of participants who are only weakly interrelated, and who come together primarily to share information, as they have no intention of changing the status quo.
Task Forces are established to accomplish a specific objective and disband when the purpose is accomplished. The participants tend to view problems from the perspective of their respective organizations. They may begin to seek solutions that represent some combination of their respective individual goals and as well a goal or goals common to all. They will involve a narrow set of participants who may be either weakly or strongly interrelated. They come together to engage in limited joint problem solving, but they are essentially satisfied with the status quo.
Regular Coordination involves collaboration through a formal arrangement that involves more than information sharing. The participants may begin to develop a shared perspective about problems and may begin to seek solutions that represent some combination of their respective individual goals and as well a goal or goals common to all. While the membership is relatively narrow in scope, the interdependence among participants can range from weak to strong. Like the Task Force, this structure involves participants who come together to engage in limited joint problem solving, but who are essentially satisfied with the status quo.
Coalitions occur when membership in the organization is relatively stable and there is a formal agreement that defines relationships and resources committed by each member. In this structure, membership tends to be broader than in the first three structures. The members take interdependent strategic actions, but the purposes are narrow in scope and all actions occur within the participant organizations or involve the sequential or simultaneous activity of the participant organizations. The problems that are tackled by coalitions tend to be more complex than those tackled under the previous three structures, but the participants still are satisfied with the status quo at the system level.
Networks entail a broad mission and joint and interdependent actions. Networks require strong commitment to overriding goals. Members agree to allocate significant resources over a long time period, and as well agree to jointly assume an element of risk. They exhibit a shared perspective about common goals; have comprehensive membership, with participants linked by strong interdependence; and engage in complex problem solving dedicated to system transformation.
Types of Outcomes
In terms of the degree of change it is intended to foster among participants in a system, the objectives of a CSCO-launched initiative can differ from others the CSCO may have previously launched or may choose to launch in the future. This article paraphrases, elaborates, and fine-tunes the ideas of Bryson et al. (2006), who incorporate different types of interdependence and different orders of “effects” in their descriptions of CSCs as they identify three types of outcomes.
This article says that first-order outcomes are those in which stakeholders come together to share knowledge and reach agreements about the way they might structure their future courses of action. They are governed by arrangements in which each party contributes to the whole, but in a discrete manner, and in which the activities of the parties are coordinated via standardization. Following Bryson et al, it further says that first-order outcomes form, norm, and inform stakeholders.
Second-order outcomes are those which primarily change the structure and behavior of respective stakeholders, call for actions by operation-level managers and teams to leverage existing knowledge and technologies, and involve coordination and cooperation among participants under an agreed plan in which the activities of one organization serve as preconditions to the activities of the next organization. The key word for second-order outcomes is reform.
Third-order outcomes involve a change in power structures. Due to the alteration, the activities of any stakeholder provide a contingency for all others, and the activities of stakeholders are coordinated via mutual adjustment and co-evolution. Furthermore, the alteration leads to calls for engagement and decisions by those who hold the highest governance positions in their respective organizations, and more generally to a request for stakeholders to accept new approaches to knowledge formation and problem solving. Third-order outcomes transform.
A Descriptive Framework
The Collaboration Cube depicted in Figure 3 focuses on relationships between organizational structures and intended outcomes. The framework consists of two planes. Each plane includes two axes. Moving from left to right in either plane, the horizontal axis denotes the five increasingly more sophisticated types of organizations identified by Mandell and Steelman. Moving from bottom to top in either plane, the vertical axis displays first-order, second-order, and third-order outcomes.
As noted in the Legend, in either plane, the shapes of the various nodes are intended to suggest the likelihood that an initiative launched under a particular structure will successfully promote a desired type of outcome. (A strong caveat is in order. At this point, the probabilities included in the Legend of Figure 3 are only illustrative in nature: They are not based on fieldwork involving multiple organizations and associated empirical analysis, which remain tasks for future research.) The plane in the forefront of the framework, which includes Nodes 1 through 15, is relevant to initiatives launched by AF4Q-SCPA in its role as a community health care cross-sector collaboration (CHC-CSCO). That is, any initiative launched by the organization would bring together a group of participants under a structure in hope of cultivating a either a first-order, second-order, or third-order outcome within a circumscribed health care service area.
In contrast, the plane at the back of framework, which includes Nodes 16 through 30, is relevant to initiatives launched by AF4Q-SCPA in its role as a regional health care cross-sector collaboration (RHC-CSCO). Thus, outcomes in that plane are Intra-Health Care System in nature.
The likelihoods embedded in the framework reflect the inherent complexity of managing collaboration among organizations and the presence of the previously noted co-innovation, adoption-chain, and execution risk. For example, in the front plane or the back plane, for any Organizational Structure, if one considers moving from First- to Second- to Third-Order outcomes, the likelihood of success of an initiative tends to decline.
Furthermore, if one keeps constant Organization Structure and Order of outcome, the likelihood of success of any initiative will decline as one extends geographic boundaries of engagement, which is evident by comparing Node 1 to Node 16, Node 8 to Node 23, Node 15 to Node 30, and so forth. Simply speaking, the model illustrates the idea that success in launching any type of initiative at the regional level will be harder to realize than launching a similar initiative at the community level. This article assumes that would be true, even if the payoffs to regional cooperation exceed those in community organization, as would be the case, for example, with returns to scale benefits associated with payment system reform.
One might use the model to think about past events, that is, in an ex post fashion. The following two observations illustrate that approach. First, in the early years of operations, acting in its capacity as a CHC-CSCO, AF4Q-SCPA had launched the previously described I Can! Challenge in the two-county area. The initiative was a success. While it resulted in both Type 1 (Form, Norm, Inform) and Type 2 (Reform) outcomes among community members, it essentially only needed to generate Type 1 outcomes among physician practices. AF4Q-SCPA accomplished those outcomes via a structure among physicians and other community stakeholders that was consistent with a Task Force. The hexagon shape of Node 2 suggests that in retrospect, one may have anticipated that the initiative would have a moderate to high likelihood (50%-75%) of success. Second, in its role of RHC-CSCO, AF4Q-SCPA had established the previously described PRICE Working Group. The Working Group, which as of 2013 had been in existence for about 2 years, had established common definitions and measures among participants. That progress essentially represented a First-Order Outcome, accomplished via a structure consistent with Regular Coordination. The hexagon shape of Node 18 suggests that in retrospect, one may have anticipated that the initiative would also have a moderate to high likelihood of success.
Looking Ahead—Strategic Alternatives
As consultants for AF4Q-SCPA, the authors of this article came to recognize and appreciate that AF4Q-SCPA had a range of strengths and had met with success in launching several important and valuable initiatives. Furthermore, the attributes of the health care environment confronting AF4Q in its formative years continued to be relevant as of 2013, and suggested that in the years ahead there would still be a need for an organization such as AF4Q-SCPA in South Central and Southeastern Pennsylvania. Nevertheless, the scheduled end of funding from the RWJF loomed large.
As the Leadership Team wrestled with the decision about the future of the organization, the authors advised they consider the ideas of Hambrick and Fredrickson (2001), who argue that if the heads of an organization cannot offer answers to five important questions, then they do not have a strategy. Those questions are as follows: How will we get there (Vehicles)? How will we win (Differentiation)? Where will be active (Arenas)? How will we obtain our returns (Economic Logic)? What will be the speed and sequence of our moves (Staging)?
As elaborated below, if the Leadership Team chose to continue operations, the authors believed at the time that while the answers to the first two of those questions would be relatively straightforward, the ability to answer the latter three would involve some tough choices and necessitate some important steps.
How Will We Get There? (Vehicles)
The initial funding from the RWJF had anticipated that AF4Q-SCPA would serve as a catalyst for collaboration among a range of stakeholders in the health care field. The organization had helped launch a range of initiatives in five policy areas that were intended to influence two sets of determinants of the comprehensive health care goal. One might say therefore that if the team chose to move forward after cessation of RWJF funding in 2015, AF4Q-SCPA still represented at both the organizational and operational levels of analysis an appropriate vehicle for making progress toward health care goals.
How Will We Win? (Differentiation)
As illustrated in the Activity System illustrated in Table 2 and Figure 2, AF4Q-SCPA had a well-articulated organizational culture that infused its high-level strategic themes and activities which in turn were appropriate to the health care environment of South and South Central Pennsylvania. Simply speaking, if the team chose to move forward, then in judgment of the authors, those attributes would continue to serve the organization well.
Where Should We Be Active (Arenas)?
To remain in operation, the Leadership Team of AF4Q-SCPA would have to make three types of choices relevant to the question as to where they would be active. First, they would have to decide which among the five types of policies AF4Q-SCPA should choose to address. Second, they would have to decide if AF4Q-SCPA should primarily focus on formulating strategy and in creating working groups and councils, or if it should also be involved in implementing policies and maintaining programs. Third, and most important, the leadership would have to make decisions about the size of the geographical region for which they would provide services, which would essentially dictate the type of HC-CSCO AF4Q-SCPA would be.
If in the future the Leadership Team of AF4Q-SCPA were to choose to return to a CHC model, then the organization would devote its efforts solely to serving an arena that concentrated on Adams and York counties. AF4Q-SCPA would most likely concentrate on Patient Engagement, Performance Measurement, and Performance Improvement. As a community resource, AF4Q-SCPA would be actively and deeply involved in planning, implementation, and management of collaborative initiatives.
If the Leadership Team chose a pure RHC-CSCO model, then AF4Q-SCPA would attempt to reposition itself as the leading regional health improvement collaborative in South Central and Southeastern Pennsylvania, recognized for its ability to improve service quality and efficiency on a regional basis. AF4Q-SCPA would concentrate on initiatives associated with Performance Measurement, Performance Improvement, and Payment and System Delivery Reform, or might attempt to become the hub in a network of community health networks, primarily focused on Strategic Planning, or both.
If the leadership opted for the existing hybrid model, then AF4Q-SCPA would certainly acknowledge and celebrate its history and roots in York and Adams counties and would play a role in York and Adams county-focused initiatives. Nonetheless, AF4Q-SCPA would also seek to become the leading regional health improvement collaborative in South Central and Southeastern Pennsylvania.
The Collaboration Cube sheds light on these considerations. In the case of AF4Q-SCPA, differences across the two planes would be associated with comparing the likelihoods of success of an initiative limited to the two-county area versus one intended to influence the service areas of multiple health systems. Given that AF4Q-SCPA had evolved into a hybrid CHC/RHC-CSCO and was simultaneously engaged in two arenas, some of its initiatives resided at nodes in the front plane of the framework and others at nodes in the back plane of the framework. The necessity to operate in both the community and regional arenas brings to mind a warning provided by Porter (1996): Even as managers purposely choose the niche they intend to fill in an external environment, they should also be mindful of what they should not attempt to do; otherwise, they risk having their organization straddle strategic positions in the environment, a situation which will tend to stretch resources, loosen the internal “fit” among themes and activities, and undermine the ability of the organization to create value.
How Will We Obtain Our Returns? (Economic Logic)
If they chose to continue operations following the anticipated cessation of RWJF funding in 2015, the Leadership Team understood that to first survive and second to build capacities and competencies, the organization would need to secure financing and earn revenue from one of three channels: in-kind contributions, nonoperating revenue, and operating revenue.
In-kind contributions
In coming years, in-kind contributions from the private sector—such as those which had been provided by AF4Q-SCPA Leadership Team members over the life of the organization—had the potential to meet a small but significant part of the organization’s operating requirements. Opportunities to secure in-kind resources from the public sector were also a possibility. For example, under a program that was in place from February of 2010 to February 2014, the state of Pennsylvania had received an award from the Office of the National Coordinator for Health Information Technology (ONC) intended to help build capacity for exchanging health information, increasing connectivity, and enabling the exchange of patient-centric information. The ONC award called for the state of Pennsylvania to commit matching funds, which, when combined with US$17.1 million of federal funds, created a pool of US$19.4 million. Those funds could be used to reduce costs and enhance capabilities within state government agencies; in turn, those agencies could provide technology or labor either without charge or at reduced cost to organizations such as AF4Q-SCPA.
Nonoperating revenue
During the 2000s, some important government agencies at the national level, such as the Centers for Medicare and Medicaid Services (CMS), awarded grants to promote community health care. As of 2013, those agencies remained a potential source of funds. There were also sources of public funding at the state level. To illustrate, the Office of Medical Assistance Programs of the Pennsylvania Department of Public Welfare (DPW) received funding, through the American Recovery and Reinvestment Act of 2009 and other programs to promote HIE initiatives. To enhance prospects, AF4Q-SCPA might choose to pursue grants in concert with other health care focused entities, including foundations, nonprofit service organizations, CSCs, or academic medical centers.
With respect to the private sector, at the national level there were a range of foundations which supported improving health care outcomes. In terms of the cumulative total of grant dollars awarded in 2011, the top-20 list was headed by the Bill and Melinda Gates Foundation (US$3.3 billion), followed by the RWJF (US$303 million), and extended down to the Ford Foundation (US$25.2 million). There were also numerous regional and local foundations which supported community health initiatives, and while awards from any one of this group were not large when compared with those available from either the public sector or national foundations, over one-half of the grant funds awarded each year in the United States originated from those sources. As well, to court and win over additional institutional sponsors from multiple sectors and industries throughout the region, AF4Q-SCPA could recruit delegates from those organizations to fill governing roles.
Operating revenue
AF4Q-SCPA could also generate revenues by charging membership dues, consulting fees, or fees for services to health care stakeholders. Most regional HC-CSCOs generated operating revenue via membership dues that were contingent on the status and financial wherewithal of respective stakeholders.
To help make the case for revenues, AF4Q-SCPA would have to pursue courses of action that would generate first-, second- and third-order outcomes. A few examples come to mind. First, perhaps AF4Q-SCPA could create economic and social value by establishing a Resource Center that would charge fees for a range of work-related products and activities, including writing reports, providing consulting services, offering training programs, organizing workshops, and staging conferences or forums that featured recognized health care experts. Second, as a regional health care, the organization might be in position to enter service contracts with public sector entities such as the Pennsylvania DPW Office of Medical Assistance Programs to assist in monitoring the quality of services provided to DPW clients.
What Will Be the Speed and Sequence of Our Moves? (Staging)
If in the years ahead, the Leadership Team of AF4Q-SCPA chose to move ahead, they would most likely have to redefine the long-term purpose and position of the organization within the region’s health policy arena. The question about the speed and sequence of moves was for the most part contingent on decisions that the team would have to make regarding arenas and economic logic. Regardless of choices, proper staging would entail building new internal capacities and shaping new external relationships (Hambrick & Fredrickson, 2001).
Building internal capacities
To secure additional sources of nonoperating revenue, AF4Q-SCPA might need to strengthen its development expertise and capabilities, perhaps by adding a full-time grant writer to the staff. AF4Q-SCPA would also have to strengthen its technical capabilities in the areas of information technology and data analysis, especially if it were to remain active in initiatives that involved Performance Measurement, Performance Improvement, and Payment and Delivery System Reform. It could do so in one of three ways. First, it could independently develop internal technical capacity. Second (and perhaps more realistically than Option 1), it could attempt to secure the necessary capacity and competencies through a contract with an existing HIE service provider. Third, it could enter an alliance with a third party such as a regional quality measurement collaborative. An ideal partner would be one with expertise in data gathering, electronic health records, predictive modeling, risk assessment, gap analysis, provider analysis, and care and case management capabilities within the context of one integrated tool.
Building new sets of relationships with other organizations
The Collaboration Cube helps one think in ex ante fashion about future evolutionary paths associated with the question: What will be the speed and sequence of our moves? That is, as previously described, as of 2013, AF4Q-SCPA had helped to establish the PRICE Working Group, which essentially represented a First-Order Outcome accomplished via a structure consistent with Regular Coordination (Node 18). Looking ahead, to have a medium to high likelihood of achieving a Second-Order Outcome (Reform) among participants under the PRICE Working Group, the leadership of AF4Q-SCPA would have to help relationships evolve from Regular Coordination to a Coalition structure. That would entail movement from Node 18 to Node 19 to Node 24, or perhaps directly from Node 18 to Node 24. In contrast, if the Group were to attempt a Second-Order Outcome under the existing Regular Coordination structure, then the likelihood of success would be relatively lower, as reflected in the square shape of Node 23.
To take this one step further, the model also suggests that it is only as a Network that the PRICE Working Group would have a low to medium likelihood of generating the system transformation one would associate with a Third-Order Outcome, as is illustrated by square-shaped Node 30. Although the relatively low likelihood is consistent with the cautionary words of Bryson, Crosby, and Stone quoted at the outset of this article, AF4Q-SCPA would nonetheless most likely attempt to promote that Outcome. If so, then starting from Node 24, for example, the evolutionary path might run directly to Node 30, or it might run first to Node 25 and then to Node 30.
Commentary
Rising a bit above the immediate case of AF4Q-SCPA, one might argue that the U.S. health care system consists of numerous, multisector configurations of individuals and organizations collectively responsible for the delivery of health care services. Many experts argue that the U.S. system is not sustainable over the long run, given that the functional components—finance, payment, delivery of service, and insurance—embedded in the underlying economic logic of the system are not well integrated. To improve matters, the system will need to continue to transform itself in such a way that service quality is linked to service payment. This is the type of problem that cannot be solved by participants from any single sector and therefore requires ongoing CSC. In turn, CSC implies the need for active engagement by numerous HC-CSCOs to address through their policy initiatives the failures and weaknesses in and across functional components.
As another line of commentary, one might also say that to garner general support, receive investment funds, and earn substantial operating revenue, any HC-CSCO would have to accomplish a few things. It would need to achieve legitimacy in the eyes of stakeholders (Mandell & Keast, 2008), convince them it could generate real returns, and monetize its activities in ways that demonstrated tangible benefits for individual organizations and for the overall system. Those considerations suggest that possibilities for progress rested on three interrelated sets of developments.
First, key stakeholders, including those institutions directly responsible for regulating, financing, insuring, and delivering services, would have to change their perceptions and understanding of the potential role of the HC-CSCO in overall health care system planning and management, and in the centrally important knowledge-formation process. Essentially, there needed to be system-level transformation, a third-order outcome. A change in vantage points would enable stakeholders to see that HC-CSCOs should be financed on a regular basis by both public-sector and private-sector stakeholders. A change in rules could provide some real traction: For example, during talks about restructuring relations between health care institutions within the private sector, support of collaborative efforts would need to be recognized as a legitimate operating expense in calculating a health plan’s medical loss ratio or a health care provider’s service reimbursement calculation.
Second, the necessity for a HC-CSCO to achieve and maintain legitimacy implies that some evolutionary paths are preferred to others. That is, if one assumes that unsuccessful initiatives can result in a negatively reinforcing feedback loop (Meadows, 2008) that undermines the legitimacy of the organization and thus the prospects of garnering contributions, winning grants, or earning revenues, then leaders of an organization should avoid as best they can structure-outcome combinations associated with relatively low likelihoods of success. To illustrate using the case of AF4Q-SCPA, in the foremost plane of the model, if one imagines that the ultimate goal of an initiative or a series of related initiatives within the two-county area is to achieve a third-order outcome, then starting from the most formative stages, the initiative(s) might be shepherded over time through increasingly more sophisticated structures that maintain a reasonable likelihood of reaching increasingly more ambitious outcomes, represented, for example, in Figure 3 by the path including Nodes 1-2-8-9-10-15. In contrast, there would be much lower likelihood of success for initiatives launched along the path involving Nodes 1-2-7-12-13-14-15.
Third, and perhaps ideally speaking, to promote system change that would alter mind-sets and generate revenues, HC-CSCOs and other progressive and proactive entities might have to adapt the role and perspective of what Adner (2012) describes as lead innovator within an ecosystem of interrelated stakeholders. He explains that in some cases, an innovation cannot gain acceptance unless each among several stakeholders in a value chain are willing to make adjustments. In cases where the cost of adjustment exceeds the benefit to one or more of those key stakeholders, the entity in the system that will most likely be in a position to earn the largest returns—the lead innovator—might find it beneficial to share a portion of anticipated profits with the other stakeholders. The authors of this article concur that a HC-CSCO must take an ecosystem view, must understand and quantify net benefits that it is helping to generate throughout the system. They maintain, however, that the HC-CSCO must take a mirror-image approach to that advocated by Adner: The CSCO must leverage its system-level insights as it applies for grants and asks for fees for service, that is, as it attracts, rather than dispenses, funds.
Generalizable Propositions
Based on the above analysis, this article offers nine generalizable propositions about the challenges to leaders of all CSCOs operating in any field.
Possible Areas of Future Research
Looking ahead, one might imagine as three future areas of research. The first area focuses on the operational level of analysis and relationships suggested by the Collaboration Cube. As noted in the description of the model, the numerical values used to identify different levels of likelihood for various structure/outcome combinations are purely illustrative in nature and are (as of yet) not based on empirical research. Thus, an inventory and typology of both successful and unsuccessful initiatives and their corresponding structure/outcome combinations might begin to shed light on actual likelihoods of success. However, as part of that work—or perhaps as a prior step—the notion of first-, second-, and third-order outcomes as they pertain to CSCs in the health care sector must be articulated with greater precision. That need suggests a few questions. What precisely has been the nature of reforms undertaken by individual stakeholders within a health care system? What are the boundary lines between reforms of individual organizations and system-level transformation within a system? What actually are the additional challenges of attempting to achieve intersystem outcomes in comparison with intrasystem outcomes? Research in this area would be linked to Propositions 6, 7 and 9.
The second area of research would concentrate on the organizational level of analysis. That is, this article presents an Activity System model for AF4Q-SCPA. That model suggests that the success of AF4Q-SCPA over its first 6 years of operation was attributable to the fact that the culture of the organization had served as the foundation for its competitive strategic themes and associated activities, both of which were well suited to the external environment. Thus, a line of research that essentially would attempt to replicate for other CSCOs the approach taken in this article might shed additional light on relationships and would help validate Propositions 2 through 5.
The third area of inquiry would further leverage ideas originally developed by Schein (1985), as it would attempt to extend the notion of organizational culture from the CSCO to the CSC, and thus would attempt to bridge the organizational and operational levels of analysis. Schein describes three levels of organizational culture, ranging from underlying assumptions about human nature to articulated values to artifacts. He says that leaders imprint their assumptions and articulated values on their respective organizations via a combination of two sets of mechanisms. The first set comprises primary embedding mechanisms (reflected, for example, in how leaders allocate resources, serve as role models and coaches for other employees, measure and reward individual and organizational performance, include or exclude various participants from decisions, and react to incidents and organizational crises). The second set consists of reinforcing mechanisms (as exemplified by the organization’s design and structure, physical layout, systems and procedures, formal statements of philosophy, rites and rituals, and even shared stories about important people and events).
Given that a CSC will most likely include participants representing multiple sectors and types of institutions, each with its own organizational culture, a simple yet hard to answer question comes to mind. Can a CSC have an organizational culture? If so, then that prompts some follow-up questions. How might the leaders of the CSCO begin to shape and manage an organizational culture at the CSC level? What types of mechanisms are at the disposal of the initiators, leaders, and managers of the CSCO for instilling a culture within the CSC, and how do those differ from the mechanisms available to leaders in traditional organizations? Essentially this line of research would involve an elaboration of Proposition 4.
At the outset, this article observed that due to the growing complexity in the environments confronting leaders and policy makers in different sectors, collaboration is an increasingly important way to address problems and that such collaboration involves organizations from different sectors. Those developments hold true of the health care sector. There are two implications of those developments. First, there is a growing need for interdisciplinary research. Second, there is a need for both case-based, inductive studies in light of established frameworks, and for theory-building. This article is a modest attempt to make progress in those areas.
Footnotes
Acknowledgements
The authors thank the members of the Aligning Forces for Quality South Central Pennsylvania (AF4Q-SCPA) Leadership Team for requesting that the authors help them think through strategic challenges and provide them with recommendations about the members’ possible future courses of action. The authors also thank the members for all the very positive interactions. As well, the authors thank members of the Leadership Team for reading through early drafts of this article and for making recommendations that helped improve the accuracy of some informational details. The authors did receive compensation from the Aligning Forces for Quality of South Central Pennsylvania (AF4Q-SCPA) Leadership Team for the provision of consulting services. They were compensated from funds that were taken from the overall grant money received by AF4Q-SCPA from the Robert Wood Johnson Foundation.
Authors’ Note
The purpose of this article is neither to replicate the final report nor to lobby for the recommendation they made therein. Instead, the goal is to share insights from that work about the challenges confronting AF4Q-SCPA that may be of use to researchers and practitioners involved in either the health care field or in other settings. Furthermore, while the authors acknowledge that members of the Leadership Team of AF4Q-SCPA did review this article for accuracy, the members did not ask the authors to make any substantive changes to either the commentary or analysis included in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Robert Wood Johnson Foundation (Grant #70928; Grant Title “Aligning Forces for Quality: The Regional Market Project.”)