
Abstract
Worldwide, nurse shortage and high turnover rates are observed. Job satisfaction is a major determinant of retention and is influenced by intraorganizational communication and perceived communication satisfaction. This article presents a narrative review on communication satisfaction, job satisfaction, and their mutual relationship as well as their impact on turnover intention and burnout risk in the nursing profession. A literature search was conducted in the databases PubMed, Web of Science, and The Cochrane Library, and 47 articles were included. Descriptive analysis identified different types of social networks in the health care workplace. There is a positive association between communication and job satisfaction among nurses, translating into decreased turnover intention and burnout risk. Job satisfaction is required both for organizational stability as for coguaranteeing patient safety. This will be best achieved through an organization-wide multimodal prevention and intervention program, aimed at optimizing different modalities of interprofessional communication, workload, and job satisfaction.
Introduction
Measures of effectiveness in nursing, such as job satisfaction, job performance, and turnover, have been the focus of nursing-related research for the last 30 years. Such research has largely been driven by the need for hospitals to become increasingly competitive, often in response to a restriction of resources, creating new challenges in the workplace. Within the context of a worldwide nurse shortage and high turnover rates (Gandhi, Sangeetha, Ahmed, & Chaturvedi, 2014; L. Hayes et al., 2006; Kingsma, 2001; Schiestel, 2007), improving nursing effectiveness remains an important goal (Pincus, 1986; Wagner, Bezuidenhout, & Roos, 2015). This global shortage is associated with a loss of trained nurses, times of poor staffing and extra work for remaining nurses, increased costs of enrollment and orientation of new nurses, and, most important, a potential increase in adverse patient outcomes (Larrabee et al., 2003). Job satisfaction has been identified as a major determinant of nurse retention and performance (L. Hayes et al., 2006). Moreover, the quality of intraorganizational communication and perceived communication satisfaction influence job satisfaction at different levels and for all types of employees within the organization.
Aims
We aimed to perform a narrative literature review on job satisfaction in relation to communication satisfaction, with a specific focus on nursing professionals in hospitals.
Method
We searched the databases PubMed, Web of Science, and The Cochrane Library through the keywords “communication,” “patient safety,” “job satisfaction,” “burnout,” “communication satisfaction,” “nursing,” and “nurse turnover,” which were internally validated by the coauthors. Following inclusion criteria were maintained: (a) published between January 1, 1985, and October, 31, 2015; (b) fall into one of the following categories: original research, reviews, meta-analyses, or letters to the editor; and (c) available as a full text in English. Database screening was finished on November 26, 2015. Inclusion criteria were verified through title and abstract. The whole article was read if all inclusion requirements were present or if this was unclear. After reading the full text, papers that did not fulfill all requirements were excluded. The snowball method was used to search for additional literature.
Before writing the article, a predesign of five categories was framed, including interprofessional communication in health care, deficits in communication and influence on patient safety, communication satisfaction, job satisfaction and nurse turnover or burnout, and, finally, recommendations. Papers were allocated to one or more categories. During the writing process, each category was addressed separately and all articles related to a particular category were reread.
Results
The results of the search process are summarized in a PRISMA flow diagram (Figure 1). Out of a total of 4,865 papers selected, 2,161 duplicates were removed. Two thousand seven hundred four records were screened, of which 509 remained for full-text reading. Of the 509, 47 articles were included in the review.

Review stages based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Interprofessional Communication in Health Care
Within health care, much like any other work context, the behavior of each individual is influenced by the surrounding social network. This social network is important for the dissemination of information. Social networks are advantageous for people’s career and job performance (van Beek et al., 2011; Wagner et al., 2015).
Van Beek distinguishes three types of social networking in an organization: communication, consulting, and trust networks (van Beek et al., 2011). The communication network consists of employees who regularly discuss work-related issues. The advice or consulting network includes employees who are invoked to solve problems and exchange information. The trust network describes those who share and receive delicate or sensitive information in problem situations.
These networks are important for the provision of quality care to the patient. In this article, we focus on the communication networks. Such networks are strongly related to job satisfaction. Nurses working in units with a close communication network are more satisfied with their work. In units with few employees, nurses are more likely to be satisfied with their work compared with units with many employees (van Beek et al., 2011). The quality of both communication and advice networks was negatively related to the number of nursing staff on units. Job satisfaction differed significantly interindividually and between units and was influenced by the number of nursing staff.
Communication and advice networks were denser when more nurses worked part-time. Furthermore, density of communication networks increased by higher age of the nursing staff (van Beek et al., 2011).
The health care team is an intact group of caregivers who are motivated to communicate with each other about the care of the patients they are entrusted with. Poole and Real subdivided such care teams with regard to their purpose and function (Real & Poole, 2011). First, the ad hoc team is made up for a restricted period to solve a problem, after which it disappears. Second, within a nominal care team, patients are referred by General Practitioners (GPs) to specialists and both offer independent care. Third, a unidisciplinary team consists of members of a single discipline. Fourth, a multidisciplinary team is composed of different disciplines working together, but the care they offer is sequential. Fifth, an interdisciplinary team is again composed of different disciplines, this time working interdependently, that is, they work and communicate together about the patient’s care. Finally, in transdisciplinary teams, this interdependent collaboration between different disciplines allows caregivers to transcend competencies in their own field and to benefit from the skills of the other disciplines involved in the collaboration. These teams each have their own particular forms of communication. For caregivers, it is important to be able to identify with a type of team to know what the best way to communicate and to work efficiently and effectively is (Brock et al., 2013; Iseke, 2014; Kudo et al., 2010; Liu, While, Li, & Ye, 2015; Real & Poole, 2011). Nurses can belong to different types of teams with their particular modalities and requirements of communication.
To better understand communication within health care teams, the input–process–output (IPO) model of communication in care teams was developed and derived from the group perspective (Real & Poole, 2011, Figure 2). This “group dynamics perspective” conveys understanding of how and why caregivers interact in certain ways and clarifies how teams function. The model describes communication structures (inputs) and processes. These, in turn, create outputs that can affect the results of the care teams (Brock et al., 2013; Real & Poole, 2011).

Input/process/output model of communication in health care teams (Real & Poole, 2011) .
Within health care teams deficient communication can arise from critical information not being communicated between team members, conflicting relationships, or a lack of clarity on roles and job descriptions. Misinterpretation of information can be caused by the use of different terminology or the provision of incomplete information. Although a whole team delivers medical care, medical quality and safety have mainly been centered on individual expert practitioners (Leonard, Graham, & Bonacum, 2004). According to Leonard et al., “Effective communication and teamwork is assumed, however formal training and assessment in these areas has been largely absent” (Leonard et al., 2004, p. i85). Recognition that the clinical care environment has become progressively more complex, combined with the inherent limitations of human performance, has spurred interest in applying the lessons of other high-reliability industries to medicine (Leonard et al., 2004). Many factors contribute to communication failures, which are “the leading cause of inadvertent patient harm” (Aiken et al., 2012). In the first place, doctors and nurses are trained to communicate in a different way (Amestoy et al., 2014; Debra, 1991). Nurses are taught to be rather comprehensive and narrative in their descriptions of clinical situations, whereas physicians need to be very concise, and quickly get to the “headlines.” Nurses often report that they are told during their education that they “don’t make diagnoses.” So, in mutual contacts, the doctors impatiently “wait to find out what the nurses want” (Finn, 2001). In addition, the hierarchy within the team can also cause disturbances in communication. Leadership with strong authority often leads to less communication within the team. In contrast, leadership that is able to handle the hierarchy appropriately, by creating a trustworthy and secure environment, ensures faster communication and more participation within the team (Leonard et al., 2004). Inadequate or incorrect information during a shift handover may also cause communication problems. A final potential risk area for miscommunication involves any transfer of the patient from one care point to the other (Greenberg et al., 2007).
Deficits in Communication and Influence on Patient Safety
Effective communication and teamwork are essential to provide high-quality care and patient safety (Vermeir et al., 2015). Poor communication can lead to various negative outcomes, such as discontinuity of care and compromise of patient safety (Vermeir et al., 2015). The complexity of medical care along with the limitations of human action reinforce the importance of standardized communication and a secure environment, in which team members can express their concerns about patient safety. In such an environment, members can speak freely and critical language can be used to create alertness and to avoid confusion (Brock et al., 2013; Kalisch, Lee, & Rochman, 2010; Leonard et al., 2004).
Interprofessional teamwork is achieved by the interactive efforts of all team members involved through good communication and respect for the role of all team members. There should be room for the contribution of each team member. Not only the technical skills of the team, such as knowledge and experience, contribute to improving patient safety, but also nontechnical skills, such as communication, team size, the psychological mind-set, and the way the team is run, can affect team performance. Despite the increased emphasis on these nontechnical skills, communication problems remain a frequent cause of reduced patient safety (Brock et al., 2013; Courtenay, Nancarrow, & Dawson, 2013; Keith, Coburn, & Mahoney, 1998; Leonard et al., 2004).
Communication takes place within and between systems, as exemplified in inpatient, transmural, and outpatient care and within the chain of pre-, intra-, and postoperative care. Communication may involve a large group of people such as surgeons, nurses, support staff, anesthesiologists, and include a range of critical issues, such as patient status, intraoperative events, and care plan. Most communication deficits occur within a single department, but can also occur between departments and between different institutions. The majority of errors in communication result from verbal communication. Reducing the number of communication errors could significantly reduce the number of medical errors and, hence, increase patient safety (Finn, 2001; Gandhi et al., 2014; Greenberg et al., 2007; Mrayyan, 2006).
Medical errors, especially those caused by communication failures, are an omnipresent problem in today’s health care organizations. In the perioperative period for instance, the prevalence of communication deficiencies is high. In an observational study of 48 surgical cases with 421 identified communication events, one third were classified as “failures” (Greenberg et al., 2007).
An analysis by the Joint Commission for Hospital Accreditation showed that 70% of 2,455 accidents in health care were caused by defective and faulty communication within a team (Leonard et al., 2004). Medical errors are predominantly the consequence of a system failure and cannot be reduced to an individual mistake. The majority of errors are made in high-risk environments such as the trauma setting (Courtenay et al., 2013). In the past, patient risks were attributed to the extent of the disease, comorbidities, and the difficulty of the procedure, with negligible focus on the role of caregivers. In the past decade, this viewpoint has changed. With the growing importance of patient safety, the influence of the health care provider on health outcomes is emphasized. Experts argue that the quality of communication between health care providers and the environment determines medical errors (Greenberg et al., 2007). Indeed, “these errors have the potential to cause severe injury or unexpected patient death” (O’Daniel & Rosenstein, 2008, p. 272). In addition, communication problems have an economic impact and may result in decreased access to care (Brock et al., 2013; Leonard et al., 2004; Thorsteinson, 2003).
Communication and Communication Satisfaction
In non–health care settings, communication has been studied as a contributor to job satisfaction and job performance (Pincus, 1986). By performing a factor analysis, Downs and Hazen (Wagner et al., 2015) identified eight dimensions of “communication satisfaction”: (a) communication climate (general satisfaction with the communication environment), (b) supervisor communication, (c) media quality, (d) horizontal communication, (e) organizational integration (information relevant to performing job), (f) personal feedback, (g) organizational perspective (information about organization as a whole), and (h) subordinate communication (for supervisors only). Their “Communication Satisfaction Questionnaire” is based on these dimensions. Two studies (Kaddourah, Khalidi, Abu-Shaheen, & Al-Tannir, 2013; Pincus, 1986) identified the first, second, and sixth dimension as the strongest predictors of job satisfaction. The other dimensions were also associated with job satisfaction. Only the second and sixth dimensions were associated with job performance (Pincus, 1986).
This positive association between communication satisfaction and job satisfaction has been demonstrated among nurses as well (Manojlovich & Antonakos, 2008; Mokoka, Ehlers, & Oosthuizen, 2011; Probst, Baek, & Laditka, 2010; Squires et al., 2015). Communication satisfaction with one’s supervisor has been shown to be associated with greater organizational commitment (Moideenkutty, Blau, Kumar, & Nalakath, 2001; Probst et al., 2010), which in turn is related to the prevention nursing turnover (Blegen, 1993).
Job Satisfaction, Intention to Leave, and Burnout
It is clear that communication affects job satisfaction and that job satisfaction affects nurses’ turnover. Low job satisfaction can lead to a high turnover, which negatively influences quality of care. Moreover, this causes extra recruitment and training costs for the organization (Probst et al., 2010). Furthermore, patient satisfaction is also influenced by nurses’ job satisfaction. Specifically, high job satisfaction is associated with higher motivation, which in turn is associated with higher patient satisfaction about received care (Tzeng, 2002).
According to Maslow’s needs theory, job satisfaction can be defined as a form of need fulfillment, as “the match of personal needs to the perceived potential of the job for satisfying those needs” or to the perception of rewards associated with the job. In contrast, Herzberg and Mausner’s motivation–hygiene theory rather defines it as “a function of satisfaction with the various elements of the job.” The presence of motivating factors lead to motivated and satisfied employees, whereas hygiene factors do not lead to satisfaction but their absence leads to dissatisfaction (Herzberg & Mausner, 1959). Hygiene factors such as indirect working environment (a hospital’s policies, benefits, leisure activities), salary, and promotion were found to be very important but strongly dissatisfying (Tzeng, 2002). However, each person experiences job satisfaction differently. This is highly dependent on intrinsic and extrinsic attributes. Concrete examples of intrinsic factors are receiving recognition for one’s work, responsibility, ability to make decisions, challenges, performances, and self-actualization. Extrinsic factors include the behavior of executives, wages, organizational culture, working conditions (including sufficient time to perform tasks), and safety in the workplace (Herzberg & Mausner, 1959). The distinction between intrinsic and extrinsic factors is, however, not absolute. Leadership style, for example, is seen as an extrinsic factor but influences job satisfaction additionally through its effect on empowerment (intrinsic; Morrison, Jones, & Fuller, 1997). In the theory of Spector, lastly, the focus is on the cognitive process: “the affective orientation of an employee towards his job.” This can be seen as a global feeling, or rather as a related configuration of attitudes about different features of the job (e.g., appreciation, job conditions, pay, security, personal growth and communication; Aiken et al., 2012; Spector, 1997).
Among nurses, intrinsic factors are especially important (Probst et al., 2010). Nurses get their motivation from protecting the patients’ lives and helping them to stay or to become healthy (Kudo et al., 2010). A review of the literature on job satisfaction among nurses revealed that interaction (with patients, colleagues and managers) is another important source of job satisfaction (Lu, While, & Barriball, 2005). Adams and Bond observed that although nurses want autonomy, they also require the support of good interpersonal relationships (Adams & Bond, 2000). Some studies focused on the importance of a good interaction with the management . Probst et al. (2010) observed that job satisfaction increases when supervisors communicate clearly, provide clear instructions, and show appreciation for the nurses’ work. Others highlight the importance of good coworker relationships (Price, 2002; Tovey & Adams, 1999). A meta-analysis of quantitative studies of nurses’ job satisfaction dating from 1993 revealed, however, only moderate correlations between job satisfaction and communication with supervisors and peers (Blegen, 1993). Thirteen variables were frequently examined with relation to job satisfaction. Four of these were personal attributes or personality traits, for example, age, education, years of experience, and locus of control. The other nine were organizational features or job attitudes: stress, commitment, supervisor communication, autonomy, recognition, routinization, peer communication, fairness, and professionalism. The variables exhibiting the strongest relationship with job satisfaction (correlation coefficients in parenthesis) were stress (.61) and commitment (.53). The following five variables were moderately related to job satisfaction. These were communication with supervisor (.45), autonomy (.42), recognition (.42), routinization (.41), and communication with peers (.36). Variables with small to moderate relationships were fairness (.30) and locus of control (.28). Age (.13), years of experience (.09), education (.07), and professionalism (.06) displayed limited correlations with job satisfaction.
A more recent cross-sectional study confirms that a high workload (due to low staffing) is related to stress, which in turn negatively related to job satisfaction (Kaddourah et al., 2013). In this study, almost 50% of nurses were overworked, dissatisfied with their income, and experienced limited autonomy as well as poor communication with superiors. In another study, seven factors related to nurses’ job satisfaction were identified: the ability to specialize in one’s work, safety at work, relations with supervisors, work–life balance, relationships with other nurses, communication, and wages (Yin & Yang, 2002). Overall, this suggests that there is a need for hospitals and government authorities to strive to implement strategies that alleviate workload and empower nurses to control their practice. The formulation of such strategies requires insights into the mechanisms of job (dis)satisfaction.
The “met expectations theory” is often used to describe job (dis)satisfaction. This theory states that individuals have certain expectations of a job. When these expectations are not met, individuals experience dissatisfaction (Best & Thurston, 2004). However, this theory does not incorporate the possible outcomes of job dissatisfaction, such as staff turnover and turnover intention. Hence, a conceptual model explaining the relationships between job dissatisfaction and staff turnover is useful (Castle, Engberg, Anderson, & Men, 2007, Figure 3).
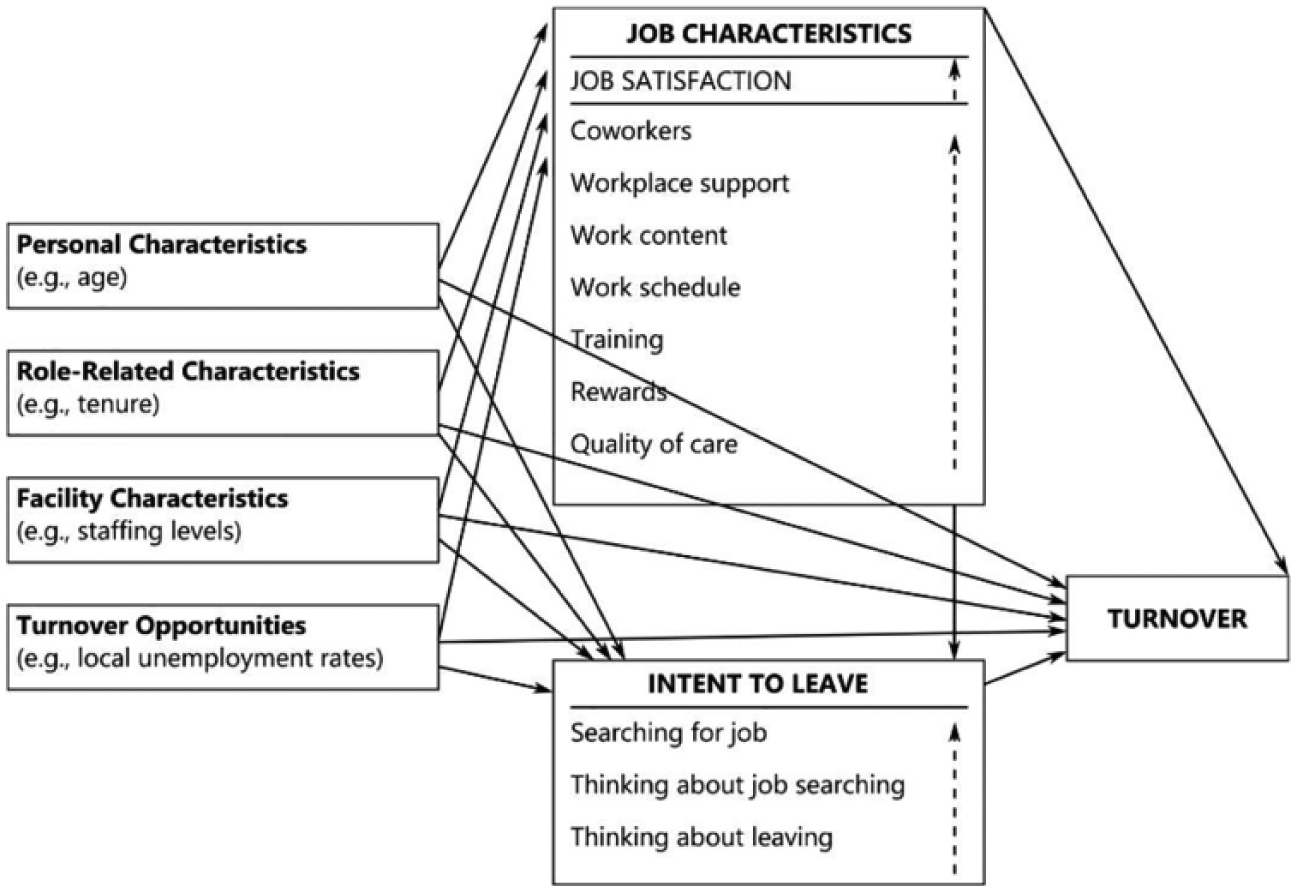
Proposed model for examining intent to leave and turnover of nurses.
According to this model, turnover intention is influenced by personal characteristics (age and gender), role-related characteristics, facility characteristics (staff level), and opportunities to change jobs. These four factors can influence job characteristics and intent to leave. The turnover intention consists of three phases: thinking about leaving, thinking about looking for another job, and actually looking for another job. In each phase, the turnover intention increases. In reality, nurses first experience job dissatisfaction and then proceed to these three phases (Castle et al., 2007; Gauci Borda & Norman, 1997; Yin & Yang, 2002).
Several studies measured the impact of job satisfaction on intention to leave and burnout. Cavanagh and Coffin have found that job satisfaction and job participation are crucial variables in the turnover process, and job satisfaction was correlated with intent to stay (r = .34, p < .05; B. Hayes, Bonner, & Pryor, 2010). A later study found an even higher correlation coefficient (r = .48, p < .005) between the two measures (Gauci Borda & Norman, 1997). A meta-analysis in 2002 (Yin & Yang, 2002) identified job dissatisfaction as one of the strongest factors related to nurse turnover. Two more recent studies confirm this (Castle et al., 2007; Kudo et al., 2010). Unsatisfied nurses reported to be strongly committed to the quality of care, which may be hampered by the experience of high workload (Castle et al., 2007; Sellgren, Kajermo, Ekvall, & Tomson, 2009). Kudo et al. found that the relationship with supervisors is a crucial factor in job turnover. In addition, older nurses were less likely to leave the organization because they have acquired more responsibility, more involvement, and more competencies to cope with problems (Kudo et al., 2010).
Job dissatisfaction is also associated with burnout among health care staff (McHugh, Kutney-Lee, Cimiotti, Sloane, & Aiken, 2011; Piko, 2006). Burnout is “a state of fatigue or frustration brought about by devotion to a cause, way of life, or relationship that failed to produce the expected reward” (Freudenberger & Richelson, 1980, p. 13) . Job dissatisfaction has been found to be associated with each of the three dimensions of burnout, namely, emotional exhaustion, depersonalization, and diminished personal accomplishment (Dolan, 1987; McHugh et al., 2011).
In 2012, an international study on patient safety, satisfaction, and quality of care (Aiken et al., 2012), including 61,168 nurses, from the United States and Europe, showed high levels of job dissatisfaction, turnover intention, and burnout. High rates of nurse burnout were found (ranging from 10% in the Netherlands to 78% in Greece), job dissatisfaction (ranging from 11% in the Netherlands to 56% in Greece), and intention to leave (ranging from 14% in the United States to 49% in Finland and Greece). Among Belgian nurses in this sample, one quarter (730/2,938) reported feeling burned out, 22% (630/3,159) were dissatisfied with their job (ranking fifth on both parameters within the 13 European countries in this report). Even more nurses, 30% (934/3,164), intended to leave their job in the next year.
Recommendations for Improvement of Communication and Communication Satisfaction as a Prerequisite for Increased Job Satisfaction
To prevent these negative outcomes described, interprofessional education, which focuses on helping teams to communicate in appropriate and effective ways, is needed (Brock et al., 2013; B. Hayes et al., 2010; Leonard et al., 2004; Mrayyan, 2006).
“Team Strategies and Tools to Enhance Performance and Patient Safety,” abbreviated as TeamSTEPPS, is an interprofessional communication training model widely used within health teams. This model was developed on the basis of empirical evidence and is the result of a collaboration between the U.S. Department of Defence (as part of their patient safety program) and the agency for health care, research, and quality. The TeamSTEPPS program consists of three phases. The first step consists of an assessment of the communication needs. Second, training and exercises are performed in a controlled and simulated environment. In the final phase, the training program is implemented and maintained in the work situation (Coburn & Gage-Croll, 2011, Figure 4).

Team strategies and tools to enhance performance and patient safety communications model.
Through this program, the competencies of leadership, situation monitoring, mutual support, and communication can be acquired. The training aims to increase mutual respect within a team and to improve the ability to act safely, regardless of the function or role within the team (Coburn & Gage-Croll, 2011). The effectiveness of this method was evaluated in 306 fourth-year medical, third-year nursing, second-year pharmacy, and second-year physician assistant students with 149 students completing a 4-hr training with pre- and postintervention assessments. Positive attitudinal and knowledge effects were seen among these students: significant improvements were found for attitudes toward team communication (p < .001), motivation (p < .001), advocating for patients (p < .001), utility of training (p < .001), and self-efficacy (p = .005). Important attitudinal shifts for TeamSTEPPS skills comprised team structure (p = .002), situation monitoring (p < .001), mutual support (p = .003), and communication (p = .002; Brock et al., 2013; Coburn & Gage-Croll, 2011). TeamSTEPPS has been successfully adapted and implemented to improve patient safety through team training. On one hand, team training increases communication and reduces error; on the other hand, building a patient safety infrastructure supports teamwork (Coburn & Gage-Croll, 2011).
The errors committed by one or more team members need to be discussed openly and minimization needs to be avoided. This is not always guaranteed. Nevertheless, within the health care culture, the emphasis lies on quality of care and delivery of flawless performance. Learning from errors should become more embedded in health care delivery. If errors cannot be openly discussed, individuals experience stress and fatigue, resulting in impaired memory and a limited ability to multitask (Blegen, 1993).
According to Greenberg et al., three interventions exist to reduce communication errors (Greenberg et al., 2007). The first is described as “a set of triggers” (Table 1). When a trigger from this list occurs, a nurse, or other team member involved in the care of the patient, is required to communicate the event with their colleagues. A second method is the use of a “read-back.” This is the repetition of a previously written message, used for confirmation. Finally, protocols for shift handover and transfers are seen as a means to reduce communication deficits.
Proposed Triggers Prompting Communication With the Attending Surgeon Currently Responsible for the Patient.

Source. Adapted with permission from “Journal of the American College of Surgeons” by Greenberg et al. (2007).
Note. ICU = intensive care unit.
Leonard et al. consider the SBAR structure as a solution for such communication problems (Leonard et al., 2004). SBAR stands for situation, background, assessment, and recommendation. “Situation” examines what happens to the patient, “background” investigates the clinical background of the patient, “assessment” analyzes the problem, and “recommendation” determines how the team could resolve the situation. By combining these four descriptions, a short and clear overview of the situation is given, and another caregiver can respond quickly. Leonard et al. (2004) also stress the importance of debriefing to avoid miscommunication and to increase patient safety. Following a procedure or at the end of the day, a brief discussion is held on what the team did well, what challenges arose, and what should be handled in a different manner in the future. A debriefing provides an opportunity to learn, for both the individual and the team.
Discussion
Job satisfaction is a complex and subjective phenomenon, as evidenced by the numerous determinants discussed in this article. Hence, an organization cannot expect to achieve a significant impact with a single targeted intervention, which is not embedded in a multilevel strategy. Our recommendations on interventions and strategies are formulated in “Relevance for Clinical Practice.”
This article presents a comprehensive review of the literature on job satisfaction in relation to communication among nurses and provides a multidimensional overview of this contemporary topic. During the literature search across a number of databases, a vast amount of articles were screened. A limitation of this review is that it has not taken cultural and social contextual factors into account, which may also influence job satisfaction.
Several recommendations can be drawn from the present literature review:
Underline the importance of the psychosocial work environment and the relationship between burnout, role conflict, job satisfaction, and psychosomatic health (problems) in health care staff (Piko, 2006).
Acknowledge that improvements in this field should be a priority and that the implementation of interventions, which focuses on the intrinsic values of nurses can help to prevent job burnout, increase job satisfaction, and reduce turnover. Information on the psychosocial work climate is necessary to provide a basis for such interventions. From a practical perspective, these issues are central to changes in management practices, which should be integrated in continuous reform.
Acknowledge that “cultural change is at the heart of this quest” (Leonard et al., 2004). Care should be transformed from the culture of the individual expert physician to a truly collaborative team environment (Leonard et al., 2004). Currently, different communication styles of physicians, nurses, and others hamper this aim. The complexity of the care system necessitates a change toward a culture of open communication and collaboration. Such change is essential for safeguarding clinical outcomes.
Create and maintain a work environment in which participative management thrives. This can be achieved by increasing psychological empowerment, while reaffirming and strengthening the role as well as the skills of nurse leaders. Spur team development activities ensuring that team members value “the importance of shared responsibility, communication, and collective decision-making, and have a good understanding of their respective roles” (Courtenay et al., 2013, p. 9).
Strive to improve work motivation by creating proper work environments that enhance autonomy and enable nurses to work as specialists. Work motivation can be increased by showing appreciation for work performed well. It is crucial that appreciation is expressed by both the general management as well as the direct leadership of nurse managers, who play a crucial intermediary role at the ward level.
Implement simulation training of interprofessional teams as a first step in establishing improved communication skills within practicing clinical teams.
Embed standardized tools and behaviors into the care process, such as the SBAR method, to improve safety. The value of such communication techniques has already been demonstrated in other high-reliability industries, and they present a valuable resource that can be adapted to present-day medicine.
Give particular attention to situations that are especially vulnerable for or prone to communication breakdown, such as handoffs and transfers in care. These can be dealt with through trigger- or checklist-structured protocolized approaches.
Aim to identify the factors involved within the particular organization and explore their relation with job satisfaction to aid the development of management interventions.
It is imperative that hospital management acknowledge the relevance of enhancing job and communication satisfaction to clinical practice and organizational integrity. Half of the nurses reported being overworked and exhibited a risk profile for burnout and mistakes, in turn compromising patient safety (Kaddourah et al., 2013). Management must provide positive leadership and pay attention to the particular factors that affect nurses to enhance nurse retention, reduce intention to leave, and avoid nurse shortage.
In conclusion, this narrative review explored determinants of effective organizational communication and communication satisfaction, and the extent to which communication satisfaction and job satisfaction are related among nurses. Both are the result of a complex and multifactorial interaction, involving both internal and external factors. Job dissatisfaction is a reliable predictor of burnout and turnover intention. Achieving a balance is important for enabling job satisfaction, which is required for both organizational stability and for guaranteeing patient safety. This can only be achieved through an organization-wide multimodal prevention and intervention program, which aims to optimize different modalities of interprofessional communication, workload, and job satisfaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.