
Abstract
Understanding personal and family support factors influencing lifestyles among older overweight and obese Hispanics with type 2 diabetes is critical for enhancing disease management. A survey was administered to 115 respondents recruited using convenience sampling. Descriptive and inferential statistics were employed for analyses. More than two thirds of participants have never received diabetes education. Family support was significantly associated with diet. Gender, marital status, and education were associated with exercise. Diabetes education was associated with both diet and exercise. Family-based diabetes education in community settings may be an effective strategy for promoting healthy behaviors among older overweight/obese Hispanics.
Introduction
Older Hispanics, one of the most rapidly growing minority groups in the United States, are disproportionately affected by type 2 diabetes and face disparities in several primary drivers of diabetes, namely, the combination of low physical activity, poor dietary intake, and related obesity. While older Hispanics (65 years and older) accounted for 3.7% of the population in 1990 (Markides, Rudkin, Angel, & Espino, 1997), in 2014, this percentage increased to 8% and it is expected to reach 22% in 2060 (Administration for Community Living, 2015). Diabetes prevalence rates among older Hispanics have almost doubled in the past two decades (from 20.3% to 37.2%) and are 2 times higher for this group relative to their older non-Hispanic White counterparts (Beard, Al Ghatrif, Samper-Ternent, Gerst, & Markides, 2009; Borrell, Crawford, Dallo, & Baquero, 2009); the prevalence of obesity (body mass index [BMI] above 30) among middle-aged and older Hispanics with type 2 diabetes ranges from 28.1% to 47.6% (Ory et al., 2009; Oster et al., 2006). Persons with type 2 diabetes who are also obese are at high risk of decreased glycemic control, reduced quality of life, and a rapid progression of diabetes complications and other comorbidities, including persistent hyperglycemia, hypertension, cardiovascular disease, myocardial infarction, cerebrovascular stroke, and end-stage renal disease (Poljicanin, Pavlic-Renar, & Metelko, 2011; Ross et al., 2011).
According to a model of determinants and processes of health behavior change proposed by Ory and colleagues (2009), personal and social factors influence health behaviors (Ory, Smith, Mier, & Wernicke, 2010). The diabetes literature shows an association between self-care behaviors and factors including gender (Albright, Parchman, & Burge, 2001; Bell et al., 2005), older age (Albright et al., 2001; Bai, Chiou, & Chang, 2009; Chang, Chiou, Lin, Lin, & Tai, 2005; Skelly et al., 2005), higher education attainment (Bai et al., 2009; Chang et al., 2005), being exposed to diabetes education (Johnston et al., 2006), and having positive social support (Albright et al., 2001; Tang, Brown, & Funnell, 2008; Wen, Shepherd, & Parchman, 2004). However, little is known about the contextual factors influencing lifestyles among older overweight and obese Hispanics with type 2 diabetes.
Hispanic individuals are adversely affected by a combination of low physical activity levels and low rates of healthy eating, and high related obesity rates. A large study measuring physical activity among middle-aged and older adults found that Hispanic adults were less likely to report walking (leisure-time) and vigorous physical activity than non-Hispanic adults (Sorkin, Biegler, & Billimek, 2015). Data from the National Health and Nutrition Examination Survey (2001-2006) indicated that the rates of individuals reporting eating at least five servings a day of fruits and vegetables was uniformly low (less than 30%) among non-Hispanic White adults and Hispanic individuals (King, Mainous, Carnemolla, & Everett, 2009). Data from 2009 to 2012 indicate that the percentage of U.S. adults who were obese was 36% for females and 35% for males in the general population; however, the rates were higher for Hispanic individuals (of Mexican decent) at 46% for females and 40% for males along the same timeline (National Center for Health Statistics, 2015).
Although self-care behaviors such as healthy eating and exercise are known to reduce obesity (Church, 2011); improve glycemic control, blood pressure, and lipid profile; and decrease diabetes-related complications (The Diabetes Prevention Program [DPP], 2002; Norris et al., 2002; Rhee et al., 2005), health promoting self-care behaviors are less prevalent among Hispanics with type 2 diabetes, especially when compared with their non-Hispanic counterparts (Brown et al., 2003; Coronado, Thompson, Tejeda, Godina, & Chen, 2007; Harris, Eastman, Cowie, Flegal, & Eberhardt, 1999; Nothwehr & Stump, 2000; Nwasuruba, Khan, & Egede, 2007; Nwasuruba, Osuagwu, Bae, Singh, & Egede, 2009; Thackeray, Merrill, & Neiger, 2004). Research shows demographics, physical and mental health (including disease comorbidities), disease duration, diabetes education, and social support influence self-care behaviors among individuals with diabetes (Albright et al., 2001; Bai et al., 2009; Bell et al., 2005; Gonzalez et al., 2007; Gonzalez et al., 2008; Huang, Courtney, Edwards, & McDowell, 2010; Johnston et al., 2006; Park, Hong, Lee, Ha, & Sung, 2004; Skelly et al., 2005; Toljamo & Hentinen, 2001; Wen, Parchman, & Shepherd, 2004; Wen, Shepherd, & Parchman, 2004). Factors known to be associated with exercise among persons with diabetes include having low income and low educational attainment, as well as being female, of older age, and obese (Morrato, Hill, Wyatt, Ghushchyan, & Sullivan, 2007; Nelson, Reiber, & Boyko, 2002). Other studies found lack of time, low family support, and poor access to equipment and facilities may influence participation in exercise programs among adults with diabetes (Foreyt & Poston, 1999; Korkiakangas, Alahuhta, & Laitinen, 2009; Mier, Medina, & Ory, 2007). Depression has been found to be negatively correlated with healthy eating and exercise (Gonzalez et al., 2007; Gonzalez et al., 2008; Park et al., 2004). Researchers documented that adults with diabetes who are also obese perceive exercise as a painful activity, which negatively affects their adherence to recommended physical activity regimens (Foreyt & Poston, 1999). However, there is paucity of studies examining the association of the previously documented factors with self-care behaviors among older Hispanics with type 2 diabetes who are also overweight or obese. Understanding these factors may provide significant insights for the development of culturally appropriate community health interventions to address both diabetes overweight and obesity status among older Hispanics. This is of particular importance considering that research shows that participation of older Hispanics in diabetes management programs is lower than their non-Hispanic counterparts (Coronado et al., 2007; Harris, 2001).
Guided by the model of determinants and processes of health behavior by Ory and colleagues (2010), and considering the research gap examining personal and family support factors influencing lifestyles among older overweight and obese Hispanics with type 2 diabetes, the objectives of this study were to (a) identify levels of healthy eating and exercise between overweight and obese older Hispanics with type 2 diabetes living in the Texas-Mexico border region and (b) investigate factors associated with diet and exercise among this population. Factors examined included personal factors (demographics), health factors (obesity status, diabetes duration, number of comorbid conditions, exposure to diabetes education), and perceived family support.
Method
Participants and Procedures
Data for this study were drawn from a larger cross-sectional study based on a community assessment conducted in 2008 in Hidalgo County, Texas, which included 249 Hispanics aged 60 years and older with type 2 diabetes. Hidalgo County, located at the Texas-Mexico border, is one of the poorest counties in the United States (Webster & Bishaw, 2007) and the majority of its population is of Hispanic of Mexican descent (83.9%; U.S. Census Bureau, 2005-2007). A convenience sampling technique was used to recruit participants from both community and clinical settings, which included senior centers, a community health clinic, and low-income neighborhoods known as colonias. Study eligibility criteria included being Hispanic, 60 years of age and older, and having been diagnosed with diabetes (self-report). Trained certified promotoras and graduate students used a structured questionnaire to interview participants. The questionnaire was administered in English or Spanish according to respondents’ preferences. All participants who agreed to participate signed a consent form. This study was approved by the Texas A&M University Institutional Review Board.
For purposes of this secondary analysis study, a sample was extracted from the larger parent study and composed of participants who were overweight or obese based on the BMI measurement. Only participants who were overweight or obese were purposively selected to assess participants at greater risk for diabetes-related complications. Furthermore, because the focus of this study surrounds nutrition and physical activity, differences between these sample subgroups can yield findings to guide specific recommendations based on associated guidelines for diet and exercise. BMI was calculated from height and weight measured by trained data collectors and converted into metrics of meters and kilograms, respectively. Participants’ weights were divided by heights and rounded to the nearest tenths. In this study, BMI is categorized as overweight (BMI = 25.0 to 29.9 kg/m2) and obese (BMI ≥ 30.0 kg/m2). Our final sample included 115 Hispanics aged ≥ 60 years with type 2 diabetes and who were overweight or obese.
Measures
Dependent variables
Diet and exercise were measured using five items from the revised version of the Summary of Diabetes Self-Care Activities. This scale assesses the frequency of self-care behaviors. Participants were asked to report the number of days they performed behaviors related to diet and exercise within the past week. Scoring of items uses the days per week on a scale of 0 to 7. Greater number of days indicates better self-care. A previous study using this scale reported the average interitem correlations between items to be high (M = 0.47; Toobert, Hampson, & Glasgow, 2000). Validity and reliability of the Spanish scale version administered among Hispanic Spanish-speaking participants has been previously reported by other researchers (Cronbach’s α = .68; Vincent, McEwen, & Pasvogel, 2008; Wen, Shepherd, & Parchman, 2004). Our sample data yielded a Cronbach’s alpha of .64, which is comparable to previous results; however, the average of interitem correlations between the scale items was lower than previously reported in the literature (i.e., M = 0.13).
To measure diet, we collected responses from the following three questions: Q1: “How many of the last seven days have you followed a healthful eating plan?” Q2: “On average, over the past month, how many days per week have you followed your eating plan?” and Q3: “On how many of the last seven days did you eat five or more servings of fruits and vegetables?” The summed score for these diet items was used as one of the dependent variables for this study. The interitem correlations of these three diet items were .85Q1toQ2, .46 Q1toQ3, and .43Q2toQ3, which varied a little more than correlations (.55 to .67) for these items in another study (Toobert & Glasgow, 1994), and the Cronbach’s alpha for these three items was .81. Factor analysis also showed these three items were closely related (i.e., they loaded on the first factor that explained 46% of variance in this diet construct).
To measure exercise, we collected responses from two items: “On how many of the last seven days did you participate in at least 30 minutes of physical activity? (including walking)” and “On how many of the last seven days did you participate in a specific exercise session (such as walking) other than what you do around the house or as part of your work?” The interitem correlation for these items was .52. The summed score for these exercise items was used as one of the dependent variables for this study.
Personal factors
Demographic variables included age group (60-64, 65-74, 75 or older), sex (male, female), marital status (married, unmarried), education level (less than high school, high school or more), living situation (living with someone, living alone), and residential location (lives in a colonia, does not live in a colonia).
Health factors
These variables included duration of diabetes, comorbid status, obesity status, and exposure to diabetes education. Duration of diabetes was calculated based on respondent’s birth date and age when diagnosed with diabetes (self-report); this variable was dichotomized as <10 years versus ≥10 years. A measure of comorbid status was calculated by summing the number of reported chronic conditions (in addition to diabetes) dichotomized for cross-tabulations into those who experienced less than three conditions versus those who reported three or more conditions. Because we excluded normal/underweight persons, the BMI categorical variable was dichotomized as overweight versus obese. Participants were asked if they ever received diabetes education—using the question, “Have you ever taken a course or class in how to manage your diabetes yourself?” (yes, no).
Family support
Family support was measured using the supportive subscale of The Diabetes Family Behavior Checklist (Glasgow & Toobert, 1998), which consists of nine items assessing support in the following four domains: medication taking, glucose testing, exercise, and diet. Responses were rated on a 5-point Likert-type scale coded as 1 = never, 2 = twice a month, 3 = once a week, 4 = several times a week, and 5 = at least once a day. A summary score from 9 to 45 was generated with higher scores indicating more supportive behaviors. Respondents were asked to think about one family member with whom they generally have the most contact and rate how often the family member performed each of the nine positive or supportive behaviors. The positive rating score has yielded an internal consistency of .71 (Glasgow & Toobert, 1998). A Spanish version of the scale has been created and used with Hispanics (Wen, Shepherd, & Parchman, 2004). For analyses purposes, the family support variable was dichotomized at the scale midpoint as low (score ≤ 26) versus high (score ≥ 27) family support.
Statistical Analyses
Data analyses were conducted using SPSS (Version 22). Descriptive statistics were used to compare average diet and exercise scores among different groups defined by independent variables. Pair-wise explorations on single factor’s effect on the dependent variables were performed using nonparametric tests including Mann–Whitney U test and Kruskal–Wallis test, because diet and exercise scores dramatically violated normality assumptions. Multiple linear regression models were used to examine the association between the independent variables and diet and exercise scores, respectively. Both full and reduced models were considered. The reduced model was constructed using predictors that were identified from pair-wise exploration. The model fit statistics (Bayesian information criteria [BIC], R2, and adjusted R2) are reported, which were used to justify the inclusion of reduced regression models. Each of the hypothesized models was found to jointly predict the corresponding dependent variable according to model fitting criteria and residual analysis. The effect sizes of the models were reported by R-squared and adjusted R-squared.
Results
Table 1 shows the averages of diet and exercise scores categorized by independent variables. Diet scores were significantly higher among respondents who had received diabetes education (p = .005) and/or reported high family support (p = .019) compared with those with no diabetes education and/or with low family support. Exercise scores were significantly higher among respondents who were male (p = .049), were married (p = .038), had a high school education or more (p = .006), and/or received diabetes education (p = .039) compared with their respective counterparts. These findings were used to guide the creation of full and reduced models in the following multivariate analyses.
Pair-Wise Explorations Between Each of Participants’ Characteristics (Predictors) and Diet and Exercise Scores, Respectively.
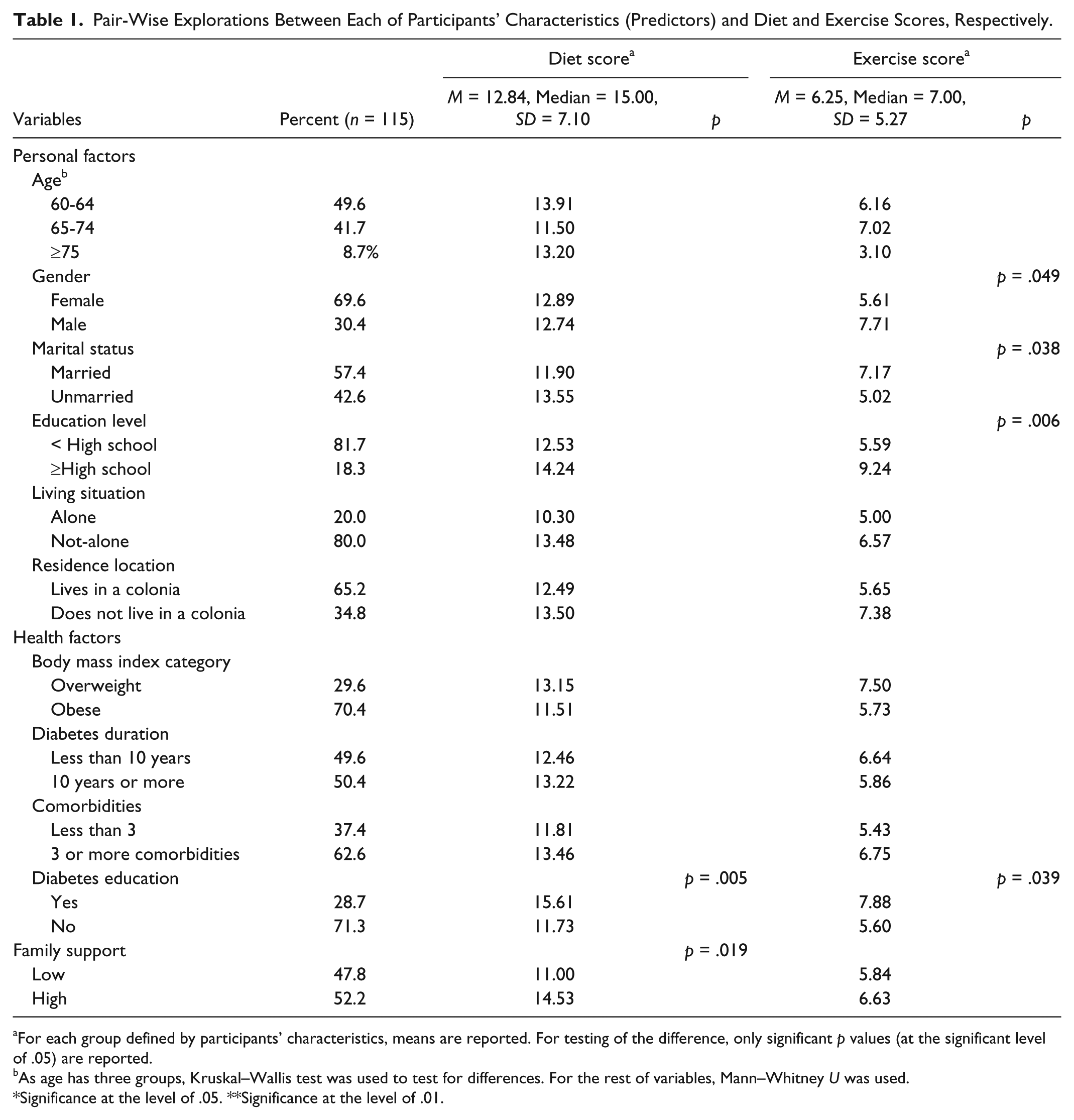
For each group defined by participants’ characteristics, means are reported. For testing of the difference, only significant p values (at the significant level of .05) are reported.
As age has three groups, Kruskal–Wallis test was used to test for differences. For the rest of variables, Mann–Whitney U was used.
Significance at the level of .05. **Significance at the level of .01.
Table 2 reports results of multiple regression models in which the diet score served as the dependent variable. Because exploratory analyses indicated social factors were of importance to diet score, we considered two multiple regression models: Model 1 contained diabetes education exposure and family support level. Model 2 was the full model including all independent variables except marital status and diabetes duration. In Model 1, the average diet score for respondents who reported receiving previous diabetes education was 3.16 more than for respondents without diabetes education. The average diet score for respondents who reported high family support was 2.90 more than that for respondents with low family support. Family support effect was not significant in the full model (Model 2). Similarly, living situation and obesity also showed higher predictive power for the diet score.
Results From Multiple Regression Models For Dependent Variable, Diet Score.
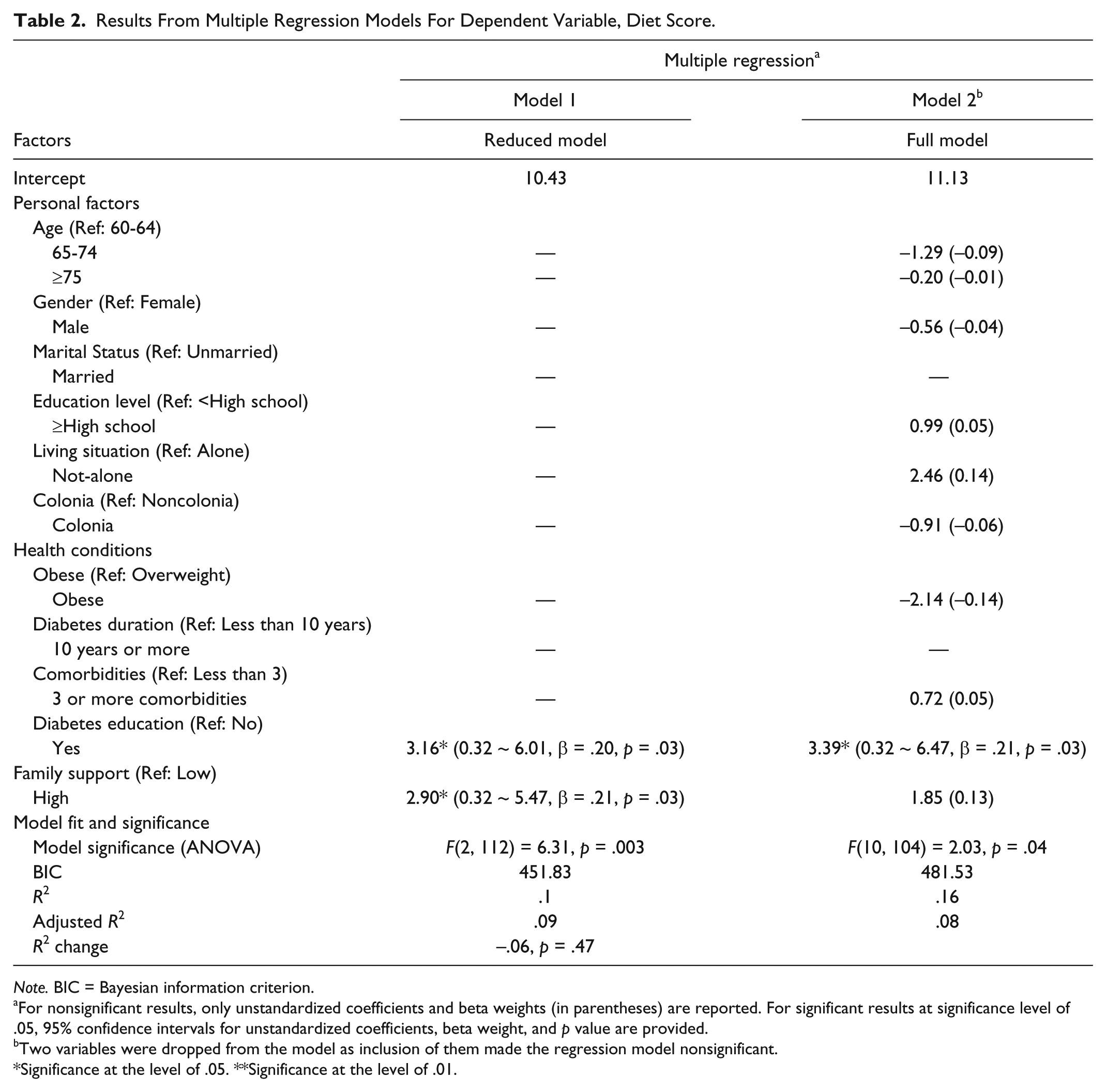
Note. BIC = Bayesian information criterion.
For nonsignificant results, only unstandardized coefficients and beta weights (in parentheses) are reported. For significant results at significance level of .05, 95% confidence intervals for unstandardized coefficients, beta weight, and p value are provided.
Two variables were dropped from the model as inclusion of them made the regression model nonsignificant.
Significance at the level of .05. **Significance at the level of .01.
Table 3 reports results of multiple regression models in which the exercise score served as the dependent variable. Because the pair-wise exploration indicated personal factors were important to exercise score, we considered two multiple regression models: Model 1 contained only personal factors; Model 2 is full model including all independent variables. Respondents who had high school or higher education reported significantly higher exercise average (3.31 in Model 1 and 2.79 in Model 2) than respondents with less than high school education. Even though other personal factors did not yield significant results, their beta weights indicated they had higher predictive power for the exercise score. For health condition and social factors, only two factors, obese and diabetes education, had relatively large beta weights.
Results From Multiple Regression Models For Dependent Variable, Exercise Score.

Note. BIC = Bayesian information criterion.
For nonsignificant results, only unstandardized coefficients and beta weights (in parentheses) are reported. For significant results at significance level of .05, 95% confidence intervals for unstandardized coefficients, beta weight, and p value are provided.
Significance at the level of .05. **Significance at the level of .01.
Discussion
This study adds to the nascent literature investigating personal, health, and family support associated with self-care practices (i.e., diet and exercise) among an overweight and obese older Hispanic population with type 2 diabetes living in one of the poorest areas of the U.S-Mexico border region. Study findings support the tenets of the model of determinants and processes of health behavior change proposed by Ory and colleagues (2009), which suggests that personal characteristics and social factors influence health behaviors (Ory et al., 2010). In this study, results indicate that contextual factors influenced diet and exercise behaviors among study participants.
Findings from this study indicate higher exercise scores were reported among males and married individuals than their respective counterparts, which is confirmed by previous research (Albright et al., 2001). Our study also found that participants with a higher education attainment had better exercise scores when compared with those with lower education (Bai et al., 2009; Morrato et al., 2007). These findings suggest community health programs targeting overweight and obese older Hispanics with diabetes should place additional recruitment-related effort to purposively reach females, unmarried individuals, and those with low education. Furthermore, community-based organizations serving Hispanic individuals with diabetes should tailor program offerings and associated content to ensure materials and activities are appropriate for individuals of all education levels (e.g., reading levels), which also resonate with the target population.
Our findings show diabetes education is significantly associated with diet and exercise among older Hispanics with diabetes and who are overweight or obese, which confirms previous research from the Behavioral Risk Factor Surveillance System, the National Health and Nutrition Examination Survey with predominately overweight and obese samples (≥18 years), and other studies involving elderly Hispanics aged 55 and older (Brown et al., 2003; Coronado et al., 2007; Harris et al., 1999; Nelson et al., 2002; Nothwehr & Stump, 2000; Nwasuruba et al., 2007; Nwasuruba et al., 2009; Thackeray et al., 2004; Wen, Parchman, & Shepherd, 2004; Wen, Shepherd, & Parchman, 2004). However, more than two thirds of participants (71.3%) in our study reported they have never received diabetes education, a much higher percentage compared with the U.S. adult population with diabetes (57.4%; Centers for Disease Control and Prevention, 2010). Further research is warranted to investigate the role and effectiveness of community health settings to disseminate self-management diabetes programs for older Hispanics living in underserved areas who are also overweight and obese. Settings where diabetes programs could be implemented include senior and community centers, adult day care centers, and other outreach venues utilized by federally qualified community health centers. Previous studies indicate that dissemination of diabetes self-management programs in community settings improve the health status and access to medical care among persons with diabetes (Lorig, Ritter, & González, 2003; Shortell et al., 2009).
Another salient finding in our study is the significant association between perceived family support and higher diet scores. This finding confirms a previous study conducted among older Hispanics (aged 55 years and older) with type 2 diabetes showing that family support resulted in fewer barriers to diet self-care and increasing diet scores (Wen, Parchman, & Shepherd, 2004; Wen, Shepherd, & Parchman, 2004). Although our study found family support to be associated with higher diet adherence, only 52.2% of the participants in this study reported to perceive high levels of support from their families. These findings suggest that health providers and community-based health programs should consider involving the entire family in their diabetes education efforts. Previous research indicates that involving the family in diabetes education programs is effective (Bai et al., 2009; Wen, Parchman, & Shepherd, 2004; Wen, Shepherd, & Parchman, 2004). In addition, it is possible that many older Hispanics do not drive or do not have the transportation means to attend diabetes programs on their own, thus they may rely on other family members to get them to programs (Foley, Heimovitz, Guralnik, & Brock, 2002). It is also worth noting that in Hispanic communities, intergenerational homes are common, therefore, family involvement in diabetes programs may be an important resource for self-care behaviors among older adults.
Limitations
This study is not without limitations. The study design was cross section with no comparison groups, and it was nonrandomized; therefore, causal inferences cannot be made. Both the dependent and independent variables were measured using a self-report instrument, which could have introduced some level of “same source” biases as well as social desirability biases. Another limitation is that we used a convenience sampling technique with a relatively small sample, which may reduce the ability to generalize our findings beyond our study population to Hispanics with similar demographic characteristics.
Disease self-management strategies for overweight and obese persons with diabetes are usually the same as for those who are not obese; the primary strategy is to encourage healthy eating and exercise (Hauner, 2004). It is worth noting that lifestyle programs addressing obesity may be challenging for many individuals with diabetes (Bakris, Weir, & Sowers, 1996) particularly seniors (Mier, Ory, Zhan, Wang, & Burdine, 2007); however, randomized controlled trials indicate behavioral interventions can be effective in producing weight loss and fitness results among obese people with diabetes (Neuhouser et al., 2012; Stern et al., 2004; Unick et al., 2013; Wadden et al., 2011; Woo et al., 2007). Yet, there is scarce research examining determinants of diabetes self-care behaviors as well as effective behavioral change strategies among older Hispanics who are overweight or obese. This study documents that among this population, family support was significantly associated with diet; gender, marital status, and educational attainment were associated with exercise; and diabetes education was associated with both diet and exercise. Understanding these factors could provide valuable insights to design and promote community-based diabetes self-management programs for older Hispanics with an emphasis on weight issues. Community health programs should also be inclusive of families and social support networks. Researchers and diabetes educators should pay particular attention to older adults who are female, not married, low educated, and who have ever received diabetes education.
In addition, there was limited information about neighborhood factors that may influence physical activity, aside from whether individuals lived in colonias. Identifying neighborhood walkability and safety may also play a role in one’s decision to engage in physical activity. Therefore, future research should include neighborhood factors that may influence physical activity. Furthermore, the availability of sources of healthy food (e.g., food markets with fresh fruits and vegetables) was not considered. Identifying the presence of food deserts or the availability of fast food sites should be incorporated into future studies. Adding these geospatial aspects will allow for a more complete picture of factors influencing obesity-related outcomes.
Conclusion
Policy makers and other decision makers, in addition to community partners, are seeking to identify effective strategies that target and ameliorate health disparities, particularly related to preventable obesity and associated conditions including diabetes, among this growing population of Hispanic older adults. Therefore, identifying factors that work to increase physical activity and increase healthful dietary habits are two critical components to combating the obesity epidemic and associated chronic conditions. Our findings can help to inform stakeholders about the role of multiple factors related to obesity and thereby positive aging (e.g., aging in place, increasing the number of years of high quality of life) among this vulnerable population. More attention, funding, and research should be directed to understanding the role of both individual and neighborhood factors that influence obesity-related behaviors among Hispanic individuals in this border region both in and out of the colonias in addition to the broader Hispanic population, especially given the already present health disparities facing these individuals. Doing so will enable greater awareness and allow for informed targeted efforts to increase positive aging among this rapidly growing older adult population in the years to come.
Footnotes
Authors’ Note
This study was conducted as part of a Community Assessment with support and input from Nuestra Clinica del Valle, the Texas A&M University CHUD Colonias program, the Office of Border Affairs for the Texas Health and Human Services Commission, the Lower Rio Grande Valley Area Agency on Aging, and the Research Development and Enhancement Awards Program, the School of Public Health McAllen Campus of the Texas A&M Health Science Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.