
Abstract
We examined whether locus of control (LOC) moderates the apparent relationship between perfectionism and postpartum depression (PPD). It was predicted that external LOC would moderate the relationship between self-oriented perfectionism and PPD, and socially prescribed perfectionism and PPD. A sample of 243 women completed an online self-report questionnaire assessing perfectionism, LOC, and PPD. Self-oriented and socially prescribed perfectionism were significantly associated with PPD. Increased personal loci of control (i.e., low external LOC and high internal LOC) moderated (strengthened) the relationship between perfectionism and PPD. LOC may be an important concept and one of the underlying factors at work in the perfectionism–PPD relationship. This outcome may be attributed to the self-directed nature of self-oriented perfectionists.
Postpartum depression (PPD) is a debilitating mood disorder, and is characterized by a perinatal onset any time between the third trimester of pregnancy to 4 weeks postpartum (American Psychiatric Association, 2013). PPD symptoms mirror major depression and include pervasive low mood, sleep disturbances, weight changes, poor coping, impaired concentration, anxiety, feelings of worthlessness or guilt, and reduced confidence and self-esteem (O’Hara & McCabe, 2013; O’Hara & Swain, 1996). PPD symptoms may reduce the mother’s parenting capacity, and her PPD symptoms may persist into a major depressive disorder (Post and Antenatal Depression Association, 2013). Consequently, the infant can suffer lifelong effects leading to an insecure attachment, impaired socioemotional functioning, attention deficits, and behavioral disturbances (Chabrol & Callahan, 2007). Many women fail to seek a treatment for PPD, however, believing their symptoms are those typical of the baby blues (Post and Antenatal Depression Association, 2013). The baby blues are characterized by transient symptoms that usually pass within 2 weeks post birth, whereas PPD symptoms are more pervasive and have a greater impact on the mother and child. While the literature is rich for certain types of risk factors, other areas remain underresearched. For example, perfectionism and locus of control (LOC) are two factors that, despite associations with PPD, have been largely neglected.
Perfectionism remains a contentious concept, although growing consensus suggests it is characterized by the setting of high standards coupled with extreme self-critical evaluations (Hamachek, 1978; Hewitt & Flett, 1991a). At low levels, perfectionism is considered adaptive and linked to positive affect (Frost, Heimberg, Holt, Mattia, & Neubauer, 1993), while at high levels, it is considered maladaptive and a risk factor for depression (Dimitrovsky, Levy-Shiff, & Schattner-Zanany, 2002). A common conceptualization divides perfectionism into three dimensions. Self-oriented perfectionism is characterized by the standards one holds for the self; socially prescribed perfectionism is defined by the standards one thinks society holds for them; and other-oriented perfectionism is characterized by the standards one holds for others (Hewitt & Flett, 1991a, 1991b). This approach is taken in the present study.
Positive associations have been identified between self-oriented perfectionism and depression (Hewitt & Flett, 1991a), and between socially prescribed perfectionism and depression (Shafran & Mansell, 2001). Hewitt and Flett (1991a) claimed that both dimensions are pivotal to predicting depression. It is argued that self-oriented perfectionists generate their own failures as they tend to set unrealistically high standards and stringently critique their performance, which leads to increased failure. Ashby, Rice, and Martin (2006) supported this claim by identifying moderate to strong effect sizes (r = .38-.68) for maladaptive perfectionism (defined as self-oriented perfectionism) and major depression. The researchers concluded that self-worth and self-criticism play a central role for perfectionists with depression. While this research has focused on the link between perfectionism and depression, there is suggestion of a similar relationship between perfectionism and PPD (e.g., Gelabert et al., 2012; Mazzeo et al., 2006; Oddo-Sommerfeld, Hain, Louwen, & Schermelleh-Engel, 2016). For example, Mazzeo et al. (2006) identified a link between socially prescribed perfectionism and PPD (r = .34) among 1,119 female twins. The perfectionism–PPD relationship also has to be understood in relation to perceptions of LOC as it may have important implications for identifying women at risk of PPD.
LOC is characterized as an individual’s perceived ability to exercise control over the outcome of life events (Rotter, 1966). The theory purports that people with an internal LOC (“internals”) believe they are in control of the outcomes in their life, whereas people with an external LOC (“externals”) believe their life outcomes are left up to chance/fate (Rotter, 1966). External LOC was later expanded to include an additional dimension of “powerful others,” whereby control is placed with other people such as parents, teachers, or doctors (Levenson, 1973). Internals do not have greater control over their life, just the perception that they do, consequently, they are more emotionally adjusted, whereas externals feel powerless to achieve their outcomes. Dimitrovsky, Perez-Hirshberg, and Itskowitz (1987) concluded that externals may be more sensitive to external influences and have extreme responses to critical life events such as childbirth.
Perfectionism theory purports that high level self-oriented perfectionism and socially prescribed perfectionism are maladaptive (Hamachek, 1978) due to self-oriented perfectionists generating their own failures and socially prescribed perfectionists experiencing cognitive dissonance (Hewitt & Flett, 1991a). LOC theory characterizes externals as maladaptive, as externals feel powerless (Rotter, 1966). Thus, the concept of uncontrollability exists both in the literature for LOC (external) and perfectionism (socially prescribed perfectionism). Despite this theoretical connection between maladaptive perfectionism and LOC, few studies have investigated this relationship alongside PPD.
Empirical evidence shows that socially prescribed perfectionism, self-oriented perfectionism, and external LOC are all independently linked with PPD (Hewitt & Flett, 1991a). Hewitt and Flett (1991b) found external LOC to be positively associated with socially prescribed perfectionism, r = .20. They asserted that self-oriented perfectionists with internal LOC can be proactive in changing their standards, whereas socially prescribed perfectionists with external LOC are more reactive (Hewitt & Flett, 1991b). Recent studies have found similar results between maladaptive perfectionism and high levels of external LOC (Periasamy & Ashby, 2002; Stewart & De George-Walker, 2013).
The present study investigates (a) the associations between perfectionism, LOC, and PPD; and (b) whether LOC moderates the relationship between perfectionism and PPD. It is hypothesized that both self-oriented and socially prescribed perfectionism will be positively correlated with PPD and external LOC will be positively correlated with PPD. It is also hypothesized that LOC acts as a moderator on the perfectionism and PPD relationship. Finally, it is predicted that high internal LOC and low external LOC will reduce the impact of socially prescribed perfectionism and self-oriented perfectionism on PPD.
Method
Participants
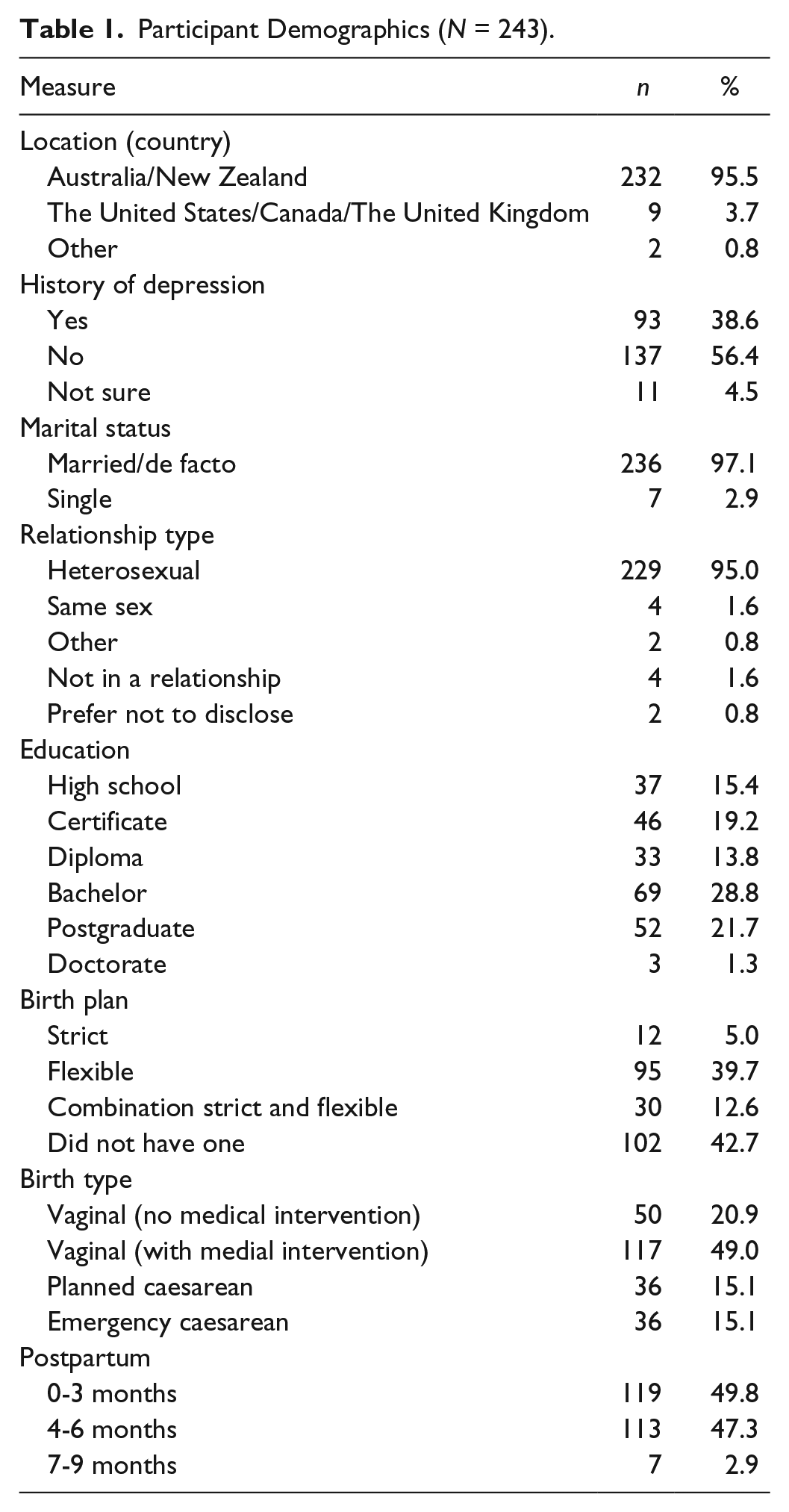
A sample of 326 female participants, including those who had recently given birth to those 9 months postpartum, participated anonymously in the present study. Eighty-one (24.8%) participants were excluded from the final analyses due to not completing all components of the questionnaires, leaving data for 243 participants aged 20 to 42 years (M = 30.40, SD = 4.37). Table 1 shows the key demographics for the sample (e.g., percentage postpartum, education, and relationship status).
Participant Demographics (N = 243).
Materials
The demographic questionnaire included questions pertaining to participants’ age, sex, location, education level, marital status, and history of depression.
The Edinburgh Postnatal Depression Scale (EPDS; Cox, Holden, & Sagovsky, 1987) is designed to screen the likelihood of PPD and suicidality in postpartum women. It is a 10-item scale with each item answered on a 4-point Likert-type scale ranging from 0 to 3 with anchors varied in line with the different questions (e.g., yes, most of the time to hardly at all). Participants respond to statements about how they felt over the last 7 days. A score of 9 or below is considered unlikely to have PPD; 10 to 12, possible PPD; and 13 or above, as likely PPD (Cox et al., 1987). The scale has high construct validity, r = .98 (Glaze & Cox, 1991) and good internal consistency, α = .80 (Teissedre & Chabrol, 2003). The internal consistency for the current sample was excellent, α = .91.
The Hewitt and Flett Multidimensional Perfectionism Scale (HP-MPS; Hewitt & Flett, 1991a, 1991b) has 45 items measuring three subscales: Self-Oriented, Socially Prescribed, and Other-Oriented Perfectionism. Statements are answered on a 6-point Likert-type scale from 1 (disagree) to 6 (agree). Higher scores on any one dimension indicate unhealthier perfectionistic attitudes and behaviors. The HP-MPS is a reliable measure of the severity of perfectionism dimensions, and has adequate concurrent validity and strong test–retest reliability. Using Cronbach’s alpha, the internal consistency for the three dimensions in the current sample was excellent for the Self-Oriented Perfectionism subscale (α = .93), Socially Prescribed (α = .88), and Other-Oriented Perfectionism dimensions (α = .81).
The Internal-External Locus of Control Scale (Levenson, 1973) is designed to determine LOC across three dimensions of internal, external (chance/fate), and powerful others. The 24-item instrument consists of a series of attitude statements that represent commonly held opinions. Participants rate different statements on a 6-point Likert-type scale from −3 (strongly disagree) to 3 (strongly agree). There are eight items on each of the three subscales; the higher the score on a dimension, the more likely that dimension is upheld. Twenty-four points were added to each score to reflect the 24 items. The scale has good construct validity (Levenson, 1973). The internal consistency for the scales are considered moderate to good and range between α = .64 and α = .78 (Richardson, Field, Newton, & Bendell, 2012). For the current sample, the internal scale was acceptable (α = 66), and good for the external (α = .77) and powerful others scales (α = .83).
Procedure
Ethical approval was obtained from the relevant university body (approval code HE14-126). Participants were recruited over a period of 12 weeks from social media channels (e.g., postnatal depression support websites such as PANDA and parenting forums on social media such as Canberra Mummy, Baby Centre, and Essential Baby), and PPD support organizations/groups with the facilitator’s permission (e.g., posters in community-based parenting clinics). Participants provided implied consent before commencing the surveys. The testing materials for this project were conducted using an online self-report questionnaire in English hosted by Qualtrics™ Software (Qualtrics, Provo, UT). The order of the questionnaires involved the demographics questionnaire followed by the EPDS, HP-MPS, and LOC. At the conclusion of the questionnaire, participants were thanked for their participation and provided with information about PPD support services. The data used in this study have been made publicly available (Jackman, Thorsteinsson, & McNeil, 2017).
Statistical Analysis
All analyses were run using SPSS (version 21). Moderation analyses were conducted using a SPSS macro, PROCESS model 1; the settings were for 1,000 bootstrap samples for bias correction and to establish 95% confidence intervals and centered predictors (Hayes, 2013). To overcome any reduction in power by performing multiple moderation analyses, one-tailed tests of significance were conducted and a larger sample was recruited (A. Hayes, personal communication, 11 September, 2014).
Results
Of the total sample, 136 participants (56%) had unlikely PPD, with 72 (30%) likely, and 34 (14%) possible. Table 2 shows the means, standard deviations, and correlations for perfectionism, LOC, and PPD. Self-oriented perfectionism, socially prescribed perfectionism, and powerful others LOC, all showed positive correlations with PPD. All perfectionism dimensions were correlated with one another. Internal LOC was positively correlated with all perfectionism dimensions, while external LOC was negatively correlated with all perfectionism dimensions. Powerful others LOC was only correlated with other-oriented perfectionism.
Correlation Matrix and Means and Standard Deviations for Key Measures.
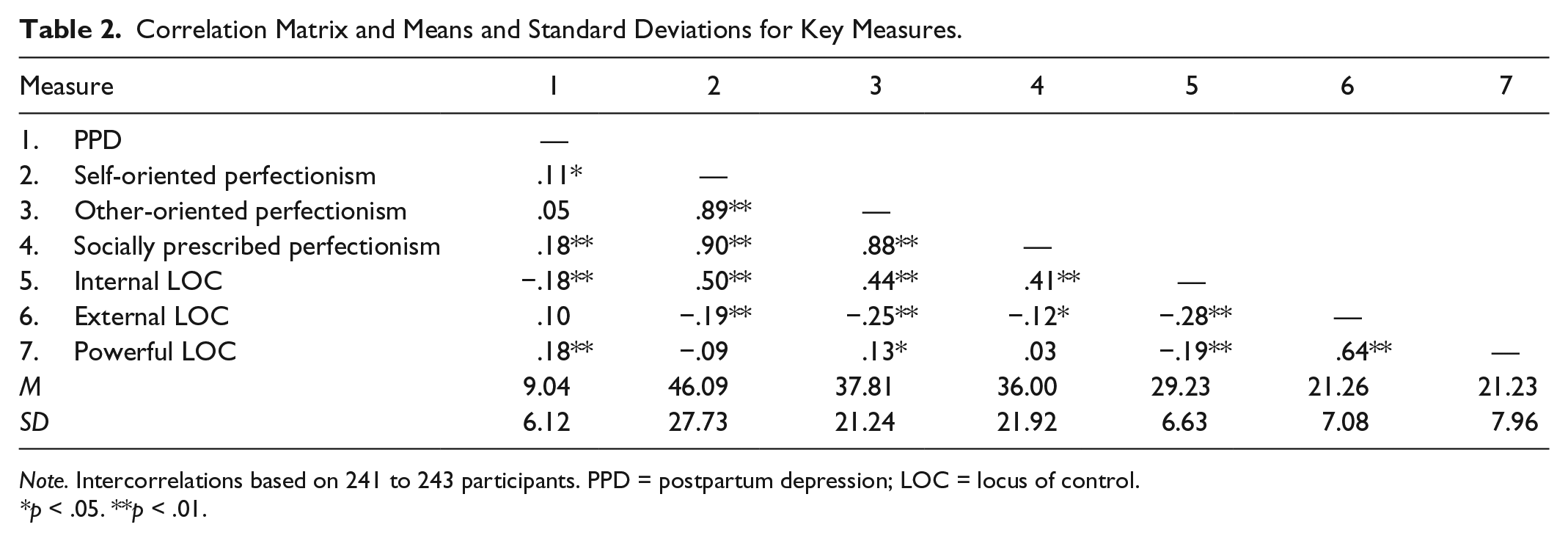
Note. Intercorrelations based on 241 to 243 participants. PPD = postpartum depression; LOC = locus of control.
*p < .05. **p < .01.
External LOC moderated the relationship between socially prescribed perfectionism and PPD, predicting 7% of the total PPD variance (Table 3). As Figure 1a shows, low (raw b = 0.14, p < .001) and medium external LOC (raw b = 0.07, p < .001) accentuated the relationship between socially prescribed perfectionism and PPD. As predicted, external LOC moderated the relationship between self-oriented perfectionism and PPD; thus, the lower the external LOC, the stronger the relationship, see Figure 1b. The moderation model predicted 5% of the total PPD variance. Main effects of external LOC (raw b = 0.22, p < .001) and self-oriented perfectionism (raw b = 0.05, p = .006) were significant. As Figure 1b shows, the interaction is similar to the socially prescribed perfectionism and external LOC moderation model. There was a significant relationship between self-oriented perfectionism and PPD for participants who scored low (raw b = 0.10, p = .03) and medium (raw b = 0.05, p = .02) external LOC.
Significant Interactions for LOC (Internal and External) as a Moderator Between Perfectionism (Self and Social) and PPD.

Note. LOC = locus of control; PPD = postpartum depression; CI = confidence interval.
p < .05. **p < .01.

External LOC as a moderator between (a) socially prescribed perfectionism and PPD and (b) self-oriented perfectionism and PPD.
Internal LOC also moderated the relationship between socially prescribed perfectionism and PPD; however, this relationship was positive; thus, the higher the internal LOC, the stronger the relationship. Overall, the model predicted 12% of the total PPD variance. Main effects of internal LOC (raw b = −0.35, p < .001) and socially prescribed perfectionism (raw b = 0.11, p < .001) were significant. As shown in Figure 2a, a simple slopes plot revealed a significant association between socially prescribed perfectionism and PPD for participants who scored low (raw b = 0.07, p = .002), medium (raw b = 0.11, p < .001), and high (raw b = 0.15, p < .001) internal LOC.

Internal LOC as a moderator between (a) socially prescribed perfectionism and (b) PPD and self-oriented perfectionism and PPD.
Internal LOC also moderated the relationship between self-oriented perfectionism and PPD. Overall, this model predicted 10% of the total PPD variance. Main effects of internal LOC (raw b = −0.38, p < .001) and self-oriented perfectionism (raw b = 0.08, p < .001) were significant. As shown in Figure 2b, a simple slopes plot revealed the interaction to be similar to the socially prescribed perfectionism, PPD, and internal LOC relationship. A significant association was found between self-oriented perfectionism and PPD for participants who scored low (raw b = 0.04, p = .002), medium (raw b = 0.08, p < .001), and high (raw b = 0.13, p < .001) internal LOC.
Powerful others LOC moderated the socially prescribed perfectionism and PPD relationship; thus, the lower the powerful others, the stronger the relationship. The model predicted 8% of the total PPD variance, F(3, 238) = 9.87, p = .03. Main effects of powerful others LOC (raw b = 0.21, p < .001) and socially prescribed perfectionism (raw b = 0.07, p < .001) were significant. Examination of the interaction revealed the interaction to be similar to the external LOC moderation models. A significant association was found between socially prescribed perfectionism and PPD for participants who scored low (raw b = 0.10, p < .001) and medium (raw b = 0.07, p < .001) powerful others LOC.
Main effects of powerful others LOC (raw b = 0.22, p < .001) and self-oriented perfectionism (raw b = 0.04, p = .01) were significant. The interaction, however, was not significant (raw b = −0.005, p = .13). Therefore, powerful others LOC did not act as a moderator between self-oriented perfectionism and PPD.
Discussion
Self-oriented and socially prescribed perfectionism were positively correlated with PPD, supporting the views that high levels of self-oriented or socially prescribed perfectionism is a determinant to increased risk of having PPD. This outcome also corresponds to previous research that suggested high levels of self-oriented and socially prescribed perfectionism may be maladaptive and linked to depression (Shafran & Mansell, 2001). There were also relationships between LOC and PPD in the expected directions. There was only a weak relationship between external LOC and PPD, but there were moderate significant negative association between internal LOC and PPD, and a moderate positive association between the powerful others LOC and PPD. As powerful others LOC is an externally based dimension, these results collectively signify a decreased likelihood of PPD for people who perceive themselves to be in control compared with people who consider external factors responsible for their life.
The hypothesis that external LOC moderates the relationship between socially prescribed perfectionism and PPD, and the relationship between self-oriented perfectionism and PPD, was supported. Participants with low external LOC had a low likelihood of PPD, but only when they were low on perfectionism. In contrast, participants with high external LOC had a high likelihood of PPD, irrespective of their level of perfectionism. Internal LOC strengthened the relationship between perfectionism and PPD. Powerful others LOC had a similar relationship with socially oriented perfectionism and PPD as external LOC, an unsurprising result given they are both externally based loci of control.
The moderation is consistent with the perfectionism (Hamachek, 1978) and LOC (Rotter, 1966) theorems and supports the claim that perfectionism at high levels is maladaptive (Hamachek, 1978), as shown by the positive association between self-oriented and social-prescribed perfectionism and PPD. It appears this relationship only manifests when external LOC is high or when internal LOC is low. This outcome reinforces Rotter’s (1966) argument that internals are more emotionally adjusted than externals. It is possible that self-oriented perfectionists align their self-worth with their performance; therefore, when little control is perceived, they are more likely to have PPD (Hewitt & Flett, 1991a). Socially prescribed perfectionists may fear societal failure and experience cognitive dissonance, which in turn makes them more vulnerable to depressive episodes when minimal control is perceived (Hewitt & Flett, 1991a). Thus, it is possible that perfectionists may be protected by their internal LOC and that they are, consequently, less likely to have PPD.
Socially prescribed and self-oriented perfectionism had similar relationships with LOC but this goes against expectations. The association between self-oriented perfectionism and LOC provides support for the literature (Hewitt & Flett, 1991a). However, the socially oriented perfection and LOC relationship outcome contradicts previous research (Periasamy & Ashby, 2002; Stewart & De George-Walker, 2013), where socially prescribed perfectionism was positively associated with internal LOC and negatively associated with external LOC. It is possible that socially prescribed perfectionists experience cognitive dissonance and attempt to reduce the discrepancy between their “ideal” and “actual selves” by perceiving an internal LOC (Festinger, 1957). While this explanation is plausible, it is more likely that these similarities are due to the perfectionism dimensions being similar constructs resulting in a high correlation (r = .90). Previous studies have found mixed results with some finding overlapping between self-oriented and socially prescribed perfectionism (Hewitt & Flett, 1991b), while others finding them differentiated (Shafran & Mansell, 2001). These variations in outcome highlight the limitations of the perfectionism literature failing to delineate clear dimensions of perfectionism.
Limitations
The results of the present study are bound by the limitations typical of cross-sectional self-report study designs. Some women may have underestimated their symptoms due to a social desirability bias (Boyce, 2003), while others may have overestimated their symptoms due to a demand characteristics bias (Gelabert et al., 2012). Information about previous history of diagnosed depression (“Do you have a history of diagnosed depression?”) was sought in the survey. However, analyses controlling for previous history of depression were not conducted as such analyses would be underpowered as the sample size would effectively be halved. The participants’ mental health literacy levels may also have affected the outcome (Thorsteinsson, Loi, & Moulynox, 2014) as well as their beliefs and attitudes toward mental illness (Gibbons, Thorsteinsson, & Loi, 2015). However, the efficient nature of the self-report questionnaires contributed to a large sample being recruited. Furthermore, the questionnaires used were reliable and valid suggesting that the data collected are indicative of the concepts being investigated.
Future Research
Future research investigating the triad relationship between perfectionism, LOC, and PPD should include a longitudinal design that recruits pregnant women to determine if the relationship changes during pregnancy and through the postpartum period. There is a need to increase our understanding in the clinical realm of how perfectionism and LOC interact to potentially contribute to PPD, which may lead to women being screened for perfectionism during pregnancy. Future studies might also measure time since delivery to examine if this interval has any impact on PPD relationships.
Conclusion
The results indicate that a complex yet intuitive relationship between LOC, perfectionism, and PPD exists. LOC exacerbates the perfectionism and PPD relationship indicating women at risk of PPD are those who have self-oriented and socially prescribed perfectionism with high external LOC or low internal LOC. These results may be attributed to the self-directed nature of self-oriented perfectionists. Powerful others had a similar moderating relationship to external LOC on socially prescribed perfectionism and PPD. This may be due to these two loci of control being externally based. The association that LOC strengthens the relationship between perfectionism and PPD may be an important factor in the likelihood of PPD occurring, and is a relationship that merits further investigation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.