
Abstract
Most validation studies of the Freiburg Mindfulness Inventory (FMI) involved healthy subjects. Validation in patients who suffer from a life-threatening medical illness is needed, to investigate the FMI’s validity in medical psychology research and practice. Psychometric properties of the Dutch FMI were examined in two patient groups of two different studies: (Sample 1) cardiac patients (n = 114, M age = 56 ± 7 years, 18% women) and (Sample 2) severely fatigued cancer survivors (n = 158, M age = 50 ± 10 years, 77% women). Confirmatory factor analysis (studied only in Sample 2) provided good fit for the two-factor solution (Acceptance and Presence), while the one-factor solution provided suboptimal fit indices. Internal consistency was good for the whole scale in both samples (Sample 1 α = .827 and Sample 2 α = .851). The two-factor model showed acceptable to good internal consistency in Sample 2 (Presence: α = .823; Acceptance α = .744), but poor to acceptable in Sample 1 (Presence subscale: α = .577, Acceptance subscale: α = .791). Clinical sensitivity was supported in both samples, and construct validity (studied only in Sample 1) was acceptable. The Dutch FMI is an acceptable instrument to measure mindfulness in patients who experienced a life-threatening illness in a Dutch-speaking population.
Introduction
Mindfulness-based interventions (MBIs) have shown to effectively reduce psychological symptoms in patients who suffer from life-threatening medical illnesses, such as coronary heart disease (Nyklíček, Dijksman, Lenders, Fonteijn, & Koolen, 2014; Tacón, McComb, Caldera, & Randolph, 2003) and cancer (Carlson & Garland, 2005; Chambers, Foley, Galt, Ferguson, & Clutton, 2012; Foley, Baillie, Huxter, Price, & Sinclair, 2010; Hofmann, Sawyer, Witt, & Oh, 2010; Ledesma & Kumano, 2009; Ott, Norris, & Bauer-Wu, 2006; Sharplin et al., 2010; Shennan, Payne, & Fenlon, 2010; van der Lee & Garssen, 2012). In these interventions, patients learn to focus their attention to the present moment experience, in an accepting, nonjudgmental way (Bishop et al., 2004; Kabat-Zinn, 1990; Segal, Williams, & Teasdale, 2002). It is proposed that this attention regulation may lead to symptom reduction through exposure, a change in attitude toward one’s thoughts, self-management, relaxation, and acceptance (Baer, 2003). Mindfulness is defined by “a mental state achieved by focusing one’s awareness on the present moment, while calmly acknowledging and accepting one’s feelings, thoughts, and bodily sensations, used as a therapeutic technique” (Oxford Dictionaries, 2016).
To investigate whether, or to what extent, mindfulness skills are a working mechanism in MBIs in these patients, there is a need for reliable and valid tools to measure mindfulness (Baer, 2007). With a valid tool, researchers can investigate whether mindfulness changes during the intervention, whether this is related to treatment outcome (mediator, or working mechanism), and if the level of mindfulness can predict treatment outcome (moderator, or effect predictor). This knowledge can be applied in health care to better inform patients about how the intervention may work and to improve allocation of patients to suitable interventions.
A group of Dutch experts in the field of mindfulness research and medical psychology (the second [M.L.V.L.] and fouth author [I.N.], Dr. M. Schroevers of Leiden University, the Netherlands, Dr. B. Garssen and Dr. C. Völker of the Helen Dowling Institute, the Netherlands), came together in 2007 to discuss all available mindfulness questionnaires, and to select or create one Dutch questionnaire suitable for measuring mindfulness as a working mechanism in MBIs in patients who experienced a life-threatening medical illness. They chose the Freiburg Mindfulness Inventory (FMI; Buchheld, Grossman, & Walach, 2001; Walach, Buchheld, Buttenmüller, Kleinknecht, & Schmidt, 2006) as it includes two fundamental facets that these experts considered most crucial in medical psychology: (a) focus on the present moment including bodily awareness and (b) nonreactivity to the inner experience, thus an accepting attitude (Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006; Bishop et al., 2004). For patients who experienced a life-threatening illness, bodily sensations can often be stress evoking as it may remind them of trauma. Therefore, some patients tend to either avoid sensing bodily symptoms (Hayes, Wilson, Gifford, Follette, & Strosahl, 1996) or are preoccupied with them (Hayes & Feldman, 2004). When practicing mindfulness, patients are invited to investigate present bodily experiences, in an accepting, nonjudgmental way (Bishop et al., 2004; Kabat-Zinn, 1990; Segal, Teasdale, Williams, & Gemar, 2002), thereby exposing themselves to their fears and bodily symptoms which leads to reduced stress (Baer, 2003). Furthermore, the FMI is a short questionnaire which makes it feasible to assess mindfulness several times during an intervention which is needed if we want to study mindfulness as a working mechanism.
The German FMI has been demonstrated to possess good psychometric qualities (Heidenreich, Ströhle, & Michalak, 2006; Kohls, Sauer, & Walach, 2009; Ströhle, 2006; Walach et al., 2006). French, Finnish, English, and Chinese translations of the FMI have been validated in middle-aged nonclinical samples (Chen & Zhou, 2013; Lehto, Uusitalo-Malmivaara, & Repo, 2015; Leigh, Bowen, & Marlatt, 2005; Trousselard et al., 2010). Only Sauer, Walach, Offenbächer, Lynch, and Kohls (2011) investigated the psychometric properties of the FMI in a clinical sample, namely patients with psychosomatic conditions. They found good properties for the two-factor solution (Acceptance and Presence) and showed the scale to correlate positively with health indicators.
Most validation studies of the FMI involved healthy subjects (Chen & Zhou, 2013; Kohls et al., 2009; Lehto et al., 2015; Sauer et al., 2011; Sauer, Ziegler, Danay, Ives, & Kohls, 2013; Trousselard et al., 2010; Walach et al., 2006), but validation in specifically patients who suffer from a life-threatening medical illness is needed (Ziegler, 2014b), to investigate the FMI’s validity in medical psychology research and practice. To our knowledge, there are no previous validation studies of the FMI involving patients who experienced a life-threatening illness.
Aim of This Study
The aim of the present study was to investigate the psychometric properties of the Dutch translation of the FMI in patients who experienced a life-threatening illness. Following the recommendations of Ziegler (2014b), the validity will be investigated in the following ways:
To investigate the structural component, we studied the factorial validity of the Dutch FMI.
To investigate the internal structure of the item pool, we studied the internal consistency of the (sub)scales.
To investigate the construct of mindfulness measured with the FMI, its relation with other constructs was investigated, to study the convergence and divergence regarding other constructs (construct validity).
To investigate whether the Dutch FMI translation had sufficient sensitivity to measure change in mindfulness, we studied the clinical sensitivity—also called responsiveness—before, during, and after a MBI.
Materials and Method
Selection and Development of Dutch FMI
The following mindfulness questionnaires were available in 2007 and were taken into account by the expert panel to select or create one Dutch questionnaire suitable for measuring mindfulness as a working mechanism in MBIs in patients who experienced a life-threatening medical illness: Mindfulness Attention Awareness Scale (MAAS; Brown & Ryan, 2003), Southampton Mindfulness Questionnaire (SMQ; Chadwick et al., 2008), Kentucky Inventory of Mindfulness Scale (KIMS; Baer, Smith, & Allen, 2004), Cognitive and Affective Mindfulness Scale–Revised (CAMS-R; Feldman, Hayes, Kumar, Greeson, & Laurenceau, 2007; Hayes & Feldman, 2004), Toronto Mindfulness Scale (TMS; Lau et al., 2006), Five Facet Mindfulness Questionnaire (FFMQ; Baer et al., 2006), and FMI (Buchheld et al., 2001; Walach et al., 2006). The SMQ was developed and cited as an unpublished manuscript in 2005 (Baer et al., 2006; Lau et al., 2006), but published in 2008 (Chadwick et al., 2008), and therefore the SMQ was not included in the expert panel’s decision-making process.
The expert panel started by selecting which of the five facets of mindfulness presented by Baer et al. (2006)—(a) nonreactivity to inner experience; (b) observing sensations, perceptions, thoughts, and feelings; (c) acting with awareness; (d) describing/labeling with words; (e) nonjudging of experience—they considered specifically important in medical psychology. They agreed that nonreactivity to inner experience (acceptance) and observing sensations, perceptions, thoughts, and feelings (presence or awareness) were the most important aspects of mindfulness in medical psychology.
The panel agreed on choosing the FMI based on several reasons. First, the FMI involves the most important facets of mindfulness for evaluating MBIs in medical psychology. Second, it holds only 14 items, so it is short and feasible to assess multiple times during an intervention. And third, the items are both negatively and positively framed. Concerning the other questionnaires, the TMS was judged to be more suitable to study specific elements of mindfulness, rather than the overall change in mindfulness in MBIs. CAMS-R was judged to focus more on concentration, rather than acceptance and presence. The SMQ was judged to mostly measure negative thoughts and not emotions, though MBIs are experiential interventions so emotions need to be addressed in evaluation of these interventions. As FFMQ and KIMS hold 39 items, these were not preferred, though FFMQ also measures acceptance and presence. KIMS does not involve presence (Baer et al., 2004).
The German FMI as well as the English FMI were translated into Dutch, by respectively a German native speaker and an English native speaker who both spoke Dutch fluently. Both translations were then critically examined by the expert panel mentioned in the introduction, until consensus about the Dutch translation of the items had been reached. In Supplementary material 1, the Dutch translation of the FMI is presented).
Procedure
Data from the Dutch version of FMI were collected in two different samples. The first sample (Sample 1 of the MindfulHeart study) involved cardiac patients who recently had a percutaneous coronary intervention (PCI) and who followed a brief Mindfulness-Based Stress Reduction (MBSR) group intervention. For a detailed description about the MindfulHeart study, see Nyklíček et al. (2014). In the current article, we used data from 107 participants who filled in the FMI (M age = 56 ± 7 years; 18% women) who were randomly assigned to either a four-session MBSR group intervention (n = 55) or a minimal MBSR self-help control group (n = 52). All participants filled in several questionnaires (see Nyklíček et al., 2014, and “Measurements”), including the FMI, before and after the intervention.
The second sample (Sample 2 of the eMBCT study) involved severely fatigued cancer survivors who followed a therapist guided, web-based, individual 9-week Mindfulness-Based Cognitive Therapy (eMBCT) aimed at reducing cancer-related fatigue (mixed cancer types). The FMI was filled in by 158 patients (M age = 50 ± 10; 77% women). They were asked to fill in the FMI through a link on their personal webpage at the beginning of Weeks 1, 3, 6, and 9 of the intervention. For a detailed description about the eMBCT study, see Bruggeman-Everts, van der Lee, and de Jager Meezenbroek (2015).
Measurements
The FMI claims to measure Mindfulness with its subfacets Acceptance and Presence. The internal consistency, measured with Cronbach’s α in the German FMI was good (α = .86; Walach et al., 2006). Support was found for sensitivity to change and suitability for the use of FMI in subjects without previous meditation experience (Walach et al., 2006). The current Dutch translation of the FMI was used in one other study, and internal consistency was acceptable (α = .79; Klaassen, Nyklíček, Traa, & De Nijs, 2012). The following questionnaires were assessed to measure construct validity (see Table 3).
The CAMS-R (Feldman et al., 2007) is proposed to measure the willingness and ability to be mindful, rather than how mindful a person is during the day. It demonstrated acceptable internal consistency (two samples of university students: α = .74 and α = .77) and evidence for convergent and discriminant validity (Feldman et al., 2007). A strong correlation between the CAMS-R and FMI-30 (r = .60, Baer et al., 2006; r = .66, Feldman et al., 2007), and CAMS-R and MAAS (r = .51, Feldman et al., 2007) have been found, which indicates good convergent validity.
The Balanced Index of Psychological Mindedness (BIPM; Nyklíček & Denollet, 2009) is assumed to measure psychological mindedness, which refers to a person’s interest and ability to be in touch with and reflect on one’s psychological states and processes. The BIPM showed moderate construct validity (r > .40 with related constructs), acceptable to good internal consistency (Interest: α = .85; Insight: α = .76), and strong test–retest reliability (Interest: r = .63; Insight: r = .71) (Nyklíček & Denollet, 2009).
The Perceived Stress Scale (PSS; Cohen, Kamarck, & Mermelstein, 1983) is a measure for how often a person has perceived stress in the last month. It showed to have acceptable to good internal consistency (α = .75-.86) and showed sufficient test–retest reliability and construct validity (Cohen et al., 1983; Cohen, Tyrrell, & Smith, 1993). A Dutch translation has been used before (Nyklíček & Kuijpers, 2008).
The Symptoms of Anxiety-Depression index (SAD-4; Denollet, Strik, Lousberg, & Honig, 2006) was developed as a Dutch screening method for mixed and interrelated symptoms of depression and anxiety in post-myocardial infarction patients. Criterion validity has been supported and internal consistency was good (α = .86) (Denollet et al., 2006).
The Dutch Global Mood Scale (GMS; Denollet, 1993) measures Positive and Negative Affect, and it showed to have excellent internal consistency (α = .91 and α = .94, respectively). Test–retest reliability (r = .55) and convergent and discriminant validity have been demonstrated (Denollet, 1993).
The World Health Organization Quality of Life–Bref questionnaire (WHOQOL-Bref; WHOQOL Group, 1998) is used to measure generic quality of life in four domains: physical health, psychological health, social relationships, and environment. The internal consistency of the four domains was moderate to good (α = .66 for social relationships to α = .82 for physical health). Sufficient test–retest reliability (r = .66-.87) and adequate discriminant validity was found (WHOQOL Group, 1998).
The Seattle Angina Questionnaire (SAQ; Spertus et al., 1995) is used to measure physical health in cardiac patients, in five domains: physical limitation, angina stability, angina frequency, treatment satisfaction, and disease perception. All domains showed moderate to good internal consistency (α = .66-.89) (Dougherty, Dewhurst, Nichol, & Spertus, 1998). Its content, construct, and criterion validity have been demonstrated and it showed to be a reliable and valid instrument for patients who had previously undergone PCI (Spertus et al., 1995).
Statistical Analyses
Demographics were calculated for both Samples 1 and 2 separately, and differences between groups were tested using independent samples t tests and χ2 tests. Significance level was set at p ≤ .05. We used multiple imputation (Rubin, 1996) to impute missing items. To study the factor structure, we used Mplus version 7.31 (Muthén & Muthén, 2012). All other analyses were performed using SPSS Version 19 for Windows package (SPSS Inc., Chicago, IL).
Factor structure
Confirmatory factor analysis (CFA) using maximum likelihood and oblique rotation (Promax) was performed. Model fit was considered adequate if chi-square/degree of freedom ratio (CMIN/df) < 2; comparative fit index (CFI) > .90; Tucker–Lewis index (TLI) > .90; normed fit index (NFI) > .90; root mean square error of approximation (RMSEA) < .08, and χ2 test of p > .05 (Kline, 2011; van de Schoot, Lugtig, & Hox, 2012). We tested for measurement invariance to see if data of Sample 1 and 2 could be combined for the factor analysis (see Supplementary material 2 for results), but this showed that the FMI lacked configural, metric, and scalar invariance across our two study samples. This indicated that the FMI was not stable between these two patient groups and combining the datasets would lead to uninterpretable results. We decided to study the factor structure of Sample 2 (n = 158) only, as Sample 1 had too small sample size (n = 102) that is likely to lead to statistical artifacts (Ziegler, 2014a). We expected a two-factor structure, as was found in the German (Kohls et al., 2009; Ströhle, 2006), Chinese (Chen & Zhou, 2013), and Finnish version (Lehto et al., 2015). To test whether two competing models were significantly different, χ2 difference testing was performed.
Internal consistency
Based on previous research (Chen & Zhou, 2013; Klaassen et al., 2012; Trousselard et al., 2010; Walach et al., 2006), we expected the internal consistency of the Dutch FMI to be at least Cronbach’s α > .70 (“acceptable”).
Construct validity
Using Pearson’s correlations, we investigated whether the FMI (factor) scores correlated with (subscales of) questionnaires assessed in Sample 1. We considered correlations r < .3 as weak, .3 ≤ r < .5 as moderate, and r ≥ .5 as strong (Cohen, 1988). We expected that FMI scores correlated strongly with another mindfulness questionnaire (positive: CAMS-R), and moderately with constructs related to psychological well-being (positive: BIPM, GMS positive affect, WHOQOL-Bref; negative: PSS, SAD-4, GMS negative affect) (convergent validity). We expected the FMI scores to correlate weakly with a questionnaire assessing physical health (SAQ; divergent validity).
Clinical sensitivity
To record the FMI’s ability to capture and record a patient’s change over time (also called responsiveness), we calculated the standardized response mean (SRM; change divided by standard deviation of change; Anderson & Chernoff, 1993). In Sample 1 (n = 51), the SRM of FMI scores was calculated between pre- and postintervention. In Sample 2, the SRM was calculated at Weeks 3, 6, and 9, compared with Week 1, using all available data (n = 95). Based on previous studies in which it was found that an increase in mindfulness is associated with improvement of clinical outcome (Branstrom, Kvillemo, Brandberg, & Moskowitz, 2010; Gu, Strauss, Bond, & Cavanagh, 2015; Kabat-Zinn, 1982), and that the FMI is able to distinguish between meditators and nonmeditators (Walach et al., 2006), we hypothesized that after MBSR in Sample 1 and during MBCT in Sample 2, mindfulness increased and that this would be measured with FMI.
Results
The group of Sample 1 involved more men, more comorbidities, lower education, and older patients than the group in Sample 2 (see Table 1).
Demographics of Participants in the MindfulHeart (Sample 1) and eMBCT Study (Sample 2) and Results of Independent Samples t Tests and Chi-Square Tests to Study Differences Between Groups.

Note. ns = nonsignificant.
Lower vocational education.
Secondary education, community college.
High professional education or college/university.
Factor Structure
In Table 2, the model fit indices for the one-factor and two-factor model for Sample 2 are shown. The two-factor structure provided good fit indices, while the one-factor model provided suboptimal fit indices.
Fit Indices for the One- and Two-Factor Models of the FMI of Sample 2.

Note. Adequate fit: CMIN/df < 2; CFI > .90; TLI > .90; RMSEA < .08; and chi-square statistic (χ2) of p < .05. The model with the lowest BIC and AIC best fits the data. CMIN/df = chi-square/degree of freedom ratio; CFI = comparative fit index; TLI = Tucker–Lewis index; NFI= normed fit index; RMSEA = root mean square error of approximation; AIC = Akaike information criterion; BIC = Bayesian information criterion.
The factor loadings of each model are shown in Table 3 and the Supplementary material 3. Item 14 (I am able to smile when I notice how I sometimes make life difficult) was below 0.5 in the one-factor solution.
Factor Structure of One- and Two-Factor Models of Sample 2.
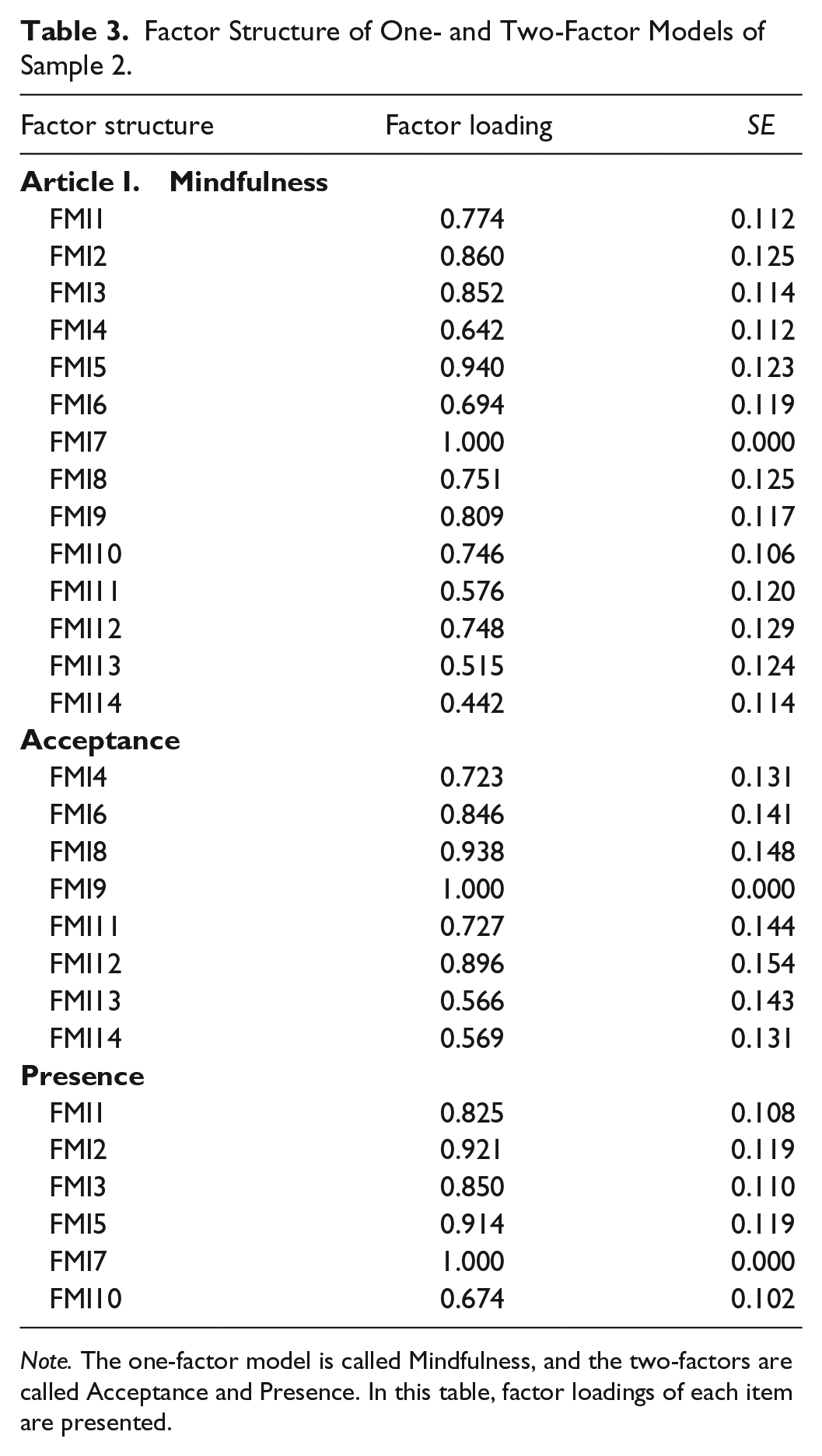
Note. The one-factor model is called Mindfulness, and the two-factors are called Acceptance and Presence. In this table, factor loadings of each item are presented.
Internal Consistency
Good internal consistency was found for the one-factor FMI scale in both Sample 1 (α = .827) and Sample 2 (α = .851). The internal consistency of the two-factor solution in Sample 1 was poor for the Presence subscale (α = .577) and acceptable for the Acceptance subscale (α = .791). In Sample 2, the internal consistency was good for the Presence subscale (α = .823), and acceptable for Acceptance subscale (α = .744).
Construct Validity
In Sample 1, we found moderate to strong correlations between the FMI factors and other psychological constructs, and weak to no correlations with questionnaires assessing unrelated constructs (physical health). We found higher correlations with perceived stress (PSS; negative) and psychological health (WHOQOL-Bref-Psychological health; positive), than with a mindfulness questionnaire (CAMS-R; positive; see Table 4).
Pearson’s Correlations of One- and Two-Factor FMI Solution With Questionnaires Assessed in Sample 1 (n = 107).

Note. A measure for internal consistency of the SAQ–Angina Stability subscale was not applicable, as it holds one item. α = internal consistency measured with Cronbach’s alpha; CAMS-R = Cognitive and Affective Mindfulness Scale–Revised (Feldman et al., 2007); r = Pearson’s correlation; BIPM = Balanced Index of Psychological Mindedness (Nyklíček & Denollet, 2009); SAD-4 = Symptoms of Anxiety-Depression index (Denollet et al., 2006); GMS = Dutch Global Mood Scale (Denollet, 1993); PSS = Perceived Stress Scale (Cohen et al., 1983); WHOQOL-Bref = World Health Organization Quality of Life–Bref questionnaire (WHOQOL Group, 1998); SAQ = Seattle Angina Questionnaire (Spertus et al., 1995).
p < .05 (two-tailed). **p < .001 (two-tailed).
Clinical Sensitivity
In Sample 1, an SRM of .598 was measured at postassessment, meaning there was a moderate responsiveness of mindfulness measured with FMI. In Sample 2, SRM changed from 0.4894 in Week 3, to 0.9479 at Week 6, and to 1.3136 at Week 9, meaning the responsiveness of FMI increased from low to high during the intervention.
Discussion
This is the first study that investigated the psychometric properties of the Dutch translation of the FMI in patients who experienced a life-threatening illness. Two different samples were used in this study, namely Sample 1 that consisted of cardiac patients from the MindfulHeart study, and Sample 2 that consisted of severely fatigued cancer survivors from the eMBCT study. Factor analyses in Sample 2 provided more support for the two-factor solution. than the one-factor solution. The internal consistency was good for the one-factor model in both samples. The two-factor model showed acceptable to good internal consistency in Sample 2, but poor to acceptable internal consistency in Sample 1. We found that FMI was clinically sensitive in both samples, and that construct validity (studied only in Sample 1) was acceptable. We conclude that the Dutch translation of the FMI is an acceptable instrument to assess mindfulness in patients who experienced a life-threatening illness.
In line with the findings of the Finnish validation study (Lehto et al., 2015), we found a high correlation between the FMI, and perceived stress (PSS) and psychological health (WHOQOL-Bref). This suggests that mindfulness measured with the FMI, is related to these constructs, which are important outcomes in medical psychology. This high correlation may suggest the usefulness of introducing mindfulness to alleviate stress, although it does not teach us anything about causality. Therefore, it is important to study working mechanisms, not only with mediation analyses but also assessing if a rise in mindfulness precedes drops in perceived stress in prospective investigations.
This study is subject to some limitations. First, the Mindfulheart study and the eMBCT study were not originally designed to investigate the psychometric properties of the FMI, which resulted in a too small sample size to perform factor analysis in Sample 1, and item deletion to improve, as this may lead to statistical artifacts (Ziegler, 2014a). Also construct validity could only be investigated in Sample 1. Second, to investigate if the FMI is indeed measuring the concept of mindfulness, one needs a “gold standard” to compare it with (criterion validity). However, despite that mindfulness research has grown in the last decade (Grossman, 2011), there is still no consensus about a gold standard. Third, this study lacked a control group, and therefore we could not investigate test–retest validity to control for response shift bias (Grossman, 2008; Howard, 1980). The results of clinical sensitivity were dependent on whether mindfulness indeed increased during MBSR in Sample 1 and MBCT in Sample 2, and thus, one could not test whether poor responsiveness of the measurement would be due to a lack of treatment effect, or a lack of clinical sensitivity. And fourth, though self-assessed questionnaires have the advantage that it is quick and convenient, they are subject to systematic bias such as the Hawthorne effect, the overconfidence effect, social desirability, and cognitive dissonance (Grossman, 2008).
As mindfulness is a complex construct, we prefer to focus on certain aspects of mindfulness that are not only key facets of mindfulness definitions but also are thought to be the key working mechanisms of MBI in patients who have experienced a life-threatening illness: focus on the present moment including bodily awareness, with an accepting attitude. This study showed acceptable psychometric properties of the FMI in these patients, and therefore we conclude that the Dutch FMI is an acceptable instrument to measure mindfulness as a working mechanism in MBIs for patients who experienced a life-threatening illness.
Footnotes
Acknowledgements
We thank the Alpe ‘d HuZes/Koningin Wilhelmina foundation for supporting F.Z.B.E. (Project 2011-5264). We thank Math Leistra and Matthew Young for translating the German and English version of the FMI, and Suzanne Dijksman, Pim Lenders, and Willem Fonteijn for preparing the data of the Mindfulheart study. We thank Arnold van Emmerik for his critical feedback on the design of the study.
Ethical Approval
All persons gave their informed consent prior to their inclusion in the study. The MindfulHeart study was approved by the Medical Ethics Committee of the Catharina Hospital at Eindhoven, The Netherlands, and registered in the Dutch Trial Registry (Trial NTR 3397: ![]() ). The eMBCT study was approved by the ethical board of the Helen Dowling Institute. In the general usage conditions, patients actively agreed on their answers to the questionnaires being used for research purposes.
). The eMBCT study was approved by the ethical board of the Helen Dowling Institute. In the general usage conditions, patients actively agreed on their answers to the questionnaires being used for research purposes.
Authors’ Note
F.Z.B.E. wrote the manuscript and performed the analyses. M.L.V.L. designed the outline of the manuscript and gave critical revisions on this manuscript. E.F.M.vt.H. prepared the data, and E.F.M.vt.H. and F.Z.B.E. performed the analyses. I.N. gave critical revisions on this manuscript. The raw data may be sent upon request after agreement of all authors. Please contact the first author for more details.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.