
Abstract
The well-being of the elderly population in India is of prime importance in the context of a weak social security system, breakdown of family structure, and increasing noncommunicable diseases. In this context, this study aims to understand the linkages of the living arrangements of the elderly with their work status, morbidity, and treatment-seeking behavior in four states in South India. This study was based on cross-sectional secondary data from the 60th round of National Sample Survey (NSS) on “Morbidity, Health Care and the Condition of the Aged” conducted in India in 2004. A subsample of 7,853 elderly from four demographically advanced states in South India formed the study population. Results showed that most of the elderly were working as unpaid workers in their later ages. A significant number of the elderly with primary or more education and living with their children without spouse or with other relatives worked as unpaid workers. Multivariate analyses suggest that those elderly living with their children were less likely to suffer from any morbidity and more likely to seek treatment. Economic well-being and usual activity status are significant predictors of morbidity and treatment-seeking behavior. Those elderly who lived alone were more vulnerable to poor health and more likely to work for their livelihood. Irrespective of the living arrangement, treatment seeking among the elderly was relatively higher in Kerala compared with the rest of the states. Thus, the family plays a significant role in elderly care, and living arrangement affects the work status and morbidity condition of the elderly population in the states of South India.
Keywords
Introduction
A study of the determinants of aging reflects the psychosocial, emotional, economic, and health status of the elderly. Aging is a comparatively new phenomenon in developing countries where fertility has declined significantly over the last few decades. Following rapid fertility decline, the pace of aging in developing countries is much faster than that in developed countries (Bloom, 2011). The challenges related to aging are more prevalent in developing countries, especially in India, when compared with developed countries. The well-known phrase “getting old before getting rich” is the most prominent feature of the population in most developing countries (Goli & Pandey, 2010). Most of the developing countries do not have the capacity to provide proper health and social security to their graying population. Issues related to population aging, such as social security and health care financing in developing countries, have not been major public policy concerns despite the fact that the older population is growing rapidly (Shrestha, 2000). According to the Census of 2011, India accounts for over 8% of the population aged 60 years and above, which is projected to rise to 20.2% by 2050. In terms of size of the population, India ranks second globally, but the number is doubling once in 23 years (Bhat, 1992; United Nations, 2013).
Among the elderly population, the oldest old are the most vulnerable due to their health status, cognitive ability, insufficient social support, and lack of knowledge (Kim & Geistfeld, 2008). Loneliness increases their vulnerability as their need for social interaction increases, which makes them more susceptible to fraud and cheating (S. Agrawal, 2012; Lee & Geistfeld, 1999). Poverty, lack of social support, personal limitations, and physical locations are some of the important dimensions that increase the elderly population’s vulnerability (Mechanic & Tanner, 2007). A reduced capacity for income generation and a growing risk of severe illness are likely to increase the vulnerability of the elderly regardless of their original economic status (Lloyd-Sherlock, 2000). The elderly population is vulnerable to multiple chronic diseases, and the prevailing low socioeconomic status (SES) worsens the situation. Noncommunicable diseases (NCDs) are the leading cause of disease burden among the elderly. It has been estimated that nearly half the disease burden in low- and middle-income countries is from NCDs (Quigley, 2006). Studies show that the socioeconomic condition of older women makes them more vulnerable in the context of the demographic and sociocultural changes (Tout, 1989). Owing to the low mortality rate, women outnumber men in the older age bracket, which results in an increased number of widows in the 60+ population. Elderly women thus live without spousal support in their old age, which leads to the feminization of aging (United Nations, 2005). In developing countries, the elderly who live alone or with only the spouse, without financial support, have to work in the latter part of their lives, and very often, they live in poor conditions. The scenario is different in developed countries, where the government provides social and economic security to support the vulnerable sections of society.
Financial Security for the Elderly Population
Providing financial security to the elderly population is a significant challenge to the nations with a growing aging population and the situation worsens in countries with a transition economy. The institutional setting related to pension provision differs remarkably within demographically advanced Western nations. In some countries, intrafamilial income transfers are an important source of old age security, while many countries rely on large financial conglomerates.
Social security provided by the Indian government is mainly of three forms—subsidized food through the Public Distribution System (PDS), public works through the Mahatma Gandhi National Rural Employment Guarantee Act (MGNREGA), and unconditional cash transfer like the Indira Gandhi National Old Age Pension Scheme (IGNOAPS). The amount of money transferred through social pension is very low. Although, the assistance paid through the social support program does play a role in reducing poverty, various studies have found that cash transfer is the better way to reach the poor (Subramanian, Kapur, & Mukhopadhyay, 2008). India’s safety net costs around 2% of the gross domestic product (GDP), which is relatively high for a country of India’s income per capita (Weigand & Grosh, 2008). Dutta (2008) showed that though pension, however small it may be, is an important source of income for the elderly in their later stages of life, the coverage rate relative to the number of elderly is of about 7% for old age pension. The elderly in India are either economically dependent on a traditional support system or work for their survival or to support the family.
Living Arrangement and Familial Support
In the Western countries, more than 60% of the elderly aged 65 years and above live either alone or only with the spouse (Palloni, 2001). In India, the familial bond is stronger, and the culture of living with children in old age is preferred and socially recognized. This is a two-way arrangement—On one hand, the elderly get financial and emotional support, and on the other, the grandchildren are looked after by the grandparents, who also help with the household chores. Most of the elderly women prefer to live with their adult children and preferably with the married son (Mehio-Sibai, Beydoun, & Tohme, 2009). Many studies reveal that the elderly living with their children enjoy more economic well-being than those who prefer to live independently. However, researchers have found that there is an increasing trend toward the elderly living alone or with only the spouse. Even in India, around 16% of the elderly either live alone or with only the spouse (National Sample Survey [NSS], 2006).
Different factors determine the living arrangement of the elderly. Studies have identified a number of background factors such as age, sex, occupation, education, place of residence, number of children, and so on, as the relevant variables that shape the living arrangement (United Nations, 2005; Yadava, Yadava, & Sharma, 1996). Velkoff (2001) found that living arrangements are influenced mainly by financial well-being, marital status, family size and structure, as well as cultural traditions. However, the relative importance of these factors has not been examined carefully. Studies have tried to determine the critical factors that affect the living arrangement of the elderly. Increasing urbanization and the growth of individualism and desire for independence and autonomy on the part of the young generation affect the status of the elderly (Serow, 2001).
This study focuses on the demographically advanced states of South India, that is, erstwhile Andhra Pradesh, Kerala, Tamil Nadu, and Karnataka, which consist of a relatively high proportion of the elderly population. According to the Census of India 2011, the proportion of elderly was above the national average (7.4%) in all the four southern states with Kerala at the top with 12.7% (out of Kerala’s total population), followed by Tamil Nadu (10.6%), Karnataka (9.6%), and erstwhile Andhra Pradesh (9.8%). The age disaggregated morbidity prevalence in India showed a “J” shaped relationship between age and morbidity, indicating that children and the elderly are more susceptible to a higher incidence of disease (Gumber & Berman, 1997; NSS, 1998). Chronic ailments have led to morbidity prevalence among the elderly, which is rising where the share of NCD is increasing (G. Agrawal & Arokiasamy, 2010).
Old age poses many challenges in India in the absence of adequate economic and social security programs for the elderly by the government, and the problem has been aggravated because of lack of personal savings. In India, about 85% of the total workforce is engaged in the unorganized sector with little or no old age income security. According to the Census of India 2001, the work participation rates among the elderly in erstwhile Andhra Pradesh, Tamil Nadu, Kerala, and Karnataka are 41%, 43%, 23%, and 39%, respectively.
There is a paucity of literature that examines the impact of different living arrangements on health outcomes, and the social and economic security of the elderly. The main purpose of this study is to explore the living arrangement, work status, and morbidity conditions of the elderly in the states of South India and associated determinants in different settings of living arrangements.
Data and Method
Data Source
This study is based on the data from the 60th round (Schedule 25.0) of the NSS on “Morbidity, Health Care and the Condition of the Aged” conducted in India during 2004. In this round, a sample of 34,831persons (aged 60+) was surveyed at the national level out of which 7,853 individuals were sampled from erstwhile Andhra Pradesh, Karnataka, Kerala, and Tamil Nadu. Direct questions were posed, and information on their living arrangements, whether they had any ailment, whether treatment was being taken for the same, and what was their usual activity status was collected.
Main Variables Used in the Analysis
The description of variables used in the study is given below:
Age groups: (a) Younger old (60-69 years), (b) older old (70-79 years), and (c) oldest old (80 years or above).
Usual activity status: (a) “Did not work” included did not work but was seeking and/or available for work; attended educational institution; attended domestic duties only; attended domestic duties and was also engaged in free collection of goods (vegetables, roots, firewood, cattle feed, etc.), sewing, tailoring, weaving, and so on, for household use; and not able to work due to disability, (b) “Paid workers” included worked as regular salaried/wage employee and worked as casual wage labor: in public works, in other types of work, and worked in household enterprise (self-employed)—own account worker and employer, and (c) “Unpaid workers” included worked as helper in household enterprise (unpaid family worker), beggars, prostitutes, others, rentiers, pensioners, remittance recipients, and so on.
Living arrangement: (a) Living with only spouse, (b) with spouse and children, (c) without spouse but with children, and (d) others include living alone: as an inmate of old age home, not as an inmate of old age home; other relations, and nonrelations.
Method
Morbidity prevalence rate is calculated as the number of reported ailments from a particular category per 100 population exposed to the ailment from the same category:

The binary logistic regression model is used to estimate the odds ratio of suffering from any ailment, or suffering from NCD and also their treatment-seeking behavior. The dichotomous dependent variables for the models are as follows:
First model: 1, if suffering from any ailment and 0, otherwise
Second model: 1, if suffering from NCD and 0, otherwise
Third model: 1, if treatment is taken for any ailment and 0, otherwise
Fourth model: 1, if treatment is taken for NCD and 0, otherwise.
The multinomial logistic regression model was used to study the work status of the elderly, which has multiple responses. The basic assumption of the multinomial logistic regression model is that the categories of the response variable should be mutually exclusive and exhaustive. The usual activity status of the individual has been categorized into three mutually exclusive and exhaustive categories—nonworker, paid worker, and unpaid worker, where nonworker was treated as the reference category. The effect of socioeconomic, demographic, and health determinants were examined in the light of the multiple responses of work status.
The following multinomial logistic regression model was estimated to access work status patterns by predictors of background variables:

where ai = 1, 2: constant, and bij, where i = 1, 2; j = 1, 2, . . . , n: multinomial regression coefficients.
P1: estimated probability of not working by an older adult;
P2: estimated probability of being paid worker by an older adult; and
P3: estimated probability of being unpaid worker by an older adult.
Here P1 is the reference category. For simplifying the interpretation of the result of multinomial logistic regression, coefficients were converted into adjusted percentages.
Results
Profile of the Elderly Population in Four States in South India
Table 1 shows the proportion of the elderly in different living arrangements and their distribution according to various background characteristics in four states in South India. Almost half of the elderly in Karnataka and Kerala were living with the spouse and other family members, whereas one fifth of the elderly in erstwhile Andhra Pradesh and Tamil Nadu were living only with the spouse.
Percentile Distribution of Older Population by State and Background Characteristics, 2004.

Note. MPCE = monthly per capita expenditure.
Others include living alone: as an inmate of an old age home, not as an inmate of an old age home, other relations, and nonrelations.
Others include Sikhism, Jainism, Buddhism, Zoroastrianism, and others. Weighted percent and unweighted total are shown in the table.
There is a disproportionate distribution of the elderly with the advancement of age among the states. Kerala has the highest share of population in the older old and the oldest old categories. Females outnumbered males in the later ages of life in all the three states, except Karnataka. Rural areas have a substantially larger proportion of elderly than urban areas, showing rural–urban difference at around 46%. Majority of the elderly had no education or had completed primary education. Unlike the other three states, Kerala had the highest number of older population who had completed primary-level education (44.7%); erstwhile Andhra Pradesh had the highest proportion of elderly with no education (74.7%) followed by Karnataka (68.9%) and Tamil Nadu (61.6%). Most of the older persons belonged to the lower monthly per capita expenditure (MPCE) quintiles, but in Kerala they were concentrated in the higher quintiles.
Living Arrangements of the Elderly in Four States in South India
Table 2 shows the distribution of the elderly in different living arrangements by background characteristics in each of the four states in South India. In the early phases of elderhood (60-69 years), most of the elderly live with the spouse and other family members followed by without spouse but with children. In the later phases of life, most of the elderly live with children in the absence of the spouse. Majority of the elderly males live with the spouse and other members of the family, whereas females usually live with children in the absence of the spouse. The higher life expectancy of females when compared with males accounts for this type of arrangement. The uneducated elderly usually live with their children in the absence of the spouse, followed by with spouse and other members. Most of the educated older persons live with the spouse and other family members. In all the religious communities, people usually live with members of the family in the later phases of life. A large proportion lives with only the spouse among the Christians in all the South Indian states except Kerala. A similar type of concentration in living arrangement is observed by social groups, place of residence, and MPCE quintile groups.
Percentile Distribution of Elderly With Different Living Arrangements by Background Characteristics in the States of South India, 2004.
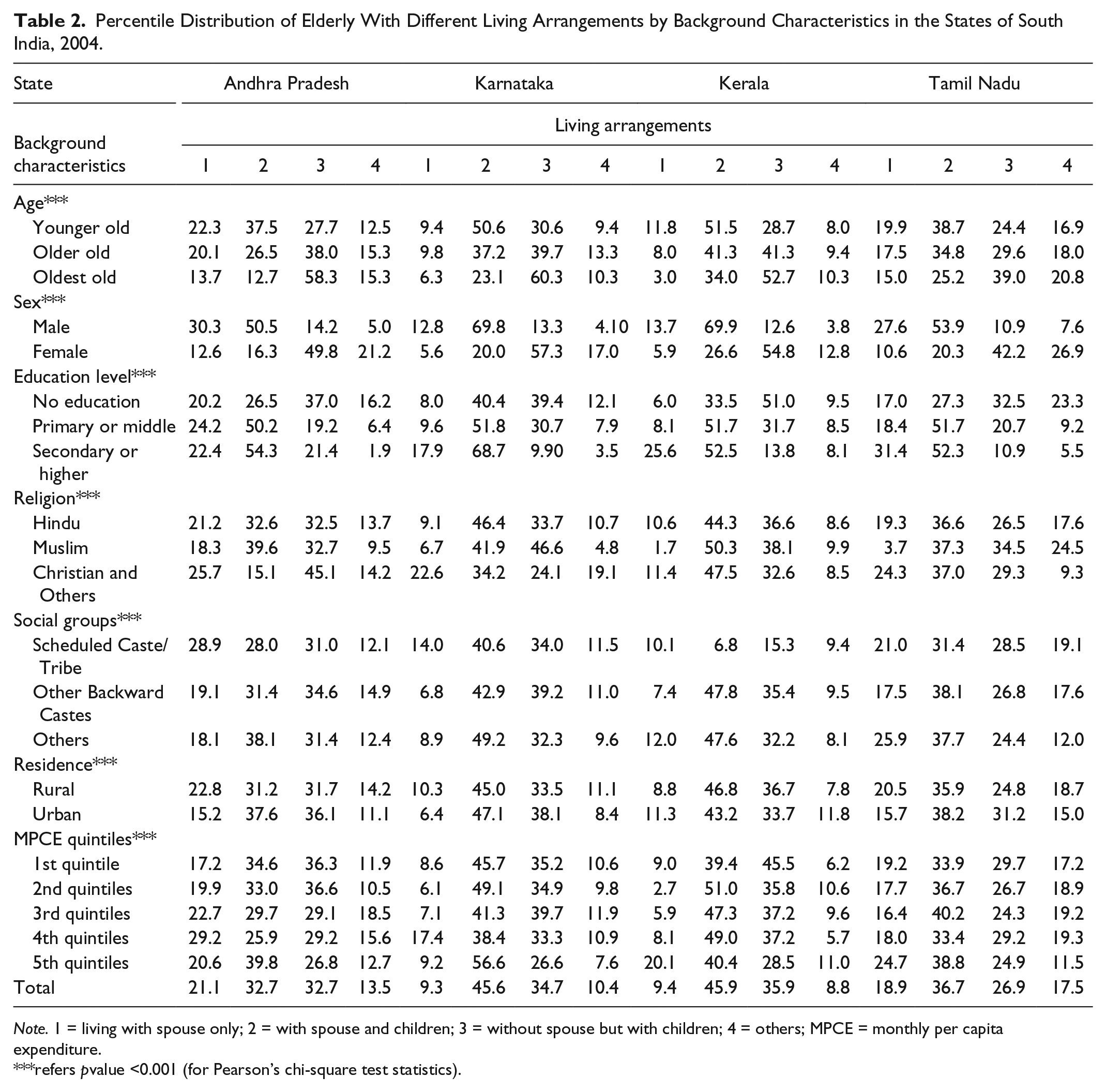
Note. 1 = living with spouse only; 2 = with spouse and children; 3 = without spouse but with children; 4 = others; MPCE = monthly per capita expenditure.
refers pvalue <0.001 (for Pearson’s chi-square test statistics).
Work Status of the Elderly by Living Arrangements in Four States in South India
Table 3 reveals that more than half of the elderly who lived with only the spouse were economically independent, whereas 32% were fully dependent on others for their economic needs. Three fourths of the older adults, living with children in the absence of spouse, were fully dependent economically. Out of all elderly living with others, 46% were fully dependent, and 36% were economically independent. A large proportion of the elderly population was not being paid for their economic contribution, and this was highest among those who were living with others, that is, apart from spouse and children. Most of the economically dependent elderly were supported by some other living arrangement, not with spouse or children.
Percentile Distribution of the Elderly From Different Living Arrangements by Their Economic Conditions and Activity Status in the States of South India, 2004.

Table 4 shows the result of multinomial logistic regression analysis in terms of adjusted percentage of usual activity status of the elderly by their background characteristics. Results revealed that a huge proportion of the elderly were working in the advanced years of their life, though most of them were working as unpaid workers. Around 61% of the workers in the 75 to 79 years age group and 77% of the oldest old population worked as unpaid workers. There were no significant rural–urban differences within different categories of work. Females were more likely to work as paid workers than their male counterparts. A substantially higher proportion of the elderly from the Hindu or Muslim community worked as unpaid workers. A significantly high proportion of the elderly from Other Backward Castes (OBC) and other social groups, with primary education or more and living either with the children in the absence of the spouse or with others, worked as unpaid workers.
Multinomial Logistic Regression Analysis of Usual Activity Status (%) Among the Elderly Population, 2004.

Note. MPCE = monthly per capita expenditure.
refers 0.05 < p value < 0.1.
refers 0.01 < p value < 0.05.
refers p value <0.01.
Morbidity Prevalence and Treatment Seeking Among the Elderly in Four States in South India
Table 5 suggests that the prevalence of any ailment was highest among the elderly from Kerala, followed by those in erstwhile Andhra Pradesh, Karnataka, and Tamil Nadu. Prevalence of NCDs did not vary substantially by living arrangement irrespective of the state the elderly belonged to, but there were significant variations in the prevalence of NCDs among the four states. Regardless of the type of living arrangement, around 45% of the elderly suffered from NCDs in Kerala, which was the highest when compared with the three other states of South India, and the lowest prevalence was in Tamil Nadu. NCDs were more prevalent among the elderly from the oldest old age groups, urban, female, Muslim or OBC, and in higher education or highest MPCE quintile. Prevalence of NCDs was relatively lower among the elderly living either with only the spouse or with children, and high among those who lived with others.
Prevalence of Morbidity (Values in %) Among the Elderly by Background Characteristics in Different Settings of Living Arrangements in the States of South India, 2004.
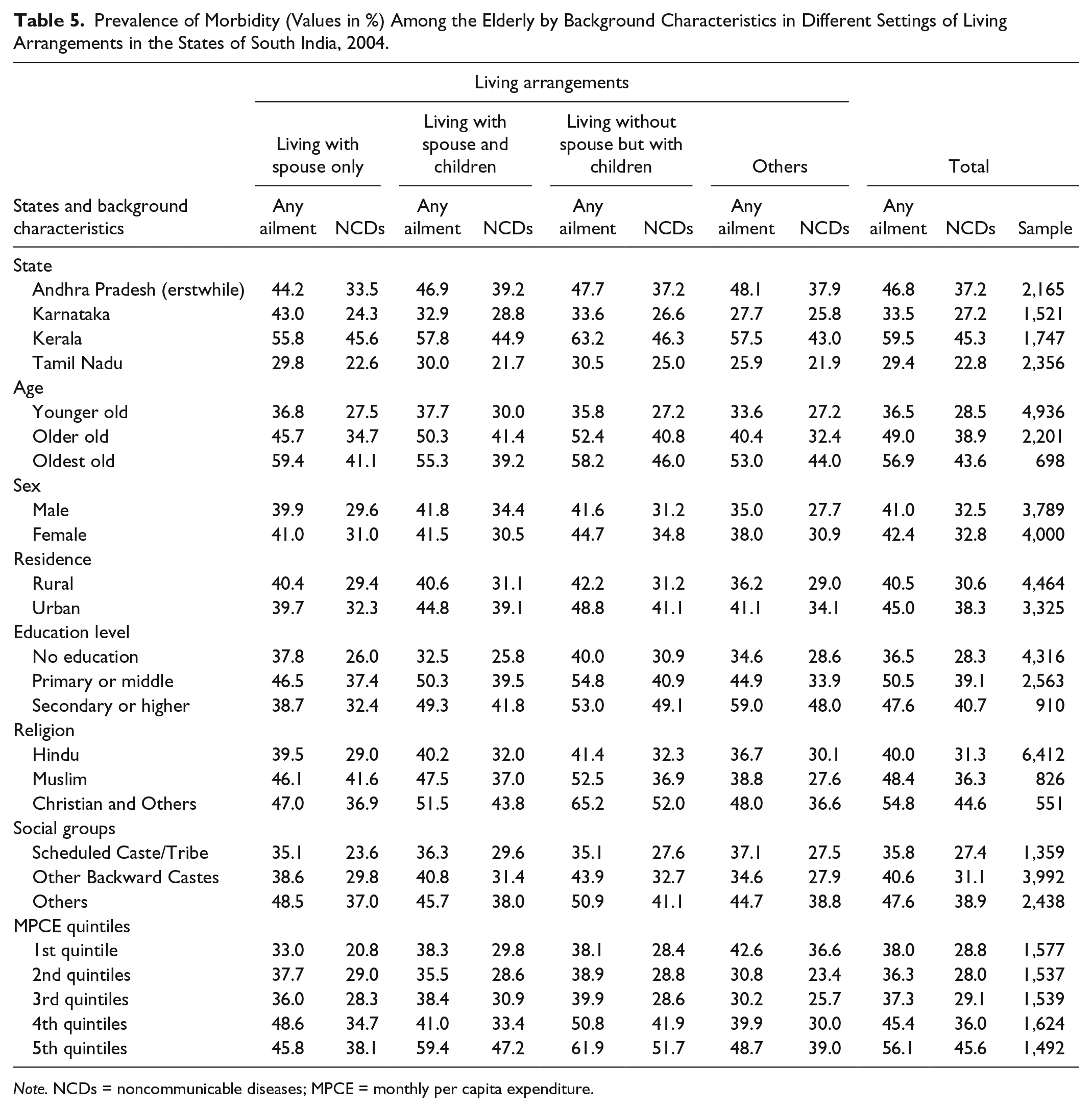
Note. NCDs = noncommunicable diseases; MPCE = monthly per capita expenditure.
The proportion of elderly seeking treatment for any ailment as well as for NCDs was highest in Kerala (around 85%) and lowest for Karnataka (around 62%). Table 6 suggests that in Kerala and Karnataka, the treatment rate was higher for those elderly who were living only with the spouse, whereas in erstwhile Andhra Pradesh and Tamil Nadu, the treatment rate was higher for those who were living with the spouse and children. This pattern indicates better availability and accessibility of health facilities in Kerala and Karnataka. The treatment rate declined for any ailment as well as for NCDs as age increased, but it was lowest for those elderly who were living with only the spouse. The treatment rate was slightly higher among the male elderly and those who belonged to urban areas. Treatment of NCDs was higher among the elderly from the higher education group, higher MPCE quintile, Muslim community, and OBCs.
Treatment Rate by Different Background Characteristics of the Elderly in Different Settings of Living Arrangements in the States of South India, 2004.

Note. 1 = living with spouse only; 2 = with spouse and children; 3 = without spouse but with children; 4 = others; MPCE = monthly per capita expenditure; TAA = treatment for any ailment; TNCD = treatment for Noncommunicable disease.
Factors Related to Prevalence and Treatment Seeking of Any Ailment and NCDs Among the Elderly
Age, sex, MPCE, and usual activity status show significant associations with the prevalence of any ailment among the elderly (Table 7). On the contrary, place of residence shows considerable differences in the prevalence of NCDs among elderly. Urban elderly were 48% more likely to suffer from NCDs than their rural counterparts. Treatment seeking for any ailment or NCDs decreased as the elderly move from younger old to the oldest old age group in spite of increasing prevalence of any ailments with age. Those elderly with primary- and middle-level education were more likely to go seek treatment than their uneducated counterparts. The likelihood of treatment seeking increases with the rise in economic status as reflected by the MPCE quintile for both ailments and NCDs. The elderly from Karnataka were 45% less likely to seek treatment, whereas the elderly from Kerala were 45% more likely to seek treatment when compared with the elderly living in erstwhile Andhra Pradesh.
Result of Logistic Regression Analysis Representing Odds Ratio of Suffering and Treatment of Any Ailment and NCD Among the Elderly in the States of South India, 2004.

Note. Models are adjusted for caste, religion, economic dependence, and education level of elderly. NCD = noncommunicable disease; ® = reference category; MPCE = monthly per capita expenditure.
refers 0.05 < p value < 0.1.
refers 0.01 < p value < 0.05.
refers p value < 0.01.
Summary and Conclusion
The elderly population in the late stages of life seeks more attention in terms of emotional, social, and economic support and proper health care (Golandaj, Goli, & Das, 2013; Rajan & Kumar, 2003). Thus, in the four states in South India, that is, erstwhile Andhra Pradesh, Karnataka, Tamil Nadu, and Karnataka, the family still plays an important role and the elderly live mostly with the members of their family, either with or without spouse. The Indian traditional joint family system has started changing into the nuclear system and this raises the point of vulnerability among the elderly. But, till now majority of the elderly live with the spouse and other members or with children in the absence of the spouse. Various researchers have expressed concern about the likelihood of an increase in the proportion of the elderly living either alone or with only the spouse in the near future (Conklin, 1988; Dhruvarajan, 1988; Sharma, Dak, & HelpAge India, 1987). The SES of the elderly is very poor even in the relatively more developed states of South India. Among the four states in South India, Kerala presents a better picture for the elderly in terms of their educational and financial status.
Second, living arrangement tends to affect the work status of the elderly living with only the spouse, and most of them are economically independent, whereas females who are living without spouse but with their children are mostly, totally dependent. Most of the elderly living with others work as unpaid workers. Thus, the evidence based on the analyses suggests that living arrangement affects the work status of the elderly in South India and probably in India as a whole. Generally, in the Indian setting, the elderly, despite their poor health, are bound to work for their livelihood if they live alone or with only the spouse. Availability of government-funded institutional care for the elderly is very uncommon in India, even in states with increased proportions of the elderly. Therefore, this study underlines the urgent need for the government to provide financial support and institutional care to the needy elderly and build government-run old age homes at least for the vulnerable elderly.
Finally, the analysis suggests that the prevalence of NCDs is lower among those elderly who live either with only the spouse or with children. The prevalence of NCDs is higher among the elderly living with spouse along with other members of the family, and this perhaps can be attributed to the actual reporting of ailments. Treatment seeking is highest among the elderly living with spouse and other members of the family and lowest among those living with others. The treatment rate is proportionately related to education, MPCE quintile, caste, and place of residence, whereas it changes disproportionately with age. Those elderly who live with others apart from spouse or children are more vulnerable to poor health and are likely to work for their livelihood. If those elderly who work are in good health, it is a positive sign for the country’s economy; on the contrary, if the elderly are in poor health and have to work for their livelihood or to support their family, it sheds a negative hue on that society and economy.
This study throws light on the emerging consequences of a weak social support system on the aging population in Indian society. The increasing number of female elderly at later ages, their poor SES, changing family structures, and the consequences of living alone or with only the spouse indicates the vulnerability of the Indian elderly. Familial support at later ages plays a significant role in elderly well-being. Those elderly who live with their children are more likely to have better health and health care compared with those who live without children. A significant proportion of the elderly are forced to earn their livelihood even in their later ages, and this situation becomes miserable for the elderly who come from lower SES. This situation points to the dire need to strengthen the social support system for the elderly and provide them a better and healthier life.
This article advocates for a strong social support system for the elderly in India, the need to ensure the availability of proper geriatric health care facilities so that changing familial norms do not affect their well-being. With the establishment of a proper elderly support system, India will be able to prove that its elderly population are assets rather than liabilities. On the eve of the International Day for Older Persons, the United Nations announced that the healthy elderly are a resource of the family, society, and even the economy of their country.
Footnotes
Acknowledgements
We acknowledge the contribution of Dr. Sanjay Kumar Mohanty, Professor, Department of Fertility Studies, International Institute for Population Sciences, Mumbai, for his valuable comments and suggestions during preparation of the final draft of this article. We are also grateful to Dr. Debasis Barik, Associate Fellow, National Council of Applied Economic Research, New Delhi, for his advices and suggestions during research design and analysis of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.