
Abstract
Fertility divergence amid declining in use of modern contraception in many states of India needs urgent research and programmatic attention. Although utilization of antenatal, natal, and post-natal care has shown spectacular increase in post National Rural Health Mission (NRHM) period, the contraceptive use had shown a declining trend. Using the calendar data from the National Family Health Survey–3, this article examines the reasons of contraceptive discontinuation among spacing method users by socio-economic groups in India. Bivariate and multivariate analyses and life table discontinuation rates are used in the analyses. Results suggest that about half of the pill users, two fifths of the condom users, one third of traditional method users, and one fifth of IUD users discontinue a method in first 12 months of use. However, the discontinuation of all three modern spacing methods declines in subsequent period (within 12-36 months). The probability of method failure was highest among traditional method users and higher among poor and less educated that may lead to unwanted/mistimed birth. Although discontinuation of condom declines with economic status, it does not show any large variation for pill users. The contraceptive discontinuation was significantly associated with duration of use, age, parity, contraceptive method, religion, and contraceptive intention. Based on these findings, it is suggested that follow-up services to modern spacing method users, increasing counseling for spacing method users, motivating the traditional method user to use modern spacing method, and improving the overall quality of family planning services can reduce the discontinuation of spacing method.
Keywords
Introduction
Investment on family planning has multiple returns: demographic, health, social, and economic benefits at individual, familial, and societal levels. Improved access and use of family planning improves child survival, reduces unwanted pregnancies and abortion, and improves health of mother and children (Gipson, Koenig, & Hindin, 2008; Kavanaugh & Anderson, 2013). The social and economic benefits include increased schooling of children and mothers, higher familial stability, increased work participation among women, increased wage, and reduction in poverty (Sonfield, Hasstedt, Kavanaugh, & Anderson, 2013). At societal level, increased use of contraception acts as a catalyst in the process of development and reduces regional disparity.
Despite strong benefit of contraception, the pattern and use of contraception varies largely across countries. In developing countries, though the use of any contraceptive method has increased from 44% in 1980 to 61% in 2009, the unmet need of contraception remains high, the method mix of contraception remain skewed, the quality of care of family planning services remained poor, and contraceptive discontinuation remained high (Bradley, Schwandt, & Khan, 2009; Seiber, Bertrand, & Sullivan, 2007; Steele & Diamond, 1999; Sullivan, Bertrand, Rice, & Shelton, 2006). Contraceptive continuation is considered to be a summary outcome indicator of the quality of family planning services (Bertrand, 1994; Blanc, Curtis, & Croft 1999; Bruce, 1990; Jain, Bruce, & Mensch, 1992; Koenig, Hossain, & Whittaker, 1997; Magnani, Hotchkiss, Florence, & Shafer, 1999; Pariani, Heer, & Van Arsdol, 1991; RamaRao, Lacuesta, Costello, Pangolibay, & Jones, 2003; Steele, Curtis, & Choe, 1999). To large extents, the unintended pregnancies are attributable to contraceptive discontinuation due to method failure and abandonment of contraception while being in the need (Cleland & Ali, 2004). In countries passing through demographic transition, a further decline in fertility depends upon the consistent, correct, and effective use of contraception (Blanc, Curtis, & Croft, 2002; Vaughan, Trussell, Kost, Singh, & Jones, 2008). Jain (1989) and Blanc et al. (2002) propounded to shift the focus of family planning program from providing contraception to new clients toward quality services to promote the continuation.
The contraceptive discontinuation varies greatly by the level of overall contraceptive use and by type of methods. The contraceptive discontinuation was lowest among IUD and implant users followed by injectable, condoms, and oral contraceptive users (Ali & Cleland, 1995; Blanc et al., 2002; Bradley et al., 2009; Steele & Curtis, 2003). Steele and Curtis (2003) concluded that the method choice is endogenous to discontinuation. The reasons associated with contraceptive discontinuation can be broadly categorized into four groups: method-related reasons, contraceptive failure, reduced need, and non-method-related reasons. Among method-related reasons, health concerns and side effects were frequently cited by pill and IUD users, whereas accidental pregnancy was frequently cited among traditional method users (Ali & Cleland, 1995; Mitra & Al-Sabir, 1996; Singh, Roy, & Singh, 2010). The differentials in failure rates were largely due to differences in service delivery, user characteristics, and defining the failure rates (Ali & Cleland, 1995; Jejeebhoy, 1991; Sambisa & Curtis, 1997). In United States, the failure rates for implants and IUDs were lowest, and it was highest for the traditional methods and spermicides (Trussell, 2011). Lack of adequate counseling and partner disapproved the use of method were more likely to discontinue a method (Cotten, Stanback, Maidouka, Taylor-Thomas, & Turk, 1992). The reduced need includes the following: those who wanted to become pregnant, husband away, infrequent sex, difficult to get pregnant/menopausal, and marital dissolution. The non-method-related reasons are desire to get pregnant, lack of access/availability, wanted more effective method, cost, inconvenient to use, did not like method, lack of sexual satisfaction, lack of privacy for use, husband disapproved, fatalistic, and other reasons (Bradley et al., 2009). Literature suggests that age at the time of discontinuation, family size, fertility preferences, the prior use of a method, contraceptive method chosen, and prior experience with the method were significant predictors of discontinuation (Ali & Cleland, 1999; Arifin, 2003; Bradley et al., 2009; Curtis & Blanc, 1997; Fathonah, 1996; Hamill, Tsui, & Thapa, 1990; Mitra & Al-Sabir, 1996; Moreno, 1993; Perez & Tabije, 1996; Sambisa, 1996; Steele, Diamond, & Wang, 1996; Zhang, Tsui, & Suchindran, 1999). On the contrary, place of residence and educational attainment had little or inconsistent impact on method failure across and within countries (Curtis & Blanc, 1997).
India’s demographic transition is of global significance due to its size (accounting 17% of global population) and large variation in demographic and health parameters within the country. Also, the country has launched the largest flagship program, the National Rural Health mission (NRHM), in 2005, to improve the utilization of reproductive and child health (RCH) services in the country and achieve the demographic targets. Although the Total Fertility Rate (TFR) has reached 2.3 in 2013 (Office of the Registrar General, India, 2013), fertility trends are diverging across states and districts of India (Mohanty, Fink, Chauhan, & Canning, 2016). The TFR in the state of Bihar was estimated at 3.4 in 2015 with only 24% women using any contraceptive method (International Institute for Population Sciences [IIPS], 2016). With regard to contraceptive use, the use of modern spacing methods of contraception remained low in India. By 2005 to 2006, only 10% women were using any modern spacing method with large variation across socio-economic groups and space. Not only the adoption of spacing method is low but the continuity of these methods also remains a concern: 49% pill users, 45% condom users, and 20% IUD users discontinued the method within a year of adoption (IIPS and Macro International, 2007). Moreover, the median age of female sterilization has declined from 26.6 years in 1992-93 to 25.5 years by 2005-06, and about 5% sterilized women regretted their decision of getting sterilized. The NRHM has been successful in increasing the facility based delivery, reduced cost of delivery care, and reduced maternal, neonatal, and infant mortality in India (Lim et al., 2010; Mohanty & Srivastava, 2013). However, the use of modern spacing method has not increased in India. This is further confirmed by reduction in use of modern contraceptive method in 10 of the 15 states for which the key indicators from National Family Health Survey–3 (NFHS-3) have been recently released (IIPS, 2016). In a recent study on contraceptive use in India, Chaurasia (2014) has identified 13 distinct groups that need programmatic attention to improve the family planning services.
Studies in India have extensively focused on trends, differentials, and determinants of contraceptive use (Bhat & Zavier, 2005; Blanc, Tsui, Croft, & Trevitt, 2009; Guilmoto & Rajan, 2001; Mohanty & Ram, 2011; Ram, Dwivedi, & Goswami, 2007) and less focused on the post-adoption contraceptive behavior (Zhang et al., 1999). The increasing use of traditional methods, high unmet need for modern spacing method, high unwanted childbearing, and low birth spacing necessitate an investigation of the correlates on discontinuation of spacing method in India. Accordingly, the aim of this article is twofold: (a) to examine the socio-economic and demographic differentials in discontinuation of spacing methods and (b) to understand the factors associated with the reasons of discontinuation of spacing method in India.
Data
Research on contraceptive discontinuation in India is limited due to paucity of data on contraceptive history. The NFHS-3, 2005-06, third in the series of demographic and health survey in India, for the first time collected contraceptive history along with information on fertility, nutrition, morbidity, and so on from a representative sample of more than 124,385 women throughout the country. The calendar data in NFHS-3, collected month-by-month history on four events: (a) births, pregnancies, and contraceptive use and non-use; (b) reason for contraception discontinuation; (c) marriage; and (d) ultrasonography during pregnancy. These information were collected from sampled women aged 15 to 49 years in the 5 years preceding the survey. A detailed description of the sample design, preliminary finding, and the schedule is available in the national report (IIPS and Macro International, 2007). We have used the calendar data along with women and household files from the NFHS-3 to analyze the reasons of contraceptive discontinuation by methods among socio-economic groups in India.
The calendar data are decoded, and episodes of contraceptive use are prepared. An episode is defined as an uninterrupted period of specific contraceptive method use. A switch to another method initiates a new episode of contraceptive use. A woman may use more than one method of contraception and also may restart using the same method; therefore, she may also contribute more than one episode in the study sample. For example, in an observation period of 5 years, if a woman uses pills for 10 months and discontinues it for 20 months and again reuses IUD for 15 months, she is said to have contributed two episodes. To analyze the calendar data, for each episode, five types of variables were created: the current method of contraception, the corresponding reason for discontinuation, the next month’s status after discontinuation, the duration of use, and the beginning date of current method of contraception in century month code (CMC). The episodes started in 3 to 62 months prior to the survey have been included in the analysis. Episodes started 3 months immediately before the survey were excluded to avoid the first trimester underreporting of contraceptive failure (Curtis & Hammerslough, 1995; Moreno, 1993). The episodes of pill, IUD, condom, and traditional methods (periodic abstinence and withdrawal) were analyzed while episodes of use of injections, diaphragm, norplants/implants, female condom, and other traditional methods were not analyzed because of too few cases. The number of episodes for pill, IUD, condom, and traditional methods were sufficiently large to draw the socio-economic differences by reasons of discontinuation at national level. The survey recorded 20 reasons of discontinuation, and for analytical reasons, we have grouped them into four categories: contraceptive failure (became pregnant while using), side effect/health concern (side effect, health concerns, gained weight, and created menstrual problem), reduced need (wanted to become pregnant, husband away/infrequent sex, difficult to get pregnant/menopausal, and marital dissolution), and others (access/availability, wanted more effective method, cost, inconvenient to use, did not like the method, lack of sexual satisfaction, lack of privacy for use, husband disapproved, fatalistic, other reasons, don’t know, and missing).
Method
Descriptive statistics, bivariate analyses, discontinuation rates using the single/multiple decrement life table, and multi-level multinomial competing risk analyses have been carried out. The unit of analysis is episode of contraception use among all women aged 15 to 49 years. In the calendar data, a woman is at the risk of discontinuation at any point in time for various reasons and so this type of data is often described as competing-risks data. The gross life table rates are calculated for comparisons across subgroups or countries. The net life table rates are calculated with the multiple decrement life table approach for modelling the observed dependent rates. The multi-level discrete-time competing-risks hazards models (equivalent to multi-level multinomial logistic model; Goldstein, 1995; Steele & Diamond, 1999; Steele et al., 1996) are used to understand the factors associated with each type of reason for discontinuation at a given duration of use. The model used in the analyses is of the following form:

where hrtijk is the hazard of reason of type r at duration t for use episode of i of woman j in cluster k. The term h4tijk is hazard of continuing use of the same method. The αrt term (baseline hazard; is some function of the duration of the episode t) has been presented in a quadratic formulation
Results
We begin the discussion by schematic presentation of eligible women and episodes considered in the analyses. Out of 124,385 women, 62,766 women never used any contraception in the last 5 years, and 23,534 women were sterilized prior to the observation period 1 and so excluded from the analyses (Figure 1). A total of 38,085 women used any spacing method or encountered termination or opted for sterilization at the any time in the 5-year period preceding the survey and contributed 57,087 episodes. The left censoring 2 excluded 31,395 episodes, and therefore 25,692 episodes were used in the analyses.

Schematic presentation of the sample selected.
Sample Characteristics: Mean Number of Episodes Per Woman
Table 1 presents the percentage distribution of episodes and the mean number of episodes according to women’s selected socio-economic and demographic characteristics. About 73% women had one episodes of contraceptive use, 19% women had two episodes of use, and 7% women had three or more episode of use. Majority of the episodes were ended as one episode (three fourths) because female sterilization is largely practiced in the country. Women go for sterilization soon after reaching the desired number of children. The mean number of episodes was 1.4 and varies marginally by age. Among women aged less than 25 years, 25% episodes were of Order 2 and above compared with 29% among women aged 25 to 34 years. The percentage distribution of two or more episodes and the mean number of episodes increased with educational attainment and economic well being of women. This suggests that higher educated and economically better-off women are more likely to use more contraceptive methods because they are aware of different methods and can afford these methods. The contribution of two or more episodes increased with the parity and declined slightly among women with three or more children. The mean number of episode among women in Parity 0 was 1.17 compared with 1.5 for those who were in Parity 2. Women who used contraceptives with the intention of limiting the births were more likely to add two or more episodes compared with spacers. The percentage of women with two or more episodes was maximum in the Northeastern region and minimum in the Northern regions. Although the IUD users had 4.5% of two or more episodes, it was 20% among traditional method users, 13% among condom users, and 12% among pill users. There are not many differences in mean episode by caste and religion. Similarly, the mean episode use does not vary by living arrangement, analyzed by nuclear and non-nuclear families.
Percentage Distribution and Mean Number of Episodes of Pill, IUD, Condom, and Traditional Methods by Women’s Background Characteristics, India.

Contraceptive Discontinuation by Methods and Reasons in India
Figure 2 presents the method-specific gross life table cumulative probabilities of discontinuation for pill, IUD, condom, and traditional methods. The overall discontinuation for any reason was highest among pill users, followed by condom, traditional methods, and IUD users (Figure 2). The level of discontinuation of each of the four methods increased steadily with the duration of use. The probability of discontinuation of pill was 0.49 for the first 12 months, 0.64 in 24 months, and 0.73 in 36 months. The pattern is similar in case of condom: 0.44 for the first 12 months, 0.59 in 24 months, and 0.67 in 36 months. In case of IUD, the probability of discontinuation was lowest: 0.19 in the first 12 months, 0.34 in 24 months, and 0.56 in 36 months. This is possibly because the discontinuation of IUD requires the help of clinician, whereas the pills may be discontinued due to irregular use or lack of supply. The traditional method users may become non-users due to sporadic sex or switched to modern method. These findings are consistent from cross-national studies reported elsewhere (Ali & Cleland, 1995; Bradley et al., 2009; Curtis & Blanc, 1997; Singh et al., 2010).
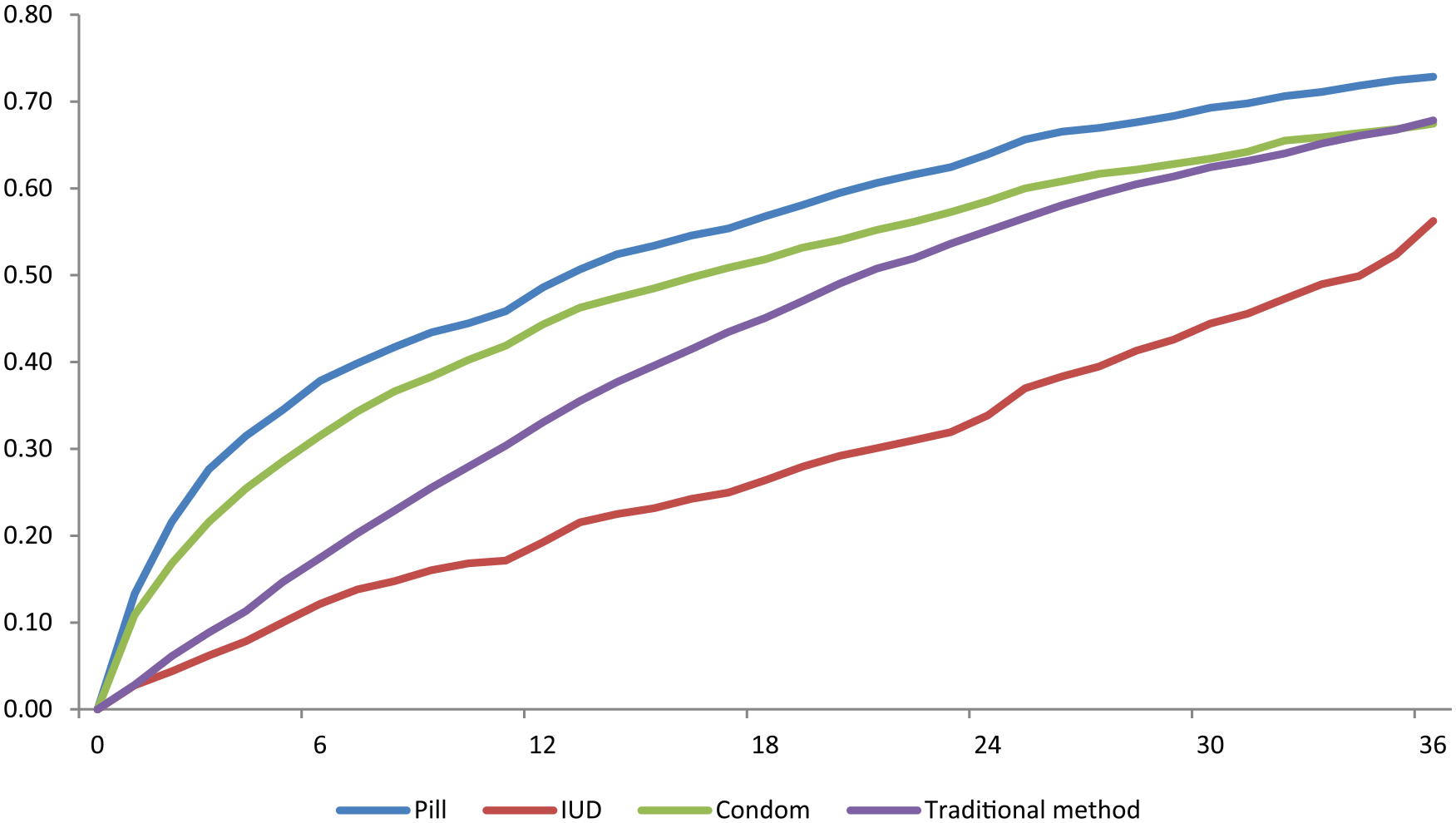
Gross life table cumulative probability of discontinuation for reversible methods, India, 2000 to 2006.
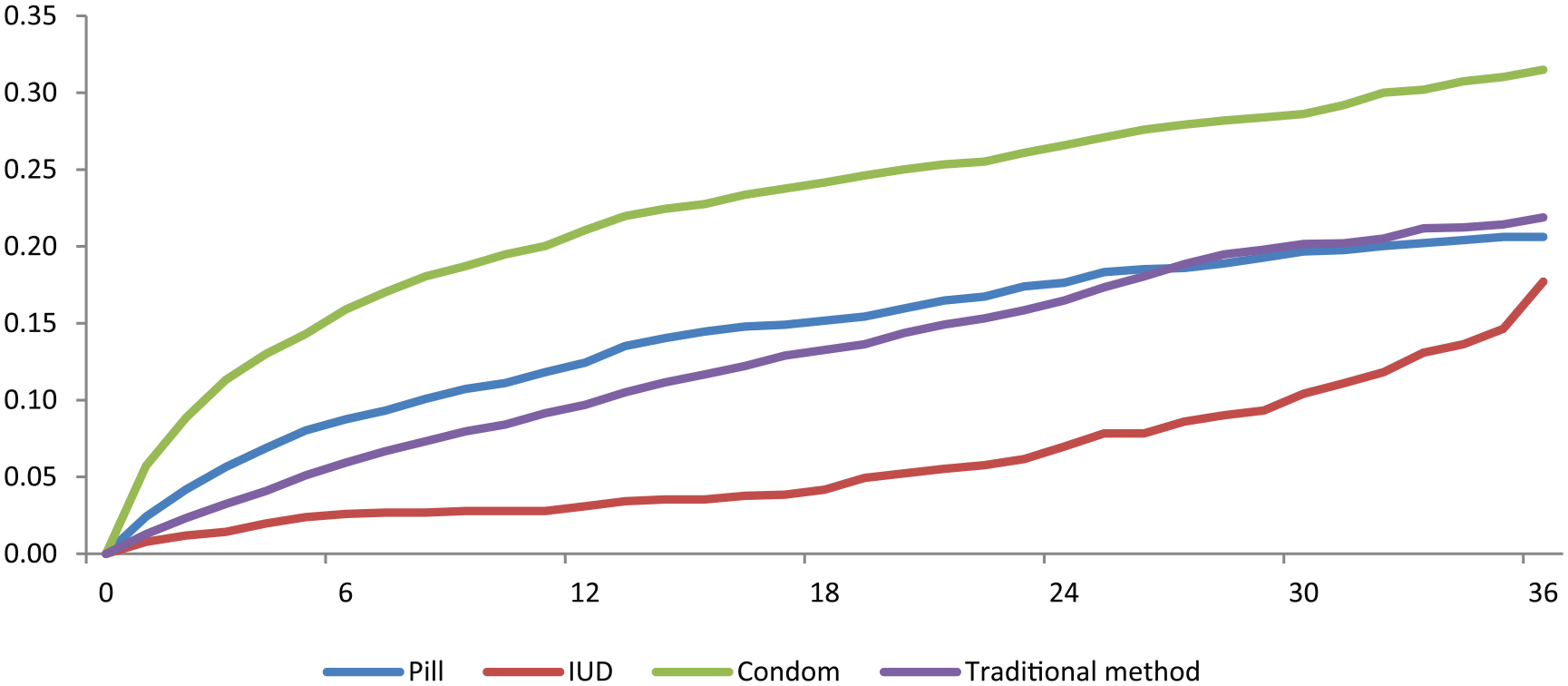
We further present the probability of discontinuation by reasons of discontinuation (Figures 3-6). The probability of discontinuation due to method failure was highest among traditional method users: 0.04 in first 12 months, 0.17 in 24 months, and 0.24 within 36 months. On the contrary, the discontinuation of IUD due to method failure is lowest: 0.009 in 12 months, 0.015 in 24 months, and 0.017 in 36 months (Figure 3). The probability of discontinuation due to side effect/health concern was highest for pill and IUD and lowest for traditional methods. The probability of discontinuation of pill due to side effect/health concern was 0.25 in 12 months, 0.33 in 24 months, and 0.40 in 36 months (Figure 4). Although the level of discontinuation for IUD is lower than pill, the patterns of discontinuation due to specific reasons are similar for both the methods. The side effect of pill and IUDs are the main reason of discontinuation of these methods. Many women using IUD and pill complain about weight gain, physical disorder, nausea, and related health problem compared to traditional method use. As expected, the discontinuation due to side effect/health concern remained low for condom and traditional method users. This is because the condoms are male methods whereas the traditional method does not involve use of any chemical substances. However, discontinuation due to reduced need was maximum among condom users followed by traditional method users (Figure 5). The probability of discontinuation due to reduced need among condom users was 0.23 in 12 months, 0.36 in 24 months, and 0.44 in 36 months. We have combined the reasons like husband did not approve or did not like the method into other reasons. We found that the probability of discontinuation due to other reasons was highest among condom users followed by pill and traditional method users (Figure 5). A comparison across the methods reveals that the side effect/health concerns were the main reason for discontinuation of pill and IUD while accidental pregnancies were among traditional method use and other reasons for discontinuation of condoms. The discontinuation rates are higher among those living in non-nuclear families than those living in nuclear families.

Gross life table probabilities of discontinuation due to method failure for reversible methods, India, 2000 to 2006.

Gross life table cumulative probabilities of discontinuation due to side effects/health concerns for reversible methods, India, 2005 to 2006.

Gross life table cumulative probabilities of discontinuation due to reduced need for reversible methods, India, 2005 to 2006.
Gross life table cumulative probabilities of discontinuation due to other reasons, India, 2000 to 2006.
Socio-Economic Differentials in Discontinuation Rate of Contraceptive Methods in India
In this section, the life table net discontinuation rates within 12 months of initiation for each of the pill, IUD, condom, and traditional methods by socio-economic and demographic characteristics of women are discussed (Table 2-3). Among pill users, the level of discontinuation decreased with age: from 60% among women below 25 years to 39% each in age groups 25 to 34 and 35 to 49. Similarly, the level of discontinuation decreased with parity because women with higher parity might have achieved their desired family size while women at younger parity are likely to postpone childbearing for certain time. With education, the discontinuation of pill declines first, and rises afterward with educational attainment. For example, the discontinuation rate was 48% among women with no education, 42% among women with less than 5 years of schooling, 47% among women with 5 to 9 years of schooling, and 53% among women with 10 years or more schooling. This is in contrast to the global trend where the discontinuation of pill users is more among less-educated women. The higher discontinuation of pill among educated women is possibly due to side effect of methods and switching to female sterilization. Similarly, the discontinuation of pill by wealth quintile varies in the smaller range of 6%: 51% among the poorest, 50% among the poorer, 48% among the middle, 45% among the richer, and 49% among the richest. This is possibly because, like female sterilization, the pills are also distributed by public health centers at free of cost and accessible to rich and poor alike. The discontinuation of pill was higher among women residing in rural areas and women belonging to Hindu religion. In case of IUD, the discontinuation was maximum among Muslims and minimum among Christians. There are no significant differentials in discontinuation of traditional methods by caste and religion. On the contrary, women who practiced contraception with the intention of limiting are likely to continue longer than those who had intention to space (discontinuation rate of 41% vs. 59%). This is indicative that a significantly higher proportion of woman used pill to space between the births. The discontinuation rates of pills are stark among the regions of India: varying from 38% in Northeast to 67% each in Central and Southern regions. In Southern and Central regions, the female sterilization is the most practiced method and women opt for sterilization on achieving their desired family size. It also depends on the promotion of method by the respective state governments. The discontinuation of pills by reasons showed that it was largely due to side effect/health concern followed by reduced need and others. Although the level of discontinuation varies by reasons, the reasons are similar across socio-economic characteristics of women. The side effect/health concern is the single most reason of discontinuation of pill across socio-economic groups.
The 12-Month Net Cumulative Life Table Discontinuation Rates for Oral Pill and IUD by Reason For Discontinuation, According To Women’s Background Characteristics, India, 2000 to 2006.
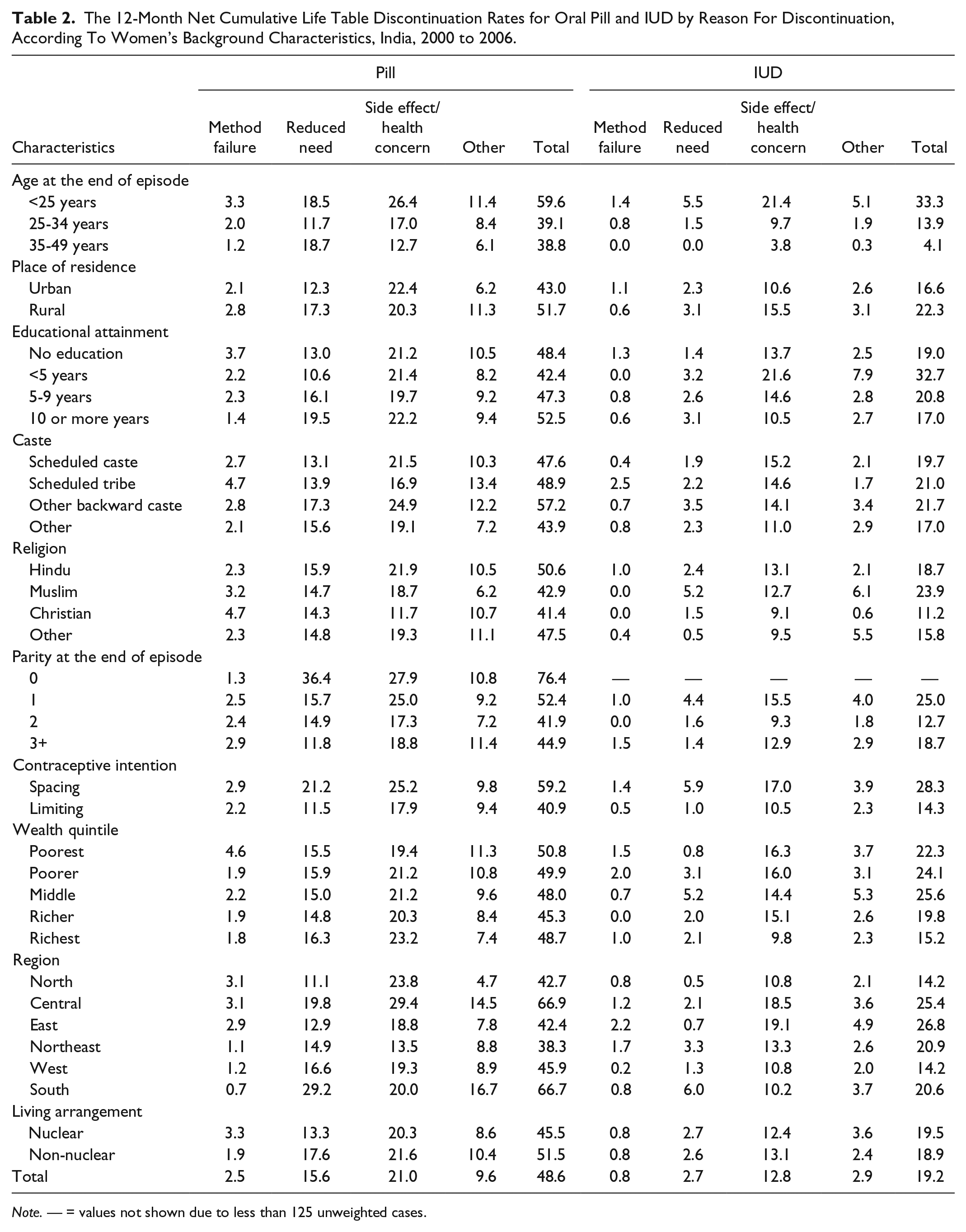
Note. — = values not shown due to less than 125 unweighted cases.
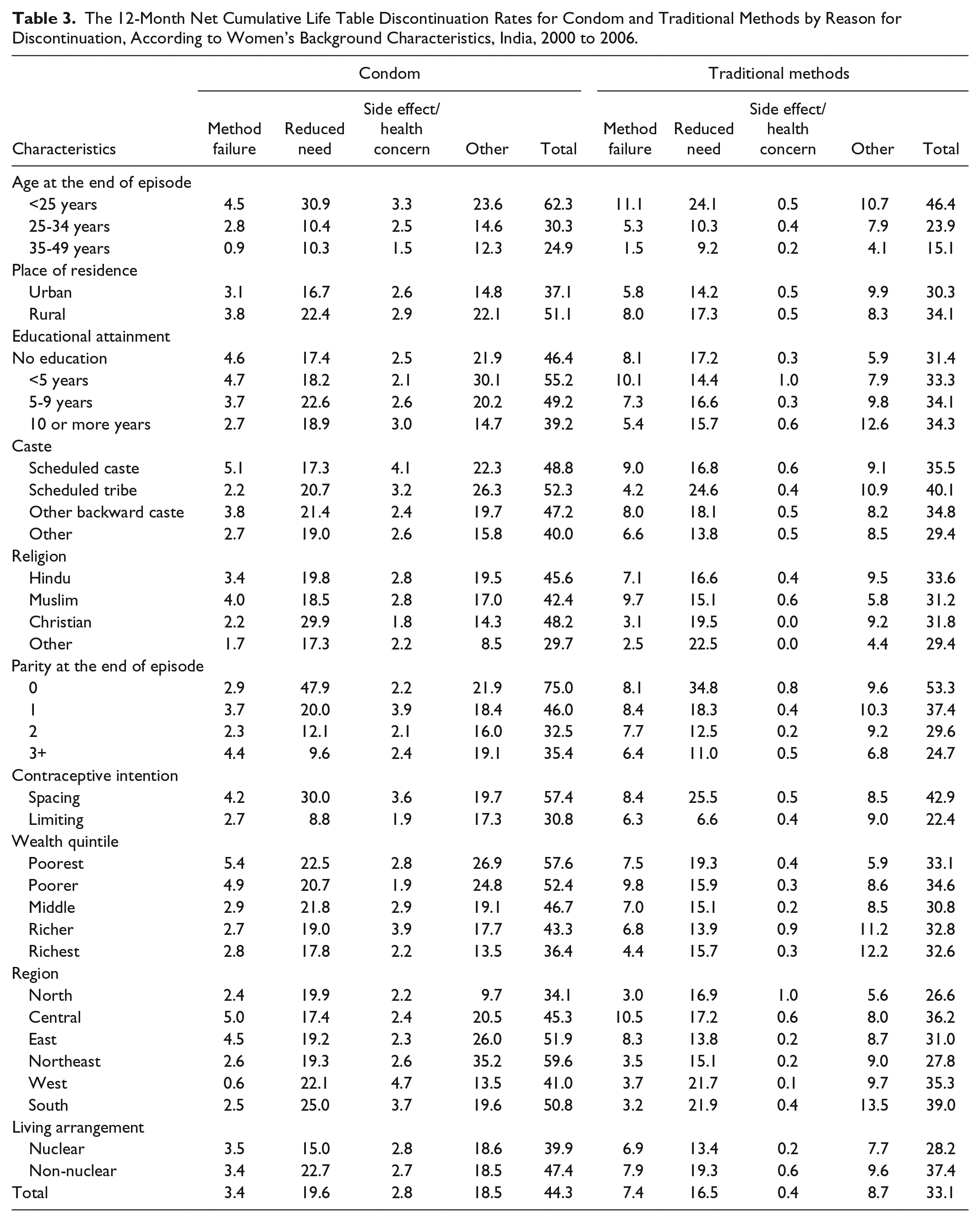
The 12-Month Net Cumulative Life Table Discontinuation Rates for Condom and Traditional Methods by Reason for Discontinuation, According to Women’s Background Characteristics, India, 2000 to 2006.
Like pill, the discontinuation of IUD decreases with age: from 33% among women below 25 years to 14% in 25 to 34 years and 4% among women in 35 to 49 years. The discontinuation is higher among younger women compared with older women because younger women want to go achieve their desired family size and also try different methods while older women might have achieved their desired family size. With respect to education, we found a sharp increase in discontinuation rate of IUDs: from 19% among illiterate to 33% among those with less than 5 years of education which further declined to 20% among women with 5 to 9 years of education and 17% among women with 10 or more years of education. In general, women with little education are more likely to discontinue IUD than illiterate or better-educated women. Similarly, with respect to wealth quintile, the discontinuation of IUD was lower among poorest and richest wealth quintile but higher in middle wealth quintile. The discontinuation of IUD among women intended to space between the births/delay pregnancies was double to that of those intended to limit the births. The discontinuation of IUD was low in Western and Northern regions and highest in Eastern regions. Like pill, the side effect/health concern is the single most cause of discontinuation and minimal for method failure. The overall rate of discontinuation for IUD is lower than the pill across all socio-economic groups in India.
Among the condom users, the first 12-month discontinuation rate declined sharply with the age, parity, educational attainment, and wealth quintile. With respect to age, the discontinuation rate was 62% among women below 25 years, 30% in 25 to 34 years, and 25% in 35 to 49 years. The discontinuation rate was 75% in Parity 0, 46% in Parity 1, 33% in Parity 2, and 35% in Parity 3. It may be mentioned that the condom is a male method and also used for prevention of HIV/AIDS. Younger couple may be using condom to space for birth or delay pregnancy and so discontinue the method. Although the discontinuation of condom did not show any pattern with respect to education, it declines with respect to economic status of household. The discontinuation of condom among poorest wealth quintile was 58% compared with 36% among richest wealth quintile. The discontinuation rate of condom was substantially high in rural areas, and among scheduled tribe and Hindu women. Compared with limiters, the level of condom discontinuation was almost double among those who were practicing contraception with the intention of spacing or delaying the births. At the regional level, the discontinuation rate among condom users varied from 34% in Northern states to 60% in Northeastern states. The reasons associated with the discontinuation of condom were mostly reduced need and other reasons, though this pattern differed across subgroups. For example, the discontinuation due to reduced need and other reasons was 48% and 22%, respectively, in zero parity, compared with 10% and 19%, respectively, in Parity 3 and above. The method failure as reason of discontinuation for condom is higher than that of pill and IUD. It was 5% among women belonging to poorest wealth quintile and scheduled caste. Although the socio-economic differentials in the discontinuation of pill, IUD, and condoms were evident, the reasons of discontinuation were similar across the subgroups.
Among traditional method users, the discontinuation rate declined with the age and parity. The 12-month discontinuation was 46% among women under 25 years, 24% among women in 25 to 34 years, and 15% among women aged 35 years and older. The pattern is similar with respect to parity. No large difference in discontinuation of traditional method was observed by educational attainment, wealth quintile, and place of residence. The regional differentials in discontinuation of traditional method vary from 27% in Northern states to 39% in Southern states. The method failure as reason for discontinuation is quite large for many socio-economic groups. With respect to age, the method failure of traditional method accounts 11% of discontinuation compared with 2% in age group 35 to 49. It was also high among less-educated, poor, and schedule caste women. Reduced need also accounts substantial discontinuation of traditional methods. Almost two fifths of traditional method users form Southern states discontinued within first 12 months of adoption; a large of proportion cited reduced need (22%) followed by other reasons (14%). However, the 12-month discontinuation rate driven by method failure was very high in the Central (11%) and Eastern regions (8%).
Factors Associated With the Reason For Discontinuation
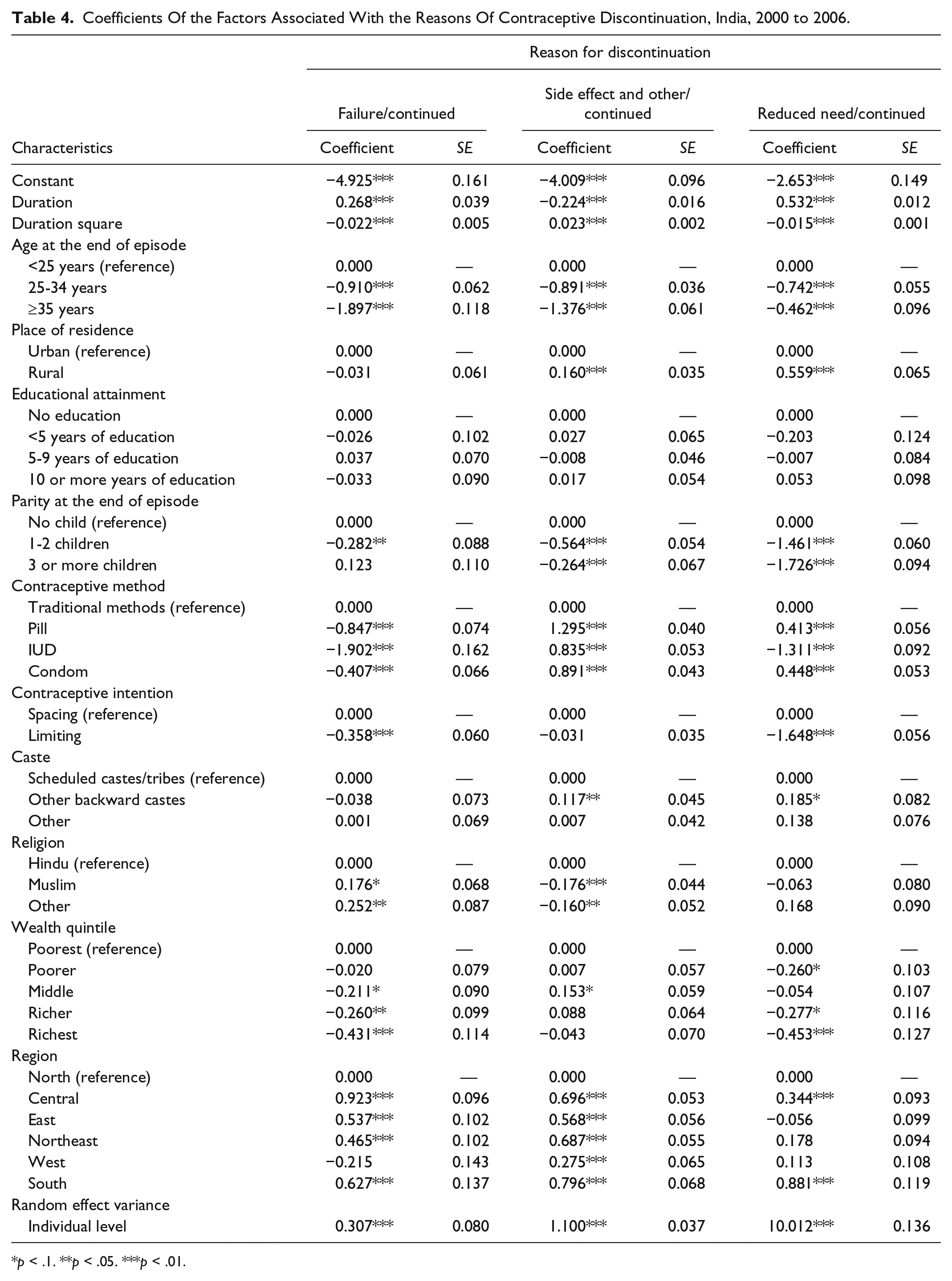
Results from the multi-level discrete-time competing-risks hazard model are presented in Table 4. The contraceptive discontinuation was significantly associated with the duration of use, and with age, parity, contraceptive method, and contraceptive intention. The discontinuation due to method failure was significantly positively associated with the duration of use; however, method failure was not associated linearly with the duration of use. Women aged 25 to 34 years and 35 to 49 years were significantly less likely to discontinue due to contraceptive failure compared with women aged less than 25 years. Discontinuation due to contraceptive failure was significantly lower among women with 1 to 2 children, limiters, and in the users of pill, IUD, and condom compared with their counterparts. The method failure was significantly negatively associated with wealth quintiles. Contraceptive failure was significantly higher among Muslims and other religions compared with Hindus. Except Western region, the contraceptive failure was significantly more in all regions compared with Northern region. Among the predictors of contraceptive discontinuation due to side effect and other reasons combined, the duration of use, age at discontinuation, parity at discontinuation, and religion were significantly negatively associated; however, place of residence, contraceptive method, Muslims and women belonging to other religions, and region of residence were significantly positively associated. The discontinuation due to side effect, health concern, or other reasons declined with the duration of use; however, this was not linearly associated with the duration. Discontinuation due to side effects was less likely among older women and women with children compared with their counterparts. Rural women; users of pill, IUD, and condom; other backward caste women; and women from Central, Eastern, Northeastern, Western, and Southern regions were more likely to discontinue to their method due to side effects.
Coefficients Of the Factors Associated With the Reasons Of Contraceptive Discontinuation, India, 2000 to 2006.
p < .1. **p < .05. ***p < .01.
Discontinuation due to reduced need increased with the duration of use. Discontinuation due to reduced need was significantly negatively associated with older women, with children, practicing with the intention to limit childbearing, IUD users, and in richer wealth quintiles. The factors like rural place of residence, pill and condom users, other backward castes, and Central and Southern regions were significantly positively associated with the discontinuation due to reduced need. After controlling for all these covariates, a large level of heterogeneity remained at the women level. This indicates unobserved factors operating at the level of women, which are unexplained, have role in reasons associated with discontinuation. Steele and Diamond (1999) attributed two women-level factors, which can influence the discontinuation: women’s commitment and motivation to avoid childbearing and experience with the earlier methods and constrain in women’s mobility.
Discussion
In India, the use of modern spacing method remained low due to varying reasons: overemphasis on female sterilization in official family planning program, restricted method choices (pill, IUD, and condom are on official list), poor quality of services, inaccessibility and un-affordability of services, and lack of knowledge on birth spacing (Akoijam, Hanjabam, Longjam, & Thangjam, 2005; Koenig, Foo, & Joshi, 2000; Zavier & Padmadas, 2000). Even among those using a modern spacing method, the discontinuation of methods is high. However, the use of traditional spacing method (abstinence and withdrawal) has shown an increasing trend but the efficacy of such methods in preventing births and pregnancies is low (Ali & Cleland, 1995; Creanga, Acharya, Ahmed, & Tsui, 2007). On the contrary, the unmet need for modern spacing method remained high, and a significant proportion of women articulate their desire to use the modern spacing method in future. Although the RCH program in India has emphasized in promotion of modern spacing method, it has not shown any significant improvement over time. An understanding of the reason for discontinuation is essential from program point of view. In this context, this article examines the pattern and reasons of discontinuation of pill, IUD, condom, and traditional method among socio-economic groups in India using the contraceptive history from the NFHS-3.
We discuss our main findings and their programmatic implications. First, the discontinuation of spacing method was highest for pill users followed by condom, traditional method, and IUD. The discontinuation of IUD needs clinical help whereas that of condom and pill may be discontinued due to irregular use or lack of supply. Furthermore, the discontinuation of each of the method is higher in first 12 months compared with in 12 to 24 months and 24 to 36 months. This clearly suggests that if a woman is satisfied with the method possibly in first few months of use, she is unlikely to continue the same for a longer period. Hence, the follow-up service and counseling for modern spacing method users can increase the continuity of spacing method. The program can benefit by increasing the follow-up visits and expanding the counseling services to the modern spacing method users. Second, the probability of method failure was highest for traditional method user confirming lower efficacy of the method compared with modern spacing method. Moreover the discontinuation due to method failure increases with increase in duration of use of traditional method. From the programmatic point of view, it will be beneficial to motivate the traditional method users to opt for modern spacing method as traditional method users have the desire to space or limit childbearing. The probability of discontinuation due to method failure was least among IUD users followed by pill and condom. The irregular use of pill might result in method failure. Third, the probability of discontinuation due to side effect was highest for pill followed by IUD and least for condom. This is further confirmed as discontinuation of pill is maximum among high-educated women. The side effects of IUD are serious: ranging from menstrual bleeding, to inter-menstrual pelvic pain, to dysmenorrhea (Farr & Amatya, 1994; Trieman, Liskin, Kols, & Rinehart, 1995), whereas the common complains with the use of pill are breakthrough bleeding, dizziness, headache, lightheadedness, bloating, or nausea (Cushman, 2012; Vlieg, Helmerhorst, Vandenbroucke, Doggen, & Rosendaal, 2009). The long-term use of oral pill is associated with blood coagulation, increased risk of cardio-vascular problems, and chronic immune disorders with an inflammatory component, including cancer (Cushman, 2012). These issues need to be addressed, and better quality of method should be provided. Fourth, women reporting discontinuation of pill and IUD citing reasons such as husband’s opposition, fatalistic, did not like the method, inconvenient to use need counseling. These women are more likely to continue the method if they are provided with good quality services. Fifth, the discontinuation of condom declines with increasing economic status and varies in a small range for pill users and does not show any pattern with respect to IUD (maximum among middle wealth quintile and lowest among richest wealth quintile). This links the affordability as condoms are generally procured from private health centers or chemist. Provisioning of good quality IUDs and condoms at public health center can increase the use and continuation among poorer and poorest section of the society. Sixth, the discontinuation rate declines with age and parity but varies by methods. The younger women used reversible method to space between births and were more likely to discontinue. However, older women can continue the method in long run if good quality of services is provided. Seventh, regional differentials in use of reversible method are large. Among spacing method, although condom and pills are largely used and retained in Northeastern states, the traditional methods are largely used in Eastern regions. It is possibly due to program priority and individual preferences in the population. Efforts for condom promotion were made in Northeastern states to prevent HIV/AIDS both by the government and non-governmental organizations, and similar effort in other states can increase retention of spacing method. Finally, about three fourths of users ended in one episode confirming the overemphasis on female sterilization in family planning program. Majority of women are opting for female sterilization soon after achieving their desired family size. The median age at sterilization in some states of India is below 25 years. From programmatic point of view, women with fewer children and below 25 years of age should be counseled and motivated to use the modern spacing method. The use of modern spacing method for younger women should be seen not only as demographic target but also as an human rights issue.
Based on these findings, we suggest that improving the quality of family planning services, including counseling and follow-up visit in initial few months; monitoring the quality of contraceptive pills and IUDs; and increasing provisioning of IUDs and condoms at public health centers can increase the contraceptive use and reduce the discontinuation of spacing method in India. The sustained use of spacing method protects women from unintended pregnancies, induced abortion, and unwanted births, and promotes birth spacing.
Footnotes
Acknowledgements
The authors would like to thank Dr. N. K. Singh for rendering his technical expertise in decoding calendar data and Mr. Radheshyam Mishra, research scholar at International Institute for Population Sciences, Mumbai, for editorial assistance.
Authors’ Note
This article used secondary data that are available in public domain (unit record of NFHS 3). This does not involve any ethical issues.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.