
Abstract
Despite a growing body of literature, substantial variance remains between researchers, mental health experts, clinicians, and practitioners over the nature, structure, and contents of psychosocial interventions aimed at reducing the mental health burden in war-torn and postconflict societies. We conducted a focused and systematic review of the literature published over the last two decades on the most commonly used psychotherapeutic treatment modalities in medical and humanitarian interventions as represented by expert opinion, observational and qualitative or mixed-method studies, case reports, case control, and community-based studies, excluding randomized controlled trials (RCTs) and meta-analyses of RCTs. More specifically, we aimed at searching for best practices and supporting psychosocial interventions within the domain of adult mental health in civilian populations in low- and middle-income countries affected by protracted political violence, armed conflict, and wars. We noted the need to translate existing knowledge into action (know-do gap) and the critical importance of applying qualitative evidence-based knowledge that informs and supports collective interventions and best practices in medical and humanitarian assistance programs currently being undertaken.
Keywords
Introduction
The aftermath of armed conflicts and wars is a complex and intricate process characterized by reconstruction efforts and reordering of social and political life at all levels. Governments, multi- and bilateral agencies, and civil society organizations play a vital role in conducting interventions as part of medical and humanitarian initiatives. Their actions are largely driven by the premise that not only combatants but entire civilian populations exposed to the adversities of armed conflict and war would require some form of humanitarian assistance, which may include the provision of medical and/or psychosocial services, such as psychotherapeutic counseling, psychological aid, and emotional support (Allden et al., 2009; Almedom & Summerfield, 2004; Bracken & Petty, 1998; Moon, 2009; Pedersen, 2002; Pupavac, 2005; Ritchie, Watson, & Friedman, 2006; Williams, 1998; Wood, 1996; Yehuda, 2002).
The origins of these practices can be traced back to the frontline treatment (also called “forward psychiatry”) provided to combatants by military psychiatrists during World War I, which continued during World War II driven by the principles of proximity (provision of services as close as possible to the frontlines), immediacy (treatment as soon as possible), and expectancy (rapid recovery and expected resumption of normal duties at the frontlines; Friedman, Ritchie, & Watson, 2006). Three decades later, in France, “informal” psychotherapy sessions conducted among Latin American torture victims of military regimes gave birth to what Stanislas Tomkiewicz—a psychiatrist survivor of the concentration camps—described under the name of “humanitarian psychiatry” (Fassin & Rechtman, 2009).
Over the last few decades, the assistance to war victims moved the focus from the battle field to the civilian domain, leading to the establishment of different initiatives and varying responses ranging from “relief operations,” entailing the provision of the “five essentials” (protection/rescue, health, food, water, and shelter) to more elaborate responses designated variously as “recovery,” “rehabilitation,” “post-conflict stabilization,” and “peace-building” operations (Abiew & Keating, 1999; Ballentine & Nitzschke, 2005; Goodhand, Lewer, & Hulme, 1999; Lautze & Raven-Roberts, 2006; White & Cliffe, 2000). Humanitarian assistance aimed at the provision of medical and psychosocial services was gradually adopted, either independently or as part of larger social reconstruction and development undertakings to support peace, justice, social equity, reconciliation, and reversion of the social breakdown experienced as a result of war and mass violence (Brennan & Nandy, 2001; Fletcher & Weinstein, 2002; Ritchie et al., 2006; Smillie, 1998).
In the post–Cold War era, confronted by the emergence of a different kind of armed conflicts and “new” wars (Kaldor, 2001), a variety of humanitarian experiments were conducted by the so-called “new humanitarians” (Weiss, 2012). According to T. G. Weiss (2012), these new wars had four differential features with the conventional wars of the past: first, the locus of war was no longer confined to a territory with state borders; second, nonstate, nonmilitary actors played an increasing important role (i.e., war lords); third, the economies of war were no longer supported by government funding, but by illicit activities (i.e., drug trafficking, organized crime syndicates, etc.); and fourth, the death toll was made up of increasing number of civilians as opposed to military personnel.
In response to these wars, military interventions were often conducted against governmental wishes or without explicit or meaningful consent. These interventions were carried on the grounds of humanitarian principles with the purpose of preventing massive loss of life, genocide and mass atrocities, and widespread abuses of human rights. The term of “humanitarian interventions” was coined and adopted in this particular sense, ranging across peace enforcement, coercive protection of civilians, and war fighting (Kienzler & Pedersen, 2012; Weiss, 2012; Wood, 1996). At the same time, the need for humanitarian assistance grew exponentially and new actors—represented not only by UN agencies but also by governmental agencies and international nongovernmental organizations (NGOs)—sprang up with each crisis. Funding for humanitarian assistance grew from about US$4.4 billion in 1999 to an estimated US$15.1 billion in 2009 (Weiss, 2012). In 2013, the international community responded to the dramatic escalation of needs with a record US$22 billion in funding. This was a significant increase from the 2 previous years—and over US$2.5 billion more than the previous peak of US$19.4 billion in 2010, the year of the Haiti earthquake and the Pakistani floods (Global Humanitarian Assistance Report [GHA], 2014). The proliferation of agencies, actors, and funds brought along the need for establishing norms and treatment practices, as well as setting minimum standards for emergency response.
Humanitarian assistance assumed a new identity no longer aimed to be palliative and politically neutral, but rather actively contributing to address structural problems and improve the quality of life including, whenever possible, to consolidate the peace process (Calhoun, 2010). While the provision of food and control of communicable diseases were the main focus of humanitarian assistance programs until the early 1990s, psychological trauma and the mental health consequences of human rights abuses gradually reemerged as a more salient feature and have since received increasing attention as an area deserving effective collective interventions (Barudy, 1989; Kienzler & Pedersen, 2012). As a direct consequence of this shift in both aims and composition of humanitarian assistance, a wide range of interventions addressing mental health and psychosocial needs became the focus of attention of many Western-based experts, social scientists, and health professionals (Bolton, Tol, & Bass, 2009; Crumlish & O’Rourke, 2010; Good, DelVecchio, Abramowitz, Kleinman, & Panter-Brick, 2014; Hobfoll et al., 2007; Inter-Agency Standing Committee [IASC], 2007; Meffert & Ekblad, 2013; Shalev, 2002; Silove, 2004; Silove & Steel, 2006; Somasundaram, 2014; Tol, Barbui, et al., 2011; M. Weiss, Saraceno, Saxena, & van Ommeren, 2003; World Health Organization [WHO], 2013). That is, besides the provision of basic health care, humanitarian initiatives increasingly included psychological or psychiatric aid and emotional support, and offered information, sympathetic reassurance, and fostering of resilience and social cohesion in recognition of core mental health and psychosocial needs of the affected populations. Interestingly, there remains substantial variance between researchers, mental health experts, first responders, clinicians, and practitioners over the nature, structure, and contents of psychosocial interventions aimed at reducing the mental health burden and suffering in war-torn and postconflict societies. Moreover, it has been argued that despite the many treatment options available, there is an overall lack of evidence for most psychosocial interventions currently being implemented (Allden et al., 2009; Tol, Barbui, et al., 2011).
To gain insight into this dynamic field broadly defined as “psychosocial” and assess the qualitative evidence of the most commonly used treatment modalities in collective interventions aimed at civilian populations affected by armed conflicts and wars, we conducted a focused and systematic review of the literature. The review and related discussion was driven by the following questions: (a) What are the existing paradigms supporting psychosocial interventions in medical and humanitarian initiatives aimed at reducing the mental health burden of civilian populations in conflict and postconflict settings? (b) What are the main implementation gaps in the delivery of medical and psychosocial interventions? On what kind of evidence are practices currently based? (c) In light of the above, which are considered best practices in individual and collective interventions aimed at civilian populations exposed to armed conflict and war? The overall aim of the review and critical appraisal was to inform readers and stakeholders of the assortment and range of psychosocial and/or collective interventions aimed at civilian populations, more specifically adults, exposed to armed conflict and wars in low- and middle-income countries (LMICs).
A Short Genealogy of Psychosocial Interventions
As pointed above, the “psychosocial” construct in humanitarian aid endeavors emerged toward the end of the 1900s, as an area of inquiry and practice combining both the psychological and social domains aimed at the modification of risk factors and/or behaviors conducive to disease onset or recurrence resulting from exposure to extreme adversities, such as war or natural disasters. Since then, these practices have undergone multiple and successive changes and adaptations in its recent history (Glass, 2000; Reyes, 2006). According to Glass (2000), “psychosocial” has been conceptualized as one’s psychological development within, and in dynamic interaction with, a given social environment and implies the intimate connections existing between our social and our psychological and biological existence. In conflict and postconflict settings, the attention of psychosocial advocates is, therefore, focused on the stressful social and material conditions such as poverty and destitution, food insecurity, social conflicts within the community, and erosion of the social fabric, including the marginalization and struggle of particular groups such as former child soldiers, raped and sexually abused survivors, refugees, widows and the elderly, and people with disabilities (Miller & Rasmussen, 2010).
As these conditions are believed to cause and exacerbate distress and social suffering, interventions are designed with the aim to alter the social context and its inherent inequities. Psychosocial interventions are implemented at the level of the individual, the family, the social network, the community, and/or at the wider population to improve health and mental health outcomes (International Federation of Red Cross and Red Crescent Societies [IFRC], 2009; Reyes, 2006). For nonconflict settings, five broad types of psychosocial interventions have been identified focusing on behavioral change, social support, disease management, distress mitigation, and control/efficacy enhancement (Glass, 2000). A review of the currently employed extended mental health and psychosocial support practices in humanitarian settings shows that the most commonly used interventions are counseling, providing and facilitating community-based social supports, structured social activities, provision of information, raising awareness, and psychoeducation (Tol, Barbui, et al., 2011).
For the purpose of this article, we have adopted the term “psychosocial intervention” to refer to activities designed as collective interventions variously labeled as “counseling,” “psychoeducational,” and/or “psychotherapeutic.” These interventions are aimed toward primary and/or secondary prevention, as well as exerting positive influence to the course and outcome of distress and illness, including the promotion of resilience and effective coping with major individual challenges and social adversities. Such psychosocial interventions ultimately aim at the resumption of normal life, facilitating affected people’s convalescence and preventing pathological consequences of potentially traumatic or stressful situations threatening the integrity of the lives of individuals, families, and communities. Mollica and colleagues (2004) argue that while psychosocial interventions are primarily concerned with the psychological and social well-being of individuals, they go beyond to include the repair of collective social structures. In other words, the term psychosocial implies the dynamic relations between psychological effects (e.g., emotions, behaviors, and memory) and social effects (e.g., altered social relations as a result of loss, separation, family, and community breakdown; Mollica et al., 2004). However, until now little is known about the evidence base sustaining these interventions, their effectiveness and cultural appropriateness, the planning and implementation processes followed, as well as the ways in which current practices are rendered sustainable to aid the development of long-term restructuring of mental health systems in unstable or turbulent states.
Methodology: Search Strategy and Selection Criteria
We decided to search the scientific literature published over the last two decades. In view of previously published meta-analyses and systematic reviews of randomized controlled trials (RCTs) on the evidence base of mental health interventions in war and postwar contexts (McPherson, 2012; Meffert & Ekblad, 2013; Steel et al., 2009; Tol, Barbui, et al., 2011), we decided to avoid duplication of efforts by excluding all RCTs and systematic reviews of RCTs and meta-analyses from our review. Instead, we concentrated our search of the literature on the middle and lower grades of evidence, as represented by expert opinion, observational and qualitative or mixed-method studies, case reports, case control, and community-based studies. We decided to sharpen our focus even further on the most commonly used treatment modalities in psychosocial interventions among civilian populations, because of the reported overall scarcity of studies on psychosocial support and best practices in humanitarian settings and the exclusion of “psychosocial wellbeing” as an outcome in the systematic reviews and meta-analyses already published (Patel et al., 2007; Tol, Barbui, et al., 2011).
Another issue shaping our review is the tendency of systematic reviews of RCTs to reflect clinicians’ perspectives rather than patients’ needs and community priorities for care. In reviewing qualitative, observational, and community-based studies, we aimed to restore patients’ and community views and priorities—as far as they were reported in the literature reviewed—thus broadening our critical perspective to existing systematic reviews (Berkwits, 1998).
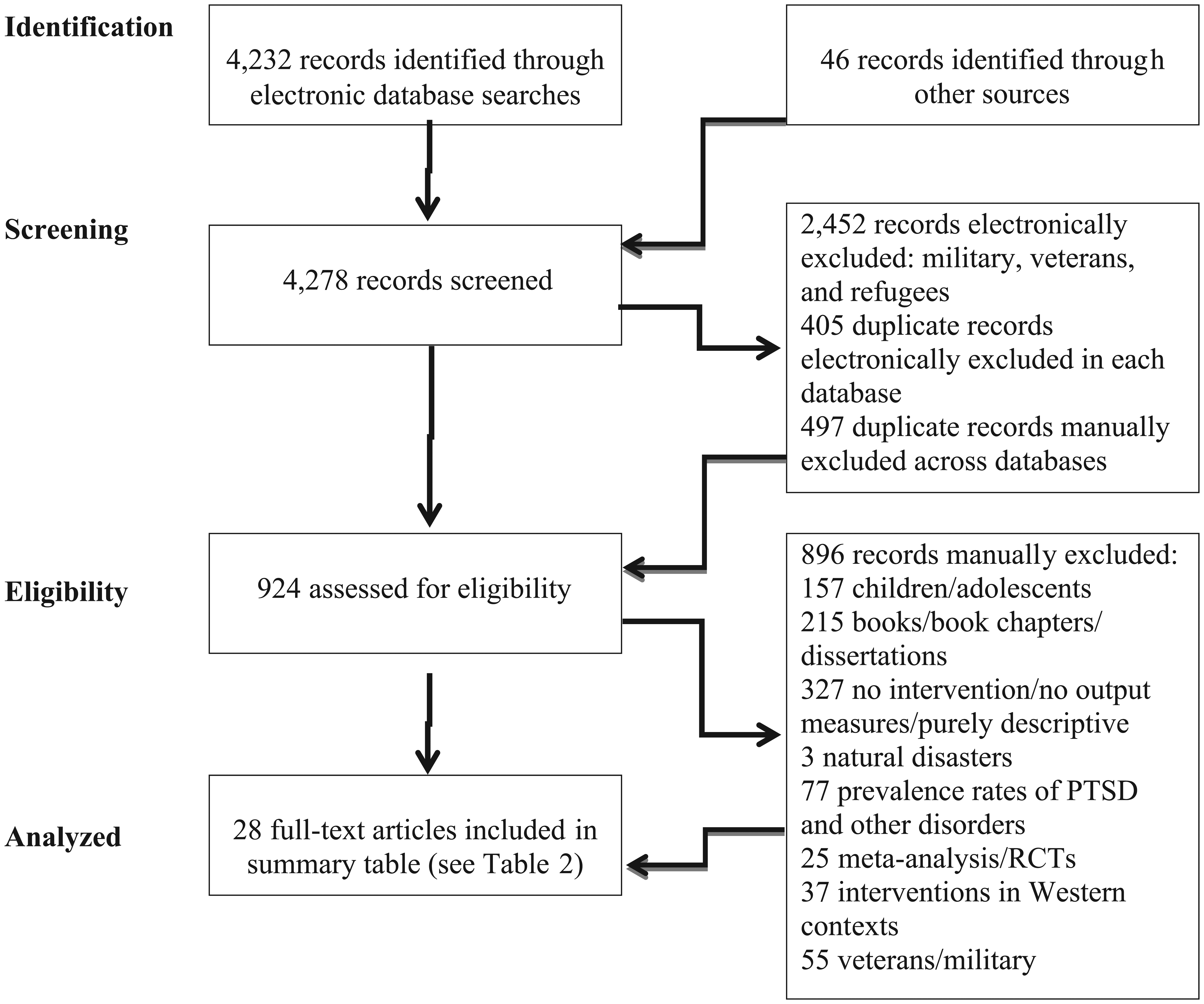
To gain insight into these particularities, we systematically searched for references listed in the following electronic databases: PsycINFO, Medline, Embase, and PubMed. For the search to be both sensitive and specific in relation to our questions, we used the keywords: war AND mental health AND trauma. Then, we combined these keywords variously with the search terms: treatment OR mental health interventions OR psychotherapy OR psychosocial OR posttraumatic stress disorder OR group therapy. Each search was, in turn, delimitated by the following criteria: (a) the search period encompassed nearly two decades, from January 1994 to October 2013, and (b) only articles written in English were included. This search identified a total of 4,232 articles (see Table 1).
Electronic Database Searches and Screening.

In addition, we searched the following journals: American Journal of Public Health; British Journal of Psychiatry; British Medical Journal; Disasters; Intervention: International Journal of Mental Health, Psychological Work and Counseling in Areas of Armed Conflict; Journal of Nervous and Mental Disease; Medicine, Conflict and Survival; Social Science & Medicine; The Lancet; Journal of Traumatic Stress; and Transcultural Psychiatry. We also searched the reference lists of particular journal articles. This manual search resulted in 46 additional articles.
As a result, a total of 4,278 articles were screened through a staged process. First, each electronic search was repeated to remove duplicates and exclude articles that contained the key words—“military,” “veterans,” and “refugees”—to focus the review on studies conducted in LMICs where most of the wars are currently raging and limit our search to adult civilian populations. Additional reasons for excluding the above-mentioned vulnerable populations were that (a) there already exist a number of systematic literature reviews focusing on mental health and psychosocial interventions directed at military service personnel (i.e., Carlson et al., 2011; Institute of Medicine [IOM], 2008), refugees (i.e., Crumlish & O’Rourke, 2010; Palic & Elklit, 2011), and children and adolescents (i.e., Jordans, Tol, Komproe, & de Jong, 2009; Tol et al., 2010; Tol, Barbui, et al., 2011), and (b) intervention strategies directed at these groups often follow particular designs that are not easily comparable with those devised for adult civilian survivors of armed conflict who recover in their respective communities (American Psychology Association [APA], 2010; Hautzinger & Scandlyn, 2013; Onyut et al., 2005).
The number of records thus excluded was 2,862, leaving us with 1,375 plus the 46 manually selected ones, totaling to 1,421 records. Second, to remove duplicate records across databases (this could not be done electronically), we screened the search results manually and were able to exclude another 497. The total number of excluded articles (electronic and manual) amounted to 3,354 (see Figure 1).
Studies included in the focused and systematic review.
A total of 924 records were then manually assessed for eligibility. In this process, we excluded all books, book chapters, and dissertations (n = 215); studies conducted among veterans and military that had slipped through the electronic screening (n = 55); studies on interventions conducted among children and/or adolescents (they are currently under review and will be published separately; n = 157); works reporting on interventions in Western contexts (n = 37); meta-analyses and RCTs conducted in Western and non-Western contexts (n = 25); and epidemiological surveys reporting only on prevalence rates of posttraumatic stress disorder (PTSD) and other disorders (n = 77). We further excluded studies that were irrelevant for our review (i.e., natural disasters; n = 3), and those that did not report on any type of intervention did not provide output measures or were purely descriptive, conceptual, or theoretical (n = 215). We retained 28 full-text peer-reviewed articles describing individual or community-based psychosocial interventions directed at adult populations in war and postwar contexts.
The procedure for data collection consisted of two consecutive rounds of independent readings conducted by the authors. After the first round, we extracted basic information for each study: source (journal/impact factor, author/s); target group and country; study design and research tools (case control study, community-based intervention, pharmacotherapy, trauma healing workshop, etc.); type of intervention (two main categories: trauma-focused interventions and broader psychosocial and community-based mental health interventions) and treatment protocol adopted (i.e., nature, content, frequency of sessions); follow-up and assessment of outcomes; and main results. The classification adopted under main results, expressed as beneficial or improved status, inconclusive and/or negative, and/or general recommendations, is arbitrary and derived from the concluding remarks or assessment made by the author/s. For example, if the majority of treated cases were reported as an improvement or as a symptom’s relief, then the results were listed as beneficial. Conversely, if the authors of a case control study reported that “no intervention effect was found,” then the results were listed as inconclusive.
As the process of independent readings was completed by the two readers (main author and first coauthor), we compared notes to ensure reliability of the data collected among researchers reading the same material. Any discrepancies in the data collected and summarized were discussed, and if needed, the opinion of the third author was requested to gain consensus and conciliate the interpretation of results. These results were then organized according to categories generated from the collected material, along themes (i.e., qualitative and quantitative research tools, individual and group therapies used, ad hoc therapies, traditional healing and coping practices, etc.) and main results (i.e., beneficial, inconclusive, recommendations, etc.).
During the second round of readings, we performed an in-depth selective reading and critical appraisal of the study design, sample size, content of the intervention, provisions for follow-up, and mental health outcomes, trying to find supportive evidence and linkages between specific therapies and reported results. We also included in our review quantitative results, perceived barriers to treatment, and patients’ self-assessment, if any. These results were then analyzed, and after data reduction and interpretation, we transfer it to a data-recording matrix, which is now presented as a summary in Table 2.
Summary Table Displaying the Results of the Literature Review on Medical and Psychosocial Interventions (Adults).

Note. NA = not available; HSCL-25 = Hopkins Symptom Checklist–25; SCL-90-R = Symptom Checklist–90–Revised; WHODAS-II = WHO Disability Assessment Scale–II; PSC = problem-solving counseling; IES = Impact of Event Scale; TFT = thought field therapy; HNI = HealthNet International; HTQ = Harvard Trauma Questionnaire; MINI = Mini International Neuropsychiatric Interview; BDI = Beck Depression Inventory; PDS = Posttraumatic Diagnostic Scale; BSI = Brief Symptom Inventory; PWBS = Psychological Well-Being Scale; MANSA = Manchester Short Assessment of Quality of Life; CBT = cognitive-behavioral therapy; PTSD = posttraumatic stress disorder; PPP = public–private partnership; SRQ-20 = Self-Reporting Questionnaire; LMICs = low- and middle-income countries; NET = narrative exposure therapy; TC = trauma counseling; MG = monitoring group; IES-R = Impact of Event Scale–Revised; EMDR = eye movement desensitization and reprocessing; PHC: primary health care; TPO = transcultural psychosocial organization; NGO = nongovernmental organization; WHO = World Health Organization; IDP = internally displaced population; APAI = Acholi Psychosocial Assessment Instrument; CVT = Center for Victims of Torture; EUROHIS = European Quality of Life scale; GHQ-28 = General Health Questionnaire-28; MSF = Médicins Sans Frontières; CAPS = Clinician Administered PTSD Scale for Diagnostic and Statistical Manual of Mental Disorders-IV; ART = antiretroviral therapy.
Results of the Literature Review
The literature review shows a wide range of intervention initiatives at the individual and collective level, ranging from clinical and observational studies to community-based interventions, quasi-experimental case and control studies, and descriptive studies outlining “real-life” interventions. The countries in which these interventions were performed are equally as diverse, including Algeria, Angola, Bosnia and Herzegovina, Burma, Cambodia, Congo, Croatia, Gaza and the West Bank, Guatemala, Guinea, India, Indonesia, Iraq, Israel, Kosovo, Liberia, Mozambique, Nepal, Rwanda, Sierra Leone, Tanzania, Thailand, Uganda, and Zimbabwe.
In Table 2, we provide detailed summary information with regard to the literature reviewed focusing on sources (author/s and year of publication), target group and country, study design and research tools, type of intervention, follow-up and assessment of results/outcomes, and main results and/or general recommendations.
The systematic review makes apparent that the study designs are extremely diverse. The research tools used range from validated clinical or screening questionnaires and scales (i.e., Beck Depression Inventory [BDI], Hopkins Symptom Checklist [HSCL], and Mini International Neuropsychiatric Interview [MINI]) to focus group discussions and semistructured and open-ended interviews accordingly. The number of community-based, observational and qualitative or mixed-method studies (20) prevailed over quasi-experimental, case and control study designs (8).
The literature review reveals a wide repertoire of interventions, including therapies used, ranging from various forms of psychotherapy and psychosocial counseling (Bass et al., 2012; K. de Jong & Kleber, 2007; Dybdahl & Pasagic, 2000; Gaboulaud et al., 2010; Kozaric-Kovacic, Kocijan-Hercigonja, & Jambrosic, 2002; Mooren, de Jong, Kleber, & Ruvic, 2003) to cognitive-behavioral therapy (CBT; Morina, Rushiti, Salihu, & Ford, 2010), Internet-based CBT (Wagner, Schulz, & Knaevelsrud, 2012), narrative exposure therapy (NET; Neuner et al., 2008), psychosocial support (Kozaric-Kovacic et al., 2002), psychological support and assistance during exhumations (Eppel, 2002), sociotherapy (Richters, Dekker, & Scholte, 2008; Scholte et al., 2011), testimony methods (Igreja, Kleijn, Schreuder, van Dijk, & Verschuur, 2004), psychopharmacological agents and counseling (Nakimuli-Mpungu et al., 2013; Somasundaram, van de Put, Eisenbruch, & de Jong, 1999), community-based mental health services and psychosocial interventions (Agani, Landau, & Agani, 2010; Anckermann et al., 2005; Johnson, Shala, Sejdijaj, Odell, & Dabishevci, 2001; Mooren et al., 2003; Somasundaram et al., 1999; Sonderegger, Rombouts, Ocen, & McKeever, 2011; Walstrom et al., 2013), and mixed Western and/or traditional healing practices (Eppel, 2002; Mercer, Ager, & Ruwanpura, 2005; Somasundaram et al., 1999; Stark, 2006; Stepakoff, Hubbard, & Katoh, 2006). While the review shows a gamut of collective interventions employed worldwide, it also reveals discrepancies between different authors regarding treatment goals and best practices to deal with trauma-related emotional distress and mental disorders. In fact, considering the extreme diversity of treatment approaches used, it seems that we are far from reaching consensus to date regarding effective psychosocial interventions in the early and/or late phases of exposure to traumatic experiences. Our findings are supported by other literature reviews that have pointed to the fact that there exists substantial variance among researchers, mental health experts, first responders, clinicians, and practitioners over the best practices and an overall lack of evidence for interventions aimed at reducing the mental health burden in war-torn and postwar societies (Allden et al., 2009; Gersons & Olff, 2005; Hobfoll et al., 2007; Miller & Rasmussen, 2010; Patel et al., 2007; Tol, Barbui, et al., 2011).
According to the type of intervention, it is worth noting trauma-focused interventions are a clear minority (Fuertes, 2004; Mooren et al., 2003), which leaves most interventions listed above addressing broader psychosocial and community-based mental health issues. These can be grouped as follows: About half of all interventions consist of psychosocial support, counseling, and psychoeducation, including CBT and NET, applied as therapies to groups and/or individuals (13). Smaller numbers are represented by ethno-cultural approaches, using traditional healing and coping practices either alone or mixed up with Western treatment practices (5), such as exhumations and reburials as catalysts for healing and reconciliation (Eppel, 2002), Tibetan and Western-based clinical consultations (Mercer et al., 2005), treatment model blending Western psychodynamic therapy with African practices in Liberia and Sierra Leone (Stepakoff et al., 2006), relaxation techniques and referral to traditional healers (Somasundaram et al., 1999), and cleansing rituals among rape victims (Stark, 2006). Finally, ad hoc interventions were reported (5): thought field therapy (TFT; Johnson et al., 2001), sociotherapy (Richters et al., 2008; Scholte et al., 2011), Internet-based CBT (Wagner et al., 2012), and case study (Keough & Samuels, 2004), followed by community-based self-help and reflection groups (Anckermann et al., 2005), promotion of community resilience (Agani et al., 2010), and social work assistance (Doucet & Denov, 2012); and only two listed as combined psychotherapy plus pharmacological treatment (Nakimuli-Mpungu et al., 2013; Somasundaram et al., 1999).
Irrespective of the type of intervention, 20 of them show results of follow-up studies, though the majority are immediate or short-term assessments following the intervention. Longitudinal, long-term assessments of mental health outcomes, and overall impact in the quality of life and well-being of survivors and/or intended beneficiaries are by in large missing. The absence of longitudinal data impoverishes further the reporting of results of the clinical encounter or intended intervention. Nevertheless, the majority of the studies (18) show beneficial or improved outcomes of the intervention, or were at least able to transform results into general recommendations. A smaller number (10) of all reviewed studies reported inconclusive results. We believe that the claimed results need to be taken with caution as most studies included in our review have no control groups and, therefore, the evidence shown is potentially weak and fails to demonstrate that the treatments chosen for the various conditions are more (or less) effective than natural recovery. It should be further acknowledged that in spite of the reported results, we are still lacking clinical evidence from the literature reviewed about (a) who should (or should not) receive specialized treatment when confronted with psychological trauma; (b) what kind of intervention is best to be prescribed and what should be the optimal duration of treatment; and finally (c) how and why a clinical intervention may work in some cases and not in others (Mollica et al., 2004; Shalev, 2002; Yehuda & Hyman, 2005).
Another finding of the review is that there seems to be a tacit agreement among the reviewed authors about the importance of designing psychosocial interventions and evaluation strategies in culturally appropriate ways to serve conflict-affected populations effectively. However, a closer look reveals that cultural adaptation is carried out and described to varying degrees. Six studies outline psychosocial interventions that were developed from the ground up by local experts or the involvement of religious leaders, traditional healers, and the wider community (Anckermann et al., 2005; Doucet & Denov, 2012; Eppel, 2002; Mercer et al., 2005; Stark, 2006; Stepakoff et al., 2006). The resulting intervention strategies are described as differing significantly from strategies developed in Western settings as they are shaped by specific belief and value structures, supported by local resources, and embedded into the available, albeit limited, infrastructure. For instance, Doucet and Denov (2012) delineate particular strategies with which social workers in Sierra Leone supported war-affected women and girls and highlight the importance to advocate for supporting local capacities, as well as the inclusion of local helpers in internationally-funded programs, which will not only benefit war-affected individuals, but also will help rebuild the social capital networks that may have been damaged by the conflict. (pp. 623-624).
Another example is the use of symbolic cleansing rituals for spiritual pollution (“noro”), and ceremonial gestures of reconciliation, resulting in significant improvement of mental health status, as perceived by elimination of symptoms, improved emotions and stigma reduction among girls exposed to atrocities of war, and sexual abuse and rape in Sierra Leone (Stark, 2006).
Five of the reviewed studies thoroughly describe culturally informed approaches to treatment by outlining how Western approaches to care were modified through the inclusion of local resources; values, beliefs, and rituals; and mediation and relaxation techniques (Agani et al., 2010; Doucet & Denov, 2012; Mercer et al., 2005; Somasundaram et al., 1999; Stark, 2006). However, the majority of studies (14) only claim to have adapted their intervention strategies in culturally informed ways without providing any further information. Typical statements are as follows: “The psychodynamic approach of trauma . . . was adapted by experts in trans-cultural psychiatry to the Palestinian culture” (Gaboulaud et al., 2010, p. 132); “During the training both trauma experts and participants adapted intervention techniques to the local culture” (K. de Jong, Kleber, & Puratic, 2003, p. 20); and “The programme combined an evidence based CBT framework, in conjunction with culturally sensitive and culturally relevant knowledge and activities” (Sonderegger et al., 2011, p. 241). None of these studies further explain what cultural adaptation entails, how it can be achieved, and what the benefits or challenges of such an approach are. Last, four studies make no reference to culture or social adaptations (Igreja et al., 2004; Morina et al., 2010; Priebe et al., 2010; Walstrom et al., 2013) and, out of these, two critically reflect on this as an omission. Igreja and colleagues (2004) note, The standardized way in which the participants were expected to give their answers proved to be problematic . . . [and] it was very difficult to find meaningful words or phrases in the local language for several other concepts related to “affect,” “remembering,” “hearing” and “thinking.” (p. 256)
On the contrary, Morina et al. (2010) reflect that to achieve better treatment results, it would have been important to adapt evidence-based treatment for survivors of war “based on their culture and life circumstances in order to recover from PTSD and experience general emotional relief” (p. 79).
Finally, it is interesting to note that not a single study included in this review has acknowledged the various international best-practice guidelines currently available. In part, this may be due to the fact that about half (13 out of 28) of the studies were conducted before international guidelines were made widely available. However, as early as 2000, the Red Cross World Disaster Report sharply criticized international mental health initiatives and issued a call for standards to better structure relief and humanitarian efforts (IFRC, 2000). Since then, a growing number of international guidelines have been launched, such as the recently published Building Back Better report (WHO, 2013), the IASC (2007) guidelines, the Sphere Project (2004), the WHO (2003) report on Mental Health in Emergencies, the National Institute of Mental Health (NIMH; 2002) report on Mental Health and Mass Violence, and the Guidelines for International Training in mental health and psychosocial interventions (Weine et al., 2002). All guidelines have specifically included agreed upon recommendations for the provision of psychological “first aid” and mental health care as part of humanitarian assistance efforts (Kienzler & Pedersen, 2012).
Notwithstanding attempts to find the middle ground and set up standards for minimum psychosocial interventions, health care providers and frontline practitioners still criticize the application of such standardized interventions, and their effectiveness continues to be contested based on the arguments that they reflect both the experts’ opinions and the general common sense, but most often the recommended interventions are insufficiently tested in real-field situations and little evidence of effectiveness or fitness-for-purpose exists (Gaboulaud et al., 2010; Litz, Gray, Bryant, & Adler, 2002; Lopes Cardoso, 2008; Rose, Bisson, & Wessely, 2003; Sensky, 2003).
Discussion
The consequences of exposure to intentional violence such as armed conflict and war are compounded by multiple factors. Researchers and practitioners remain divided along a continuum as to the psychopathological effects attributable to the traumatic experience. While some tend to minimize the psychological needs of individuals exposed to traumatic experiences, others assume all of the exposed, including victims and survivors, are in need of psychosocial assistance, including treatment and rehabilitation services. Depending on the particular outlook, the planning and delivery of psychosocial interventions are therefore differently organized as well as the nature and content of the interventions remain strongly influenced by the context and an array of individual and collective factors, including resources available and funding sources. Furthermore, as explained in the “Introduction” section, the delivery of mental health and psychosocial support is today no longer solely in the hands of governmental or multilateral agencies. Instead, NGOs, the private sector, religious-driven relief and advocacy organizations, and, more recently, the military and security companies are gradually assuming a pivotal role in conducting psychosocial interventions at various levels, under the label of humanitarian assistance (Joachim & Schneiker, 2012; Kienzler & Pedersen, 2012). These agencies and their actors, which are mostly based in high-income countries, usually promote off-the-shelf Western-based therapeutic intervention strategies, which are seldom properly adapted to the needs and expectations of potential recipients and beneficiaries, which in turn come from a highly diverse social and cultural range of LMICs and war-torn societies worldwide (Belgrad & Namias, 1997; Bracken & Petty, 1998; Locke, 2012; Tol, Patel, et al., 2011; Weiss et al., 2003).
Given these complexities, we decided to address some of these issues by organizing our discussion under the three sets of questions guiding our focused and systematic review of the literature, as postulated in the “Introduction” section to this article.
1. What are the existing paradigms supporting psychosocial interventions in medical and humanitarian initiatives aimed at reducing the mental health burden of civilian populations in conflict and postconflict settings?
Despite the apparent consensus regarding the need for evidence-based psychosocial interventions in conflict and postconflict situations, our literature review reveals the coexistence of competing paradigms among scholars and practitioners, unveiling a multiplicity of approaches with respect to individual and collective best practices in planning, conducting, and evaluating psychosocial interventions. There are those who seem to favor a narrower application, so-called “trauma-focused intervention,” addressing distress and trauma primarily within medical or psychological paradigms targeting individuals with protocols for screening, diagnosis, and treatment (Bass et al., 2012; de Jong & Kleber, 2007; Dybdahl & Pasagic, 2000; Igreja et al., 2004; Johnson et al., 2001; Wagner et al., 2012). Yet, others advocate the application of wider, more comprehensive psychosocial approaches, targeting communities and, at times, individuals at risk, adopting a “bricolage” of different therapeutic and psychosocial paradigms (Anckermann et al., 2005; de Jong & van Ommeren, 2002; Doucet & Denov, 2012; Eppel, 2002; Mercer et al., 2005; Somasundaram et al., 1999; Stark, 2006).
Miller and Rasmussen (2010) postulate that fundamentally different assumptions underlie these two main approaches: For trauma-focused advocates, the critical factor involved in the causality chain is the single and direct exposure to a traumatic event, a belief which in turn is fueled by the growing clinical field of psychotraumatology. In contrast, for those grouped as supportive of a wider psychosocial approach, the attribution of causality focuses primarily on the overall stressful social and material conditions caused or worsened by armed conflict and war, including other prior or coexisting conditions such as extreme poverty, poor housing, and food insecurity, and/or those derived from internal displacement and refugee status often resulting in stigmatization, social exclusion, and partial or total loss of social and material support.
Inspired by the Cambodian survivors of the Pol Pot period (1975-1979), Hinton and Good (2015a) have postulated what may be seen as a new paradigm or theoretical framework combining three analytic approaches: (a) a multiaxial approach (with 11 analytic perspectives ranging from biology to the nature of trauma to the social context), (b) a “typology of errors” that should be avoided to evaluate trauma in a culturally sensitive fashion, and (c) the “multiplex models” to show how trauma symptoms are generated through biocultural mechanisms, and how trauma results in episodes of distress. These may be seen as useful tools in examining trauma-related disorders across different cultures, where local trauma ontologies may be delineated and the cross-cultural study of these ontologies advanced (Hinton & Good, 2015b). Through these three analytic approaches, the researcher thus becomes aware of key processes to target in psychosocial interventions that seek to alleviate distress and build resilience of individuals and communities affected by conflict and war.
Going back to our discussion on “Results of the Literature Review” section, we are not implying that diverse—and at times competing paradigms—as well as the emerging multiplicity of approaches followed by the different authors included in this review are necessarily counterproductive, but this variability may simply reflect, on one hand, the different disciplinary backgrounds of public health experts, researchers, and practitioners involved and, on the other, the need to adapt and accommodate the intervention to the multidimensional approaches discussed above and the ever-changing contexts, the variable socioeconomic position of survivors, the polymorphic cultural expression of symptoms of distress, and the heterogeneity of trauma-related disorders (Young & Breslau, 2015), all of which defy or interfere with efforts for standardization of clinical diagnostic tools and therapeutic protocols.
2. What are the main implementation gaps in the delivery of medical and psychosocial interventions? On what kind of evidence are practices currently based?
Through our systematic review, we discerned at least four main implementation gaps:
First, the effective delivery of medical and psychosocial interventions imply the timely identification of cases (case finding) and the provision of services to people identified as positives (true cases), who are at greatest need for conditions or disorders for which proven therapies exist. In most psychosocial interventions conducted in humanitarian settings, including the ones under review, “active” case finding is rare, but cases are usually identified by symptom checklists applied to persons demanding services at the point of delivery. The screening of symptoms or triage does not necessarily make up for a diagnosis, and therefore an unknown number of “false positives” may be misdiagnosed and prescribed a superfluous or unnecessary treatment. As explained above, we are still lacking enough evidence as to who should (or should not) receive specialized treatment when confronted with massive psychological trauma (Shalev, 2002; 2007).
It has been further acknowledged the lack of evidence on the efficacy of most psychotherapeutic modalities applied in humanitarian settings (Lopes Cardoso, 2008; Patel et al., 2007; Roberts, Kitchiner, Kenardy, & Bisson, 2009), including the inefficatious, but also potentially harmful, critical incident stress debriefing (Litz & Gibson, 2006; Litz et al., 2002; Watson et al., 2003). Practitioners in the field of humanitarian assistance largely agree that despite the plethora of available treatment options, there remains an absence of a solid evidence base for most mental health and psychosocial support interventions (Allden et al., 2009). A similar claim was raised by the IOM, in their report following a systematic review of the scientific evidence on treatment modalities for PTSD among war veterans. The IOM report states that for all drug classes and specific drugs reviewed in each of the classes, the evidence is inadequate to determine efficacy in the treatment of PTSD among war veterans. With regard to psychotherapies, the report states that only for exposure therapies (i.e., CBT), there is sufficient evidence to conclude its efficacy in the treatment of PTSD (IOM, 2008).
Despite these assertions, most interventions included in this focused and systematic review have used one or other form of psychotherapeutic treatment protocol. Most of these interventions claim to have had beneficial or improved outcomes—expressed as symptom reduction—more often than failure. This may be explained by the fact that absence of evidence for a given treatment does not necessarily mean it is inefficacious. However, the qualification of beneficial has been most often made with a before and after design for which the reliability of the measures used for symptom reduction is likely to be low (Type II error), and in most cases of such exposure to extreme traumatic experiences, the remission of symptoms may be a long and often unattainable treatment goal (Marshall, Davidson, & Yehuda, 1998; Shalev, 2002).
In addition, people surviving exposure to armed conflict and war are expected to experience at least one, if not more than one, morbid condition, and for many, comorbidity is the norm. In stark contrast, the trauma-focused interventions reviewed here are aimed to deal with single morbid conditions and tend to separate mental and physical health care, disregarding the principle of providing integrated care for both aspects of collective health (Gunn, 2015).
Second, it is also noteworthy that in most of the reviewed studies, neither early detection nor early interventions were conducted, and with a few exceptions, we could find no references to the timeline between the initial assessment, the actual intervention, and the claimed postintervention response. As stated above in the presentation of results, we are still unsure as to what kind of intervention is best and what should be the optimal duration of treatment, as well as how and why a clinical intervention seems to work in some cases and not in others (Shalev, 2002; Yehuda & Hyman, 2005).
In spite of the various forms of individual therapy available (whether proven effective or not), most reported interventions outlined the provision of psychotherapy, trauma counseling, or general psychological support, with little attempts to measure or systematically validate treatment outcomes. For the most part, therapeutic aims remained ambiguous, as some focused on distress mitigation and others focused on management of trauma-related disorders or symptom relief and reduction, as measured by self-reports or symptom checklists or improved daily functioning. In the review, we still remain uncertain of the mutative factors that lead to positive outcomes in some cases, but not in others.
While it is possible that the mental health burden in the early phase of conflict or postconflict might be partly reduced by medication and brief exposure therapy, in the case of protracted violence and enduring social disruption, such focused interventions are bound to have limited impact. Moreover, the preventive efficacy of debriefing in trauma-related disorders has not yet been clearly demonstrated (Bisson, 2003; Rose et al., 2003). While most reported individual or group interventions consisted of periodic (i.e., weekly) sessions, thus avoiding an abbreviated course, eight psychosocial interventions did not specify the number of sessions conducted during the implementation phase.
In addition, while most interventions were described as psychosocial or used psychodynamic principles (counseling, CBT, NET, etc.), only two studies (Nakimuli-Mpungu et al., 2013; Somasundaram et al., 1999) reported having used psychotropic medications in conducting their clinical intervention, in combination with other therapies, with beneficial results on the first study, but inconclusive on the second. Typically, most reviewed interventions were cross-sectional, with no provisions made for medium- or long-term follow-up, which severely limits the understanding of long-term effects of exposure to violence and the process of natural recovery.
Third, planning and conducting a clinical intervention as part of medical and humanitarian aid cannot be separated from the context, the social and cultural realities of the family and the community. Informed by systemic and wider social agendas, the clinical team should be able to anticipate what may be harmful, neutral, or helpful and preserve the needed therapeutic flexibility. Recovery from acute trauma unfolds within a given context which often includes other severe daily stressors derived from overall insecurity, unresolved grief, and the adversities created by poverty, social exclusion, and the social breakdown, or severe attrition of social support networks (Kirmayer, Guzder, & Rousseau, 2013).
Several of the studies reviewed here reveal that it would be rather simplistic to regard survivors of armed conflict and war as passive repositories of negative psychological experiences and effects. However, the dynamic interaction of endogenous protective factors at play, such as resilience, and their influence in the process of healing, coping, and natural recovery was rarely mentioned, let alone discussed in the literature reviewed.
This lapse or omission may reflect an earlier treatment focus on trauma psychopathology while relatively recent emerging notions on resilience capacity, posttraumatic growth, and positive coping were still little known and were not a part of common practices (Almedom, 2005; Monnier & Hobfoll, 2000; Ruiz-Casares, Guzder, Rousseau, & Kirmayer, 2013; Ungar et al., 2007). A comparative study on bereavement conducted among Chinese and U.S adults concluded that resilience does not necessarily have the same meanings and raised questions whether or not different cultures may learn from each other about coping with traumatic experiences and extreme adversity (Bonanno, Papa, Lalande, Nanping, & Noll, 2005; Hinton, Hinton, Pich, Loeum, & Pollack, 2009). As there may be a link between personality and resilient outcomes, resilient traits may be something “relatively fixed” and therefore not easily taught or transferred to others (Bonanno, 2010), and resilience paradigms such as “mindfulness” may require training and special skills to be effectively transported across cultures and meaning systems.
The promotion of resilience appears to be a clear aim in at least one case study of the literature review. This study was conducted by Agani (University of Pristina) and U.S.-based collaborators, in postwar Kosovo (see Agani et al., 2010). The Linking Human Systems (LINC) Community Resilience Model was grounded in indigenous resources, and family-focused and community-based interventions culturally adapted and modified to the Kosovar situation. The aim of this type of community intervention was to build resilience and empowerment by creating linkages at various levels of the social network, and make it highly participatory, with reduced long-term professional involvement and sustainable over time.
Fourth, there is a persistent gap between the local cultural expressions of distress and the PTSD construct held by Western-based mental health professionals, usually assigned to conduct psychosocial interventions such as the ones under review here. The nosologies of PTSD are problematic when applied across cultures, because emic studies suggest that the Diagnostic and Statistical Manual model of PTSD is not congruent with most trauma-related mental health constructs around the world (Bracken, 1998; Hinton & Good, 2015b; Kienzler, 2008; Pedersen, Tremblay, Errazuriz, & Gamarra, 2008; Rasmussen, Keatley, & Joscelyne, 2014).
Substantial cross-cultural variation appears to exist reflecting diagnostic and symptomatic heterogeneity and no clear coherence on what constitutes symptoms of PTSD across different cultures (Hinton & Good, 2015b). Rasmussen et al. (2014) found clusters of trauma symptoms cannot be distinguished by trauma versus chronic stress and loss, and that while avoidance is conceptualized as psychopathology in the PTSD symptom list, it has no discriminant validity linking it with impairment and may operate positively as a coping mechanism post trauma or a culturally reinforced defense strategy. The multiple sociocultural levels involved in this process may indeed inform and shape the fluidity of symptom construction and interpretation, which are essential ingredients for conducting a clinical intervention and assessing success or failure of treatment (Kirmayer, Lemelson, & Barad, 2007).
3. In light of the above, which are considered best practices in individual and collective interventions aimed at civilian populations exposed to armed conflict and war?
We must first acknowledge that developing a clinical evaluative framework for assessing individual and collective interventions among civilian populations in conflict and postconflict scenarios is extremely challenging, given the complexity of mass trauma, the heterogeneity of trauma and its victims, and the array of possible outcomes most interventions potentially have (Shalev, 2006). In clinical naturalistic studies, it may be difficult to attribute improvement to a given set of treatment practices, without randomization and controls to compare with. In this case, the final outcome of treatment may be influenced by other intervening factors, not necessarily strictly related to the treatment itself. Carefully designed psychosocial interventions studies are expensive and complex undertakings, requiring careful planning, clear definition of expected outcomes, and a solid evaluation design (Glass, 2000), conditions which are seldom applicable because of hectic and at times chaotic prevailing field conditions in conflict or postconflict settings.
Reports from clinical work conducted in recent war scenarios, where local populations were exposed to massive traumatic experiences—such as in Sri Lanka—indicate that meaning and narrative associated with trauma-related symptoms are culturally embedded (Somasundaram & Sivayokan, 2013) and further complicated by the often-neglected issues of history, identity, power, and gender. Local practitioners are fully aware of these intricate complexities, while foreign experts, clinicians, and first responders most often recruited and trained elsewhere remain oblivious to these issues. Moreover, the clinical management of trauma-related complaints among different cultures from our own, present clinicians with complex problems and demand clinical decisions that are extremely challenging. As symptoms are embedded in local systems of meaning and specific cultural explanatory frameworks, clinicians may have difficulties in understanding reactions and patients’ explanatory models, healing practices, and coping behaviors. The clinical interpretation of these interactive systems requires a solid knowledge of the local culture and their language, and the native taxonomies, including the local idioms of distress, local attributions of causality, and healing traditions (Abramowitz, 2010; Kirmayer et al., 2013; Pedersen, Kienzler, & Gamarra, 2010; Somasundaram & Sivayokan, 2013).
Nevertheless, despite the many limitations and constraints encountered in the literature reviewed, a number of approaches and actions were revealed as desirable or potentially useful in leading to best practices. The psychosocial interventions that were reported as beneficial were most often associated with the following features: (a) a primary concern in identifying those persons at risk and in greatest need for service (screening); (b) an implicit commitment to avoid inflicting further damage, while ensuring minimal disruption of existing (and still sufficient) coping and protective influences; (c) gaining in-depth insight, identifying specific cultural resources at the local level: local idioms of distress, healing practices (i.e., therapeutic rituals), and ways of coping with distress (i.e., symbolic as well as culturally significant ways of restoring social cohesion, religious practices, etc.); (d) building on the existing endogenous resources (i.e., key informants, healers, religious traditions, etc.) rather than exclusive reliance on external solutions of poor social relevance and cultural consonance; and (e) promoting empowerment using participatory action research approaches, where the community of actors and survivors is involved from the early stages of every assessment and/or intended action or proposition for strengthening social cohesion and increasing resiliency, including the provision of psychological support.
The systematic and focused review of the literature (see, for example, Agani et al., 2010; Anckermann et al., 2005; K. de Jong & Kleber, 2007; Doucet & Denov, 2012; Eppel, 2002; Keough & Samuels, 2004; Mercer et al, 2005; Stark, 2006; Stepakoff et al., 2006) clearly shows improved or better mental health outcomes when community resources and survivors were involved in the decisions regarding the support to be offered, Western and non-Western local cultural practices were sensitively combined, and activation and mobilization of local social support networks such as symbolic restoration of collective processes (i.e., for bereavement and grieving) were achieved, accompanied by the more general psychosocial support, including follow-up at later stages.
In a recently published book on Tamil populations in Northern Sri Lanka, Somasundaram (2014) makes a compelling case in favor of indigenous coping strategies and culturally mediated protective factors like rituals, funerals, and religious ceremonies, as crucial sources of collective strength, support, and meaning. Culture-specific relaxation techniques, such as the use of meaningful words according to different religions (Hindu, Buddhist, Islam, Catholic, etc.), combined with meditation, breathing exercises, and Ayurveda or Siddha oil massages and muscular relaxation, represent culture-specific powerful tools for healing massive trauma and strengthening positive resilience and collective coping strategies among the Tamils.
Other additional measures which may be considered no less important, but complementary to the best practices pointed above, have been postulated by Hobfoll and collaborators (2007) under the general title of “best intervention practices,” aimed at strengthening stress management and promote resiliency, as well as a series of supportive measures to restore the sense of safety, calm, self- and collective efficacy, connectedness, and hope (Hobfoll et al., 2007). Some but not all of these practices were used in the reviewed literature (see, for example, Agani et al., 2010; Anckermann et al., 2005; K. de Jong & Kleber, 2007; Doucet & Denov, 2012; Eppel, 2002; Mercer et al., 2005).
Finally, the discrepancies that have been made evident between some of the “recommended” best practices and the imperatives of conducting psychosocial interventions and clinical work on the ground arise from the vast divide existing between researchers, academic psychiatrists, and frontline clinicians (Litz & Gibson, 2006). Moreover, it becomes apparent that there is a crucial imbalance in the reviewed studies to effectively bridge the gulf that exists between research and action, or in other words between “what is known and what is done in practice, between scientific achievements and health realization” (Pang, Pablos-Mendez, & Ijsselmuiden, 2004, p. 720; Haines, Kuruvilla, & Borchert, 2004).
Limitations of the Study
The potential for selection bias in this literature review is acknowledged. A large number of humanitarian assistance initiatives conducted by multilateral and bilateral agencies, including international agencies, governments, and NGOs, are at risk of being underrepresented in our review. Assessments and research findings generated by such organizations are most often to be found in the gray literature, in nonindexed reports, or on websites or other media. Children, refugees, veterans, and the military were excluded and therefore are not at all represented in our review.
The results that are published in peer-reviewed journals are mostly interventions funded and conducted by foreign nationals, with variable support and actual engagement of local practitioners or researchers, which introduces the risk of bias in detriment of the latter. Consequently, there is a lack of recognition of existing local knowledge production and dissemination efforts by practitioners and researchers from LMICs, who are also underrepresented. The insufficient or limited participation of local practitioners and researchers may explain the limited follow-up and poor sustainability of most initiatives reviewed here.
Finally, as shown above, because some studies were unclear as to the methodology or research design used, lacked details on the content and duration of the interventions, and did not specify the training received and degree of professionalization of participating health workers and practitioners, the risks of misinterpretation remain moderate to high. At the same time, this also points to the fact that innovative approaches to research, capacity building, and knowledge translation are needed to achieve effective and sustainable psychosocial interventions in contexts affected by armed conflict and war.
Concluding Remarks
To summarize our main findings, we would like to raise four key issues of critical importance when considering psychosocial interventions and searching for best practices in conflict and postconflict situations.
First, while the concept of trauma in a given population after exposure to traumatic events appears to be universal, it has been described and experienced in many different ways across cultures and specific populations throughout the past few decades (Hinton & Good, 2015b). The metamorphosis and the ever-expanding and inclusive definition of the trauma construct have made the objective assessment of its existence problematic and one should exercise caution when trying to measure its occurrence and persistence over time in a given population. This “over inclusiveness” has been criticized by practitioners who point to the importance of distinguishing between what constitutes a normal versus an abnormal or pathological reaction to experienced life threatening circumstances (Horwitz, 2007).
The review of the literature shows that most interventions conducted in conflict and postconflict settings are bound to miss, distort, or transform the local idioms of the victims while translating local expressions into professional languages of complaint and restitution, which in turn are appropriated by donors and humanitarian organizations for political and moral purposes (Kleinman, Das, & Lock, 1997).
Second, as it has been stated by Shalev (2006), the interface between “stress theory” and the theories of “psychological trauma” has not been convincingly articulated. This have created additional ambiguities when distinguishing distress from disorder and introduced competing and even contradictory diagnostic and treatment practices, which are evident in the implementation gaps noted above. There is little doubt that the complexity of mass trauma and its aftermath, as well as the relative lack of theorization, have both hindered the quality of responses and efficacy of the interventions and therefore remained an obstacle to the emergence of best practices for wider application. First, responders and the medical and allied professions are still confronted with a lack of sound theoretical platform that would provide a rationale for the link between exposure, the psychosocial mechanism, and the end point of interest, introducing uncertainties and constraints in the model of clinical practice, as well as in the individual and collective interventions derived from it (Glass, 2000).
Third, our review of the qualitative literature ratifies to a large extent, what has been reported by Tol, Barbui, et al. (2011) in their meta-analysis of RCTs conducted in humanitarian settings, that most interventions had no reliable baseline data against which to measure progress, lacked specific outcome measures for assessing effectiveness, and did not specify length of time between exposure to traumatic experiences, initiation, and duration of treatment, thus limiting the analysis and interpretation of the findings. The various intervention designs reviewed here failed to specify the intervention target and expected outcomes in unambiguous terms and therefore both outcomes and impact remained difficult to assess systematically. Under these conditions, it is unlikely that some of the reviewed psychosocial interventions left behind a significant and durable impact on current local interventions and the model of clinical practice.
Fourth, the collected qualitative evidence does not support a specific intervention model nor a set of standardized best practices but reiterates the need for psychosocial interventions to remain flexible and adaptable to the prevailing social and cultural context and specific circumstances of the massive traumatic experience (Hobfoll et al., 2007; Shalev, 2002; Silove et al., 2014; Silove & Steel, 2006; Somasundaram, 2014; Summerfield, 2004). Notwithstanding, the literature review shows some promising pathways to follow, which may incrementally contribute to build-up empirical evidence for more efficacious, compassionate, and sustainable interventions across the response chain. These include devising more sensitive tools for screening, early detection, and treatment of those in need, discarding “mandatory” Western-driven interventions, which are irrelevant, unwelcomed, or not required (Ørner & Schnyder, 2003). We need to develop culturally appropriate interventions, including local practices to promote resilience and strengthen the process of natural healing and coping mechanisms, as well as focus our attention on both primary and secondary prevention domains, which are most often missing.
All of these key issues need careful consideration to develop preventive measures and early interventions for reducing chronicity and the overall burden of illness among survivors. In addition, in the mid- and long term, we need to move beyond the narrow psychological scope to restore the sense of safety, equity, and justice, while promoting agency and social cohesion among survivors. Aiming to normalization and resumption of everyday life, with the ultimate aim of reconstructing the social tissue, while, reducing inequalities, addressing social injustices, and rebuilding of local economies, appears to be the most appropriate course of action to prevent recurrent and endemic conflict and improve the overall mental health status of the affected populations.
Overall, the findings reported in this review are to some extent unexpected and may resonate well with scholars who have criticized a strictly medicalized model of care, by systematically offering psychiatric counseling and psychological support to people who have been exposed to traumatic experiences despite they may not be in need of professional care or assistance (Almedom & Summerfield, 2004; Jones, 2002). At the same time, it should reinforce the need for further research and innovation in the delivery of psychosocial support for those who just claim that the current responses are a rather insufficient or an “imperfect offering,” disproportionate to the magnitude of social suffering, despair and hopelessness survivors of mass trauma are confronted with (Orbinski, 1988).
The future global mental health research agenda should be focusing not only on the short-term impact but also the long-term impact on those exposed to intentional and protracted violence and traumatic events. We need to move beyond cross-sectional studies and refocus our attention to prioritize research on naturalistic and longitudinal studies of the clinical trajectory of posttraumatic adaptation as well as risk and resilience factors involved, acknowledging the multiple outcomes of trauma exposure. Moreover, we need to continue searching for new ways of preventing violence and conflict, reduce its sequelae and the short- as well as long-term health burden, while addressing social inequalities and pressing issues of social justice.
Finally, turning to the general area of intervention research in conflict and postconflict settings, the growing multidisciplinarity of research teams, the diversity of research paradigms and approaches, as well as the tensions between frontline health workers and clinicians, humanitarian agencies, donors, and researchers represent some of the main challenges to conducting intervention research. These issues need to be specifically addressed, especially in resource-poor countries with ethical and cultural frames of reference differing from Eurocentric Western paradigms.
In this focused and systematic literature review, we conclude that in spite of the many discrepancies and inconsistencies found, there is an emergent literature of positive empirical evidence being accumulated, derived not only from RCTs and meta-analysis but also from observational and qualitative studies, case reports, and community-based studies, including specialized reports and guidelines. There is sufficient critical input derived from these studies to support the continuing assessment, revision, and refinement of current and future guidelines for best practices in the provision of psychosocial care. This process of knowledge transfer should follow a rigorous scientific design and careful assessment of mental health outcomes, and subject to systematic field testing prior to its application. The ultimate aim would be not only the strengthening of humanitarian assistance policies and programs and improved psychosocial care for civilian populations in conflict and postconflict settings but should result in increasing the value and reducing the waste of psychosocial intervention research prevailing today.
Footnotes
Acknowledgements
The author(s) would like to acknowledge the assistance received in searching the literature from Nicole D’Souza and Consuelo Errazuriz.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authorship of this review article received partial financial support from the Global Health Research Initiative (GHRI), a collaborative funding partnership of the Canadian Institutes of Health Research, the Canadian International Development Agency, Health Canada and the International Development Research Centre.