
Abstract
If individuals believe they are healthier than they actually are, they may feel less compelled to improve their health. This study aims to examine the importance of a person’s connections in the correspondence between a person’s self-reported health (SRH) and having metabolic syndrome (MetS). Participants of the Kingston Senior Women’s Study (n = 100, 65 years of age and older) completed a questionnaire on their social background, psychosocial conditions, health behaviors, and health. Participants also provided physiological measures and medical information. Health overestimation was defined as reporting high SRH yet being diagnosed with MetS. Logistic regression was used to examine whether a person’s social networks increased the odds of health overestimation. About a third reported a high SRH and had MetS (36%), that is, overestimated their health. Participants had more than four social network ties on average, with a maximum of six reported ties. When control variables were accounted for, participants with larger network size had lower odds of health overestimation (odds ratio [OR] = 0.46, 95% confidence interval [CI] = [0.26, 0.80]). Women with larger social networks may have greater access to information about their own health, leading possibly to more accurate assessments. Such information may be conveyed via feedback from ties or via a more representative perception of what constitutes good health when self-assessing one’s health.
Background
Self-reported health (SRH) has been shown to be a strong predictor of objective health outcomes such as morbidity and mortality (Idler & Benyamini, 1997). Nevertheless, answering the SRH question “In general, would you say your health is: excellent, very good, good, fair, or poor?” is a cognitive process: (a) people must recall what they know of their health, (b) evaluate the meaning of the health aspects they recall, and then (c) make an overall evaluation of their general health status (Jylhä, 2009). Research has suggested that the meaning of excellent, good, or poor health often varies with age (Krause & Jay, 1994) and gender (Benyamini, Leventhal, & Leventhal, 2000; McCallum, Shadbolt, & Wang, 1994). For example, research has shown that the subjective health of older adults remains relatively stable, although their objective health worsens with age (Cheng, Fung, & Chan, 2007; Kunzmann, Little, & Smith, 2000). Studies have shown that women tend to have a broader view of their health, relying less than men on the presence of life-threatening conditions to evaluate their health (Benyamini et al., 2000; McCallum et al., 1994).
The disassociation between subjective health reports and objective health conditions among older adults reflects the fact that one’s expectations concerning health evolve alongside age-related health norms. Indeed, elderly people often associate their functional and physical decline with the normal aging process (Idler, 1993; Williamson & Fried, 1996). However, poor functional performance may have a detrimental effect on senior’s well-being when perceived as difficulties carrying out physical tasks (Weil, Hutchinson, & Traxler, 2014), which may further interfere with their independence and social life (Benyamini, Leventhal, & Leventhal, 2003; Østbye et al., 2006). In addition, social comparison processes and social network characteristics might also play a role in the congruence or non-congruence between subjective reports and objective health. For example, older adults seem to compare their health against worse-off same-aged peers and thus enhance their perception of health (Henchoz, Cavalli, & Girardin, 2008). In addition, according to Granovetter’s (1973) theory of weak ties, individuals with more weak ties may have access to a greater range and diversity of information, including, in this case, information related to personal health.
Metabolic syndrome (MetS) is defined as a cluster consisting of at least three of the following criteria: obesity, elevated blood pressure, low level of high-density lipoprotein (HDL) cholesterol, raised triglycerides, and fasting plasma glucose. MetS affects a large proportion of the senior population (Riediger & Clara, 2011), and has been shown to lead to type 2 diabetes and cardiovascular disease—the second leading cause of mortality among Canadians (Statistics Canada, 2011). Compared with functional health, MetS does not rely on an individual’s own assessment of their health. As such, a diagnosis of MetS represents a condition of which a person is likely unaware, and therefore, an objective condition with which to compare a person’s self health assessment.
Study Objective
This study aims to examine the importance of social networks in the correspondence between SRH status and having MetS in older women. More specifically, the study focuses on the network correlates of health overestimation, that is, reporting good health although having a poor health condition. Older women reporting a high SRH may be less likely to feel susceptible to poor health (Avis, Smith, & McKinlay, 1989; Kulik & Mahler, 1987). As a result, overestimators might be less likely to engage in health promoting behavior and thus remain with MetS, compared with those women who have a congruent perception.
Gap in Literature
Little research has examined the congruence between objective health conditions and subjective health reports and its potential health factors. Previous research has shown increased physical activity (PA) associated with lower odds of health congruence (Ruthig & Chipperfield, 2007) as well as high socioeconomic status and a greater sense of control associated with congruence (Delpierre et al., 2012; Lima-Costa et al., 2012; Rodin & McAvay, 1992). For example, Rodin and McAvay (1992) showed among the elderly that worsening health conditions were associated with a decline in their perceived health for those who initially had a higher feeling of control, while that was not the case for subjects who initially had a low sense of control. Compared with the other possible confounders, medication intake has yet to be explored in association with heath congruence, although it has been suggested that medication intake may help remind people of their specific health conditions (Johnston, Propper, & Shields, 2009).
Few studies have examined the importance of social networks in the accuracy of subjective health reports. Ruthig and Allery (2008) showed social engagement to be associated with higher risk of overestimating one’s health. Eller, Holle, Landgraf, and Mielck (2008) also found that social integration, particularly social support, improved the perceived health among diabetic seniors but it had no effect among non-diabetic ones. Nevertheless, it remained unclear which dimensions of support were associated with the overestimation of one’s health status. Facing declining health due to aging, older adults with greater support might possibly give less weight to their physiological health when assessing their overall health. Each senior adult seems to have a relatively unique definition of their health, from a physical level to a more transcendent level; individuals reporting high subjective health shown to have optimistic view and a transcendent definition of health despite actual poor objective health (Borawski, Kinney, & Kahana, 1996). Social support provides coping resources (Thoits, 2011) that may buffer the emotional impact of poor physiological health on ones’ perceived health. Consequently, it is possible that older adults with greater support give less weight to their physiological health in assessing their overall health. However, not every type of social support has the same association with health. In general, the primary network, for example, relatives, is the most efficient provider of social support and individuals expect emotional, instrumental and informational support from such close ties (Thoits, 2011). For instance, receiving support from children is often particularly meaningful for elderly people (Zunzunegui, Béland, & Otero, 2001; Zunzunegui et al., 2004). Nevertheless, it has also been found that the mere size of a social network has a positive effect on seniors’ health (White, Philogene, Fine, & Sinha, 2009). It is important to understand better what aspects of a person’s social network may be associated with health estimation.
Examining whether social networks are associated with health overestimation can aid in our understanding of the cognitive processes underlying SRH. As a first step in assessing their own health, individuals gather information about their health (Jylhä, 2009). The structure of a person’s network might play a role in this step of the cognitive process as a more diverse network can be a greater source of information (Granovetter, 1973). The cognitive processes underlying SRH may also involve a social comparison (Jylhä, 2009) in which individuals may use similar-aged peers who seem worse off as key referents (Heckhausen, 1999). As a result, older adults might enhance the perception of their own health by comparing themselves with same-aged peers in poorer health (Cheng et al., 2007; Heckhausen, 1999; Henchoz et al., 2008). This study aimed to examine the congruence between SRH and having MetS in older adult women and whether characteristics of women’s social networks might help explain this congruency. This study particularly opposes health overestimation to congruent health assessment because the former represents the risk of low perception of risk susceptibility compared with the latter (Avis et al., 1989; Kulik & Mahler, 1987).
Method
Sample
Data come from the Kingston Senior Women’s Study (KSWS) conducted in 2011. The KSWS consisted of a convenience sample of 100 women over age 65 from a mid-sized Canadian city. Using prevalence data on MetS in the Canadian population, sample size calculations were conducted for the purposes of detecting differences in MetS risk between socioeconomic groups. A sample size of 120 women would have allowed the KSWS to detect differences of 0.14 in MetS risk between high and low socioeconomic status (SES) women, with an alpha of .05 and a power of .90.
Participants completed a structured interview on their demographic background, social networks, health behaviors, and medical history. Participants also provided anthropometric data and submitted to blood pressure and cholesterol readings, which were used to diagnose MetS. This study was granted clearance according to the recommended principles of Canadian ethics guidelines, and Queen’s University policies.
Measures
Health overestimation was based on a typology of MetS and SRH. The harmonized definition of MetS was used to diagnose the MetS: To have MetS, a participant had to have at least three of the five following criteria: (a) waist circumference ≥ 88 cm, (b) triglycerides ≥ 150 mg/dL or specific treatment, (c) HDL-cholesterol < 50 mg/dL or specific treatment, (d) systolic blood pressure ≥ 130 mm Hg or diastolic blood pressure ≥ 85 mm Hg or specific treatment, and (e) fasting glucose ≥ 100 mg/dL or specific treatment (Alberti et al., 2009). Participants’ SRH was measured with the question, “In general, would you say your health is: excellent, very good, good, fair, or poor?” Based on the sample distribution, high SRH was defined as those reporting excellent or very good health. High SRH was cross-tabulated with whether a participant had or did not have MetS to produce a four-category variable. Health overestimation was defined as those participants who reported higher SRH but had MetS. Health congruency was defined as those reporting high SRH with no MetS (i.e., healthy realists) or low SRH with the MetS (i.e., ill realists). The “underestimators” group was excluded from analysis so that health overestimation could be compared with those who reported their health accurately.
Participants’ social networks were measured using a name generator/interpreter instrument. Two name generator questions were used: “name up to three people, with whom you have discussed important matters in the last six months?” and “name up to three people, with whom you have spent time on a regular basis in the last six months?” The discussant networks have been shown to have face validity in capturing members of a person’s core, supportive network (McPherson, Smith-Lovin, & Brashears, 2008). Previous work using name generators, particularly those capturing discussant networks, has shown health and health-related matters to be an important topic of discussion, particularly among women (Bearman & Parigi, 2004). Participants could report the same or different people in both generator questions. The name interpreter questions asked participants their age, gender, type of relationship, and the PA levels of their network members. Social Network Size was the number of different persons that participants nominated in the two name generator questions. Family Support Network was the percentage of relatives within a participant’s network. The Physical Activity Network was the percentage of network members with whom participants were physically active. The Presence of Similar-Aged Peers was the percentage of network members who were within 5 years of age to the participant was calculated.
In addition to our variable of interest, our analyses also adjusted for age, medication intake, subjective and objective PA levels, educational attainment, and sense of control. Medication intake was the number of different prescriptions that a participant took for hypertension, cholesterol, or diabetes. Objective PA consisted of the percentage of time when participants were physically active with at least moderate intensity while wearing an ActiGraph GT3X for a week. Accelerometers have been shown to provide reliant and valid data on PA (Berlin, Storti, & Brach, 2006). PA intensity was interpreted by the Freedson Adult equation. Subjective PA was measured by a shorten version of the Community Healthy Activities Model Program for Seniors (CHAMPS) Questionnaire (Stewart et al., 2001). Previous research has shown the validity of the CHAMPS PA Questionnaire among older adult populations (Stewart et al., 2001). Subjective PA scores were converted into caloric expenditure per week for at least moderately intense activities. For educational attainment, we considered the highest educational level of the female participant or her partner (if applicable). Educational attainment was grouped into seven ordered categories: (a) no degree, (b) high school diploma, (c) trades certificate, (d) college certificate, (e) university certificate, (f) master’s degree, and (g) doctorate degree. Sense of control was measured using Mirowsky and Ross’s sense of control scale composed of eight statements such as “I am responsible for my own success” to which participants had to give their level of agreement; participants can score from −16—lowest sense of control—to 16—highest sense of control (Mirowsky & Ross, 1991). The scale had a Cronbach’s alpha of .51. Despite the limited reliability, the scale has increased validity since it was developed specifically to cancel agreement bias among respondents (Mirowsky & Ross, 1991).
Statistical Analyses
Health overestimation may be viewed as the risk category for these analyses. To examine health overestimation and contrast it specifically with health overestimation, logistic regression analysis was used to examine whether the social network characteristics of older women increased or decreased the odds of health overestimation. Logistic compared with the possible use of multinomial regression also helped to preserve statistical power given the limited sample size. Three sets of models were run: Model 1 examining the bivariate association between health overestimation and the different network characteristics; Model 2 examining the association between health overestimation and the control variables; and, Model 3, the fully adjusted model, examining the association of health overestimation and any network variables found significant in Model 1, while adjusting for possible confounding variables A likelihood ratio test was used to compare the control model with the final including the social network size variable. Analyses were conducted using Stata 12 statistical software.
Results
Table 1 provides the descriptive statistics of the KSWS sample. Among the sample, 61% of the women reported being in high SRH; 62% of the women were diagnosed as having MetS. In terms of health overestimation, 36% of the sample reported high SRH, although having the MetS. Participants had, on average, more than four social network ties. Relatives composed almost half of the participants’ networks (49.7%), participants were involved in regular PA with 25% of their network ties, and over one third (38.06%) of the participants’ ties were within 5 years of the participant’s age.
Descriptive Statistics of the Kingston Senior Women Study (KSWS; N = 100).
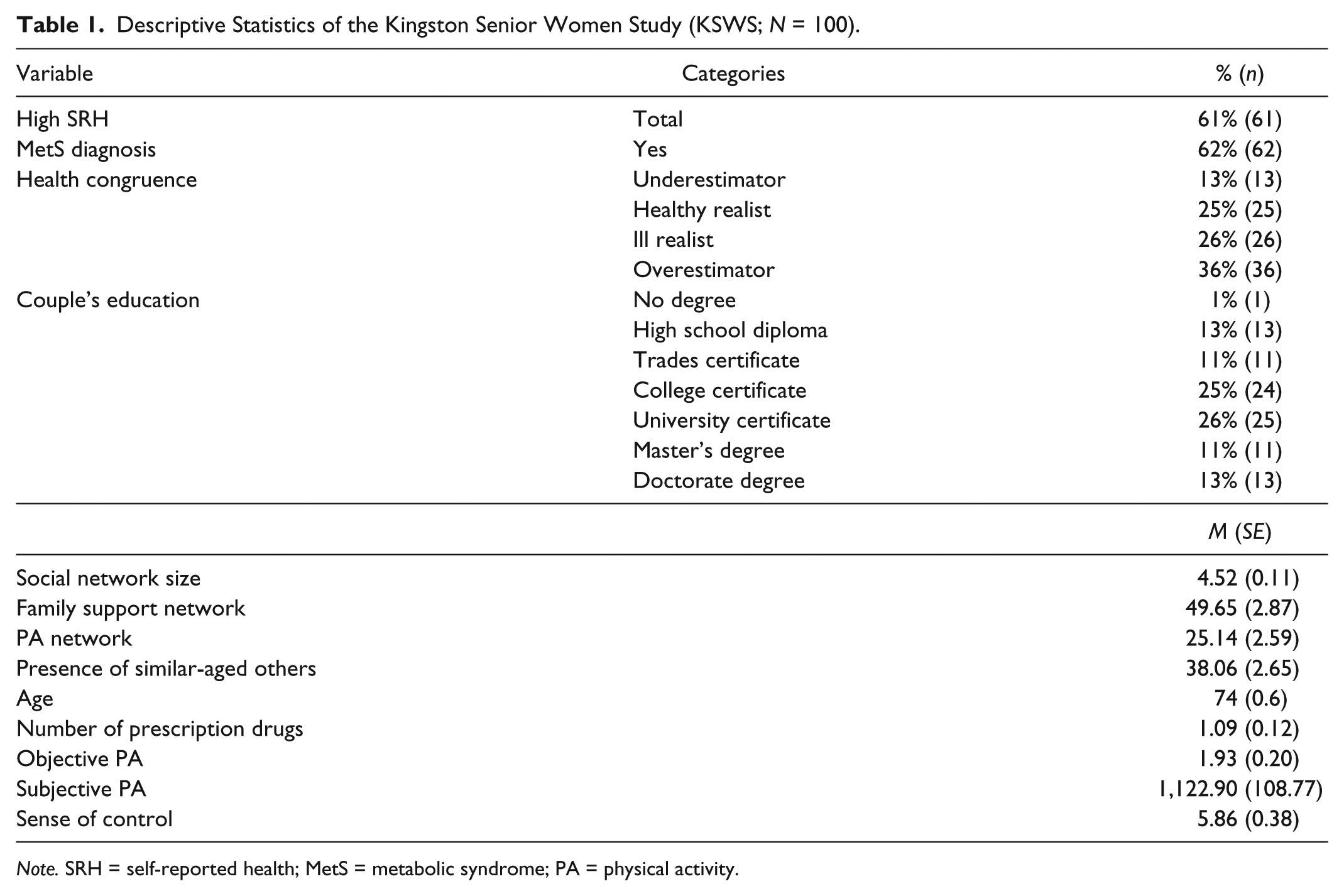
Note. SRH = self-reported health; MetS = metabolic syndrome; PA = physical activity.
Table 2 provides the estimates from the logistic regression of the association among network variables, confounding factors, and health overestimation. In the bivariate analysis (Model 1), social network size decreased the odds of health overestimation by 38% (odds ratio [OR] = 0.62, 95% confidence interval [CI] = [0.41, 0.93]). No other social network characteristics were associated with health overestimation. Social network size was also shown to decrease the odds of health overestimation in the full model. With each additional tie, participants were 54% less likely to overestimate their health (OR = 0.46, 95% CI = [0.26, 0.80]). Those with higher objective PA were also less likely to overestimate their health. No other possible confounding variables were associated with health overestimation. The likelihood ratio test showed that the social network size variable improved the fit of Model 2 (LR = 10.98, p < .001). In ancillary analyses (available upon request), social network size was not shown associated with SRH and MetS separately (Sabatier, 2014); thus, the association of network size with overestimation would not seem to be due to the association of social network size with the health conditions forming the health overestimation variable.
Logistic Regression of Health Overestimation, Odds Ratios (95% Confidence Interval).

Note. PA = physical activity.
p < .05. **p < .01. ***p < .001.
Discussion
Findings showed among older women that the greater the social network size, the less likely she was to overestimate her objective health; the composition of their close network was not associated with their health assessment, whether their ties were potentially supportive, physically active, or potential referent for social comparison. In other words, older women with larger networks tended to provide a more congruent assessment of their general health in comparison with their metabolic health. Larger networks may provide older women more accurate information about their own health. In our study, older women with larger networks tended to nominate different women with whom they discuss important matters and spend time. These women thus had different social circles in which they operated, possibly reflecting greater network diversity.
In his study of weak ties, Granovetter (1973) suggested that individuals with more diverse connections may occupy strategic bridging positions within networks, thus gaining access to a greater range of information and resources. Occupying bridging positions might aid in the accuracy of subjective health reports in two non-exclusive ways: (a) social feedback on health status from network members and (b) social comparison with a wider range of individuals when assessing one’s own health. First, social feedback from network members is a significant part of individuals’ recollections about their health when answering the SRH question (Suls, Marco, & Tobin, 1991) and receiving more feedback seemed related to a more accurate report of health conditions (Lipkus & Klein, 2006). Hence, the diversity of social relationships may be associated with the congruence between individuals’ report of general health and their objective health through providing feedback on their health status. Second, social comparison processes might also help explain the mechanisms linking network size and the reduced odds of health overestimation among older women. A larger social network may represent a wider and more representative range of referents, leading older women to have a broader perception of what constitutes average health for their age. Previous research has shown that adults are more likely to self-enhance their health perception through downward social comparison, with less healthy referents (Dunning, Heath, & Suls, 2004; Heckhausen, 1999). Adults tend to assess their health against a particular reference group rather than a wide representation of their peers (Jylhä, 2009). Nonetheless, according to Granovetter’s (1973) strength of weak ties theory, diverse networks may be more likely to include referents with a large spectrum of health conditions, possibly giving individuals access to a wider representation of what constitutes health at an older age. With a more representative perception of peers’ health, older women may use a more appropriate comparison referent when assessing their general health, reducing the chances of health overestimation.
Finally, these early findings on social networks and health overestimation suggest that SRH may be a less appropriate indicator of physiological health for older women with small networks. Future research with representative samples is warranted. However, results suggest that research on social networks and SRH may be underestimating the strength of the association between social networks and health, specifically among groups with fewer connections. PA, educational attainment, and perceived control have been shown associated with health congruency in other studies (Delpierre et al., 2012; Lima-Costa et al., 2012; Rodin & McAvay, 1992; Ruthig & Chipperfield, 2007). Nevertheless, none of these variables were associated with health overestimation among older Kingston women. In addition, this study demonstrated the lack of an association between health overestimation and medication intake, previously presented as a reminder of health condition (Johnston et al., 2009).
Limitations
This study had several limitations. First, the KSWS was a convenience sample of 100 older women in a mid-size Canadian city. Compared with older Canadian women, in general, the KSWS sample had higher proportion of women with higher educational attainment. For example, 50% of the KSWS sample earned a university degree compared with 16% of Canadian senior adults (Statistics Canada, 2014). Second, given the limited sample size, the study may have been underpowered to detect moderate to weak effects among certain variables in this study. Yet, given the small sample size and strength of the association shown between social network sizes, the study may in fact be underestimating this association. Third, the prevalence of MetS in our sample (62%) was higher than previous findings that have reported 39% of the 60- to 79-year-old individuals have MetS (Riediger & Clara, 2011). The larger prevalence may be due to the fact that the KSWS was designed to recruit older women who might have sleeping problems. Given that sleep problems have been shown to be associated with MetS (Coughlin, Mawdsley, Mugarza, Calverley, & Wilding, 2004), this aspect of the study may contribute to the higher rate of MetS in the KSWS women. Finally, this study represents a secondary analysis. Some variables were measured indirectly. For instance, social comparison was measured with the proportion of similar referents within participants’ network rather than asking “Do you compare yourself to others when assessing your own health, and if so, to whom?” As a result, the proposed interpretation of social feedback and social comparison on health is more speculative and intended to generate further hypotheses.
Conclusion
The KSWS sample size and composition restrict the types of conclusions that can be drawn. For example, given the limited variability in educational attainment among the KSWS, the study might have failed to detect the possible association between SES and health congruence, as has been found in other studies of older adults (Delpierre et al., 2012; Lima-Costa et al., 2012). Further research with a larger and more representative sample is needed to assess present findings. Despite these limitations, the study helps to generate different hypotheses, and is unique in its rich social network and physiological data on a sample of older adults. Studies of subjective–objective health congruency are limited, and even fewer have examined whether social network characteristics play a role in health estimation, particularly with a physiological health outcome such as the MetS. In addition, the sample consisted solely of women who were at least 65 years old. This homogeneity was a study strength particularly because people of different gender and age may assess their health differently (Benyamini et al., 2000; Cheng et al., 2007; Kunzmann et al., 2000; McCallum et al., 1994).
Asking a person to answer a question about their own health involves the person in a cognitive process: an assessment based on what individuals know about their health (Borawski et al., 1996; Jylhä, 2009). Our findings suggested that the social networks of older women might play an important role in the health self-assessment process: Older women with more diverse networks might have greater information on their own health. Finally, asking questions on SRH and social network diversity might help identify women at risk of cardiovascular disease but who might be less inclined to participate in health promotion programs and it might further develop targeted recruitment strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work has been supported by the Early Researcher Award program of the Ontario Ministry of Research and Innovation (ER09-06-210).